
Abstract
This article presents results from a study of clients’ experiences of attending an opioid substitution treatment clinic in Copenhagen, Denmark. The study is part of a research project about the everyday lives of marginalized people who use drugs in Copenhagen, their risk environments, and their access to formal and informal resources. Thirty-eight clients participated in structured interviews, covering topics concerning drug use, income, housing, social relations, violence, and use of health and social services. A risk environment/enabling environment framework was developed to analyze the data. The study highlights the importance of including the drug scene that surrounds the clinic to understand the clinic as both an enabling, constraining, and risky environment affecting the clients’ everyday lives, their safety, health, and well-being. The study shows that the clinic gives the clients access to different material, social and affective resources, but that access to resources often involves different trade-offs. For the clients, such trade-offs include balancing enabling and risky aspects of interaction with other clients or accepting constraints to get access to substitution medicine. Some clients accept such trade-offs, others do not and choose to find other ways to get resources, exposing themselves to potential harm. By paying particular attention to these trade-offs, this study provides a nuanced picture of the clinic’s dual role in both being a source of stability and a place that many clients associate with feeling worried and insecure.
Many studies have shown that opioid substitution therapy (OST) is an effective harm reduction intervention and treatment for opioid dependence. But studies have also shown that the lived reality of OST can be associated with a great deal of ambivalence in the people who receive the treatment. One major reason for this is that OST can, on the one hand, give access to valuable resources to help control opioid dependence and reduce harms but, on the other hand, it can also involve submission to a regime of surveillance and control that some people experience as stigmatizing and limiting their freedom. Another reason why people may experience ambivalence about OST is that, around places providing it, drug scenes can develop, which involve a number of risks for clients, including assault, getting substitution drugs stolen, or being tempted to use illegal drugs. OST can therefore involve trade-offs between things that are experienced as positive and those experienced as negative by the people who attend the treatment, and hence they associate the treatment with feelings of ambivalence. In this article, we present a study of such trade-offs, and of feelings of ambivalence among a group of people who attend an OST clinic in Copenhagen, Denmark. By focusing on such trade-offs and ambivalence, we hope to show the importance of paying close attention to the enabling, the constraining, and the risky dimensions of OST, and the different ways in which they can be interrelated, in order to improve OST.
To study such trade-offs and ambivalence, we see places that provide OST as both “enabling-environments” and “risk-environments” (Duff, 2010; Moore & Dietze, 2005; Rhodes, 2002, 2009). The term risk-environment was introduced as a heuristic tool to show how structural factors shape the distribution of drug-related risks and how harm is a product of the reciprocal relationship between individuals and their environments. The risk-environment tool can therefore both help to focus attention on necessary macro-level structural change and local environmental change in order to reduce risks and prevent harms. The latter can be seen to involve the creation of more enabling environments for harm reduction (Moore & Dietze, 2005; Rhodes, 2002). There is currently an extensive literature within social drug research that applies the risk-environment framework (Burris et al., 2004; McNeil & Small, 2014; Rhodes et al., 2012; Strathdee et al., 2010). Less attention has been paid to enabling- environments (Duff, 2010; Duke, 2011). Duff has developed analytical tools to research enabling- and risk-environments with particular attention to how “places” can involve both enabling and harmful processes and practices. This means that places are not characterized as either risky or enabling, but that attention is paid to how different dimensions of such places can be both enabling and involve risks for different people in different ways.
We therefore use the literature on risk-environments and enabling-environments, as well as the literature about client agency and constraints, to study how an OST clinic can be both an enabling, risky, and constraining environment for clients. We present such different enabling, constraining, and risk-producing processes and practices from the perspective of clients at the clinic. We hope to contribute to the literature on OST as well as the literature on risk- and enabling-environments by showing the complex trade-offs and associated ambivalences that OST clients experience.
The case study of the OST clinic we present here originates from a larger research project that has mapped the risk- and enabling-environments for marginalized people who use drugs in three different areas of Copenhagen. Through this research, we mapped the important places in the lives of marginalized people who use drugs in each area, and this mapping showed that the OST clinics in each area were some of the most important places for the participants.
Opioid Substitution Therapy Constraints, Risks, and Resources
OST was first developed as treatment that should make it possible for opioid-dependent people to be included in society. The idea is that stabilization of the physical dependence on opioids, and the substitution of illegal opioids (drugs) with opioids (medicine) prescribed by a doctor should make it possible for people who are dependent on opioids to become included in society (Dole et al., 1966). According to this model, some people would need additional psychosocial treatment and social rehabilitation in order to socially and emotionally detach from the drug scene and be included in non-drug-related social institutions and communities. Later, OST also became a public health measure that should prevent the spread of infectious diseases such as HIV/AIDS and HCV, and reduce other risks associated with injecting drug use. In addition to this, OST has also been used as a means to reach those people who use drugs but have been hard to connect with through other social and public health initiatives. OST has proven to be an effective treatment modality, improving treatment retention and reducing illicit opioid use, drug-related HIV risk-behavior, crime, and mortality (Corsi et al., 2009; Fugelstad et al., 2007; Fullerton et al., 2014; Gibson et al., 1999; Marsch, 1998).
