
Abstract
In Washington State, the dynamic drug policy around fentanyl has not only transformed policing but also the ways people who use drugs make sense of their own practices. Drawing on in-depth interviews with 20 people who use both opioids and methamphetamine, this article shows how legislative changes associated with the changing “moral panic” from methamphetamine to fentanyl have affected how people conceptualize the health and legal risks associated with each substance. We build on Garriott's concept of narcopolitics (the social regulation of behavior through drug policy) to show that policing plays a constitutive role in shaping how people who use drugs assess risk and experience addiction. Participants consistently associated opioids, especially fentanyl, with criminal activity, community danger, and heightened health risks, even when methamphetamine was also involved. Methamphetamine, by contrast, was frequently described as less dangerous, more functional, and even beneficial for productivity or safety. These distinctions were not reducible to intrinsic properties of the substances themselves, but mirrored policing priorities and widespread public health messaging. In this way, policing imparted moral valuations, risks, and use patterns onto individual substances, reshaping how participants interpreted their own experiences. We argue that narcopolitics offers a critical framework for understanding polysubstance use as a socially mediated practice contingent upon larger social and political structures. Policing does not just respond to, but helps actively construct, legal and health risks. In a political climate marked by dynamic drug policy and volatile politics, this study demonstrates how these shifts reflexively transform the lived realities of polysubstance use. These findings underscore the need for policy and treatment approaches that recognize the unequal regulation of different substances and its implications for harm reduction and care.
Introduction
Over the last 3 years, Washington State has moved from decriminalizing drug possession to reinstating criminal penalties and escalating arrests. In 2021, the Washington Supreme Court struck down the state's felony drug possession law (State v. Blake, 2021), following similar trends in decriminalization and a greater focus on treatment in places like Oregon (Russoniello et al., 2023). The legislature then passed a stopgap measure that reclassified drug possession as a misdemeanor requiring at least two diversion attempts before arrest. When the 2021 law expired in 2023, politicians pushed for tougher penalties, passing another law increasing possession to a gross misdemeanor and removing the diversion requirement. The Seattle City Council also passed a citywide ordinance mirroring the state law with a specific focus on public drug use (Collins, 2023). Voter polls showed that despite supporting treatment-first models, many people linked substance use to street crime and showed a preference for increased police presence (Esteban, 2023).
These shifts have unfolded against the backdrop of not only the introduction of fentanyl into unregulated drug markets but also a rise in the combined use of opioids and methamphetamine (co-use). Co-use has been increasing not only in Washington State (Glick et al., 2021) but throughout the United States (Jones et al., 2020). Fentanyl poses an acute, immediate threat of respiratory depression and fatal overdose, while methamphetamine is associated with long-term cardiovascular effects and neurotoxicity. Compared to opioid use alone, co-use is associated with higher morbidity (Shearer et al., 2020), hospital utilization, housing instability, and legal system involvement (Howell et al., 2021). Co-use is also associated with a higher likelihood of non-fatal (Al-Tayyib et al., 2017; Hoots et al., 2020) and fatal overdose (Jones et al., 2022), constituting a “fourth wave”—following heroin, prescription opioids, and fentanyl—in the overdose crisis in the United States (Ciccarone, 2021). Medical management of co-use is also challenging. People who co-use have lower utilization rates of medications for opioid use disorder (MOUD) (Frost et al., 2021), which is not only the standard of care for opioid use disorder (OUD), but has also been shown to correlate with decreased methamphetamine use over time among people who co-use (Tsui et al., 2020). The turn to criminalization presents further harms to people in general, and particularly for those who use drugs. Incarceration in the United States is independently associated with a variety of poor health and economic outcomes (Binswanger et al., 2011; Schnittker & John, 2007; Wildeman & Wang, 2017), including an increased risk of drug overdose death (Binswanger et al., 2013; O’Connor et al., 2022).
Many of the legislative changes in Washington were modeled after earlier methamphetamine laws that sought to “protect children from fentanyl exposure” by criminalizing public drug use. Although convictions remained challenging, the 2023 state law resulted in an increase in drug possession arrests in Washington (Wilson, 2024), which were disproportionately for fentanyl. Fentanyl seizure cases in Washington have also increased drastically, while methamphetamine cases have remained stable (Washington State Drug Trends, n.d.). Despite this focus on fentanyl, methamphetamine use remains more common in Washington State (Kingston et al., 2024).
The impacts of these legislative changes on use practices and perceived risks are important to understand, considering how larger shifts in the U.S. drug policy landscape are changing in response to shifting substance use patterns and a dynamic political environment. Yet little is known about how people who co-use experience and react to these changes and how they conceptualize the legal and health consequences associated with different substances. This understanding is crucial because drug risks are not experienced solely as pharmacological outcomes but are shaped through social, institutional, and political processes. Critical drug studies scholars have argued that drug effects emerge relationally through interactions among substances, bodies, environments, and governance regimes rather than from intrinsic properties alone (Duff, 2013; Fraser & Moore, 2011). Policing, public health messaging, and spatial regulation can therefore influence how harms are recognized, attributed, and acted upon. Fitzgerald (2015), for example, demonstrates how enforcement practices and urban governance render particular forms of drug use visible and actionable, shaping both policy responses and lived experiences. Such work suggests that shifts in policing priorities may reorganize not only material risks such as arrest or incarceration but also the interpretive frameworks through which people who use drugs understand their own behaviors.
