
Abstract
The present study uses longitudinal data to investigate whether differences in exposure to community violence discriminate among serious juvenile offenders in terms of mental health symptomatology for depression, anxiety, posttraumatic stress, and hostility. Group-based modeling and moderation analyses are used to assess the influence of exposure to violence on mental health outcomes. The results demonstrate a moderating effect of psychosocial maturity and social support between exposure to community violence and adverse mental health consequences for youth on the stable low exposure trajectory. In addition, youth who experience stable high exposure to violence consistently suffer worse outcomes. The study contributes to the development of empirically derived profiles of serious youth offenders. While all of the youth in this study may face the stigma of being labeled as dangerous, some (particularly those on the chronic exposure trajectory) might find themselves in a situation where their psychological status exacerbates an already tenuous situation: reentry. Therefore, reentry services should better target the specific needs of this returning subgroup of serious youth offenders.
According to the National Survey of Children’s Exposure to Violence, between 80% and 90% of children witness, learn about, or are victims of violent acts (Finkelhor, Turner, Ormrod, Hamby, & Kracke, 2009). Despite the large number of children exposed to violence, the prevalence, forms, severity, and reactions are not equally distributed across all youth. In terms of community exposure to violence, the occurrence is highest for urban, poor, and minority youth (Aisenberg & Herrenkohl, 2008), with rates of exposure ranging from 75% to 90% (Farrell & Bruce, 1997; Finkelhor et al., 2009; Selner-O’Hagan, Kindlon, Buka, Raudenbush, & Earls, 1998). Unfortunately, over the last 30 years, a steady stream of research demonstrates a strong connection between childhood exposure to community violence and adverse consequences, such as mental health problems (see Fowler, Tompsett, Braciszewski, Jacques-Tiura, & Baltes, 2009, for a review). Some studies indicate that children exposed to violence are up to 5 times more likely to experience negative effects than other children (Saunders, 2003).
While much research exists on the psychological consequences of exposure, few studies parse out these effects from their associations with various risk factors across multiple domains: individual, family, peer, and neighborhood. In addition, prior studies primarily rely on samples selected from general populations of adolescents, which may underrepresent the experiences of those youth on the extreme end of the continuum of exposure and as a result, find small or moderate effect sizes (Fowler et al., 2009).
The present study attempts to address these issues in several ways. First, we use longitudinal data from the Pathways to Desistance Project to investigate whether differences in exposure to community violence differentiate among serious juvenile offenders in terms of negative mental health outcomes. Second, we include an extensive number of controls so as to isolate the specific effects of exposure to community violence. We also include the personality trait of impulsivity, which has been found to correlate with adverse mental health statuses, yet is rarely examined. Third, we include multiple moderating variables to see whether they explain the relationship between exposure and mental health. And fourth, we examine whether such violence exposure is related to mental health symptomatology for depression, anxiety, posttraumatic stress, and hostility, a broader range of mental health outcomes than considered in previous work.
The study also uses latent class growth analyses that offer an opportunity to simultaneously explore changes in exposure to violence as they relate to risk covariates and moderating factors. In this way, the present study contributes to the literature on developmental psychopathology by explicitly examining the interactions among individual-, small-group-, and neighborhood-level variables in terms of their potential relationships to changes in exposure and mental health. As a result, it may be possible to identify trajectory subgroups that can then be targeted for interventions in ways that are more in line with their unique pathways.
The use of a sample of serious juvenile offenders has a few advantages. First, juvenile offenders in general, and serious (felony-charged) juvenile offenders, are more likely to be exposed to community violence than their counterparts not involved in the justice system (Cuevas, Finkelhor, Turner, & Ormrod, 2007). Second, they are more likely to have greater mental health problems and shared risk factors than the general youth population (Halliday-Boykin & Graham, 2001; Schubert, Mulvey, & Glasheen, 2011), thus making it easier to parse out the role that exposure may play in producing adverse outcomes, net other commonly identified risk factors.
Mental Health Consequences of Exposure to Community Violence
Overall, research suggests that exposure to community violence is related to the development of internalizing disorders such as depression, anxiety (see Fowler et al., 2009, for a review), and posttraumatic stress disorder (PTSD; Scarpa, 2001; Wood, Foy, Layne, Pynoos, & James, 2002); independent of sociodemographic factors (see Lynch, 2003, for a review); and especially among those with high and/or chronic levels of exposure (Cooley-Quille, Boyd, Frantz, & Walsh, 2010). Children who are chronically exposed adopt ways to cope with feelings of threat and loss of control (Aisenberg & Herrenkohl, 2008), including hostility (Flannery, Singer, & Wester, 2001; Moses, 1999). For that matter, studies indicate that the negative impact of exposure more strongly predicts hostility than any other mental health outcome, including depression, PTSD, and anxiety (McDonald & Thomas, 2008).