In addition to this, qualitative research has shown that the lived reality of OST, underlying the positive results that epidemiological research presents, is complex and involves many contradictions (Anstice et al., 2009; Bourgois, 2000; Holt, 2007; McNeil et al., 2015; Neale, 2013; Ning, 2005). Central in much of this research is how the regulatory framework, and the institutional systems that govern and implement OST, have adverse effects on the lives of people who receive treatment, particularly in regard to how they constrain clients’ freedom and agency. Such frameworks and systems are designed to make substitution drugs work as a “medicine” in the recovery of clients and not as a “poison” that results in overdoses, or as a “drug” used for experiencing euphoria (Houborg, 2012). This makes OST a treatment regime that often involves a large measure of surveillance and control. OST has therefore also been presented as a system of social control that seeks to pacify and subjugate a particular segment of the population through a combination of disciplinary power and bio-power (Bourgois, 2000; Dahl, 2006; Friedman & Alicea, 2001; Harris & McElrath, 2012; O’Byrne & Jeske Pearson, 2019). Many studies have shown how OST can create experiences of disempowerment, humiliation, anger, hopelessness, and stigmatization among clients and how it can have adverse consequences for them (Bourgois, 2000; Fraser & Valentine, 2008; Järvinen & Miller, 2010). Without ignoring such troubling dimensions of OST, other research has shown how clients can exercise agency within the constraints of the OST system (Gomart, 2002b; Holt, 2007; Ning, 2005). Studies show how clients seek to negotiate the treatment system in order to make treatment as beneficial possible for themselves. The way that clients use OST does not, therefore, necessarily comply with the institutional goals of the treatment system. They can use OST as a break from the drug scene, as a stable source of drugs, or to navigate “between street and mainstream worlds” (Ning, 2005, p. 372) etc. OST can thus give people who are dependent on opioids access to important resources, but the treatment conditions can be difficult to cope with and can diminish the value of the resources for them. For some, the conditions under which OST is provided can be so difficult or unacceptable that they cannot or will not receive treatment, but others are able to negotiate treatment to suit their own purposes. OST is a complex phenomenon that involves both enabling and constraining dimensions, sometimes simultaneously. This is summarised in Gomart’s (2002b) idea about “generous constraints.” With reference to Foucault’s conceptualization of “subjectification” as both constraining and enabling, because becoming a subject always involves subjection, Gomart investigated how the staff at a methadone clinic in France actively sought to produce constraints for clients that could mobilize activity and agency. Houborg (2006) used the same idea to research OST in Denmark and showed how some OST clients could control their dependence on drugs and maintain distance from the drug scene by becoming part of a materially heterogeneous treatment assemblage that involved both enabling and constraining processes and practices. For some clients, losing agency in some aspects meant that they could gain agency in others.
The more requirements and controls that treatment involves, the higher is the threshold for treatment. Strict requirement of abstinence from illegal drugs and a rigorous regime of urine testing and other forms of control will exclude some people who use drugs from treatment. In order to include more people in treatment, and to make the harm reduction benefits of OST available for them, demands that less strict requirements and control be put in place. This has happened in Denmark and particularly in Copenhagen, where previous OST requirements of abstinence from illegal drugs, and obligatory urine and needle mark control, have been suspended along with a requirement that clients should participate in psychosocial treatment (Houborg, 2006). The lower thresholds have meant that the distance between the drug scene and the treatment institutions has been reduced, in the sense that people and practices that were previously excluded from treatment are now allowed. It has also meant that the treatment institutions and the areas around them have become important local drug scenes, which can be problematic and risky for some clients (Fraser & Valentine, 2008). In this way, the OST clinic can become a risk-environment in its own right for some clients. Institutions that provide OST can therefore be places with many different enabling, risky, and constraining processes and practices for clients. We found it useful to use the concepts of risk-environments and enabling environments to investigate how clients experienced these different dimensions of the clinic, and the trade-offs and ambivalences involved.
The term risk-environment has been presented as a social science for harm reduction (Rhodes, 2002, 2009). It represents a more general orientation toward the social and structural determinants of harm in public health research and practice, as opposed to approaches that focus on individual behavior. The term risk-environment is used to show that risk and harm are not solely dependent on individual behavior, but are created in an interplay between the individual and the environment and the social situations where drug use takes place. In his presentation of risk-environment as a heuristic tool for harm reduction research, Rhodes (2002, 2009) distinguishes between four ideal types of intersecting environments that influence how individuals and groups are exposed to harms: the physical, the social, the economic, and the policy environment. The influence from these different environments on harm is seen to work at the micro-level and the macro-level, and through relationship and interaction between these levels. The micro-level dimensions of a risk-environment could be the social norms, values, social relations, social networks, and social controls that dominate a particular drug scene, as well as the immediate social and material setting and the nature of the area where it takes place. The macro-level dimension can be related to economic, ethnic, and gender inequalities, as well as legislation and particular policies including drug policy, public health policy, and social welfare policy.