The current fentanyl crisis and the dynamic public policy milieu in Washington State, therefore, create a unique opportunity to understand how policing and public policy influence how people who co-use understand polysubstance use. To analyze the social and political work that drug policing and criminalization policy does and how it affects the experiences of people who co-use, we apply William Garriott's (2011) concept of “narcopolitics.” Building on Michel Foucault's theory of biopolitics, which describes how health and behavior are regulated through norms, discourse, and institutional practices or “techniques of governance” (Foucault, 2008), narcopolitics refers to how drug policing (as one such technique) produces and enforces social, political, and moral order. In Garriott's (2011) study of rural West Virginia, narcopolitics operated through local law enforcement to frame methamphetamine use not only as a public safety issue but also as a symbolic expression of broader social decline. Providing punishment and the possibility of rehabilitation, policing became a rational tool for managing a public health crisis. In so doing, it changed how people viewed themselves and led them to adopt narratives of personal and social responsibility.
Prior research has shown that institutional encounters, culture, everyday practices, and legal intervention can reshape drug use by structuring experiences and intercalating subjects into systems of governance (Duff, 2016; Seear, 2020). We extend this insight by examining how selective enforcement may contribute to the social production of risk hierarchies across substances. Analyzing our participants’ experiences using this framework allows us to draw important conclusions about how the changing policy landscape affects the way legal and health risks are conceptualized and narrativized. We therefore seek to elaborate on the effect drug policy and policing have on creating different schemas for different substances that affect behaviors around—and experiences of—substance use. This perspective advances theoretical understandings of polysubstance use, reinforcing how it is a socially mediated practice in which the meaning and effects of each drug emerge through shifting public health discourses, criminalization, drug policy, and lived experience.
Methods
Study Sample
We recruited 20 hospitalized participants initiating treatment for opioid use disorder who also reported methamphetamine use in the last 30 days from a parent study testing an adherence intervention for buprenorphine (Bhatraju et al., 2025). The parent study recruited from a large hospital in Seattle, Washington, which serves patients in King County and the larger Pacific Northwest region as a level 1 trauma center. The current study enrolled patients from the parent study who reported interactions with the criminal legal system within the last year, defined broadly as incarceration in a prison or jail, probation or parole, interactions with law enforcement, or involvement in a court-mandated drug treatment program with the stated purpose of conducting interviews to hear their experiences with the legal system and how it has related to their substance use and treatment. Exclusion criteria of the parent study included current incarceration, being non-English speaking, discharge to a setting that would impact the ability to use the adherence tool, acute or chronic cognitive impairment impeding the ability to provide informed consent, and behavioral issues that could put research staff at risk.
Data Collection and Analysis
Two members of the research team (NI and LE) conducted in-depth, semi-structured interviews with participants from January to November 2024. Participants were invited to share any experiences they had with the criminal legal system, using our above definition that were most significant to them. These open-ended responses served as a starting point and guided most of the interview. Follow-up questions were asked to explore other interactions with the legal system, understandings of the relationship between legal involvement and co-use or individual substances, experiences with treatment services, and ideas about how these systems could be improved. We used an interview guide to prompt further discussion of specific topics, including how opioid and methamphetamine use each specifically contributed to legal involvement, perceptions of the legal system, what their visions for the future were, and any barriers they identified to achieving success. Participants were compensated $50 for their time. Fieldnotes were taken directly following the interviews, documenting initial perceptions, context, and observations. Demographic data were collected for all participants.
Interviews were recorded, transcribed, and coded in MAXQDA (VERBI Software, 1985). After a close reading of the initial interview transcripts, they were coded using both inductive and deductive codes (Green & Thorogood, 2004), which were regularly reviewed with the rest of the research team.
Analytical Methods
The data and codes were iteratively queried based on the study aims as well as trends, surprises, and interests that were sparked from the narratives using a grounded theory (Charmaz & Mitchell, 2001) approach to generate themes and explore connections in the data. Findings were reviewed with clinicians and researchers familiar with local drug laws, policing policies, substance use patterns, and treatment services. We situated participants’ narratives in this larger social context and used this knowledge to triangulate the data, affording a more comprehensive understanding of their experiences and how they related to existing policy (Bernard, 2018). Frequent, collaborative data analysis with research team members and outside experts allowed us to cross-check our interpretations and explain data that deviated from common themes (Morse, 2015).