Domains of Risk Factor Covariates
Family
Although research on the mental health outcomes of exposure to community violence shows a strong association, much of that work does not consider a range of confounding variables that may affect this relationship. For instance, there is an abundance of research suggesting that the impact of exposure is dependent on the qualities of the family. While families are expected to provide for the emotional and physical well-being of their children, those that do not meet these expectations are deemed “risky” (Repetti, Taylor, & Seeman, 2002). Risky families are characterized by a variety of negative attributes, including substance abuse, justice system involvement, mental illness, and parental hostility. In addition, single parenthood is considered a risky family structure that puts kids at a developmental disadvantage.
Studies indicate that exposure to community violence and adverse mental health consequences are not exclusive to children. Parents also suffer from high rates of exposure-related mental health problems (Aisenberg, Trickett, Mennen, Saltzman, & Zayas, 2007), which lead them to model hyperarousal, helplessness, and hostility, while remaining emotionally distant and intolerant of their children (Self-Brown et al., 2006).
Similarly, parental substance abuse exacerbates the exposure–symptomatology nexus due to the presence of many risk factors, including but not limited to intimate partner violence (Kelley et al., 2010), child maltreatment (Amstadter et al., 2011), and greater exposure to dangerous situations (Amstadter et al., 2011). Research also indicates that the combination of growing up in a family where there is parental substance abuse and exposure to violence elevates the potential for adverse consequences well beyond that of each factor individually (Meyerson, Long, Miranda, & Marx, 2002). In addition, parental justice system involvement contributes to family risks by negatively affecting family stability, independent of other family risk factors (S. D. Phillips, Erkanli, Keeler, Costello, & Angold, 2006). As a result, children become particularly vulnerable to impulsivity, anxiety, and depression (Dallaire & Wilson, 2010). Importantly, parental hostility also is considered a particularly pernicious element common to risky families (Repetti et al., 2002). This is verified in both cross-sectional and longitudinal studies showing a strong link between parental hostility and adverse mental health consequences for children (Davies & Cummings, 1998; Rothbaum & Weisz, 1994), including child hostility (Matthews, Woodall, Kenon, & Jacob, 1996).
While research on most of the risky family attributes is robust, studies related to single parenthood equivocate. For instance, research suggests that it is not single parenthood per se that is related to poorer mental health outcomes for children. Rather, it is economic (Waldfogel, Craigie, & Brooks-Gunn, 2010) and overall emotional and general instability that drives the tendency for worse outcomes (Liu & Heiland, 2012), especially child hostility, controlling for both demographic and moderating factors (Waldfogel et al., 2010). It is critical to note that research also shows that whether a family is risky or not does not seem to make a difference in contexts of high violence exposure (Kliewer et al., 2004).
Neighborhood
Neighborhood characteristics, particularly physical and social decay, are tied to negative outcomes for children (Fauth, Leventhal, & Brooks-Gunn, 2004). This is particularly true for the development of hostility (Gorman-Smith & Tolan, 1998), depression (Gorman-Smith & Tolan, 1998; Margolin & Gordis, 2000), PTSD (Martinez & Richters, 1993), and anxiety (Gorman-Smith & Tolan, 1998), independent of other life stressors. Distressed neighborhoods, much like risky families, are less likely to have moderating factors that would buffer children from the onslaught of violent experiences, images, and attitudes that plague these communities, leaving youth more vulnerable to becoming anxious, depressed, traumatized, and hostile.
Peers
Youth exposed to violence are also more vulnerable to the influence of deviant peers. Maschi, Bradley, and Morgan (2008) proposed that violence-exposed children are unable to regulate affect and emotion resulting in problematic interactions with prosocial peers. As a result, these children are more likely to suffer rejection (Lynch, 2003) and turn to companionship with antisocial peers. The elimination of prosocial friendships negatively affects protective factors such as psychosocial maturity (Chassin et al., 2010) and social support (O’Donnell, Schwab-Stone, & Muyeed, 2002), thereby fortifying pathways to adverse consequences (Caspi & Moffitt, 1995).
Academic Factors
While not all children who are exposed to community violence suffer adverse consequences, those with lower IQs and those who drop out of school are more likely to be affected (Losel & Farrington, 2012; Schwartz & Gorman, 2003). Attenuated school bonds (such as dropping out) disrupt normal developmental processes, leaving at-risk children vulnerable to the influence of deviant peers, void of important prosocial support (Sprott, Jenkins, & Doob, 2005), and unable to deal with life stressors (Freudenberg & Ruglis, 2007).
