
Abstract
This article presents interview and focus group data from veterans of recent conflicts in Iraq and Afghanistan about their use of cannabis as a coping tool for dealing with posttraumatic stress disorder. Veterans’ comparisons of cannabis, alcohol, and psychopharmaceuticals tended to highlight advantages to cannabis use as more effective and less complicated by side effects. Some participants suggested that cannabis can be part of an approach-based coping strategy that aids with introspection and direct confrontation of the sources of personal trauma. Others, however, held that cannabis use was part of a less productive, avoidant coping strategy. Some self-reports suggested the need for more nuanced theorizations of coping behaviors, as they indicated motivations for use that were grounded in symptom alleviation rather than any direct confrontation with (or avoidance of) sources of trauma.
Introduction
A medical and political controversy currently surrounds the use of cannabis for posttraumatic stress disorder (PTSD). Even in states with fully implemented medical cannabis programs, PTSD is often not recognized as a disorder treatable with cannabis (Frosch, 2010a), and research has been hindered by a lack of federally sanctioned sources of cannabis (Frosch, 2011). The U.S. combat veterans are one of the most vocal groups seeking access to cannabis for alleviation of PTSD symptoms. A petition with more than 8,000 signatures lodged at the We the People section of the whitehouse.gov website (Whitehouse.gov, 2011) received an official response from the Office of National Drug Control Policy head, Gil Kerlikowske, who presented skepticism about the status of smoked cannabis as a “safe and effective medicine.”
Although the Obama administration has tabled the discussion of federal mandates for medical cannabis use, the departments of Veterans Affairs (VA) and Veterans Health Administration (VHA) have taken action to remove VA patients’ barriers to state-sanctioned cannabis use. Where, in the past, veterans could be denied analgesic medications and other treatments whether they were determined to be cannabis users, a new 2011 policy removed such obstacles. Under the new policy, veterans “participating in state marijuana programs must not be denied VHA services” (Department of Veterans Affairs & Veterans Health Administration [VA & VHA] 2011), although referrals to medical cannabis dispensaries cannot be provided by staff themselves (see also Durkin, 2013; Frosch, 2010b).
These recent policy shifts inform this article’s documentation and categorization of recent veterans’ narratives about the use of cannabis within the context of PTSD. The research findings reviewed subsequently suggest a number of potential mechanisms for cannabis’ efficacy, and this article offers a unique evaluation of recent veterans’ own perspectives on the multiple ways in which cannabis can aid in the management of PTSD.
Background
PTSD Among Recent Veterans
Many veterans returning from Operations Enduring Freedom and Operations Iraqi Freedom in Iraq and Afghanistan (hereafter “recent veterans”) experience mental health challenges. Developing precise estimates is challenging (Ramchand et al., 2010), but one large-scale study of recent veterans who had presented at the VA found that over 35% of the sample had received mental health diagnoses, PTSD being the most prevalent (Cohen, Gima, Bertenthal, Marmar, & Seal, 2010). Other studies of veterans presenting at VA hospitals have found that PTSD prevalence can surpass 50% (Lew et al., 2009).
Research indicates many recent veterans’ mental health conditions go undiagnosed and untreated (Vazan, Golub, & Bennett, 2013), often due to confusion about benefits, stigma (Brown, Creel, Engel, Herrell, & Hoge, 2011), and/or mistrust of the VA (Hoge et al., 2004). What is evident from the body of emerging research on this topic is that PTSD affects a far greater proportion of recent veterans than was previously thought, due in part to the slow manifestation of the disorder in some individuals and the large number of individuals who experience at least some PTSD symptoms but do not meet clinical criteria for an official diagnosis or deliberately avoid official diagnoses (Andrews et al., 2007; Seal et al., 2012).
One of the principal challenges for PTSD diagnosis, treatment, and recovery efforts (including informal coping behaviors) is the disorder’s symptomatological complexity. Recent revisions to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) require exposure to a traumatic event (or vicarious exposure to an individual with direct experience of trauma) as well as the experience of symptoms in each of the following four categories: intrusion, avoidance, cognitions/mood, and arousal/reactivity (American Psychiatric Association, 2013).
Intrusion refers primarily to recurrent memories, nightmares, and/or flashbacks of a traumatic event. Avoidance refers to the persistent effort to avoid trauma-related stimuli and reminders (often referred to as “triggers”). Alterations in cognitions and mood can range from dissociative amnesia to fear, horror, guilt, blame, social alienation, and anhedonia. Arousal- and reactivity-related symptoms include aggression and irritability and issues with concentration as well as hypervigilance and an exaggerated startle response.
Not only are some of these symptoms seemingly contradictory (e.g., social aggressivity and withdrawal), but their manifestation often appears cyclical, moving between periods of intense involvement in intrusive memories or social–environmental triggers and periods of equally intense social and emotional withdrawal or detachment (Litz, 1992). As a result, understanding the equally variable and time-sensitive strategies employed to cope with PTSD has become a pressing and timely topic of research.
