
Abstract
Parents of preterm infants often experience high levels of stress resulting in feelings of trauma after discharge from the neonatal intensive care unit (NICU). However, post-traumatic growth can occur after a stressful incident resulting in more favorable individual outcomes. One predictor of post-traumatic growth that has not been studied in relation to the NICU is parents’ religiousness and spirituality. This study focused on filling this gap in the literature by conducting a pilot study comprised of 25 parents’ reports on their experiences of post-traumatic growth post-NICU discharge. Specifically, we explored associations between parents’ reports on religiousness and spirituality through measures of parent–child sanctification, religious coping, and spiritual disclosure in relation to parents’ distress and their post-traumatic growth. We found that parents who sanctified their parent–child relationship experienced higher levels of post-traumatic growth even in the presence of stress. Parents who reported increased use of positive forms of religious coping and open spiritual disclosure with their spouse/partner also reported higher levels of post-traumatic growth. Results support a continued focus on family-centered NICU care during and after discharge with the caveat of also considering parents’ spiritual and religious worldviews.
The appearance of a fragile, sick infant and changes to the parental role can cause significant distress and even trauma in parents who have a child in the neonatal intensive care unit (NICU) (McIntosh, Stern, & Ferguson, 2004; Seideman et al., 1997; Shanmugam & Ramachandra, 2015). Many parents are unprepared for their infant’s hospitalization and are unaware of the potential for long-term negative outcomes (McIntosh et al., 2004), which can include developmental, psychological, and physical challenges. Initially, not being able to hold the infant causes parental distress, and later, due to the infant’s potentially unstable condition, a variety of difficult emotions can emerge (Seideman et al., 1997), including anxiety and depression. This distress can impact parents’ ability to emotionally bond with their infant and respond to her/his needs (McIntosh et al., 2004; Shanmugam & Ramachandra, 2015), which can affect parental confidence in caring for their infant. These emotional difficulties combined with prolonged parent–infant separation, frequent lack of privacy during infant care, and lack of support for the parental role of the neonate (i.e. a newborn less than four weeks of age) can exacerbate stress while in the NICU and have implications for parenting post-NICU discharge. Thus, parents’ experiences in the NICU may result in feelings akin to a trauma due to this unforeseen and unpredictable intensive care experience, which can result in post-traumatic stress, anxiety, and depression (Aftyka, Rozalska-Walaszek, Rosa, Rybojad, & Karakula-Juchnowicz, 2016).
Family-centered care, which focuses on actively engaging parents and caregivers in emotional, social, and developmental care of the neonate in a medical setting (Griffin, 2006), would benefit from understanding how parents’ psychological perspectives are affected following their NICU experience. Thus, a focus on the newborn in the context of their family, which is fundamental for family-centered NICU care, would entail exploration of parents’ trauma and subsequent post-traumatic growth following this intensive care setting.
The ways in which trauma negatively influences people’s lives have been well documented, but in response to traumatic events, some individuals, surprisingly, are able to change in positive ways (Forinder & Norberg, 2014; Joseph, Murphy, & Regel, 2012; Picoraro, Womer, Kazak, & Feudtner, 2014). According to Joseph and colleagues (2012), “trauma need not be a wholly destructive force in a person’s life” (p. 317). This idea is echoed by Colville and Cream (2009), who found that traumatic experiences are not universally negative even when parents were dealing with a critically ill child. Thus, emerging from a trauma with an experience of post-traumatic growth (PTG) can result in several broad positive outcomes: relationships are made stronger or more meaningful; individuals begin to see themselves in a new way; and a new appreciation for life develops (Colville & Cream, 2009; Forinder & Norberg, 2014; Joseph et al., 2012; Taku & Cann, 2014; Tedeschi & Calhoun, 1996). In a more general sense, PTG has been conceptualized as the processing of learning from and finding meaning in traumatic events (Jayawickreme & Blackie, 2014). Furthermore, the cognitive ability to reframe one’s sense of the world can lead to post-traumatic growth. This concept, developed by Janoff-Bulman and Yopyk (2004), is sometimes referred to as appreciation through existential reevaluation (Barr, 2011; Joseph et al., 2012). In extreme cases, such as NICU hospitalization, the unconscious awareness of mortality can result in reappraisal and post-traumatic growth (Barr, 2011). For some parents, the awareness of the fragility of life brought about by the NICU experience results in parents being more appreciative of life and no longer taking things for granted (Forinder & Norberg, 2014).