Impulsivity
Although all of the previously mentioned covariates receive considerable support, impulsivity is considered one of the most important emotional dysregulatory risk factors for the development of mental health problems (Loeber et al., 2002), such as hostility (Ferguson et al., 2005) and internalizing symptomatology (Southam-Gerow & Kendall, 2002). It also exacerbates the effects of risky families on child mental health (Katz & Gottman, 1995), independent of neighborhood contexts (Vaszonyi, Cleveland, & Weibe, 2006) and other personality traits (Castellanos-Ryan & Conrod, 2011). Importantly, impulsivity is linked to rejection by prosocial peers (Cassidy, Parke, Butkovsky, & Braungard, 1992) and reduced social competence overall (Repetti et al., 2002).
Early Onset of Problem Behaviors
Research has demonstrated a strong correlation between childhood problem behaviors and a wide range of adverse psychosocial outcomes, including poor mental health (particularly affective and anxiety disorders) and substance use. Co-occurring mental health problems are the norm rather than the exception among children and adolescents with early behavioral problems in both community and clinic samples (see Barkley, 2006). For example, approximately half of youth with early childhood problems have a comorbid anxiety or depressive disorder (Barkley, 2006). These rates of comorbidity are much higher than would be expected by chance, suggesting that early onset of behavioral problems places youth at risk for the development of other mental health problems (Wilens, Biederman, & Spencer, 2002).
Moderating Factors
Although a strong correlation between exposure and adverse outcomes is demonstrated in previous research, some violence-exposed youth evade such consequences (Cicchetti & Lynch, 1993) due to quality social support and individual differences in psychosocial maturation and prosocial belief systems.
Social Support
The role of social support in mitigating vulnerability to mental health problems among adolescents is well documented (see Cohen & Willis, 1985; Rothan, Head, Klineberg, & Stansfeld, 2011; Stice, Ragan, & Randall, 2004). While some studies point to the significance of parental support (Stice et al., 2004), others demonstrate that having a strong attachment to any meaningful adult can reduce the negative effects of violence exposure (Ozer & Weinstein, 2004). Nonetheless, some research suggests that the positive effect of social support may be weak under conditions of high victimization and/or exposure to risk factors across multiple domains (Gerard & Buhler, 2004; Hammack, Richards, Luo, Edlynn, & Roy, 2004).
Religiosity
Similar to social support, religiosity is found to moderate the effects of a plethora of life stressors. However, religiosity is a complex construct and not all dimensions moderate mental health outcomes. One dimension that does receive empirical support, though, is the belief in the importance of religion (James & Wells, 2003). Research suggests that religiosity provides a foundation for self-regulation (Perez, Little, & Henrich, 2009) and positive affect (McCullough & Willoughby, 2009). Religiosity is also associated with greater human agency, leading youth to believe that they accomplish their goals, including problem solving and coping (Perez et al., 2009; Shorkey, Garcia, & Windsor, 2010). It is a particularly strong protector against depressive symptomatology (Koenig, George, & Peterson, 1998) and anxiety (Bergin, Masters, & Richards, 1987), controlling for sociodemographic factors (Perez et al., 2009).
Psychosocial Maturity
A growing body of research argues that the development of psychosocial maturity moderates the relationship between risk factors and mental health problems (Hammen, Brennan, & Keenan-Miller, 2008). With increasing psychosocial maturity, youth become more future-oriented and develop better planning and impulse control, leading to greater self-regulation (Steinberg, 2008). As a result, they become less affected by risky family, neighborhood, and peer influences (Dishion & Patterson, 2006), and are more likely to experience a decline in depression and anxiety (Hammen et al., 2008).
Nonetheless, available research has yet to determine whether commonly identified risk and moderating factors for mental health problems among adolescents not in the justice system also apply to serious juvenile offenders. The current study examines the ebb and flow of risk and moderating factors and whether such changes influence mental health symptomatology.
Method
The present article is a secondary analysis of data from the Pathways to Desistance Project, a multisite longitudinal study of serious juvenile offenders. Beginning in 2000, project staff recruited 1,354 adolescents ages 14 to 18 who were found guilty of a serious (overwhelmingly felony level) offense at their current court appearance in Philadelphia, Pennsylvania (n = 654) and Phoenix, Arizona (n = 700). The number of males adjudicated for a drug offense was capped at 15% of the sample so as to avoid overrepresentation of drug offenders. However, all females who met enrollment criteria were recruited to participate.
Immediately after enrollment, researchers conducted a structured 4-hr baseline interview with each adolescent. The interview included a thorough assessment of the youth’s social background, developmental history, psychological functioning, psychosocial maturity, attitudes about illegal behavior, intelligence, school achievement and engagement, work experience, mental health, current and previous substance use and abuse, family and peer relationships, use of social services, and antisocial behavior.