Coping With PTSD
PTSD is a chronic condition for many and has no simple cure. A wide variety of treatments has emerged, spanning an enormous range of psychological, pharmacological, and alternative healing modalities (Cukor, Spitalnick, Difede, Rizzo, & Rothbaum, 2009). Often these strategies are tailored to an individual’s changing condition and evolving needs. Similarly, the informal coping behaviors that individuals employ to alleviate PTSD symptoms and move toward recovery are likely to vary considerably and involve multiple coping behaviors or “strategies” (Lazarus & Folkman, 1984).
Coping strategies as they have been studied within psychological research include all forms of thought and behavior used to manage or regulate stressors and their impacts in an individual’s life. In the past, most studies categorized coping behavior according to a dichotomy distinguishing between “approach-” and “avoidance-” based strategies. Approach-based coping encompasses the numerous responses to stress that are oriented toward direct confrontation of the stress-inducing problem, whereas avoidance-based coping involves shifting cognitive or emotional focus away from the problem, often through escape, denial, distraction, or wishful thinking (Moos, 1995).
Critical reevaluations of dichotomous conceptualizations of coping have begun to suggest their limitations. Skinner, Edge, Altman, and Sherwood argued that too many discrete coping behaviors (such as social support seeking and emotional discharge) can defensibly be placed on either side of the approach/avoidance divide (2003). Another domain that challenges these dichotomies is relaxation/leisure, which would appear to be classically avoidant but has been shown in research to be a robust predictor of well-being, rivaling approach-oriented strategies (Frydenberg, 2008). This finding is particularly relevant for substance-related coping, which has traditionally been associated with avoidance and escapism but may be a part of relaxation-seeking or symptom-alleviating efforts.
Approach-based PTSD coping
Several effective treatment modalities for PTSD are based on the principles of approach-based coping. For example, exposure-based therapies are widely used to directly confront trauma-related stimuli and reminders (Foa, Hembree, & Rothbaum, 2007). These therapies often use imagery and virtual reality technologies to simulate commonplace wartime traumas and trigger painful recollections (Beck, Palyo, Winer, Schwagler, & Ang, 2007; Hoffman, 2004; Reger & Gahm, 2008), ultimately seeking extinction of PTSD symptoms through repeated exposure to the very stimuli veterans with PTSD traditionally avoid.
Avoidance-based PTSD coping
Within the field of PTSD research, empirical work has provided some support for the approach/avoidance binary in predicting symptomatological severity. Avoidant coping has been linked to more severe PTSD symptoms in war veterans (Sutker, Davis, Uddo, & Ditta, 1995). In studies of other PTSD populations, avoidant strategies have been correlated with a greater number of PTSD symptoms among victims of intimate partner violence (Arias & Pape, 1999) and survivors of car accidents (Fecteau & Nicki, 1999) and both sexual and nonsexual assault (Dunmore, Clark, & Ehlers, 1999).
Drug treatments for PTSD
Treatment as usual for most PTSD sufferers involves one or more psychopharmaceutical drugs, the use of which might plausibly be categorized as avoidant, insofar as the aim of antidepressants, sedatives, and antipsychotics is alleviation of PTSD symptoms and not direct confrontation of the source of trauma (Friedman, 1997; Steckler & Risbrough, 2012). Clearly, however, pharmacological approaches to PTSD, including a new array of substances acting upon processes of memory formation (Cukor et al., 2009), have established efficacy and may serve to enhance the effectiveness of more conventionally approach-based therapies, such as exposure-based psychotherapy. Questions remain, however, about the extent to which the same may hold for other memory-affecting substances, such as cannabis, that are being used by many experiencing PTSD symptoms.
PTSD and Substance Use
Substance use disorders (SUDs) involving alcohol, illegal drugs, or the misuse of prescription medications are extremely common among those with PTSD and may result in part from individuals’ substance-related coping. Between 60% and 80% of Vietnam vets with PTSD, for example, also have SUDs (e.g., Keane & Kaloupek, 1997). Although SUDs involving stimulants and opioids have been shown to be prevalent among veterans, alcohol remains the most commonly used substance within the population. One study of those seeking outpatient treatments through VA PTSD programs found that 44% met criteria for an alcohol use disorder (Fontana, Rosenheck, & Spencer, 1998).
Because of the association between PTSD and SUDs and the risks of dependence when substance use becomes part of a regular strategy for managing a mental health disorder, some researchers have classified attempts to remediate PTSD with substances as misguided (Keane & Wolfe, 1990). Other researchers, however, have begun to consider the ways in which alcohol and other substance use can be a component of adaptive and effective coping repertoires (Duhachek & Kelting, 2009). Abueg and Fairbank have emphasized a form of interaction (1992) predicated upon self-medication (Khantzian, 1997). Alcohol, in particular, has been shown to be able to provide a remediative effect on anxiety, stress reactivity, and even cognitive functioning among those experiencing PTSD (Levenson, Sher, Grossman, Newman, & Newlin, 1980; Meisler, 1996; Stewart, 1996; Stewart, Pihl, Conrod, & Dongier, 1998). In a clinical study of PTSD in Vietnam-war combat vets, Bremner, Southwick, Darnell, and Charney found that alcohol, cannabis, heroin, and benzodiazepines all helped alleviate PTSD symptoms affecting sleep and startle response. In contrast, cocaine had a negative effect on symptoms related to sleep and arousal (1996). Given the broad spectrum of documented effects for cannabis, including sedative, analgesic, hypnotic, and stimulant effects (Earleywine, 2002), further research into the substance’s efficacy for different PTSD symptoms is clearly indicated.