Findings
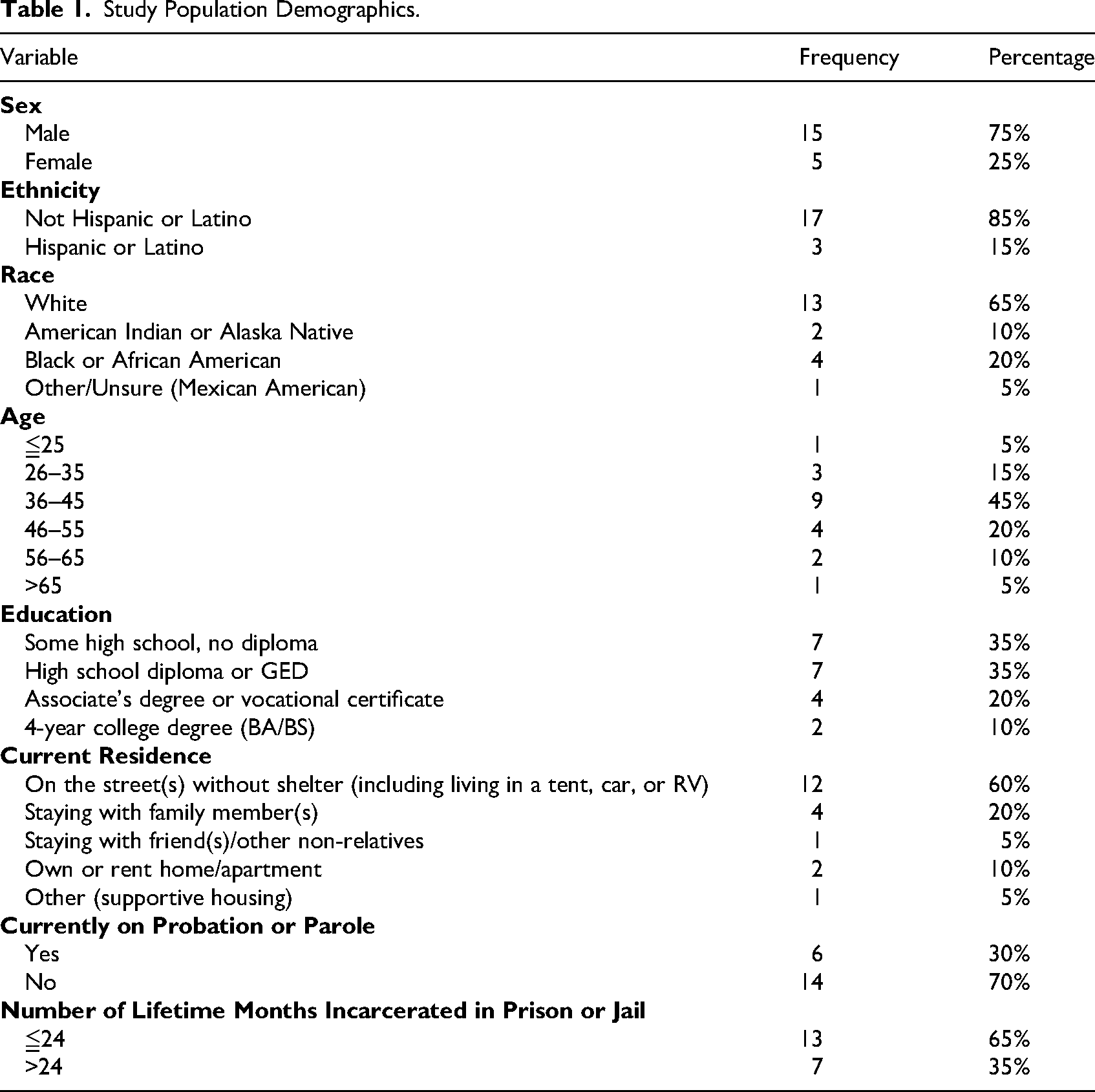
Demographic characteristics of the study participants are presented in Table 1. All names used in the following sections are pseudonyms.
Study Population Demographics.
Policing Fentanyl as Public Health Policy
Several of our participants mentioned the recent changes in drug possession laws, describing a “free for all” that resulted from the legislation during 2021–2023: “And so they say they're not taking in any, we're not arresting anybody doing [opioids] right now. And so once the word got out about that, it kind of was like, you know, free for all” (Danielle). Fred described how there was a lax attitude around opioid use in public discourse during the same time: “You know, at [that] time we got, you know, signs in Seattle saying heroin is good, you know? Weird.” More recently, however, along with the 2023 legislative changes making possession a gross misdemeanor, participants described messaging around fentanyl as a public health crisis, even in local jails: “It says it everywhere in [jail] too. Like fentanyl poisoning is a big thing in [county jail] systems, like plastered all over the wall” (Silas).
This recent messaging also coincided with an increase in policing fentanyl use. Some people referenced the 2023 legislation directly as the cause for this increased policing, while others saw it as a response to a larger public health crisis. Eric described the policy changes as a political response to fentanyl's introduction into the drug market: “Everything seemed to have its own little wave, you know, even this fentanyl shit they came out with now. […] That's because the chief of police was downtown kissing babies, saying, ‘I'm going to get these drugs off the streets’. And then came the sweeps.” Others felt it was reactive to the previous “free for all”: “I got arrested because they were doing crackdowns on the corner. One minute they’re too lenient on the next minute they're cracking down” (Eric). “But then when the law changed to go back to, back to it being illegal, like I would see cops just like, looking, just trying to seek out something to arrest somebody” (Roxanne). Others felt it was a rational response to how severe the fentanyl crisis had become and echoed political messaging around “cleaning up the streets” and the desire to shield others in the community (especially children) from public use: “They want to live in a world that's clean and pure and not so, rambunctious and have, like, a bunch of hellions. […] They're just now cracking down here. Like, I think it's because they're doing drugs and shit in front of businesses and in front of children” (Ethan). Danielle referenced this logic while internalizing it further into a sense of obligation: “So they put the fear in me to not do it publicly, which is their main thing. And I understand that because kids don't need to see that. You know, families that are just going out to do grocery shopping and stuff like that, they don't really see that. I totally get that. So I need, I needed to be aware of that and not disrespect my community” (Daneille).
While still referencing the rationale of hiding their use from the public, Tyler described how legal approaches did not achieve this goal and the ambivalence he felt around this policing strategy: “So in [town] now because of the fentanyl crisis, the mayor of the town has ordered the police to basically get back on the beat. And so they do these they do these large sweeps daily […] But, I think the bad thing about the sweeps is, you know, you push everybody out of the alleys, and now it's just like, well, you got nowhere to hide. You might as well just do it right here, you know? So, they're not going to make any difference. And so I don't think it's good for kids and you know, when other people see people doing that kind of stuff, I think it's … You know, it's a good thing and it's a bad thing.”