An example could be Danish drug policy in which all possession of illicit drugs is criminalized, but in which areas around drug consumption facilities are “decriminalized” for users of such facilities (Houborg et al., 2014). This structures a city like Copenhagen into areas of criminalization (areas without drug consumption facilities) and areas of decriminalization (areas with drug consumption facilities). This means that the risk-environments for people who use drugs in these areas differ, not just in regard to access to a harm reduction service, but also in regard to criminalization and the consequences this has for drug-related harm (Maher & Dixon, 1999).
Approach
The focus on the micro- and macro-environment of harm means that research on risk-environment can help address social situations and micro-environments that create harm, e.g. through “safer environment interventions” (McNeil & Small, 2014), as well as show how wider structural and policy changes can help reduce harm (Rhodes, 2002, 2009). It therefore follows that the opposite of the risk-environment is an environment that enables harm reduction, which has also been called the “enabling environment” (Moore & Dietze, 2005; Rhodes, 2002, 2009). This term helps to focus attention on social and structural conditions that can enable harm reduction. Moore and Dietze (2005) define enabling environments as environments that may “…facilitate or provide more conducive settings for the adaption of individual change to reduce drug related harm” (Moore & Dietze, 2005, p. 276). As an illustration, they present a series of specific micro- and macro-level proposals that can create environments that are more enabling in regards to harm reduction for marginalized people who use drugs. Another example of research on enabling environments is Harris et al. (2013) study of how barriers for hospital treatment of HCV can be removed, and how the hospital environment can become more accommodating for marginalized people who use drugs. It is important not to contrast “risk” and “enabling” environments, but rather recognize that particular settings can involve both risk and enabling factors and processes (Duff, 2010), that the composition of risky and enabling factors is subject to continuous change, and that what constitutes risky and enabling factors differs for different individuals and groups. A drug consumption facility may, for example, constitute a different kind of safe environment intervention for people who smoke crack and people who inject heroin in relation to overdoses. 1 In regard to the risk of violence, a drug consumption facility may work differently as a safe environment intervention in relation to gender and age (McNeil et al., 2014).
In a series of articles, Duff presents an approach in which enabling environments are studied as “enabling places” based on theoretical resources from human geography and different versions of assemblage theory. Central to this approach is the role played by enabling resources, which are particular aspects of specific places that can come to enable action or agency that supports health and well-being. Central to the approach is a principle of “symmetry” (Latour, 1987) in which there is no a priori distinction between human and nonhuman parts of a particular setting in regard to how they can facilitate or “mediate” action. In one article, Duff (2011) uses actor network-theory, in which action is understood as the effect of particular networks or assemblages of materially heterogeneous elements, to present his approach. This means that by getting “enmeshed” in the assemblage or network of elements that make up a place, particular practices that enable harm reduction can become possible. The enabling resources that Duff describes are thus different aspects of a setting that, when combined in particular ways and when related to people in particular ways, can function as resources for health and well-being. Duff distinguishes between three classes of resources, based on how place has been conceived of as a relational phenomenon in human geography. These resources are social resources, material resources, and affective resources. Social resources are defined as processes and interactions that support the creation and maintenance of social networks (Duff, 2012, p. 1389). Duff is particularly focused on relations that involve trust and reciprocity, and frequently uses the concept “social capital.” This draws attention to an important part of how informal social networks can mediate affective as well as material resources. However, within the context of our research, we have also found that more formal relations with social workers and health professionals could be a social resource that generated both material and affective resources helping to maintain health and well-being. Material resources are defined as objects, services, benefits, and assets that can enable the maintenance and development of health and well-being (Duff, 2011, 2012). Finally, affective resources are feeling-states and associated potentials for action, generated by engagement in particular relations and particular places that could create, for example, hope and optimism (Duff, 2012).
Through the lens of these different analytical tools, OST clinics can be seen as both enabling and constraining agency, and as places that can generate both risks and enabling resources. We therefore ask about the extent to which the OST clinic constitutes a place that facilitates the production, mobilization, and circulation of different kinds of resources, risks, and constraints, and how this can lead to different contradictions and trade-offs for people who are enrolled in treatment.
Method
This study is based on 38 structured interviews conducted in October 2018 with clients (Table 1) who were enrolled in opioid substitution treatment at a Copenhagen facility. The interviews were conducted as part of a research project that studies marginalized people who use drugs in their everyday lives in three different areas of Copenhagen, in order to understand how these areas function as enabling and risk-environments for them. A total of 243 persons were interviewed in Copenhagen, of which 164 or 67% were in OST.
Characteristics of the Participants (N = 38).