PTSD and Cannabis
Relative to alcohol, very little is currently known about cannabis’ distinct forms of interactions with PTSD symptoms. A number of studies, however, have documented correlations between PTSD and cannabis use across populations. Generally speaking, cannabis use appears to be higher among trauma survivors than in the general population (Cougle, Bonn-Miller, Vujanovic, Zvolensky, & Hawkins, 2011; Kilpatrick et al., 2000; Lipschitz et al., 2003; Rohrbach, Grana, Vernberg, Sussman, & Sun, 2009; Vlahov et al., 2002).
Several studies examine associations between individual traits and the use of cannabis for coping with PTSD. Potter, Vujanovic, Marshall-Berenz, Bernstein, and Bonn-Miller found those living with PTSD who have a lower perceived capacity to withstand emotional distress are more likely to use cannabis to alleviate negative mood states (2011). Bonn-Miller et al. found that, 4 months after discharge from residential PTSD treatment, individuals who experienced lower levels of change in treatment were more likely to use cannabis. The finding did not hold for any other substances, suggesting that cannabis may be used as a means of coping or self-medication for a hard-to-treat subpopulation (Bonn-Miller, Vujanovic, & Drescher, 2011).
Similarly, alleviation of sleep problems, especially nightmares, has been shown to be associated with cannabis use among PTSD patients (Bonn-Miller, Babson, Vujanovic, & Feldner, 2010). One recent study found that over 70% of their sample of patients with PTSD experienced considerable reduction in nightmare intensity or total cessation of nightmares after taking nabilone, an endocannabinoid receptor agonist (Fraser, 2009).
Method
This study used interviews and focus groups to study cannabis and other substance use in the context of PTSD among formerly enlisted veterans who returned to New York City (NYC) neighborhoods. Participants for this analysis were drawn from two studies. Focus group participants were recruited for an exploratory study of substance use among recently returned veterans to NYC. Individual interview participants represent a cannabis using and PTSD-experiencing subsample from a 5-year longitudinal panel study of 269 recent veterans (Golub & Bennett, 2013) recruited using respondent-driven sampling (Heckathorn, 1997, 2002). Eligibility criteria for both studies required that participants served in a branch of the U.S. military after September 11, 2001, and had separated from the military within 24 months at time of recruitment.
Focus Groups
The impetus for this study of PTSD and cannabis use emerged from preliminary focus groups conducted with recent veterans who were recruited separately for a qualitative substudy focusing on mental health concerns and substance use. This study draws on two single-session focus groups of 10 participants each, including 6 women and 14 men. Of those 20, 10 identified as Black/African American, 5 as Latino/Hispanic, 4 as Caucasian, and 1 as Asian. At the time of screening for focus group eligibility, 16 of the 20 self-reported PTSD, either as a formal clinical diagnosis or as a self-diagnosed condition. Each focus group lasted roughly 2 hr and included open-ended questions about mental health and substances in the context of civilian reintegration. Questions about how pharmaceuticals and illicit substances helped with or hindered reintegration challenges (including finding employment, housing, and living with mental health concerns) were posed, resulting in lively conversations about the advantages of marijuana for dealing with depression, PTSD, and physiological pain.
In-Depth Interviews
After discussing the main themes identified by focus group participants, project staff sought to conduct in-depth interviews with a small sample of veterans in the parent study, who had already been identified by field staff as both experiencing PTSD and using cannabis regularly. The three military veterans serving on the field staff each consulted the lists of participants they had personally enrolled in the parent study and nominated those whom they felt would be ideal candidates for in-depth interviewing. Potential participants were contacted by field staff, informed that a substudy looking at “marijuana and PTSD” was underway, and provided the lead author’s contact in the event that they wanted to participate. Potential participants were informed that their decision to participate or not would have no bearing on their incentives or status as participants in the parent study. Of those initially nominated, 11 out of 12 contacted the lead author. After potential participants were informally screened to confirm current cannabis use and experiences of PTSD, interviews were scheduled. PTSD checklist scores from baseline and Wave 1 parent study data were also checked for each participant to verify that a PTSD Checklist Military version score indicating at least some PTSD symptomatology had been collected for each participant. The mean score across the 11 participants was 44.25, corresponding with “moderate PTSD symptomatology” but slightly below the “severe PTSD” cutoff of 50. Of this group of 11 focal participants, 2 were women, 5 identified as Black/African American, and 4 as Latino/Latina.