Notably, the way these policing strategies were described reiterated the legislative rationale of shielding the public from substance use and, in the process, shifted blame for harm to individuals rather than offering them help. Ethan captured this sentiment bluntly. He pointed out how the focus he mentioned above for eliminating public use in front of businesses or children enabled law enforcement to disregard harm—even death—caused by their substance use: “And, that's why they're just like, if you hurt yourself or do drugs, they're like, whatever. Let them kill himself. Yeah. So I think that's why law enforcement looks at it like that now” (Ethan). Though some people referenced referrals to treatment directly from the police as part of the 2021 law, none of our participants had direct experiences with this. Danielle did describe how the police took her to a local emergency room to get medical attention for leg wounds, where she received resources: “So they talked amongst each other and came back and were like, ‘We're going to take you to the hospital instead’. So then they took me to the hospital, and they released me there to be seen by the emergency room. And that's where I stayed.” Tyler highlighted the ongoing challenges with following arrests up with prosecutions while also referencing his lack of experience with treatment referrals: “Like they caught me smoking fentanyl in an alley, arrested me and then released me. And I asked him like, hey, what's the what's the punishment for something like this, you know? And they said, oh, probably nothing. Which I thought was weird because up until recently they just refer people to treatment, you know, and offer them a business card with a treatment program or something. I don't know, I never have had it happen.”
Methamphetamine was described as less addictive and dangerous, both compared to fentanyl and to the methamphetamine of the 2010s, making it less of a public health, public safety, and political concern. Roxanne described this phenomenon in detail: “The name of the game right now, like any time the cops have any interaction with anybody, it's going to be for fentanyl. But methamphetamine is going to be secondary. Usually by then they just don't even care because they're working to get the fentanyl off the streets. And so it's like I've never been arrested for methamphetamine use. Matter of fact, my ex, because he smokes meth and the cops had pulled him over several times and saw a meth pipe in his car and did not arrest him. They really don't care because it's one of those things. It's like, yeah, you know, meth has never killed anybody. You know, fentanyl is killing everybody.” She continued, emphasizing the difference she and others saw between methamphetamine now and in the 2010s: “And so if the dope now [were] like that, then I think the cops would give a shit because that kind of dope was causing an increase in criminal behavior for people to be able to fund their needs, to get higher, to continue to get high, because it was so addictive back then. […] Because they locked down ephedrine, and, you know, it's really hard to get enough ephedrine that you need to make it right. So, yeah, like, if this stuff was like that, then, yeah, the cops would be all over people. But now, anymore, it's like the name of the game is going to be fentanyl […] When you talk to them and you talk to anybody in the community, when you talk to, officers of the law, and you ask them what it is that they're looking for, they're going to tell you it's fentanyl. […] fentanyl is the name of the game.” Danielle offered a similar take: “There's less methamphetamine on the streets. less interaction, less police calls about that, and less worry. And now it's all the focus is on fentanyl, especially with the overdosing and stuff. So I feel like they'll just, if you're using meth, they don't quite as much care. If you're using opioids, smoking them and shooting up, you're definitely going to jail, you know?”
Policing fentanyl was seen to fulfil a public health role by discouraging public use through fear and by “setting an example”: “They like to make an example of you, especially when other people are around, make a scene so that it's known that we’re doing opioids. […] So I guess that they hope that other people don't do the same thing. But it would just be funny. Like, I felt like the difference in drugs, even when I did heroin, was different. Because they weren't as strict. And didn't want to, like, I don't know what the word is, but they're just, like, taunting you. Like, they know what you're doing. And so then they'll just make fun of it and make you feel bad and make you embarrassed” (Danielle). One of our participants, Buzz, even described this in terms of control: “They're still looking for a way to clean up the streets, but they just don't know how to do it. They threw so much money at it. You know what I'm saying, different options just to sort of still not get it, but I think it's drugs first. If you can control the drug, you can control the people better.” Fred similarly mentioned how police confiscating drugs may be in the “best interest” of the person: “If they do, it might be in your best interest, because I've had that happen. They're like, oh we're going to [take] these morphine pills or whatever.”
Differential Policing Helps Construct Hierarchies of Risk and Harm
Some participants discussed how their arrests and involvement with the legals system were linked to possession or public use, specifically of fentanyl, around the changing legislation. However, several people also associated other charges with their opioid use rather than methamphetamine. The other charges that came up most often in our interviews were DUI, parole violations, theft, trespassing, and domestic violence. After he had discussed charges of trespassing and theft to obtain money to buy drugs, a young man named Glen stated simply, “Fentanyl was the one that got me to doing all that type of stuff” adding, “I used meth when it was there. It was not something that I went to look for.”
People attributed legal involvement to opioids even when they were using both opioids and methamphetamine at the time. Amy, a young woman who was incarcerated after breaking into a house to steal money for opioids, relayed the negative associations she had with opioids and how they led her and her ex-partner to lose their jobs and start pawning stolen goods to make money: “So, we both ended up losing our jobs. Started pawning things, to pay our rent and to fulfill our habit, pawning our own things, and we ended up losing our place to live. […] So we started, I mean, crime kind of fell into that. It started with, just like, breaking into cars and, like, little storage sheds and getting people's tools and things.” After being arrested for selling stolen goods, she went through withdrawal and was still actively withdrawing when she was released and broke into a house. Even though she disclosed later in the interview that she had used methamphetamine that evening, she related the activity that led to her arrest to a desire to avoid withdrawal: “So I had done a shot of meth […] and I was walking by this house. All the lights were on, it looked like nobody was home. I walked up onto the porch and there was like a dog and a cat inside. I knocked on the door. Nobody came to the door and I tried it, and it opened. So I went, I went upstairs. […] And, yeah, all I could think about was being sick, that I was going, like, not the being incarcerated part, not that I did something wrong, but I just the fear of being sick and being jailed.” She continued to associate opioids with things that had gone poorly in her life and set a boundary on future relationships with people who used opioids: “But opiates is where I draw the line. Like, I will not be with somebody who does opiates. Because it had ruined my life and like, you know, it had taken my marriage from me and like, sent us both to prison and taken everything we had worked so hard for. And that was the one thing that really stuck in my mind. And it was very specific. It was like opiates did that.”