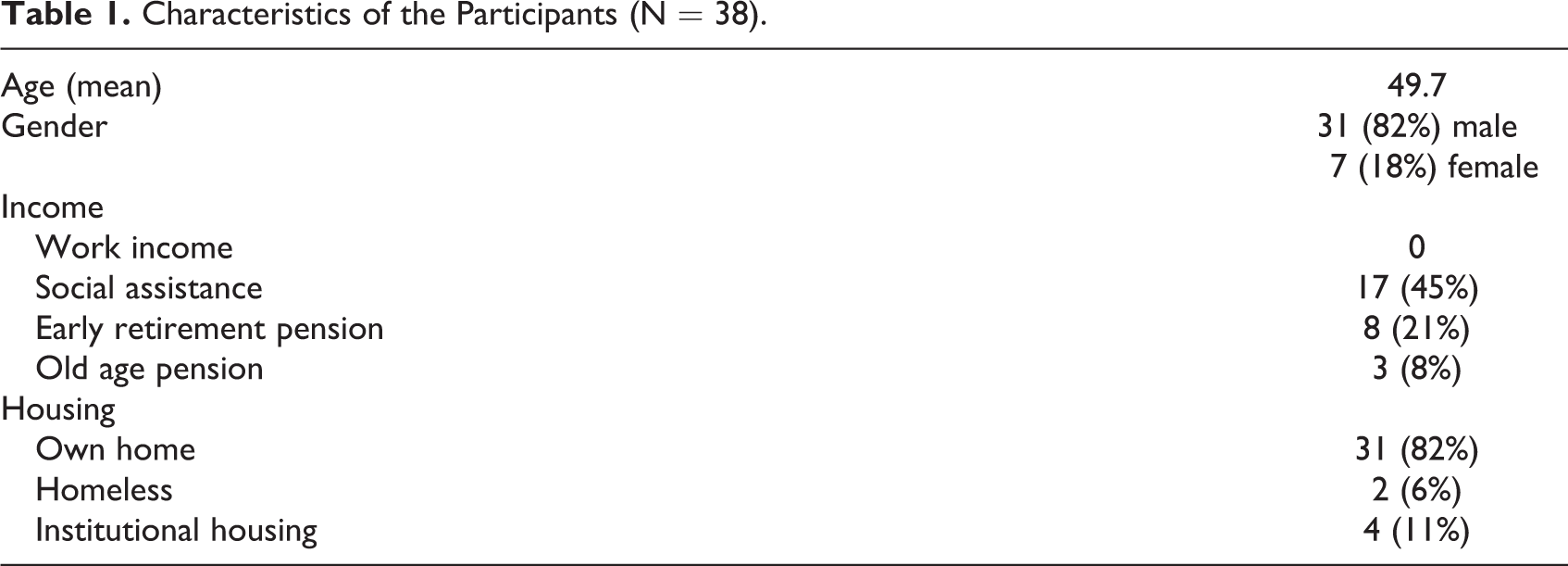
Recruitment took place at the substitution treatment facility, using convenience sampling (Etikan, 2016) by inviting people who were waiting for an appointment with the facility’s professionals, or who came to pick up their substitution medicine. The only criteria for participation were that the participants were enrolled in substitution treatment at the facility and that they understood and spoke Danish. The participants received two supermarket gift cards (valued at 200 Danish kroner) as an honorarium for their participation. Before the interviews, we ensured that the purpose of the study was explained to the participants and that their informed consent was obtained. Also, we informed them of their anonymity in the analysis and their right to withdraw from the interviews at any time. In the analysis, participants are referred to by pseudonyms. The study was approved by the Danish Data Protection Agency, and all data was stored in adherence with the Danish Data Processing Agreement.
Data collection consisted of both qualitative and quantitative data. The interviews followed both a questionnaire and a complementary semi-structured guided interview, with the purpose of elaborating on the participants’ answers and getting more in-depth qualitative data. The questionnaire consisted of 92 items and explored different aspects within the risk-environment framework, and themes connected to the everyday lives of people who use drugs. Besides socio-demographic characteristics, the questions explored health, drug use, social network, safety, violence, crime, and economy.
Interviews were conducted by two interviewers (author #1 and #2), who filled out the questionnaire based on the answers of the participants. Interviews lasted 40–90 minutes and were audio-recorded. Recordings were transcribed verbatim. The analysis of this paper is based solely on the qualitative data. The process of coding and analyzing data was inspired by the approach of Braun and Clarke (2006). Thematic analysis and coding were influenced by our analytical interest in risk and enabling environments. However, we ensured that data-driven codes were also included to explore as many nuances of the informants’ experiences as possible. The interviews were coded using NVivo version 11. We used an interactive process of ordering and grouping codes into themes. Connections between the themes were explored by making a mind-map showing the complexity and interplay between different factors in the lives of marginalized people who use drugs.