Religiousness is a salient aspect of an individual’s belief system and can have a significant influence on many areas of a person’s life, including post-traumatic growth following traumatic experiences. Religiousness and spirituality have played demonstrable roles in the degree of post-traumatic growth experienced after difficult life experiences (O’Rourke, Tallman, & Altmaier, 2008; Taku & Cann, 2014). Generally, individuals may seek out religion when they are experiencing post-traumatic growth, or engagement in religion may serve as a catalyst for growth following a challenging life situation (Calhoun, Cann, Tedeschi, & McMillan, 2000). Moreover, O’Rourke and colleagues (2008) speculate that, in some instances, religious or spiritual beliefs develop as a result of difficult circumstances.
The field of the psychology of religion and spirituality has a depth of knowledge on how religion and spirituality affect individual mental health (See Emmons & Paloutzian, 2003) and has made significant advances in studying religiousness, spirituality, and family relationships in the recent decade (Mahoney, 2010). However, the extant medical and psychological literature remains scant when exploring distressed families or families who are struggling with a significant life event (Mahoney, 2010). The birth of an infant who must be admitted to the NICU is one of these stressful situations in family life. In particular, parents may call upon spiritual resources to handle challenging decisions about their babies’ health or to deal with their expectations of parenting that have been tested as a result of having a baby admitted to the NICU. The existing literature finds that, in particular, mothers tend to struggle with higher levels of anxiety and depression while their baby is in the NICU (Pisoni et al., 2014) and may even display symptoms of post-traumatic stress following their infant’s NICU experience (Greene et al., 2015).
People may also sanctify their relationships with theistic or spiritual significance (Pargament & Mahoney, 2005). This imbuing of the sacred into familial relationships has been related to better familial functioning and greater relationship satisfaction (Brelsford & Mahoney, 2008). Sanctifying the parent–child relationship in the instance of a NICU experience may be of the utmost importance in respect to dealing effectively with this distressing situation. More religious parents may find they sanctify their parent–child relationship through a manifestation of God or feeling God is present in the relationship. Less religious parents may find that a non-theistic pathway is more meaningful in that they imbue their parent–child relationship with sacred meanings. Taken together or separately, both theistic manifestations of God or non-theistic sacred qualities comprise the notion of sanctification of the parent–child relationship (Murray-Swank, Mahoney, & Pargament, 2006).
Furthermore, how a parent copes with their child’s hospitalization through religious or spiritual coping strategies also impacts the family. Religious coping can be both negative and positive in that parents may feel that God is supporting them and they use God through prayer to deal with their child’s hospitalization, or they may feel angry or abandoned by God during this time (Pargament, Feuille, & Burdzy, 2011). Parents can experience both positive and negative forms of religious coping as they are not dichotomous, but are often co-occurring (Brelsford et al., 2016). Positive religious coping can include looking for a stronger connection with God, seeking God’s love and care, or putting plans into action together with God, whereas negative religious coping involves questioning the power of God, feeling that God was punishing or had abandoned the individual, or questioning God’s love (Pargament et al., 2011). Clearly, the latter reflects spiritual struggles that tend to have deleterious effects, whereas the former emanates a sense of working together with God through a difficult or challenging situation resulting in more favorable outcomes.
In addition, parents may find spiritual disclosure (Brelsford & Mahoney, 2008) with their partner, which entails sharing views on religious beliefs and faith journeys, to be another NICU coping strategy. Open and supportive spiritual disclosure can foster a sense of spiritual intimacy between parents due to the sharing of deeply held foundational spiritual and religious beliefs. There has been scant work on spiritual disclosure between NICU families, but findings from college student–parent dyads have revealed that having this level of relational spirituality can been helpful for parent–young adult child relationship functioning (Brelsford, 2013; Brelsford & Mahoney, 2008). In sum, parents’ religious and spiritual worldviews are nuanced and complex. Therefore, exploring multiple facets of parents’ religiousness and spirituality during and after NICU discharge can illuminate pathways to individual experiences of distress and post-traumatic growth, which to date remains unexplored.