Silas, a young man who was arrested for a DUI, related his DUI to methadone, saying, “I guess I got too messed up on methadone.” He had just dosed at his methadone clinic and was involved in a car crash on his way home. Later in the interview, just prior to discussing his methamphetamine use, he relayed that “I had other stuff in my system, but the last place I was at was at the methadone clinic, and I fell asleep driving and just … Yeah, methadone's strong stuff […] stronger than heroin, I'm pretty sure. […] And you call it liquid handcuffs because it's just like being on … It's like being on dope still.” Despite recognizing some of the negative health effects of methamphetamine (specifically in his mother's use), he saw his use as incidental and did not relate it to his DUI despite having used that evening: “And the last time I was got pulled over by law enforcement, like my first DUI. I smoked some [meth] by accident. And that's where I was kind of getting that, the anxiety, I think. And my mom, she had a stroke from overdosing on the crap. And yeah, I really try not to do it, but I end up doing it once in a while because it's just how it is, I guess, being part of the game, you know.”
When participants related opioids to their criminal charges or legal involvement, they did so in various ways: how it was “strong” and altered their judgment, how their cravings or withdrawal would drive them to do illegal things to pay for drugs, or even how an original drug charge would lead to more illegal activity to satisfy conditions of parole. Zac stated, “Me and my partner might have to go borrow and be creative and borrow stuff from corporate stores to subside our addiction and for fuel and to get to all those appointments and to make [parole] and all that kind of stuff. So sometimes it's like you almost have to steal more to do the stuff they want you to do, or do whatever you have to, however you get your money.” Roxanne commented, “Like, people fund their drug use however they need to, be it like stealing things from retail stores and reselling it, or prostitution or stealing or, you know, just like many, many, many ways and at the end of the day.” Alexis reaffirmed this and described her impression of the relationship between crime and opioids: “When I find out that they do heroin or those blues, because most people, that's what they got to do is thieve and lie to be able to maintain that habit.”
Several people also meant that increased policing was neither a deterrent to use nor to crime they associated with addiction, even if it did make them more cautious. Tyler said, “The nature of, like, fentanyl is that they're going to keep using it. They don't really have a choice. It's a gripping addiction. They're going to do whatever they have to do or whatever they can do. To make sure that they stay okay.” Zac reiterated, “It almost didn't matter anymore if I was going to be. It's either going to get caught by the cops or the security guard in the store, out of the store, but at least you're giving it a shot to, to get the money to get the drug.” Participants did not make direct connections to their legal involvement and methamphetamine use. Tyler commented that methamphetamine “kept me from being the best me, so to speak” and called it a “lame excuse for poor behavior,” specifically when discussing his domestic violence charges. Others had similar responses when discussing assault or public disturbances. Another one of our participants, Mark, mentioned that he was caught by police and arrested for manufacturing and distributing methamphetamine. He blamed his getting caught partially on the fact that he was also using: “You get so spun out, you think you’re doing the right thing and you’re just going around the mountain,” but blamed substance use more generally on crimes he had committed: “And yeah, drugs had a major effect on all that.”
Some other participants acknowledged, like Silas above, that methamphetamine use heightened anxiety around encounters with law enforcement or made them targets for police interactions that would rarely result in arrest. Ethan remarked, “I've been like high like on meth and like talking to the officers and I'm like, this is my worst nightmare. […] They see me tweaking and then I'm like, talking to one like, oh my God, I don't want to be talking to this guy, he so knows I'm fucked up, but he's sitting there making jokes about it.” Gabby acknowledged being high on methamphetamine could make her more vulnerable to arrest, but that she felt more confident in those encounters and could even help her avoid arrest: “Oh, yeah. I'm probably a little more lippy, honestly. Like, [I] have a little more confidence when I'm high because I'm like, I know my rights.” When asked if one drug had more of an effect on legal involvement than another, Buzz said, “Like when somebody's on methamphetamines, it's more alert. You know what I'm saying like, he's just kind of stand, standoffish.”
Patterns of Co-Use
Methamphetamine was described as less dangerous compared to fentanyl and other opioids when people spoke about perceived risks and patterns of use. Conrad mentioned this, also referencing changing substance use trends and the relative safety of private use: “Now they have this monster crawling around called fentanyl. […] Heroin and the crack or cocaine was a monster. There's nothing ever crawled around this world like fentanyl is crawling around.” He went on to convey the relative risk of methamphetamine and fentanyl specifically, saying, “I think I think it's better for people to smoke meth than it is to smoke fentanyl […] I don't think there's a safe way to do that monster, that fentanyl. But you know, the opiates and you know, methamphetamines, you know, I guess they figure it's a safe way to do it at your home.”
Fentanyl was seen by some as more dangerous, specifically due to risk of overdose, especially after periods of abstinence: “Because I know a lot of people the only way out with fentanyl is either dying or, you know, choosing to get better. And that's really hard to do. I know so many people have died from that crap, and it's and it's usually when they're out of just get out of treatment and they go back and relapse and then they just drop dead from the crap because their bodies aren't used to it” (Silas). “I had tried a couple blues here and there, but I wasn't really into it. I never really got too hard on fentanyl. I was like into blues because fentanyl kind of scared me. It was like a lot of my friends were dying and stuff” (Danielle). Gabby also mentioned this in comparison to methamphetamine, referencing the control it had over her: “I don't like downers. I don't want something to have that much control over me and like, be out of it. Like, that doesn't sound fun. […] When I started smoking meth, I could kind of like, pretend like I had, like, this shield, you know, to protect me.”