At each annual follow-up interview (six interviews post-baseline), researchers gathered information on the adolescent’s self-reported behavior and experiences during the prior 12 months, including any illegal activity, drug or alcohol use, and involvement with treatment or other services. In addition, the follow-up interviews collected information about changes in life situations (e.g., living arrangements and employment), developmental factors (e.g., likelihood of thinking about and planning for the future, and relationships with parents), and functional capacities (e.g., mental health symptoms). Information was also gathered from two additional sources: Parent/guardian interviews were conducted near the time of baseline assessment, and official court records were reviewed and coded for criminal history information. There was close correspondence between collateral and court information, indicating acceptable levels of validity. Sample retention for the Pathways Project was high at each follow-up, ranging from 84% to 94% (M = 90%) of the full sample. Additional details regarding the study can be found in Mulvey et al. (2004).
Multiple imputation (MI) was used to address missing data because other strategies for managing missing data (e.g., listwise or pairwise deletion, mean imputation) may result in biased analyses (Bodner, 2008; Graham, 2009; Rubin, 1987). MI entails filling in missing data by computing predicted values based on available data, and then averaging these results across multiple imputed data sets to obtain final estimates for the missing data (Rubin, 1987). Because MI imputes multiple values for each missing value, variability due to both sampling error and model uncertainty is still allowed for, which is an advantage of MI compared with other types of imputation (e.g., single imputation). In addition to the study variables of interest, it is recommended that auxiliary variables that are expected to predict attrition should be included in the MI (e.g., Graham, 2009). Thus, in the MI for the current study, we included sex, age at baseline, study location, ethnicity, mental health outcomes at all follow-up time periods, self-reported offending variety scores at all available follow-up time points, and measures derived from official records (e.g., total number of court petitions prior to and including baseline and total number of arrests during the 7-year follow-up). Following recommendations by Bodner (2008), 20 data sets were imputed using STATA 12. The sample is primarily male (86.4%) and minority (33.5% Hispanic, 41.4% Black, and 4.8% Other). The mean age at baseline is 16.54 years (SD = 1.10 years). All data were based on self-reports by the youth. Table 1 displays the complete list of variables used in the regression analyses.
Descriptive Statistics (N = 1,354)
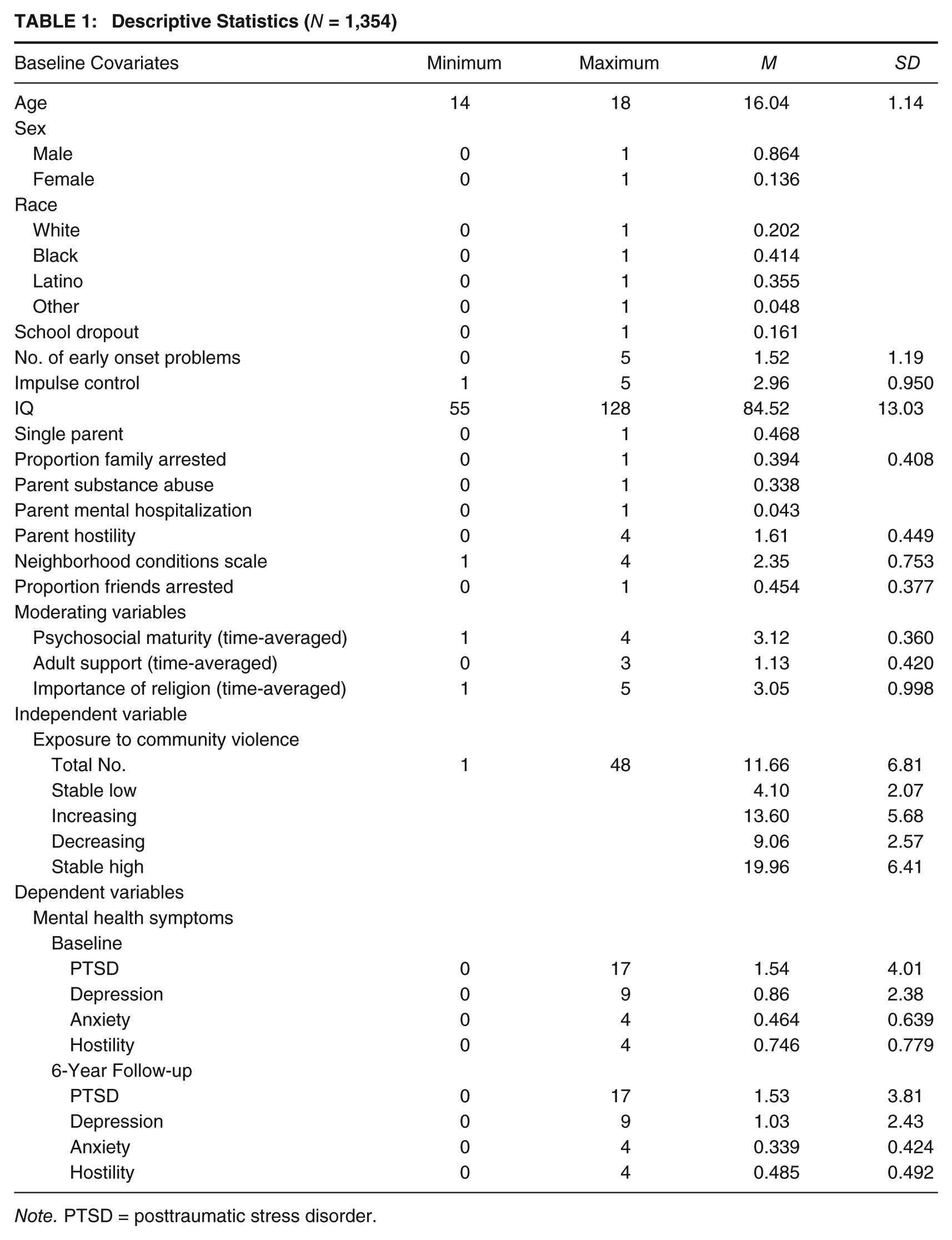
Note. PTSD = posttraumatic stress disorder.
Outcome Measures
Mental Health Problems
Two assessment tools were used to indicate the presence of mental health problems, the Composite International Diagnostic Interview (CIDI; World Health Organization, 1990) and the Brief Symptom Inventory (BSI; Derogatis & Melisaratos, 1983). Two modules from the CIDI were used to assess the past year presence of major depression and PTSD symptoms. Depression and PTSD were measured as the number of symptoms each respondent experienced in the past year prior to the baseline and at the Year 6 follow-up interviews.