Current study
The objective of this study was to explore associations between parents’ post-traumatic growth, distress (e.g. depression, anxiety, and stress), and aspects of their religiousness and spirituality post-NICU discharge. We explored parents’ religiousness and spirituality through their sanctification of the parent–child relationship, use of spiritual conversations with partners about religious and spiritual beliefs, and use of both positive and negative forms of religious coping, all providing a more intricate and nuanced view of their religious and spiritual landscapes. We hypothesized that increased religiousness and spirituality via markers of sanctifying the parent–child relationship, open spiritual discussions with a partner, and increased positive forms of religious coping would be related to lower levels of stress, anxiety, and depression and greater levels of post-traumatic growth. We also hypothesized the increases in negative religious coping would have a positive association with parents’ stress, anxiety, and depression and would have an inverse relation to post-traumatic growth. Finally, we did not have any a priori hypotheses on links between anxiety, depression, or stress in relation to post-traumatic growth since some individuals grow from distress whereas others do not.
Method
Participants
In this exploratory study, after securing institutional review board approval from our university and medical school, we obtained responses from 25 parents of preterm infants (13 mothers and 12 fathers) six weeks after discharge from the NICU. Parents completed self-report questionnaires related to their post-traumatic growth, current distress level (anxiety, depression, and stress), use of religious coping, experiences of spiritual disclosure with their spouse/partner, and sanctification of the parent–child relationship. This study was part of a larger study that involved an initial assessment of 52 parents at time one (5–7 days after entrance to the NICU). For this study, inclusion criteria were that parents must be 18 years or older with fluency in English. Parents may have had a singleton or multiples born between 25 and 35 weeks gestation and admitted to the NICU within 48 hours of delivery. Exclusion criteria included infants born with congenital syndromes, severe or life-threatening illnesses, or significant deformational abnormalities. In addition, parents were not contacted if there was a maternal illness that provided challenges with study consent. This study’s participants were taken from a third wave of follow-up questionnaires, thus attrition occurred from 52 down to 25 respondents, which is commonplace in longitudinal research.
For this study, parents were almost equally comprised of men (N = 13) and women (N = 12) with a Mage of 30.36 (SD = 4.10), and were mostly white (88%) and married (96%). Religious affiliation was listed as Protestant or Catholic for 40% of the sample, 20% reported no religious affiliation, 20% reported being agnostic or atheist, and 20% reported their religious affiliation as “other.” Parents’ reports on religiousness and spirituality demographic variables indicated a majority of the small sample was slightly to very religious (60%) and spiritual (80%). Further, 52% reported praying a few times a week to more than once a day, and 68% reported religious service attendance from once or twice a year to every week.
Measures
Brief Religious Coping Scale
The Brief Religious Coping Scale (RCOPE) is a 14-item measure used to assess both positive (seven-item subscale) and negative (seven-item subscale) types of religious coping. Participants rate positive (“Sought God’s love and care”) and negative (“Questioned the power of God”) statements on a 1–4 scale (1 representing “Not at all” and 4 representing “A great deal”).
Developed by Pargament and colleagues (2011), the Brief RCOPE has demonstrated high internal consistency for both positive and negative religious coping subscales. High to average alphas were also evinced in this study, with positive religious coping at .93 and negative religious coping at .72.
Spiritual Disclosure Scale
The Spiritual Disclosure Scale (SDS) (Brelsford & Mahoney, 2008) is a 20-item measure developed to assess the extent of personal spiritual or religious discussions within a family unit. Participants responded to items about their spouse/partner on a four-point Likert scale (1 = “never,” 4 “often”). The SDS includes overarching items pertaining to spiritual disclosure as well as items pertaining to specific aspects of spiritual and/or religious beliefs or practices. Sample items include, “I talk to my spouse/partner about spirituality and religion” or “My spouse/partner and I discuss changes that have occurred in our views of religion.” In previous studies the SDS demonstrated high internal consistency (Brelsford, 2013) and moderate convergent validity (Brelsford & Mahoney, 2008). In this study, Cronbach’s alpha was .96.