With methamphetamine, participants described using to maintain productivity. Mark mentioned using to enhance his selling: “I used it more of like a … what do you call it when you're an athlete and … performance enhancing? You know, that's how I would use it. You know, I wasn't really like abusing it, but I mean, you're abusing it, you know. Of course. But yeah, I thought, oh it's okay. I'm only getting, you know, use it for the game.” Roxanne also described how it was beneficial to her, drawing a distinction between her experience and someone committing a crime: “When I started smoking amphetamines […] I wasn’t staying up all night. Like I could sleep on it and eat on it and, like, go to sleep and wake up. And it kind of became like a, like my morning coffee or like my afternoon cigarette type of thing. […] I wasn't staying up all night, geeked out and like, trippin and like, robbing houses or stealing copper. You know what I mean? […] Like it became something that was kind of helping me, like, focus a little bit better than what I was before.”
Similar to Roxanne's comment that methamphetamine helped her focus, other participants also mentioned methamphetamine's benefits for self-medicating attention or mood disorders. “When I was out there, I was self-medicating because, you know, if you use meth, you don't sleep, there's no nightmares. You, you begin to feel anxiety or something like that and, use heroin because that wraps up a nice warm blanket and tucks you in” (Leo). “Methamphetamine calms me down and I don't get jacked up like I used to” (Zac). They also described the benefits of stimulants to maintain vigilance against the threats of living on the street: “I wanted to stay awake and, like, know everything. I was like, if I fall asleep, somebody. Like I became super paranoid, but super uncomfortable and scared that somebody was going to hurt my family. So I was like, I'm just going to stay up forever” (Gabby). An older man named Walter also described needing to stay up after another person in his encampment attacked him: “The meth was to get up, to be up. And especially after [the attack], you know? I was afraid to go to sleep like I am now. But before this, I was afraid to go to sleep, too.”
Furthermore, participants described methamphetamine as less addictive with some (like Roxanne above) stating that current methamphetamine is less potent than it was the 2010s. Leo said, “I'm a lifelong meth user, I don't after 2 or 3 days sober, I don't feel the need to use it. It's one of those things, you eat a couple bowls of Captain Crunch, you know, you don't start using it unless you want to.” Zac, who also used methamphetamine most of his life, described how he only discovered that he had an addiction to opioids when he was incarcerated, and compared that to emerging thought on methamphetamine use: “Methamphetamines are on board on my life since I've been 12 almost, almost daily. And, uh, the fentanyl was becoming a real bad problem [for me]. […] I guess I was kicking methamphetamines at the time. They didn't even really say the methamphetamines was a physical problem, but now they're figuring out the meth might have a use disorder also like opiates.” Participants also downplayed the negative health effects of methamphetamine, mostly referring to weight loss. Tyler described its effects as subtle: “That drug is really subtle. You know, like the changes are gradual, you know, even in, like, the first time you use it, like, after a couple of days, you know. You slowly lose your grip and the transition is slow enough and subtle enough that you don't really see it.” Gabby even mentioned how she got compliments while using methamphetamine: “And they were like, oh, the medications are working for you. You look so good. You sound so good. I'm like, I'm smoking dope. But they didn't know. I'm like, I've been up for three days. I haven't even looked in a mirror. But but people kept complimenting me.”
When discussing negative effects, many brought up how others found their opioid use detrimental. Like Amy's boundary around having a partner who used opioids, several male participants mentioned that their female partners did not like it when they used opioids or did not tolerate their use. Zac said, “And my life partner was saying, you're pretty much a different asshole on fentanyl, so you better figure out something before I leave your stupid ass. And so I figured out, and I knew it was a big problem at that point.” Mark also said, “And my girl, my ex-girlfriend hates opiates, right? And I'm smoking, like, 25 pills a day. Two grams of, you know, of fentanyl a day, along with the 5 or 6 g of meth a day, you know what I'm saying? So she's not really worried about the meth because, you know, you can go to work and you can function, but she can't stand it when I'm over there, nodded out.”
Two of our participants also described how prior relapses began with a return to methamphetamine use. As mentioned above, Amy expressed how she felt opioids were associated with negative things that had happened in her life, stating, “I wanted nothing to do with opiates.” She also described how a period of abstinence from use ended first with what she felt was innocuous methamphetamine use, which led to a return to opioids. Her response also echoes some of Roxanne's comments about the reduced effects of methamphetamines compared to the 2010s: “I weaseled my way in [a trap house] and, ended up going in, and there was meth. And so I was like, oh, well meth won't hurt. And so I, I smoked some meth and it was like it didn't even do anything to me compared to how it was eight years ago. […] So I ended up taking a hit of a blue. And it made me feel good. […] So, yeah, I kind of I fell into it.”
Tyler mentioned how, after being arrested for outstanding warrants and his history of theft and domestic violence, he returned to methamphetamine use: “After getting out of prison, I was, sober and doing pretty good up until the point where I started using meth again. And then I lost my job and ended up homeless.” His experience of homelessness and the reduced policing of opioids during that time contributed to his fentanyl use even during the time when police sweeps ramped up as he mentions above. Although he acknowledged methamphetamine's role in his relapse, he emphasized opioids’ harms rather than any intrinsic harms of methamphetamine.