The BSI is a 53-item self-report inventory in which participants rate the extent to which they have been bothered (0 = “not at all” to 4 = “extremely”) in the past week by various symptoms. It can be used for both adults and adolescents. Adolescent norms are based on 2,408 individuals (1,601males and 807 females). Derogatis and Melisaratos (1983) reported internal consistency coefficients (Cronbach’s αs) of .71 to .85 and test–retest reliability coefficients of .68 to .91. The current study included two subscales from the BSI designed to assess anxiety (e.g., “feeling tense or keyed up”) and hostility (e.g., “having urges to break or smash things”). Anxiety and hostility were each measured as the mean of the individual items comprising their respective subscales. Confirmatory factor analysis was conducted with the Pathways sample, examining each subscale as a single factor solution. The values generated from this analysis for Anxiety are as follows: χ2 = 161.4, df = 9, root mean square error of approximation (RMSEA) = .11, α = .779. The values generated from this analysis for Hostility are as follows: χ2 = 187.0, df = 5, RMSEA = .16, α = .746. See Appendix A for the distribution of mental health measures.
Key Predictor Variable: Exposure to Violence
The Exposure to Violence Inventory (ETV; Selner-O’Hagan et al., 1998) was modified for this study to assess the frequency of exposure to violent events. Items document the types of violence the adolescent both experienced (i.e., Victim, composed of six items) and observed (i.e., Witnessed, composed of seven items) during the past year. Higher scores indicate greater exposure to violence (see Appendix B for list of scale items).
Risk Factor Covariates: Baseline Measures
Moderation analyses included baseline adjustment (i.e., statistical control) for a number of well-established risk factors to reduce the confounding effects of subject differences and avoid bias due to measurement ceilings or floors. Baseline rather than time-averaged measures were used for two reasons. First, some risk covariates were measured only at baseline (e.g., early childhood problems, school dropout, single parenthood). Second, for most covariates, there was a large amount of missing or invalid data subsequent to the baseline data collection (e.g., neighborhood conditions, proportion of family member arrests, proportion of peer arrests, parental substance use, and impulsivity). In the present study, risk covariates were measured across four domains: individual, family, peers, and neighborhood.
Individual Characteristics
The study included several individual characteristics. School dropout was coded as a dichotomous variable (yes/no). Early onset problems before age 11 was a total count of 5 early onset problems: getting into to trouble for cheating, disturbing class, getting drunk/stoned, stealing, or fighting (range = 0-5). In addition, impulse control was measured with an eight-item Impulse Control Scale from the Weinberger Adjustment Inventory (Weinberger & Schwartz, 1990). Participants rated the frequency with which their behavior in the past 6 months matched a series of statements (e.g., “I stop and think things through before I act”) on a scale from 1 (almost never) to 5 (almost always). High scores indicate greater impulse control. And, intelligence was assessed by the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999), which estimates general intellectual ability based on two subtests, Vocabulary and Matrix Reasoning. Higher total scores indicate greater intellectual ability.