Semi-structured interviews lasted between 80 and 120 minutes and were organized around three main topic areas (1) the participants’ history of cannabis use, (2) the participants’ history of PTSD, and (3) the participants’ experiences with cannabis use within the context of PTSD. To avoid leading participants or superimposing a priori constructs of interest on the dialogues, narratives about PTSD and cannabis were elicited separately and specific questions relating to the ways in which cannabis use is experienced as affecting PTSD experiences or symptoms saved until the end of the interview. References to other substances and medications were pursued by the interviewer but not asked about systematically. All 31 participants whose firsthand accounts were included in this analysis were compensated US$40 for their participation, either in a qualitative interview or in a focus group session. All recruitment and data collection procedures were approved by the National Development and Research Institutes’ institutional review board (IRB). All names used in this article are pseudonyms selected by participants themselves.
Coding and Analysis
The interviews and focus groups were digitally recorded, transcribed, and reviewed for accuracy. Transcripts and field notes were entered into Atlas.TI for electronic storage, coding, and data analysis (see Figure 1). At the time of coding, several overarching, a priori code categories were identified for the project director, coinvestigator, and research associate who served as the three coders for this analysis. These included the symptom categories for PTSD as well as the approach/avoidance coping binary reviewed above. Coders were encouraged to identify emergent themes as they reviewed interview and focus group transcript data employing the principles of grounded theory (Charmaz, 2000; Glaser & Strauss, 1967). New, emergent and in vivo codes were discussed at weekly staff meetings. The inductive process entailed suggesting new code categories and rereading transcripts in light of proposed changes. The principal a posteriori code described in this article resulted from an ongoing discussion between coders about the difficulties in identifying substance use for coping as either approach-based or avoidant. After reviewing the transcript segments that resisted easy coding within this binary, staff determined that the use of cannabis to mitigate or alleviate PTSD symptoms (without explicitly seeking to engage or avoid memories of traumatic events) warranted an emergent coping category that has been provisionally identified as “symptomatological coping” in the analysis that follows.
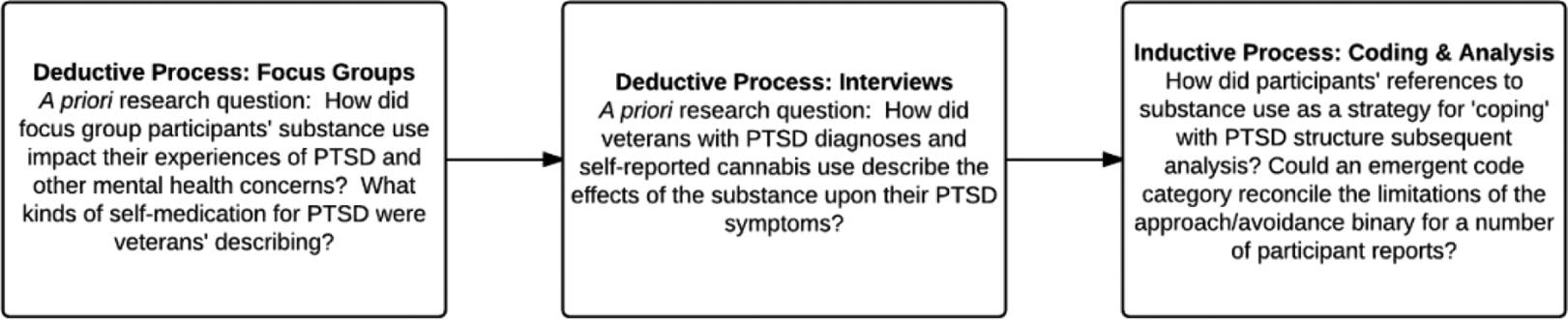
Deductive and inductive processes.
Figure 1 details the sequencing of deductive and inductive processes involved in this study’s theoretical, data collection, and analytic methods.
Results
The organization of findings below follows the sequencing of methods diagrammed in Figure 1, beginning with a more general review of participants’ experiences with psychopharmaceuticals and alcohol in the context of PTSD before moving into more detailed findings about cannabis from the in-depth interviews. The perceived effectiveness of cannabis for coping with different symptom categories is addressed, and reports throughout are discussed in terms of their suggestion of an approach-based, avoidant, or symptomatological coping strategy. Finally, the emphasis in current therapeutic approaches to PTSD is considered in conjunction with accounts, suggesting that cannabis can be used as an aid to conventional exposure- and approach-based therapies
Treatment as Usual—PTSD and Psychopharmaceuticals
Participants universally spoke to the strong personal dedication required to overcome the challenges of PTSD. A few spoke positively about professional counseling. More commonly, they spoke of their mistrust of the VA or “the system” and the therapies and medication that they provide. As one focus group participant, Oliver, a 37-year-old a Black male Army veteran, argued, treating PTSD or other psychological disorders has to be more than an impersonal application of diagnostic categories: Personally, [the problem with PTSD] comes down to the medical field.…That’s what’s sad because we come home, we’re vets and they write you off. They just throw a [PTSD] title on you and keep you moving, and you’re labeled. You have to be a person who understands people…to have an idea of what they are going through.