Results
For most clients, the clinic is a place that generates important material resources, most importantly substitution drugs. For some though, the way these resources are generated involves serious drawbacks and requires difficult trade-offs. For some clients, the clinic facilitates social resources, both formal and informal. For others, there are social drawbacks associated with attending the clinic; for example, being “forced” to encounter people they seek to avoid. For some clients, the clinic generates important affective resources that make clients experience a greater sense of agency. For others, encounters with the clinic and/or the drug scene around it creates negative affects that can undermine their sense of agency. In the following, we will analyze the relationships between the material, social, and affective dimensions of a methadone clinic and the drug scene that surrounds it, from the clients’ perspective. We will present how the clinic can be an enabling, constraining, and risky place for clients and how sometimes there are complex relations and trade-offs between the enabling, constraining, and risky processes that constitute the clinic.
Substitution Medicine as a Material Resource
The most important reason why clients come to the clinic is to get their substitution drugs. For many, the substitution drug serves as a crucial stabilizing resource in their lives. Without it, they would need to find other (illegal) ways to get drugs in order to avoid withdrawal symptoms. There are several different factors that influence whether and how the substitution drugs become a resource that helps them maintain health and well-being, and sometimes a number of concessions and trade-offs are involved.
As in other research on OST in Denmark, the clients in our study usually talked about substitution drugs as a medicine that helps them to stay well (Houborg, 2006; Järvinen, 2008; Järvinen & Miller, 2010; Johansen & Johansen, 2014), because they avoid withdrawal symptoms. The substitution drug was also often described as allowing the client to live a normal life without having to engage in the drug scene. One client, Oscar, who had a regular full-time job and collected his methadone once a week, compared methadone with the insulin that a person with diabetes needs. For him, this medicine had the effect that he could live what he called “a normal life” and stay away from the drug scene. The interviewer asked Oscar if methadone has given him peace, and he answered: It has, it makes it possible for me to keep my work and have a home and pay my bills and all that, like normal people do. I would never have succeeded without methadone. [Interviewer: So, you take it easier, now that you get methadone?] Yes, not having to go out and chase, not to go out and hustle and make a mess of things in order to get well. Methadone saves me. It is the best thing that the municipality of Copenhagen has ever done, that thing with the methadone. (Oscar) I think that it is OK that it [the clinic] exists. It is better than people having to steal to get heroin, right? It is a good, what do you call it, substitution for heroin, right? If it hadn’t been for methadone, I would be dead. […] Because I cannot go out and make money. I can’t steal, and I can’t all those things […] I think I will come here [to the clinic] for the rest of my life. Because it is an anchor for me to get methadone instead of smoking heroin, right? When I take methadone, I don’t smoke heroin, so it is fairly effective, right? (Bente)
For both clients quoted above and many others, the clinic is an enabling place because it generates OST as a resource that, in different ways, can work to make their lives better in terms of health and well-being, economic resources, housing, etc. as well as providing them with a sense of hope and security. But it is important to note that a vast amount of work is behind the generating and functioning of material resources (Gomart, 2002a), which can also involve different concessions and trade-offs for clients (Gomart, 2002b).
Concessions and Trade-offs Involved in Receiving Substitution Medicine
In the account of a woman who once a week has to go to the clinic to get her methadone, we get an indication of all the work that makes methadone effective as a medicine and the trade-offs that can be involved. Because of the clinic’s distance from her home and the long time it takes for her to get there, she experiences withdrawal symptoms that one day a week. I go to the clinic once a week to get my methadone. […] It is hell because I usually have withdrawal symptoms when I get there on Tuesdays. It is located in [neighborhood in Copenhagen], and I live 40 minutes away, so I get pretty sick on Tuesdays, Tuesday morning. You just want to go there and get your pills. (Ulla)
Drugs can work in different ways, depending on the circumstances under which they are used (Duff, 2017; Gomart, 2002a; Houborg, 2012; Zinberg, 1984). OST aims to make substances work as a “stabilizing medicine” and avoid it working as a poison (overdoses) and as a drug (inducing intoxication). A complex of different guidelines, procedures, and practices has been established to attempt to make it function in this way. In Copenhagen, OST is governed by municipal guidelines that implement the Danish Health Authority’s national guidelines. These guidelines define Suboxone as the first-choice treatment because it reduces the risks of overdoses and leaking into the illegal drug market. While the guidelines state that clients should be involved in deciding the type of treatment, several clients told of difficulties in getting the treatment they wanted (mostly methadone). In the example below, a client who had been treated at another clinic with methadone and heroin accepted starting treatment with Suboxone. But he quickly experienced mental health issues owing to the absence of methadone, and he wanted to resume its use. However, the doctor refused, and as a consequence, the client bought methadone on the black market, ingested it, and went back to the doctor, now with a methadone tolerant body. After that, he was treated with methadone. Then I said, “I am not going to do this [be on Suboxone]. I think I need to get back on methadone now.” “But you can’t do that, Jens” [says the doctor]. “You want to bet?” [says Jens]. And then I went out into the streets and bought it myself. I had had my Suboxone in the morning, so I waited for four hours, and then I took a large dollop of methadone, and then I was not clean anymore. And it worked like it should; it worked like it used to. (Jens) When you want it increased, you get maximum 20 mg. a day.