Family Characteristics
In the current study, single parent household was coded as a dichotomous variable (yes/no). This measure includes both female-headed and male-headed single parent households. However, the overwhelming majority of the 459 single parent households were female-headed (87.1%). Family arrests was measured as the proportion of family members who resided with the subject and who had been arrested and/or jailed. Furthermore, parental substance use problems was derived using three anchors: (a) no substance use problem, (b) parent had past drug or alcoholism problem, and (c) parent currently has a substance use problem. The variable was re-coded into a dichotomous variable indicating no substance use problem (0) and has/had a substance use problem (1). The study also included a measure of mental hospitalization, which indicated whether the biological mother or father had ever been hospitalized in a mental hospital (yes/no). And, parental hostility was measured by the Quality of Parental Relationships Inventory (Conger, Ge, Elder, Lorenz, & Simons, 1994) and was adapted for this study to assess the affective tone of the parental–adolescent relationship. The separate mother and father scales were combined into one parent hostility measure. Items from the measure tap parental hostility (e.g., “How often does your mother get angry at you?” “How often does your father throw things at you?”), and participants responded on a 4-point Likert-type scale ranging from “never” to “always.” Higher scores indicate greater parental hostility.
Peers
Peer deviance was measured as the proportion of four closest friends ever arrested.
Neighborhood
Neighborhood disorder was measured using items adapted from other large-scale studies of neighborhood functioning (Sampson & Raudenbush, 1999). Adolescents were asked 21 items about physical and social disorders in the blocks surrounding their homes (e.g., abandoned buildings, gang activity). They responded using a 4-point scale ranging from 1 (never) to 4 (often). Scores are averaged across all items to determine the levels of neighborhood disorder.
Time-Averaged Moderating Variables
The present study followed the work of others (Labouvie, Pandina, & Johnson, 1991; Wiesner & Silbereisen, 2003) who argue that time-averaged covariates may better distinguish among varying groups than using initial covariates. Wiesner and Silbereisen (2003), for instance, found that risks that remain high throughout an entire study period were more salient characteristics of distinctive adolescent groups compared with those that were only high at a single point of time (i.e., the beginning of early adolescence). Therefore, the present study included three time-averaged potential moderating variables in the analysis: psychosocial maturity, social support, and religiosity. Each measure was modeled as a cumulative average across the 84 months of the study.
Psychosocial maturity was measured using the Psychosocial Maturity Inventory (PSMI Form D; Greenberger, Knerr, Knerr, & Brown, 1974). The 30 items assess identity (i.e., self-esteem, clarity of the self, and consideration of life goals), self-reliance, and work orientation. Responses are on a 4-point scale from 1 (strongly agree) to 4 (strongly disagree). Higher scores indicate more maturity. Social support was measured using the Depth of Social Support Scale (J. Phillips & Springer, 1992), in which youth self-reported the number of caring adults (e.g., adults you could talk to if you needed information or advice about something, adults you could talk to about trouble at home, adults with whom you can talk about important decisions, adults you can depend on for help, adults you feel comfortable talking about problems with, special adults who care about your feelings) and indicated whether the sources of support were familial versus non-familial. Higher scores indicate a greater number of relationships with adults who spend time with the adolescent and provide support. And, religiosity, which refers to the subjective importance of religion or the salience of religious identity for an individual, was assessed with the Importance of Spirituality measure (Maton, 1989). This measure contains three items that ask participants to indicate how much their actions are influenced by belief in a god. Responses are on a 5-point Likert-type scale ranging from “not at all true” to “completely true,” with higher scores indicating a greater degree of spirituality. These three items were summed into a single scale score.
Analytical Strategy
Latent class growth analysis was used to identify groups that followed distinctive patterns or pathways of exposure to violence over time. Trajectories were estimated using the Latent Gold 4.5 program. Specifically, the procedure identified distinct groups of participants demonstrating within-group homogeneity in terms of patterns of exposure to violence throughout time and then modeled a separate developmental trajectory for each group. Because analyses were based on count data (the number of exposures to community violence), we used zero-inflated Poisson modeling to account for the clustering at zero (Lambert, 1992). We estimated the probability that each individual belonged to a given group on the basis of the data and simultaneously derived maximum-likelihood parameter estimates associated with membership in each of the defined trajectories (i.e., posterior probabilities of group membership). On the basis of posterior probabilities, individuals were assigned to their most likely group trajectory.