For a sizable number of the veterans with whom we spoke about PTSD, distrust and dissatisfaction with treatment was at least partly directed at their prescribed PTSD medications. For some, like Jane, who addressed others in the room during a focus group, psychopharmaceuticals were dismissed as part of a larger system based on profits: I commend all of ya'll for being vets, but there are ways of snatching yourself out of your depression…I know it doesn’t happen overnight. I’m speaking from experience: really you don’t need medications—it’s just a hustle. At the end of the day, don’t feel reliant on pills or the system, which is failed.
Although political opposition to the VA and to the military in general ranked high among the stated objections to seeking out pharmaceutical assistance for PTSD, for others, like Ian, a White 28-year-old Army veteran, the problem was articulated as a spiritual one: I think I should go to the VA and see somebody about like my depression, maybe try some anti-depressants, [but] I’m kind of torn about that. I feel like if I take some pills it would be great, but, you know: taking drugs to be happy kind of clashes with my spirituality in a weird way.
For the majority of participants reporting avoidance of pharmaceuticals, however, it was firsthand experience with PTSD medications and their side effects that had led to a rejection of all prescription drugs. Bambi, an African American veteran with a history of military sexual trauma, for instance, spoke of specific activities with which her PTSD medications had interfered: I don’t want to be on no psychotic meds right now, ’cuz I don’t know what they are. The medication, I don’t know…I don’t want shit that’s gonna stop me from having sex, or from laughing hard. I don’t want shit that’s just gonna change my whole mood. I was on some shit before and I didn’t even realize [that I had lost my sex drive and sense of humor].
Given the range of symptoms defining of PTSD and the highly personal experience of living with them, treatment often involves a lengthy period of multiple, alternating medications. Blue, a Black male Army veteran, described his difficult process of first being diagnosed with PTSD (after an incorrect diagnosis of bipolar disorder, he noted) and then trying to find the right combination and balance of medications to alleviate his PTSD symptoms: Oh boy, I was given, Remeron, Paxil, Depakote, Celexa…[and] 3 other things.…Mainly my meds were to give me clarity, to stop my racing thoughts, and to help me sleep. I took the medications and I was very uncomfortable, because I felt like wrapping myself in a blanket.…I felt like an earthworm. I could not be up and around people. Definitely withdrawn, so I just stopped. I figured out after I got to my fifth pill that it wasn’t going to work. I needed my own medicine.
For many with whom we spoke, this theme of “needing one’s own medicine” appeared to take precedence in their decision to reject pharmaceutical therapies in favor of a self-medicating approach to chemical coping.
Alcohol-Related Coping
Veterans reported only negative experiences of trying to cope with PTSD by drinking. Mr. Afghan, an African American Army veteran, described his own experimentation with alcohol for self-medication and the resulting depression and loss of clarity: I think alcohol is a lot more counterproductive to those dealing with this kind of situation [PTSD]. I really do. Because it can get severe. It can get to self-loathing. You know, PTSD paired with too much alcohol can [escalate from depression to suicidality]. You know? I’ve seen that. There’s no clarity in alcohol! I’ve been drunk all over the world, and I’ve never found it!
For others, like Manuel, drinking increased the chances of aggressive behavior or a violent outbreak, reducing its viability as a form of PTSD-related self-medication. “Tell me,” he queried the interviewer, “how many stoned people have you seen getting in bar fights?” Wolverine echoed this theme, speaking of the danger of becoming the incredible hulk (a creature defined by what he called “rage and uncontrollable emotion”) when drinking.
Cannabis-Related Coping
Participants reported various PTSD-related benefits resulting from their cannabis use, which are organized below around DSM symptom categories for PTSD.
Alterations in cognitions and mood
Logic, a Latina Navy veteran, offered a broad account of cannabis’ contributions to her readjustment and PTSD. Unlike most of the participants in the subsample, Logic confided that her PTSD was grounded in a traumatizing marriage to a fellow Navy veteran, followed by a divorce, a period of self-realization about her own lesbianism, enrollment in a full-time college degree program, and her new status as a single mother of an autistic child. Regarding cannabis’ role in her difficult recovery process, she remarked: I’m pretty open about it [telling people I use cannabis]. [Cannabis] cures the PTSD, the depression, the anxiety at times, especially while I’m going to school. Engineering school. Real stressful. And I try to handle it as calm as possible.
Logic’s belief that cannabis can mitigate stress and anxiety was one shared with most of our other participants. One of the most frequently cited reasons for smoking cannabis by veterans living with PTSD was its generally relaxing effects. Speaking as a veteran who had not used cannabis prior to or during deployment but had experimented with it post-separation, in the context of mounting difficulties relating to civilians, Bambi explained: I noticed that [after smoking] I just relaxed. It even felt like, I felt like I felt my muscles just go limp, like they just relaxed. My shoulders just went down.