Post-Traumatic Growth Inventory
Developed by Tedeschi and Calhoun (1996), The Post-traumatic Growth Inventory (PTGI) is a 21-item scale used to measure personal growth following the experience of a traumatic or stressful life event. Items are rated using a six-point Likert scale with statements ranging from “I did not experience this change” to “I experienced this change to a very great degree.” Sample items include, “I changed my priorities about what is important in life” and “I can better appreciate each day.” Prior research demonstrated high internal consistency (.90) and construct validity, which also occurred in this study with a Cronbach’s alpha of .96.
Sanctification (theistic): the Manifestation of God Scale
Adapted from Mahoney et al. (1999), the Manifestation of God in Parent–Child Relationships scale is a 14-item theistic measure focusing on the traditional view of God and the perception of God’s presence in the parent–child relationship. Statements include, “God is present in my relationship with my child” and “I experience God through my relationship with my child.” Parents rate responses using a 1 (strongly disagree) to 7 (strongly agree) rating scale. The Manifestation of God Scale has shown high levels of convergent validity (Murray-Swank et al., 2006) and good internal consistency (ranging from .97–.98). For this study, Cronbach’s alpha was .98.
Sanctification (non-theistic): Sacred Qualities Scale
The Sacred Qualities Scale is a nine-item semantic differential measure that uses contrasting adjectives (blessed vs. cursed, spiritual vs. worldly, holy vs. unholy) to focus on the perception of the sacred in the parent–child relationship. The two opposing adjectives were placed on a line labeled “very closely describes” at both ends and “neutral” at the midpoint, with ratings on a seven-point scale. Parents read each word pairing and then indicated the point on the line that most closely represented their relationship. Higher scores represented an increased presence of sacred qualities in the parent–child relationship. Coefficient alphas range from .87 to .88 (Mahoney et al., 1999). For this study, Cronbach’s alpha was .91.
Depression Anxiety Stress Scale – 21
The Depression Anxiety Stress Scale (DASS) (Lovibond & Lovibond, 1995) is a measure comprised of 21 items focused on assessing depression, anxiety, and stress within the past week. The scale is comprised of three subscales, depression, anxiety, and stress, each containing seven items, ranging on a scale from 0 (did not apply to me at all) to 3 (applied to me very much for most of the time). Sample items include, “I found it hard to wind down” and “I couldn’t experience any positive feelings at all.” For this study, Cronbach’s alphas were .86, .71, and .79, respectively for each subscale (depression, anxiety, and stress).
In addition to these questionnaires, parents also completed demographic information on biological sex, race, age, marital status, income, education, and employment status. They also completed religious and spiritual demographic questionnaires including frequency of prayer and religious service attendance, self-reported extent of religiousness and spirituality, and religious affiliation.
Procedure
Approximately six weeks post-NICU discharge, parents were mailed survey packets containing questions related to their coping, mental health variables, religiousness and spirituality, and post-traumatic growth. These surveys were sent with self-addressed return envelopes that were to be returned to the research team. Fifty-two surveys were sent following responses from stage 1 of this study, with a return rate of 48% (N = 25).
Data analysis
After calculation of psychometric properties of the instruments’ subscales (see Table 1), we computed participant demographics, and Pearson product-moment bivariate correlations between major study variables using SPSS version 25 (see Table 2). Correlations were followed by hierarchical regression analyses to determine if there was an association between parents’ sanctification of the parent–child relationship and post-traumatic growth after accounting for parents’ biological sex and parental reports of stress. Due to the small sample size, limited variables were entered into the regression equation.
Means, standard deviation, minimum and maximum scores, and internal consistency of primary study variables and scales.