Exposure to violence was examined across six annual measurement points (post-baseline). Data were tested for various numbers of latent classes and the fit of different models was compared with the Bayesian Information Criterion (BIC; Jones, Nagin, & Roeder, 2001). Mixtures of up to six latent classes were considered. The best trajectory solution was determined by three criteria: the lowest BIC value across models, a conceptually clear model, and a model in which each group included at least 5% of the sample. Using the above criteria, we decided on the number of classes and then determined the form of the polynomial (e.g., linear, quadratic, cubic) used to capture the shape of each trajectory. Based on these criteria, the four-group trajectory solution was chosen as the overall best-fitting model for exposure to violence.
The analysis examining the sample for trajectory groups took into account the effect of institutional confinement on the youth’s level of exposure to community violence (Piquero et al., 2001). Exposure time or the amount of time the subject was free to experience exposure to violence in the community was used as a time-varying covariate in the analyses. This value was a proportion indicating the total days during the 6-month recall period that the individual was reported to be in the community. This information was not available for the baseline observation, so these values were set uniformly to 1 for this starting period (Nagin, 2005).
We estimated a series of negative binomial regression models to examine Time 1 predictors (i.e., baseline) of PTSD and depression at Time 2 (i.e., 6-year follow-up). Traditional linear (i.e., least squares) regression models are inappropriate for analyzing count outcomes because count data do not follow or approximate a normal distribution, and thus, analysis from these models can lead to biased and inconsistent estimates (King, 1988). We conducted negative binomial regression analyses because the deviance statistic for a Poisson model indicated overdispersion (when the true variance is bigger than the mean). Ordinary least squares (OLS) was used to model the effects of baseline covariates on the Time 2 mean scores for anxiety and hostility. Both model approaches controlled for the baseline levels of the dependent variable in examining the temporal relationships between violence exposure and mental health symptoms.
Next, we examined whether the main effect of exposure to violence on mental health symptoms was moderated by psychosocial maturity, adult social support, and religiosity. Moderator variables affect the strength and/or direction of the relation between a predictor and an outcome: enhancing, reducing, or changing the influence of the predictor. Moderation effects are typically discussed as an interaction between factors or variables, where the effects of one variable depend on the levels of the other variable in analysis (Aiken & West, 1991). As such, each of the regression models included the interaction between exposure to violence and the respective conditioning variable (i.e., exposure–maturity, exposure–support, exposure–religiosity).
Results
Table 1 displays descriptive statistics for all variables used in the analysis. Exposure to violence was commonplace for this sample of serious adolescent offenders. All respondents were exposed to violence over the 7-year study period. However, 19.2% of the sample (n = 176) had only witnessed violence. Overall, the average number of exposures (direct victimization and witness) was 11.66 and the mean number of direct victimizations was 2.81.
At baseline, 19% of the adolescents in this sample reported one or more PTSD symptoms in the past year, and 12% reported one or more depression symptoms. Approximately 4% of the sample at baseline had moderate to high levels of anxiety and 10.1% had moderate to high levels of hostility.
The trajectories of exposure to violence (Figure 1) reveal a variety of patterns among the youth. Approximately 28% of the sample was on a stable low trajectory, which had consistently low levels of exposure throughout the time period of the study. Group 2, the low-increasing (11%) trajectory, began with low levels of exposure but then showed an increase throughout time. The third group (27% of the sample) had moderate levels of exposure to violence at baseline, but there was a steep decrease in their exposure over the 6-year follow-up period. Finally, 34% of the sample had consistently high levels of exposure to violence.