Logic’s and Bambi’s accounts of cannabis’ effects suggest a form of potentially avoidant coping grounded in physiological release and cannabis’ purported anti-anxiogenic effects. Their accounts, however, focus on particular PTSD symptoms and suggest a more targeted effort to alleviate them than we found in other accounts. Evan, a White Army veteran living in a homeless shelter when recruited into the project, for example, offered an explanation of cannabis’ effectiveness for PTSD grounded in what he referred to as “distraction”: [Cannabis is] a great distraction, it will distract your mind from everything else that doesn’t make you feel good. The only thing that you’re going to do when you’re stoned is things you like. Being stoned makes everything interesting. It’s like, let’s watch C-SPAN. I’m telling you that was the most interesting episode of C-SPAN EVER! [Laughter.] I can see how people use it as an anti-depressant. How many people do you see pissed off when they’re stoned?
Evan’s elaboration on the potential for cannabis to make even mundane TV an immersive experience is indicative of classically avoidant or escapist coping strategies, although his narrative is complicated by the reference to cannabis as an antidepressant. As Cali, an African American Marine veteran contended, relieving the alterations in mood characteristic of PTSD can have more wide-ranging value than just a simple, short-term distraction. Speaking of his PTSD-related anxiety, he explained that his own experiences of the disorder were often somatic, resulting in high levels of chronic pain and making cannabis more than a simple relaxation aid: [Cannabis] helps with the pain. Because I didn’t even know that PTSD caused physical pain. But upon doing further research…[I learned that] stress causes physical reactions.
Implicitly addressing the commonplace lack of pleasure and enjoyment experienced by veterans with PTSD, another focus group participant, Blue, an African American male, explained that learning to cope with PTSD is about identifying one’s own pathways to positive emotions and outlooks: Every disorder has different triggers. [You need to] find something that triggers the happiness. I self-medicate. [Cannabis] is my mental and social support system. If I want to detach from any emotional or mental pain, I go smoke weed [with other people].
Blue’s commentary here is complex and suggests a twofold effect for cannabis, that is, its antidepressant qualities (a means of “triggering” happiness) and its distancing effect on psychological distress. Even the suggestion of a use-pattern based upon “detachment” in the account is complicated, however, by cannabis’ place within supportive social relationships, such that a classically avoidant strategy of detaching is coupled with a traditionally approach-based appeal to social support. Further, his use of the term self-medicate—a term used without prompting by a number of our participants—indicates a deliberate action rather than a haphazard or avoidant strategy.
Intrusion symptoms
As Blue suggested, understanding one’s triggers comprises a critical dimension of living with PTSD. A number of our interviewees suggested that cannabis had been effective in preventing unwanted dissociative reactions, or “flashbacks,” and in providing a buffer against disruptive memories and suggestive stimuli (e.g., the sound of dumpster lid closing that was interpreted as gunfire by one participant) to the point that intrusion “episodes” could be avoided. Cali explained that cannabis can create a state of calm that diminishes the likelihood of being caught off guard emotionally when confronted by civilian disrespect: I mean, I smoke and I'm mellow. I'm calm. I can take anything in stride. You know? Somebody can curse me the fuck out, tell me off at the store, and if I'm stoned I'm just like whatever. You know?
Similarly, Jason explained that he has learned to use cannabis as a preventative tool rather than a regular form of self-medication: If I have an inkling that I’m going to bug out today, I’m smoking to keep myself calm.…Oh no, I’m bugging out today. What the fuck? Let me take a smoke…sit back, alright. OK. Why did I feel that way earlier? Oh! Probably because this had happened and you let it get to you. I can do that [with cannabis]!
This theme was echoed by Chief who arrived late to his scheduled interview because of a near “episode” that led to him searching out cannabis: Part of the reason I almost had an episode today is that [I didn’t have any cannabis]. I had to find it. I had to calm down.
Logic commented succinctly: It [cannabis] calms me, as far as not having a trigger.
These accounts, taken together, suggest a more important symptomatological coping role for calming/relaxation than was anticipated. Many of the new developments in PTSD pharmacology as reviewed in articles referenced above (Cukor et al., 2009; Steckler & Risbrough, 2012) are prophylactic in nature. Little is known about how cannabis’ demonstrated effects on memory formation may impact PTSD manifestation and progression at various intervals from the experience of traumatic stress. What these reports suggest, however, is that these users believe their cannabis use leads to a state of calm by reducing their stress reactivity and susceptibility to triggers.
Alterations in arousal and reactivity
As several interviewees explained, one of the main day-to-day challenges of living with PTSD is managing a stream of unending thoughts leading to hyperactive arousal. For those reporting sleep problems, the racing thoughts and lack of concentration often associated with PTSD were frequently cited as causing their insomnia. My mind’s always going, and it fucks with you after a while.…Can I just focus on one thing for a change? It’s easier for me to concentrate on one thing at a time [when I smoke cannabis]. All the studies that are put into it.…Pfft [sound of derision]. Pot has more positives than it does negatives. There’s no way to argue with it.
Mr. Afghan, who is quoted above describing the range of pharmaceuticals he had been prescribed, spoke in more detail when asked how cannabis affected his racing thoughts. They are focused. They’re not calm. They can still race, but they’re focused because now I know why the thoughts are there, what the thoughts are, and what they’re centered around. That’s the clarity.…It doesn’t slow the thoughts down, but it gives me more time to slow down and compartmentalize things.