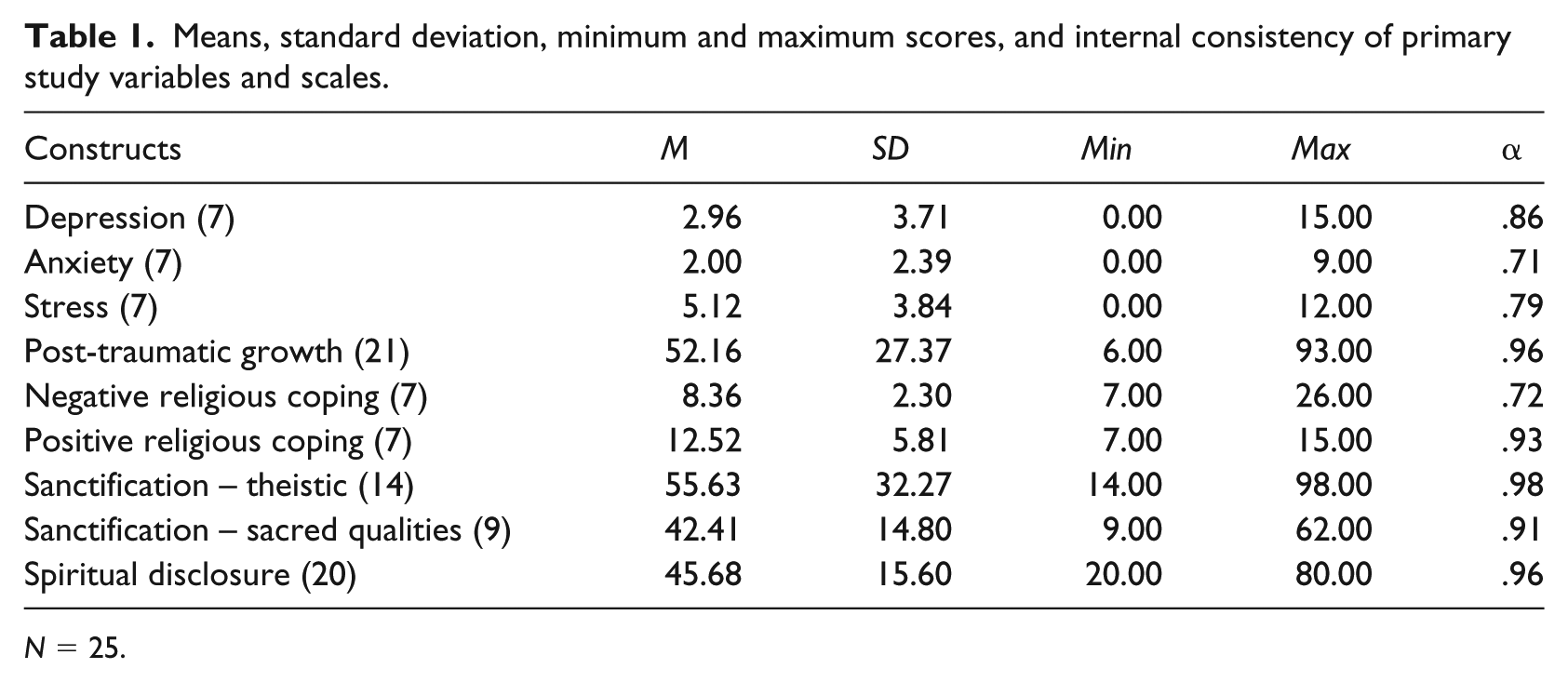
N = 25.
Bivariate correlations.
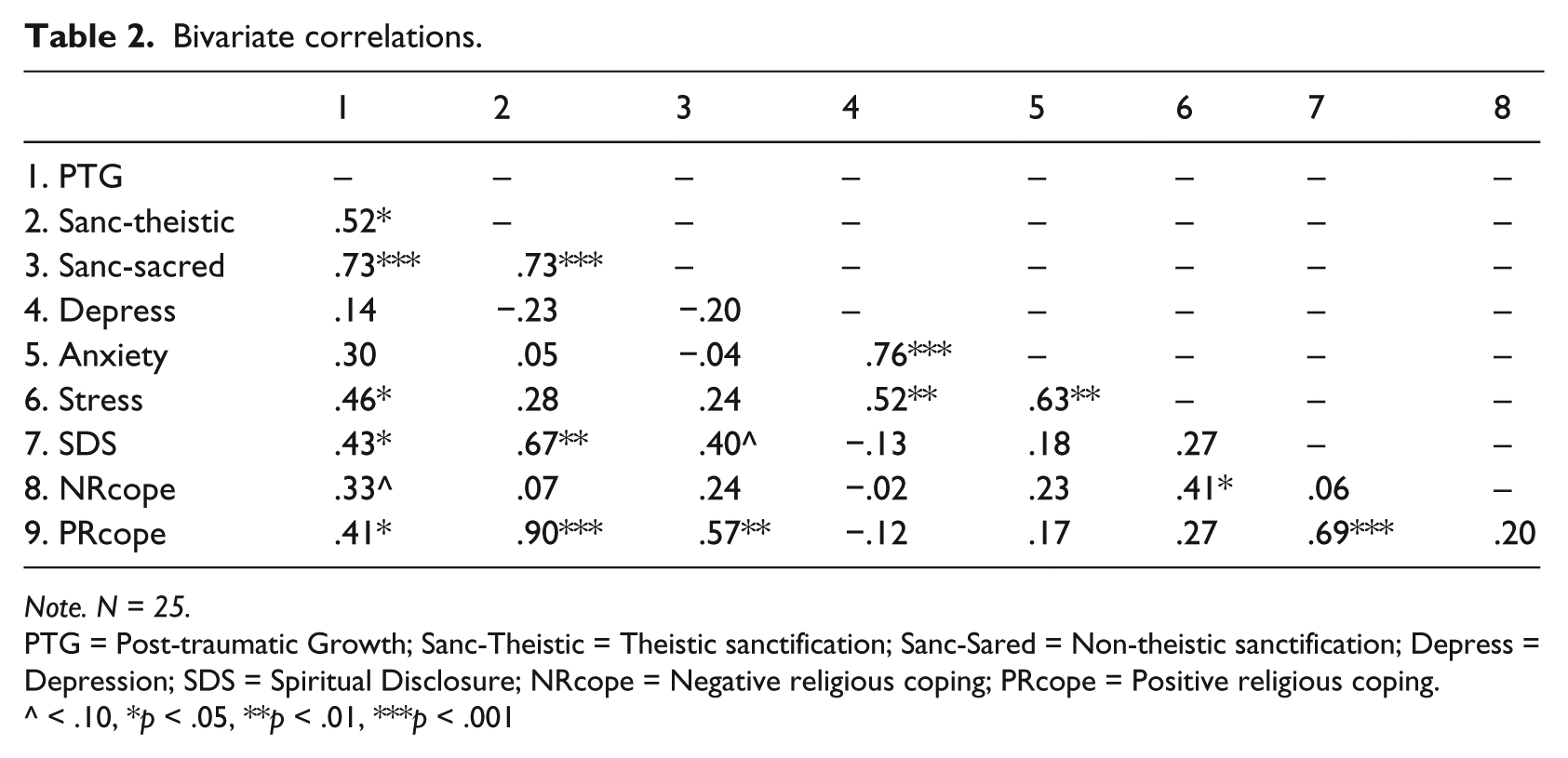
Note. N = 25.
PTG = Post-traumatic Growth; Sanc-Theistic = Theistic sanctification; Sanc-Sared = Non-theistic sanctification; Depress = Depression; SDS = Spiritual Disclosure; NRcope = Negative religious coping; PRcope = Positive religious coping.
< .10, *p < .05, **p < .01, ***p < .001
Results
Pearson product-moment correlations (N = 25) were conducted for this exploratory study. There were significant correlations between parents’ reports of religiousness and spirituality variables and PTG. For instance, correlations between parents’ religious and spiritual indices and PTG indicated that increased PTG was associated with higher levels of positive religious coping (r = .41, p < .05), spiritual disclosure (r = .43, p < .05), and sanctification of the parent–child relationship (r = .52, p < .05 – manifestation of God; r = .73, p < .001 – sacred qualities). In addition, higher levels of stress post-NICU discharge was related to parents’ increased use of negative religious coping (r = .41, p < .05), but was also significantly correlated to higher reports of post-traumatic growth (r = .46, p < .05), suggesting more stress, be it related to parenting their newborn or juggling new parenting duties and other life issues such as work or family life, might afford an opportunity for growth (see Table 2). In addition, parents’ positive religious coping post-NICU discharge was significantly positively correlated with increased theistic sanctification of the parent–child relationship (r = .90, p < .001), greater spiritual disclosure between parents (r = .69, p < .001), and increased non-theistic sanctification of the parent–child relationship (r = .57, p < .001). Finally, parents’ ratings of stress, anxiety, and depression were all significantly positively correlated with each other (see Table 2), but only stress was significantly positively correlated with parents’ use of negative religious coping (r = .41, p < .05).