2
So, when I am going to increase, it takes four days to reach the dose that I want, and I don’t have time for that right now. It’s a bit annoying because then I have to buy it on the black market until I get it under control. (Lars) My friend was ill and could not get here for two days. She called up here and said she was ill and things like that. But then it happened that the day before she got sick was a bank holiday, and the day after, it was [the]weekend. So, she arrived on the Monday, which means that it had been five days since she had gotten her methadone from this place. But in the meantime, she had bought it on the black market. Then her methadone was taken away from her, just like that. And she went from getting 200 mg for twenty years, or something like that, to 30 mg [recalculated to mg, the client talks about methadone pills]. Just like that, from one day to the next. They couldn’t care less that she had extreme withdrawal symptoms and got extremely sick. […] So, they are very harsh, unreasonably harsh, you know, because they know how sick you get. (Jørgen) It is a matter of keeping on their good side, and you actively need to do that. It is not a thing that you cannot think about and just come and get your methadone and then leave. No, you actively have to be nice and quiet and not shout. Because otherwise…as I said, they hold your life in their hands. And if they have a bad day, and I have a bad day, and we clash on the stairs, then I can lose my methadone. It is up to their discretion, and that is very, very stressful and creates insecurity. […] The atmosphere here is a bit like a kindergarten, if you like, “Now you behave yourself, Jørgen,” because we all know what is going to happen if you don’t. And so, you, of course, behave. But you feel under pressure, and you feel subjected to an unexpressed threat that they can remove the carpet from underneath you if you do not behave. (Jørgen)
Mediating Health Care
The clinic is not only a place where clients can get access to OST; it also provides social drug treatment, health care, and casework in relation to social services and social benefits provided by other public authorities. The clinic, therefore, both becomes a place that provides services and care, and a place that mediates between clients and other parts of the Danish social welfare and health care system. Without receiving this care and having this mediation, some clients would most likely not get the help they need and are entitled to. In relation to health care, Danish studies (Kohl et al., 2016; Pedersen, 2018) have shown that there are structural barriers and stigmatization that prevent marginalized people from getting the health care it is their social right to receive. One client explained how he felt stigmatized when going to the hospital. When they find out that you use methadone, from that moment, you are treated differently by the nurses. Then they think that you are just “begging” for medicine (…) Even though you are not asking for it. But they are just thinking, It’s just a f---ing junkie (…) And they wouldn’t do that with ordinary people. (Jens) I have been checked from head to bottom, and I have been told that there is no HCV, that I don’t have, yeah, you know, anything, there is nothing wrong with me. I am rather amazed and happy about that because people in this environment, they often have liver problems. (Oscar)
Social Benefits and Experiences of Being Caught Up in the System
Like the health care system, the social benefits system can also be a challenge for clients. Entitlement to social benefits involves several requirements and obligations (like having no income, making yourself available for employment, etc.) and performing certain practices (like going to interviews with caseworkers at the employment center every three months). A social benefit reform enacted in 2013 means that failure to make oneself available for job offers, work training, interviews with caseworkers, etc. can either result in one’s benefits being reduced or stopped. It is possible to be exempted from some of the requirements—and avoid the negative consequences of not living up to them—for people with social problems. However, one must provide comprehensive documentation proving why one should be exempted from standard requirements. Many clients at the clinic find it difficult to live up to the requirements and engage in the expected practices to receive benefits. The possibility of accidentally not meeting their obligations means that some clients live in constant anxiety about having their benefits reduced. The client quoted below explains how he was sanctioned for not attending a municipal employment center meeting. I think…you hear, people they have to come [to the job center] every three months, as they say. But then suddenly I had to come every month. And, because I had to come every month, then one time when I get there, she [the case worker] is ill. Nobody calls me or anything. So, I rush to the job center. I forget to call, and that has happened one single time, and then I get sanctioned and get paid [only] 3000 [DKR]. That’s not even enough to pay my rent. (Mohammad) I am lucky; I can go wherever I want to because I am on pension, so I am not tied to the job center and all that. That has actually been a liberation, not to have to worry about all that. If I want to go to Aalborg tomorrow, well then, I go to Aalborg tomorrow, and I still get my money. I don’t have to discuss with them [the job center]. That is a small liberation, I have to admit. Not having to worry about it. If you get sanctioned and not getting your money. I don’t have to think about that. (Hans)
From the two quotes above, it is clear that the value of material resources when achieving economic support can promote affective resources such as feeling relief and security. Again, we see how material, social, and affective resources are interconnected and can be generated through clients’ engagement with the clinic and how this can mediate agency for them. In such situations, the clinic constitutes an enabling place. As with the health care system, clinic staff would also help clients meet their obligations and mediate between them and the social benefits system. Staff would help clients remember meetings, coach them about what to say, or go with them to meetings. A central work task for the caseworkers at the clinic is also to provide documentation about clients’ entitlement to early retirement pension, which relieves clients from the obligations attached to receiving social assistance. Frank is a client who received help from his case manager to manage his contact with the employment center: They are helpful. They help with that f---ng employment center. I have to contact them many times. That stresses you out. She [case manager] is my connection. So, we are on the same side [in the contact with the employment center]. I think it is terrible having to provide documentation all the time. (Frank)
It is not just in relation to the employment center that the clinic mediates agency for clients. It also does so in relation to other public authorities and private companies, including landlords and banks. Gaining access to, or mobilizing, these resources that increase the capacity to interact with institutions and companies is very much mediated by the way the work at the clinic is organized. Clients experience access to social workers as a limited resource and help can therefore be dependent on the quality of the relationship with the social workers. When functioning well, the clinic can be an important social resource that increases clients’ capacity to act in ways that help them improve and maintain their health.