The broad category of relaxation/calming here appears to take on a greater significance in the alleviation of PTSD symptoms than simply providing a helpful distraction.
Confronting Traumatic Memory
Recent therapeutic approaches and technologies reviewed in the background section of this article have aimed for a more active engagement with traumatic experiences as a pathway to recovery. To a great extent, an approach involving direct engagement with traumatic memories has been taken up by these participants, a number of whom spoke to the challenge of identifying the source of one’s PTSD. For Evan, the task of resisting the characteristic tendency to avoid traumatic memories was a difficult one. As he explained, veterans who have been trained to suppress and hide all emotions return home ill equipped for readjusting to civilian life and seeking out the psychotherapy many of them need: A lot of vets never even leave the military [at least not mentally]…. They’re not normal people. They don’t have time for emotion. It just gets in the way. They’re all fucked up and half the time they don’t even realize it. They try to ignore it.
Offering a potent metaphor for the return to emotionality and the confrontation of one’s PTSD, Keisha, an African American Army veteran commented: It’s like reverse psychology. [Rather than avoid thoughts of the past] you have to go to ground zero. What started the trauma in terms of PTSD? Then from there, if you don’t want to trigger, you have to identify everything.
This process of “identifying everything” represents an enormous challenge to those experiencing PTSD symptoms, a point Evan made clearly: I don’t want to go back to therapy, because I’m afraid. Afraid of flashbacks. It’s coming back like it had happened yesterday. Why am I remembering shit like this? I don’t want to remember that!
While Evan described his cannabis use above in terms of a distraction and a context for doing things that he likes doing, others, such as Jason, acknowledged their struggles with memory while reporting that they were actively addressing them: I still don’t know what my ground zero is. There are things that I know happened that I know affected me, but I don’t remember them, because I won’t let myself. I’ve got this wall up. That’s what I’m trying to deal with right now [through my psychotherapy and cannabis use]…. Me personally, I WANT to know [where my PTSD comes from]. I want to face this. I want to address this. I don’t want to run from it. The more I hold back, the more uncertainties there could be with this.
Asked how cannabis was helping with that process, he continued: Cannabis creates a gulf between whatever I had experienced in the past and whatever I was feeling then [and my current emotional state]. I can deal with it, because I’m on the outside looking in right now. The weed, it definitely will make you think or reflect on things.
In this manner, cannabis use facilitated the introspection necessary for actively dealing with PTSD, strongly suggesting that cannabis use can be part of a classically approach-based coping strategy and not just used to alleviate symptoms or help those experiencing PTSD symptoms avoid dealing with day-to-day anxiety and depression. For Jason, this potential was elegantly summarized in his comments about how cannabis had made his psychotherapy more productive: [When I’m high], I want to get hands on. I want to engage.
The theme was taken up by Chief as well, who spoke to the therapeutic value of cannabis-related introspection: The times I used cannabis, I didn’t feel aggressive. For the most part, I was more introspective, which is actually one of the best things for dealing with PTSD. Because when you’re introspective you have uninhibited thought processes that allow you to better control your emotions and your thought processes and to communicate with other people. It’s easier to be in a social setting.
Chief’s comments here raise important questions about what might be called the secondary effects of cannabis-related coping. In his narrative, the contribution of cannabis is not limited to the immediate effects upon mood or cognition suggested by his comments about inhibition and thought processes but extend into the domain of social competency. Cannabis, he elsewhere commented, was a powerful tool for connecting with other veterans who smoke, including his Vietnam veteran uncle. When “being in a social setting” entails a form of social support seeking that is enabled by cannabis, the substance’s effects appear twofold: at once a tool for emotional regulation and a traditionally approach-based strategy for locating meaningful supports in others.
Dependence and Contraindications
Taken as a whole, the commentary provided by study participants on the topic of cannabis was overwhelmingly positive. The qualitative data set generated by this project was not without its cautionary narratives, however. For several interviewees, cannabis use in the context of PTSD was presented as a behavior that might easily be categorized as excessive and possibly involving dependence. Logic explained how her use of cannabis to mitigate anxiety had, at one point, reached excessive levels: I don’t smoke everyday like I used to. Once or twice every two weeks. It’s not as much as I used to.…When I got out, I moved back here. I was smoking every day. Crazy amounts of weed a day, because I was going through the emotions of moving from Florida.
Or as Bambi, who spoke of the immediately relaxing effects of cannabis (which she had not used prior to separation), puts it succinctly: Now, I need it. I need it to be able to keep my mind relaxed.
Mr. Afghan who spoke eloquently about the critical distance provided by cannabis and the substance’s ability to “get me away from the feeling but put me in the situation” also confided at one point in his interview: I’ll go on binges with weed, I guess because I feel down and depressed. I’m trying to get away from whatever I had experienced in the past and whatever I was feeling then.
The difference between deliberate use to confront trauma and a “binge” in his narrative is the difference, one might infer, between an active, problem-solving strategy and an avoidant, emotion-based strategy predicated upon a desire to escape or avoid traumatic intrusions and the emotionality they provoke.