Further, a hierarchical linear regression revealed that after accounting for biological sex in Step 1, and parents’ reports of stress in Step 2, sanctification of the parent–child relationship (β = .84), specifically non-theistic sacred qualities, entered in Step 3 remained significantly associated with parents’ post-traumatic growth (see Table 3). These results indicate that, after controlling for stress level and biological sex, parents’ sanctification of the parent–child relationship, specifically through non-theistic sanctification or imbuing the parent–child relationship with sacred qualities, was related to feelings of resiliency and growth post-neonatal intensive care stay.
Unique effects of parents’ biological sex, stress, and sanctification on post-traumatic growth.
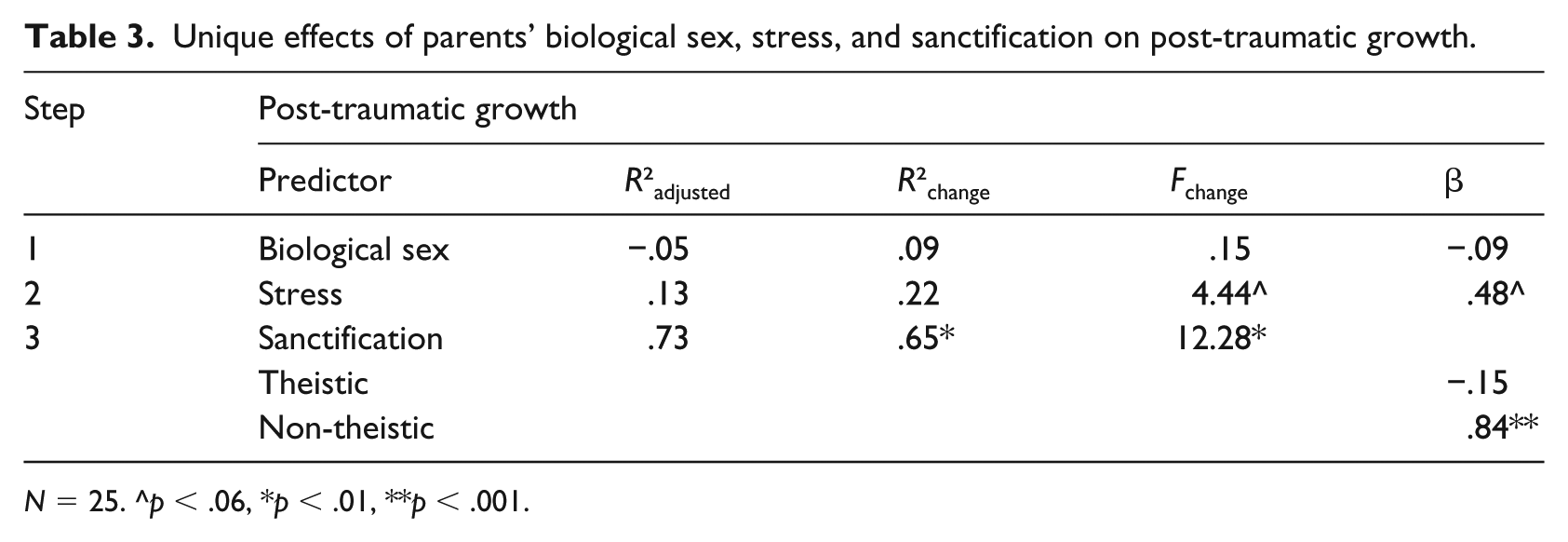
N = 25. ^p < .06, *p < .01, **p < .001.
Discussion
Parents’ experiences in the NICU and after discharge are often fraught with anxiety and stress. However, family-centered NICU care can assist parents in coping more effectively with this stress. In particular, exploring parents’ religious and spiritual views and beliefs can shape how they cope with the stress of the NICU and post discharge. In particular, based upon results from this study, it appears that a parent’s spirituality and religiousness is a necessary factor to consider in relation to their stress levels and their ability to experiencing growth following the NICU experience. In this pilot study, we found that when parents were able to sanctify their parent–child relationship, which means they imbued the relationship with spiritual significance and also felt God was part of the relationship, they experienced a higher level of post-traumatic growth. Parents who also felt that God was supportive and present, which is considered positive religious coping, experienced lower levels of distress. Additionally, this pilot sample of parents also had higher levels of stress when they were engaging in open spiritual discussions and coped in positive ways regarding the stressors they experienced while in the NICU and upon hospital discharge. As predicted, feeling angry at God or abandoned by God, which is considered to be a negative form of religious coping, was related to more stress for parents. Interestingly, higher levels of stress were also related to higher levels of post-traumatic growth, suggesting that stress levels may be necessary to grow from difficult experiences. It should be noted that this sample did appear to have non-clinically significant levels of stress, depression, and anxiety, but any level of distress (be it clinically elevated or not) can result in concerns following NICU discharge. Furthermore, parents with low levels of distress still experience challenges with their babies post discharge, including feeding difficulties and concerns about growth, and often must return to the hospital setting for follow-up care.