Social Resources: A Supportive and Risky Social Network
Social relations can be an important enabling resource in relation to health, welfare, and risk minimization (Cohen, 2004; Duff, 2010), but they can similarly be associated with increased social and health-related risks (Singer, 2006). Interviews with clients at the clinic showed difficult trade-offs between social relations as protective or enabling on the one hand, and risky on the other. As many clients have been involved in drug scenes for a large part of their lives, their social network and social contacts were largely limited to people who used or had used drugs. For this reason, relations with other clients could serve as a social resource in some respects but could involve risks in other respects. Balancing such enabling and risky aspects of interaction with other clients was an important part of the narratives of most of the clients who were interviewed. In the survey that is part of the study, one-third of clients said that they spent their days with other people who use drugs, three-quarters said they knew many people who use drugs in the area, and half said that the other people who use drugs in the area knew them. But when asked about whether they had good friends whom they could trust, among the people who use drugs in the area, only one-tenth said that was true. 3 This could explain some of the ambivalence connected to social relations and mentioned by many clients.
Enabling resources through social relations with other clients can be generated in different situations. Examples of such situations mentioned by the informants involved the circulation of, and access to, material resources such as housing, money, food, clothes, “drugs” and “medicine.” It also involved helping each other with advice and guidance, such as navigating the social welfare and health care system. One client recounted how she helped other clients with advice: Perhaps you could say, if they ask, “Well, you can, for example, try to go to that place, that’s a good place.” If it was a treatment service or something like that or a caseworker or something like that [they were searching for]. Then you usually talk about what you know is good. (Lotte)
Some clients also talked about how they would protect others against threats and violence, and help each other obtain personal security in an often violent and under-policed environment. For example, this was the case with Jens, who would help other clients in the clinic area. Asked if he helped other people, his answer reveals how risky the environment was: Yes, by not screwing them over. No, I don’t, I don’t like injustice, so I will sometimes help if someone is very obtrusive towards someone else who has a lower status. It could be someone who is getting rolled [robbed] for his medicine by someone he is afraid of down here [outside the entrance to the clinic]. (Jens) I am also being offered drugs here, and I don’t like that (…) Right down here by the entrance. That is why I don’t like coming here. It was better when I was at my general practitioner. Back there, I didn’t have any problems with [side] drug abuse or anything. It may have happened very rarely. It’s gotten worse after I started coming here.” (Gert)
Besides mutual help and support among clients, the interviews demonstrate that relations between clients are also characterized by mistrust, fear, and risk of increasing or resuming problematic use of drugs. Thus, the social context of the clinic and the drug scene around it, also forms a risk environment where it is difficult to avoid meeting other people who use drugs, as this is almost inevitably a part of being enrolled in treatment at the facility. Consequently, the treatment facility environment is formed not only by its enabling resources but also by its risk-inducing processes (Duff, 2010), which for many clients generates ambivalent feelings about it.
Trade-offs Between Social Isolation and Risking Relapse
Many clients found that the only way to avoid the risk of relapse associated with meeting other clients was to isolate themselves from them. In discussing why he doesn’t interact with other clients at the clinic, one client explained: People who use drugs are not welcome at my place. Because…I don’t want to see them. Then I know what will happen; I will slip/fall [back into taking drugs]. And that is over. I am determined to stop that shit. (Fred)
When asked if he gets help from other people who use drugs, the client Hamza explained how he seeks to keep to himself: Nobody, I do not get any help from drug users. I try to get away from drug users, so I don’t hang around with them. I keep to myself most of the time. [Interviewer: “What about people who do not use drugs?”] I don’t have any contact with them either. I kind of live in an alone-world. (Hamza) I do actually feel well. But since I’m home alone a lot, it is also very depressing. I have also asked for help for this…To get out and meet with other people. (Hans)
The lack of meaningful activities can, in addition to loneliness, challenge stability. When asked about the three places they spend most of their time, almost all clients explained that they stay at home where they watch TV, play PlayStation, smoke cannabis, or sleep. Bolette is one client who explained how the lack of activity and social interaction undermines her sense of agency: I have become really lazy lately, unfortunately. I have to put that behind me soon before the home gets too lazy. I don’t feel like having visitors anymore (…). I just sit at home and watch television. Yeah, when I feel bad. (Bolette) If you don’t have anything to do, you have your pension, but you don’t do anything; then you slip back into the drugs—a lot of times! Unless you are strong, really strong, you need to be. Then you can stay away from the drugs. If you have something to do, if you have friends who are not drug users, people who are normal, that you can talk to and do things, right? Go out fishing, play football, gymnastics, whatever. Something has to happen. To stay at home doesn’t work. That’s my experience. (Frede)
Conclusion