While our interview data were almost devoid of discussion about contraindications or negative responses to cannabis use, a lone voice in one of the study’s focus groups warrants mention. During a lively group discussion about cannabis as a coping tool, some of which is included above, a participant, Tina, interjected: Marijuana makes me bug out.
While no further elaboration was provided, this simple statement raises important concerns about the potential for unregulated and unmonitored use of cannabis, potentially by inexperienced users, to elicit unwanted and unanticipated emotional and cognitive distress.
Discussion
One of the principal research questions orienting this study was whether attempts by veterans experiencing PTSD symptoms to self-medicate using alcohol or other (sometimes illicit) substances can be universally interpreted as forms of avoidant or escapist coping or whether the (controlled) use of particular substances for alleviation of particular PTSD symptoms can be part of a healthy and balanced coping regimen. Participants in this study described a range of beneficial effects for cannabis, including a calming/relaxing effect that aids in the prevention of intrusion events and unwanted triggers, the alleviation of anxiety and depression, and the establishment of supportive social connections to others. For most of our participants, self-medication with cannabis was preferable to the use of psychopharmaceuticals and/or alcohol, both of which were reported to have unwanted side effects that cannabis did not, ranging from loss of cognitive acuity and social withdrawal to anhedonia and decreased sex drive. We explored categorizing participants’ experiences on a classical coping spectrum extending from avoidant and likely counterproductive strategies to direct, problem-based, approach-style coping. However, the majority of participants’ uses of cannabis appeared to not fit neatly into either of these categories. Instead we posit a more prosaic category of symptomatological coping. In other words, most cannabis users in our sample described the use of cannabis to increase basic functioning and social competency or to otherwise mitigate the effects of PTSD upon their lives, an aim shared with pharmacological treatment.
The generalizability of our findings is clearly limited, given the specificity and size of the sample. However, some of our participants report powerful experiences that support a call for further systematic research into the potential use of cannabis for some veterans experiencing some symptoms of PTSD. The powerful metaphor of “a return to ground zero” offered by one participant captured a therapeutic orientation to PTSD that a number of our participants appear to share with recent exposure-based research and clinical practice (see Background). Avoiding the memories of one’s trauma, a number of participants insisted, is simply not an option. Introspection and direct engagement, they argued, are the pathway to recovery, and cannabis can speed the journey by providing cognitive focus and a critical vantage point from which to calmly assess one’s own history of trauma.
Particularly now that the VA has removed barriers to treatment for those who self-medicate PTSD symptoms with cannabis (in states with sanctioned medical cannabis initiatives), these narratives of cannabis-related self-discovery suggest an important direction for future research. Clinicians in these states would seem to possess the latitude to examine cannabis use as a potentially useful adjunct to conventional treatment. Without actually administering or in any way advocating cannabis use, these clinicians could effectively assess the potential for talk-based therapy sessions to be more productive when PTSD patients who use cannabis present for therapy (or virtual reality simulations) after self-medicating.
These participants’ accounts may also contribute to future efforts to track treatment outcomes prospectively by suggesting a tentative hypothesis that the forms of cannabis-related coping strategies involved may be critical mediators. For those whose cannabis use appears part of an ongoing effort to relive the events in which trauma originated or seek social and communicative support in peers, better outcomes may result. For those whose cannabis use appears largely an effort to “detach from painful emotion” as one of our participants stated, the short-term benefits of relaxation or stress relief may ultimately serve as a long-term obstacle to real recovery.
Similarly, ongoing research might productively assess variations in effect attributable to dosage and frequency of use. As several of our participants suggested, habitual cannabis use may diminish the substance’s usefulness or represent a crutch. Conversely, self-medicating approaches built upon a situational use of cannabis in times of perceived vulnerability to an outbreak or episode or during periods of (formal or informal) introspection could represent important techniques in a well-rounded coping repertoire.
Finally, although the theme emerged as an outlier in our study, the possibility for adverse reactions to the use of cannabis remains an important consideration, both for researchers and for service providers. While sanctioned federal studies with stringent clinical guidelines and oversight likely possess adequate tools for dealing with the classic psychotic reaction suggested by our participant’s use of the term “bugging out,” the overwhelming majority of cannabis use scenarios encountered by veterans with PTSD are likely to be unsupervised. Given the substantial barriers to empirically based information about best practices at present, the reality of the situation is that the transmission of knowledge and information about how and when to use cannabis—and for whom it is likely to be effective—is a task that veterans and nongovernmental service providers must largely undertake themselves. With the help of sympathetic clinicians and researchers, grassroots organizations might effectively generate educational resources for veterans considering using cannabis for PTSD and create peer networks that could provide inexperienced users with meaningful social supports, particularly in the event of an adverse reaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the National Institute on Alcohol Abuse and Alcoholism (R01 AA020178) and the Peter F. McManus Charitable Trust. Points of view expressed in this article do not necessarily represent the official position of the U.S. Government, the Peter F. McManus Charitable Trust, NIAAA, or NDRI.