Discussion
Our participants’ narratives show how policing patterns in Washington State not only respond to the public health crisis of substance use but also play an active role in constructing perceptions of risk and harm among people who co-use. Participants consistently attributed legal involvement and harm to opioids, even when methamphetamine appeared to play an important role. These narratives reveal how risk hierarchies are produced within broader social and political contexts that define certain drugs as urgent threats while rendering others comparatively manageable. They also demonstrate that the legislative response to fentanyl was framed as a public health risk chiefly in terms of its potential harm to the general public rather than as an urgent health crisis for people who used it themselves. This framing abstracted risk away from those most affected and justified enforcement-centered legislation that failed to provide meaningful support for individuals experiencing addiction, instead intensifying participants’ feelings of shame, guilt, and devaluation through stigma from law enforcement and their social networks. While several institutional forces could be contributing to these perceptions, participants drew clear connections to law enforcement policy and echoed policing rationales in their own experiences. Through the lens of Garriott's (2011) concept of narcopolitics—the governance of populations through the symbolic and material regulation of drug use—our findings illustrate the dual role of policing as both a punitive apparatus and a conduit for public health and political messaging.
Police encounters conveyed and reinforced differential harm between substances. Participants’ accounts show how policing targeted both public opioid use and the moral meanings attached to it. Public arrests for opioid use, “making examples” of people, and visible crackdowns on fentanyl became powerful signals of what participants themselves defined as dangerous. As Buzz succinctly put it, “If you can control the drug, you can control the people better.” As a core feature of narcopolitics, participants internalized the logic that opioids were inherently linked to crime, moral decline, and community harm. In this way, law enforcement worked to embed moral valuations of opioid use into everyday life. By showing how participants attributed risk differentially to fentanyl and methamphetamine in ways that mirrored policing priorities, this study underscores risk not as an inherent property of substances but as a product of narcopolitical governance.
This governance cannot be understood apart from the ways drug policy remains deeply affected by race and class (Dollar, 2019). While participants described the 2021–2023 period as a “free for all” of liberal policy enactment in a predominantly white region of the United States, the return to criminalization after the introduction of fentanyl into drug markets and rising overdose deaths disproportionately targeted those whose use was made visible by poverty. As policing priorities, which were reproduced by our participants, shifted toward “cleaning up the streets” and protecting business districts, the burden of enforcement fell most heavily on unhoused individuals—60% of our study population (see Table 1)—whose lack of private space rendered their substance use inherently public and therefore criminal. By focusing crackdowns on public use, narcopolitics reinforces a historical pattern where the legal system manages the “disorder” of marginalized populations under the guise of public health.
Historical evidence suggests that health and legal risk perceptions may be shaped by broader moral and political climates around certain substances. During the late 2000s, increased public discourse and drove a legislative “moral panic” around methamphetamine use in the United States, citing fears about child exposure and easy production of large quantities of a cheap, dangerous drug (Omori, 2013). Research during this time period showed that people who used methamphetamine often linked their methamphetamine use with violent crime (Brecht & Herbeck, 2013), even when arrest records showed stronger associations with possession and property crime, not violent crime (Gizzi & Gerkin, 2010). The shift in these associations toward opioids evidences the shift in U.S. drug policy away from methamphetamine and toward a fentanyl-centered moral panic. An analysis of Colorado's recent felony laws around fentanyl similarly showed that perceptions of increased criminalization were led largely by fear rather than evidence, and that the laws were a misguided step toward overdose prevention and treatment for OUD (LeMasters et al., 2025). Our findings show how narcopolitics reconfigures which drugs are rendered visible as threats, demonstrating the historical contingency of the socially produced relationship between crime and drug use.
Several participants describe a decrease in methamphetamine's potency as a rationale for its reduced policing. Quinones (2021) has suggested that changes in methamphetamine manufacturing since the regulation of ephedrine and the crackdown on home “meth labs” have resulted in a higher degree of neurotoxicity and associations with schizophrenia and violence. Other data have shown that changes in methamphetamine manufacturing in the United States have not affected regional purity (Toske & McKibben, 2022). Our participants’ experiences of less consequential or potent methamphetamine therefore align more closely with changes in policing. They reported fewer physiological effects even if they risked exposure to potentially more dangerous forms of the drug, suggesting that rather than pharmacologic changes, what matters to these perceptions are the changes in the sociopolitical landscape. Thus, we show how drug-related risk perceptions (and even their physical effects) are mitigated by their everyday interactions with law enforcement.
Understanding how these legal and political changes can also produce physical effects requires attention to what Dwyer and Moore call the “ontological contingency” (2013) of methamphetamine—how its use patterns and effects vary by context—following a rich body of scholarship on how experience of substance use is contingent on environments, social structures, institutions, and affective states (see, e.g., Duff, 2016). In addition to other factors like comorbid attention disorders, combined use of sedatives, or degrees of tolerance, the beliefs and phenomenological experiences of methamphetamine being less potent are likely also influenced by its relative lack of emphasis in policing compared to fentanyl. Participants often framed methamphetamine as enabling productivity, sustaining social relationships, or facilitating daily functioning (including in encounters with police), in contrast to opioids’ associations with withdrawal management, and illegal activity. These distinctions were not inherent to the drugs themselves but emerged from a policing regime that rendered opioids highly visible, heavily criminalized, and morally charged, while leaving methamphetamine relatively unpoliced, a product both of narcopolitics and of legislative action that circumscribes how certain substances are acted upon (Seear, 2020).
Several participants also reported returning to substance use through methamphetamine because it was perceived as less dangerous or legally consequential. Malins’ (2017) conceptualization of drug use as unfolding within “desiring assemblages” is useful here, as it highlights how motivations and practices evolve in response to shifting socio-material conditions rather than remaining fixed at the level of individual choice. In this way, selective enforcement may indirectly shape relapse trajectories and treatment engagement by reorganizing perceived pathways of risk. Indeed, it may help explain why people who co-use have increased legal recidivism and lower retention rates in treatment for OUD.