In this article, we have asked about the extent to which a specific OST clinic constitutes a place that can be enabling, constraining, and risky in relation to its clients’ health and well-being. When investigating this question, we have not only focused on the formal services that the clinic provides, and how clients and staff interact. We have also included an exploration of how the clinic is a place that mediates relations between a group of people who use drugs, and we have included these relations in our understanding of the clinic, not just as a service, but as an important place in its clients’ lives and that affects their health and well-being. Theoretically, we took our point of departure from the literature about risk-environments and enabling environments to understand how an OST clinic, in complex ways, for better and worse, can affect the lives of its clients and their ability to maintain health and well-being. Our analysis explored material, social, and affective resources, which are all interconnected. Our approach led us to take a wider view of the clinic as a place that does not solely facilitate treatment but also constitutes a source of enabling processes when resources are generated or mobilized and circulated, concurrent with risks affecting the general situation of clients. Some of our results confirm results from other research that show the ambivalence that many clients experience when receiving medical drug treatment, because they both depend on the substitution medicine to “stay well” and must subject themselves to rules and regulations. For some clients, these are experienced as “generous constraints”; others experience them as less generous and as disempowering, humiliating, and a plain nuisance. Regardless, for many clients, dealing with rules and restrictions at the clinic becomes one of many trade-offs involved in accessing OST. We paid particular attention to these trade-offs to provide a nuanced picture of the clinic’s dual role in both being a source of stability and a place that many clients associated with negative affects. We saw that the clinic could also help clients realize their status of social citizenship by helping them manage their relations with other parts of the Danish welfare system, most notably the health care system and the social benefit/employment system. In this way, we have presented a more nuanced picture of how an OST clinic can be both enabling and constraining for its clients and their ability to maintain their health and well-being. Our research has also indicated how difficult it is for marginalized people who use drugs to interact with the modern Danish welfare system and how dependent some of them are on help and guidance from other people, mainly clinic staff. The staff can help mediate the agency that welfare and health care institutions require of individuals in order to realize social citizenship in practice. This highlights one of the important structural barriers for many marginalized people in the modern Danish welfare state. Even though it provides many services and benefits as a social right, it requires that citizens have the abilities and the possibilities to realize these rights; a requirement that is increasingly difficult for some to meet.
We have also shown the importance of including the social milieu that develops among clients at the clinic in our understanding of the clinic as constituting an enabling, constraining, and risky environment. Social relations among clients can help them manage their everyday lives by giving them access to material, social, and affective resources. However, the drug scene that developed around the clinic also makes it a risky place for some clients. They risk being threatened and robbed by other clients, or they can become tempted to use illicit drugs, even if they have decided to stop or minimize their use. Many clients experienced worry, stress, and insecurity when faced with other users of the facility, due to being exposed to drug trade, threats, and violence in the immediate area. We have shown that, to cope with these perceived risks, clients are likely to withdraw from the drug scene around the clinic, which leads to social isolation. Hence, we have shown that choosing between social isolation and loneliness, on the one hand, and exposing yourself to the temptation of using illicit drugs on the other, is yet another trade-off involved in accessing OST and is a dilemma that many clients have to deal with. One of the serious challenges inherent in the different goals that OST can have (harm reduction and social inclusion) is that to provide harm reduction for as many people who use drugs as possible, there needs to be a tolerance toward clients who continue to use illicit drugs and be an active part of the drug scene. On the other hand, this can make the clinic a central hub in a drug scene, which is not helpful for clients who want to leave the drug scene behind.
To understand the experience of being an OST client and improve the conditions for OST clients, it is important not just to focus on medical treatment but to have a holistic understanding of the mobilization, generation, and distribution of resources at the clinic. It is important to include both formal and informal relations that affect the resources that can become available at the clinic, and to emphasize when and how the resources generate value for clients. For practice, our findings implicate that a shift in focus, from simply making OST and related services available at the clinic, to understanding when these services create value for the individual client, could prevent some of the unintentional effects of being enrolled in OST as shown in this analysis. Such a shift involves paying detailed attention to all the different trade-offs that different types of clients have to deal with when they receive OST, both when it comes to interacting with the clinic’s staff, its guidelines and regulations, as well as other clients they encounter at the clinic. At a policy level, such a shift would require a closer emphasis on client involvement in revising treatment guidelines to better take into account their individual perception of the guidelines and the barriers that hamper their value of OST and the services it mediates. In practice, this could be implemented at an organizational level at the OST clinics by establishing local councils in which clients could participate. This might contribute even more to creating an enabling environment with meaningful practices for clients. Going forward, it is important to emphasize the OST clinics as environments which have significant influence on clients’ treatment, health, overall well-being, and everyday lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Velux Fonden.