Our results suggest focusing on the whole person in relation to proper NICU care is necessary for families to thrive after discharge. Specifically, family-centered NICUs can benefit from exploring parents’ religious and spiritual lives, including how they integrate religious and spiritual discussions into their partner relationships, if they sanctify their family relationships, and how they use both positive and negative forms of religious coping when dealing with their baby being in the NICU. It makes theoretical sense that parents who are using negative secular coping methods (e.g. through use of substances, denial, or behavioral disengagement) will likely not have positive outcomes in relation to this life challenge, but we know less about religious and spiritual forms of coping post-NICU discharge. This study was the first to explore parents’ religious coping and sanctification of the parent–child relationship following their NICU experience. Furthermore, finding that parents’ imbuing of sacred qualities into their parent–child relationship had strong associations with post-traumatic growth after the NICU experience, even after accounting for stress, is important to build upon. Thus, continuing to explore ways to assist parents must include all spheres of life, be it secular, religious, or spiritual, to address NICU families’ needs.
Limitations, future directions, and implications
Limitations of this study are related to the small size of our sample. This was an exploratory study with three waves of data that resulted in typical levels of attrition among participants. However, even with the low sample size, we believe that due to the exploratory nature of this study, our results are noteworthy. In addition, our sample was not clinically distressed, as evinced by their reports of depression, anxiety, and stress. Certainly, more highly distressed samples may provide different results related to post-traumatic growth and other personal and relational outcomes. However, even with non-clinical levels of self-reported distress, it is clear that these parents are experiencing growth. Further, this sample was rather homogenous in relation to racial/ethnic background (e.g. mostly white) and religious affiliation (e.g. mostly Christian), and most were married, but nonetheless this is a starting point for future studies that can explore more diverse groups of parents. Finally, we cannot suggest causal links between our study variables. Specifically, we cannot attribute post-traumatic growth to only the study variables at hand, but we believe that, in a pilot study with a very challenging population to survey, we have contributed to the literature in this area.
Our findings open the door to future researchers who would like to take our work a step further and explore PTG and religiousness/spirituality with larger, diverse samples and possibly with varied methodologies. Future studies may find it useful to add qualitative narrative material to illustrate parents’ spiritual meanings. A mixed method study would elucidate parents’ nuanced experiences of religion and spirituality, which would provide additional information regarding the interaction between their religious and spiritual lives and post-traumatic growth after neonatal intensive care experiences. Future research could also explore the role of caregivers, such as nurses, physicians, social workers, psychologists, or chaplains, in the amelioration of stress during and after the NICU experience. Family-centered NICU care’s emphasis on engaging parents in the treatment of their infants calls for a commitment by the system of caregivers within the hospital and beyond (e.g. pediatricians, community mental health workers, clergy) to respond to parental needs, including their psychological and spiritual issues.
In summary, our results point to the importance of assessing spiritual dimensions of parents’ lives. When exploring family-centered NICU care, it is important to determine what strategies are most helpful for parents to ensure they feel more competent and are able to cope with the residual feelings of anxiety, stress, depression, or trauma post-NICU discharge. Certainly, parents’ spirituality and religiousness can be sources of support and beacons of hope, or can provide challenges in dealing with salient life events, such as the birth of a child. Thus, not only do we need to continue to explore strategies to support and encourage families, but we also need to account for the importance of spirituality and religiousness in their worldviews and their reliance on these worldviews as methods of coping with life events.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received an internal Research Council Grant from Penn State Harrisburg, USA to fund this research.