Though none of our participants reported direct referrals to treatment by law enforcement, several had experiences of treatment offered through the legal system. We report elsewhere (Iacobelli et al., 2026) how our participants navigated this treatment—including MOUD—in carceral facilities, through drug courts, and mandated treatment. They identified features of treatment that extended the punitive aspects of incarceration in ways that also fall under the rubric of narcopolitical governance (and also prioritized fentanyl and other opioids over methamphetamine). Restricting autonomy and placing demands on treatment further regulate the acceptable ways participants move through recovery and experience sobriety, relapse, and legal involvement.
Taken together, these findings extend narcopolitics as a conceptual tool for understanding how governance produces not only compliance or resistance but also differential epistemologies and ontologies of drug risk. By demonstrating how participants’ understandings mirrored policing priorities, this study shows that risk is not simply measured or communicated through policy but actively constituted through it. Such dynamics may contribute to distorted risk communication, unequal harm reduction access, and the apparent strengthening of associations between specific drugs and crime simply by increasing arrests for use and possession.
Fentanyl's intensified policing has increased practical risks by forcing people to use in isolated spaces and exposing them to the harms of incarceration while recasting it as uniquely pathological and fostering the internalization of guilt, shame, and fear. Meanwhile, the relative downplaying of methamphetamine risks may hinder accurate assessment and intervention. Responses to polysubstance use must therefore attend not only to epidemiological indicators but also to the social afterlives of policy decisions—including how they shape the frameworks through which people who use drugs interpret their own experiences. Treatment models should be attuned to how people who co-use conceive of individual substances and to the role punitive action and public health messaging have in those constructions. Only by addressing these layered determinants can policy and clinical systems provide effective interventions.
While situated in Washington State, these findings speak to a broader pattern in global drug governance, where rapid policy shifts in response to the rise of synthetic opioids remake hierarchies of risk and reconfigure the lived realities of polysubstance use. This analysis is useful for understanding the dynamic policy responses to shifting substance use patterns and their effects on people who use drugs by directing attention to bureaucratic agencies like law enforcement that enact that policy. It invites us not to take for granted that new or changing substances are inherently dangerous or associated with increased crime, but to critically interrogate how and where those discourses are reproduced. Our findings underscore the need for policy frameworks that recognize the mutually constitutive relationship between law enforcement, public health messaging, and people's lived experiences of substance use.
Our study is limited in its ability to map our participants’ experiences to specific points in time during the legislative changes to draw clear causal links between policing and descriptions of risk. Additionally, we cannot fully account for how initiating MOUD prior to recruitment may have affected their narratives. The study has a modest sample size, though it was sufficient to identify cohesive themes and explain deviations from those themes. Some themes, like the racial dimensions of policing and substance use, were not the focus of our interviews and did not emerge often enough organically to provide a robust enough analysis here. Larger-scale ethnographic research that tracks legal involvement, public policy, and participants’ experiences with police over time would help clarify our findings and hone our analysis. Though the local context of drug policy limits this study's generalizability, we hope that the social analysis and the theoretical insights allow for its translation to other contexts.
In summary, this study reveals how changing patterns of law enforcement shape people's behaviors and attitudes around their substance use. In the context of increased fentanyl policing, participants consistently attributed legal entanglements and greater health risks to opioids, while they considered methamphetamine to be less dangerous and more beneficial. These accounts reflect not just individual belief systems, but broader political and social processes that link public health and policing through narcopolitics. Ultimately, this study underscores the need for drug policy and treatment frameworks that reckon with the unequal governance of different substances and how those dynamics shape social worlds.
Our findings offer a critical analysis of the brief window of reform in Washington, where the State v. Blake decision moved toward decriminalization. The subsequent “failure” of these policies in the public imagination, fueled in part by the introduction of fentanyl and economic instability, has been used to justify a rapid retreat toward punitive measures. This study shows how narcopolitics has constructed fentanyl as a unique threat that demands a return to punitive responses and has a strong effect on how people who co-use understand their substance use. Recognizing these dynamics is essential to building more effective, contextually grounded responses to polysubstance use that move outside the cycle of decriminalization-recriminalization. Without addressing how policing actively shapes the lived reality and risk perceptions of people who use drugs, future health-focused reforms risk being once again undermined by the constitutive link between substance use and narcopolitics.
Footnotes
Acknowledgments
Demographic data collection and management were made possible with REDCap electronic data capture tools hosted at the University of Washington, supported by the Institute of Translational Health Sciences, which is funded by the National Center for Advancing Translational Sciences of the National Institutes of Health (Award number UL1TR002319).
ORCID iDs
Ethical Considerations
The study was approved by the University of Washington IRB. Interviews were conducted privately. All direct and indirect identifiers were removed from interview transcripts, and all data were linked to a unique study ID for each participant. After data analysis, each participant was assigned a pseudonym, confirming that no real names were used. Individual narratives were made as generic as possible to protect confidentiality. Data were securely stored in an access-restricted FERPA and HIPAA-compliant cloud-based storage system. A U.S. Federal Certificate of Confidentiality issued by the National Institutes of Health/National Institute on Drug Abuse protects the data and its collection.
Consent to Participate
All participants provided verbal consent to participate after reviewing and being provided a physical consent form.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH/NIDA HEAL Supplement, National Institute on Drug Abuse (grant number R34DA057609).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are of a sensitive nature and are consequently not available to those outside of the study team and are exempt from storage in a data repository. Sufficient deidentification of the data would render it of little use to future researchers. Data summaries can be made available to researchers upon request with appropriate IRB approval.