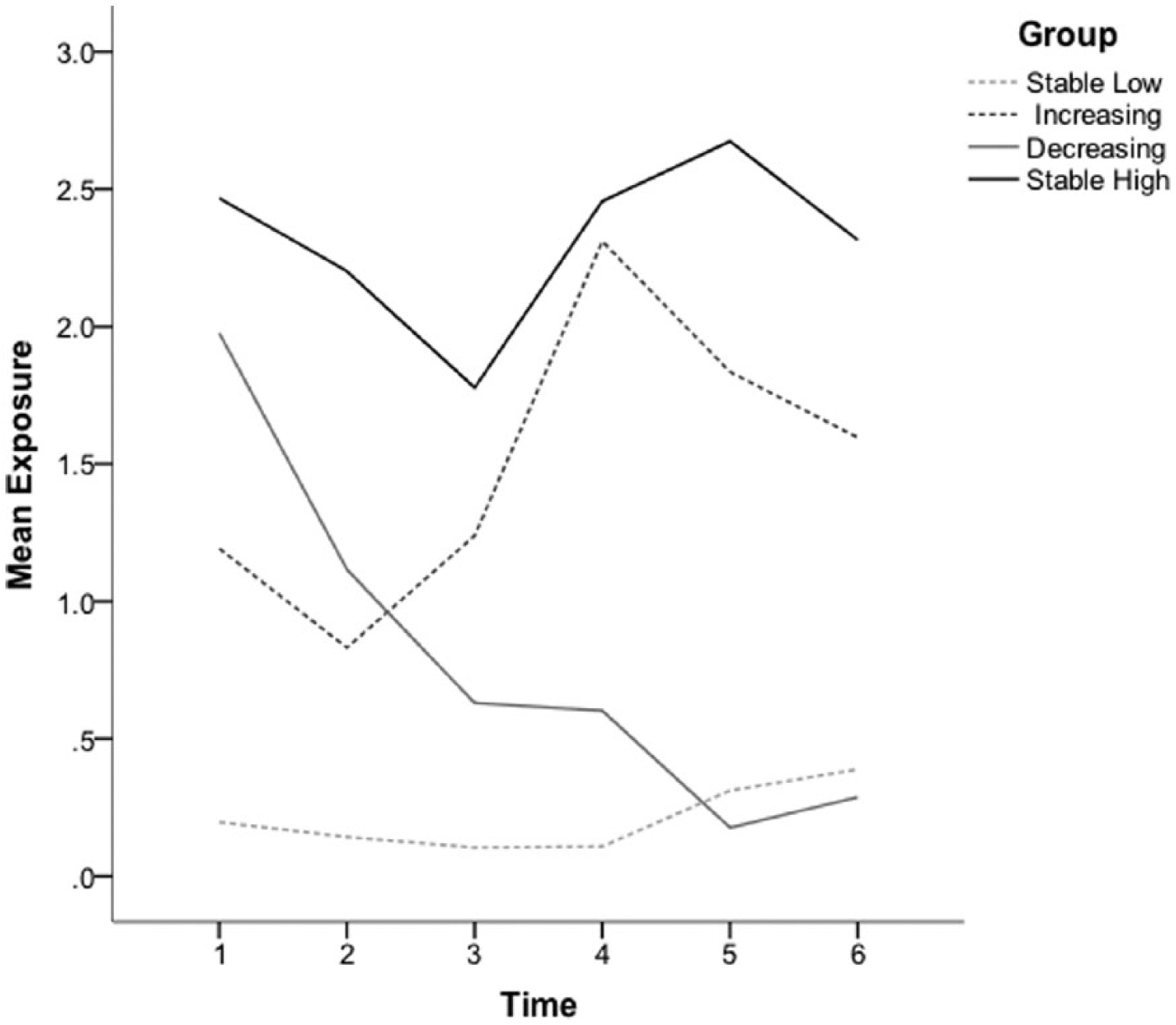
Exposure to Community Violence Trajectories
A multinomial logistic regression, entering all variables simultaneously, was performed to assess the relative associations of the covariates with trajectory group membership. Not surprising, respondents in the increasing exposure and stable high exposure groups resided in neighborhoods with higher levels of physical and social problems and were more likely to be impulsive compared with the stable low group. In addition, youth in the stable high group were more likely to be male, and respondents in the increasing group were more likely to have parents with substance use problems, as compared with the stable low group members. Similarly, participants in both the increasing exposure and stable high groups were more likely to be male and impulsive compared with youth in the decreasing exposure group. The one variable that distinguished the stable high group from the increasing exposure group was impulsivity. Subjects in the increasing exposure group were more impulsive than their stable high group counterparts. Importantly, none of the moderating variables differentiated the trajectory groups. The annual mean exposure to community violence for each trajectory group was as follows: stable high = 2.85, increasing = 1.94, decreasing = 1.29, and stable low = 0.59. Similarly, the stable high group had the highest average annual level of direct victimization (0.66), followed by the increasing group (0.46), decreasing group (0.33), and, last, the stable low trajectory group (0.26).
Table 2 displays the results of the negative binomial and OLS regression main effect models for the four mental health outcomes. As a reminder, PTSD and depression were measured as the number of symptoms each respondent experienced in the year prior to the baseline and in the 6-year follow-up interview. Participants rated the extent to which they had been bothered (0 = “not at all” to 4 = “extremely”) in the past week by symptoms of anxiety and hostility prior to the baseline and again during the 6-year follow-up interview. In all four main effect models, the data showed that those participants with stable low exposure were less likely to have higher mental health symptoms than the stable high exposure group. Specifically, the low-ETV group was 30.4% less likely than the high-ETV group to have a high number of PTSD symptoms. The respective findings for depression, anxiety, and hostility were 49.2%, 37.9%, and 27.9% lower for the low-ETV group as compared with the high-ETV group.
Negative Binomial and OLS Regression Main Effects Model Results: ORs for 6-Year Mental Health Outcomes
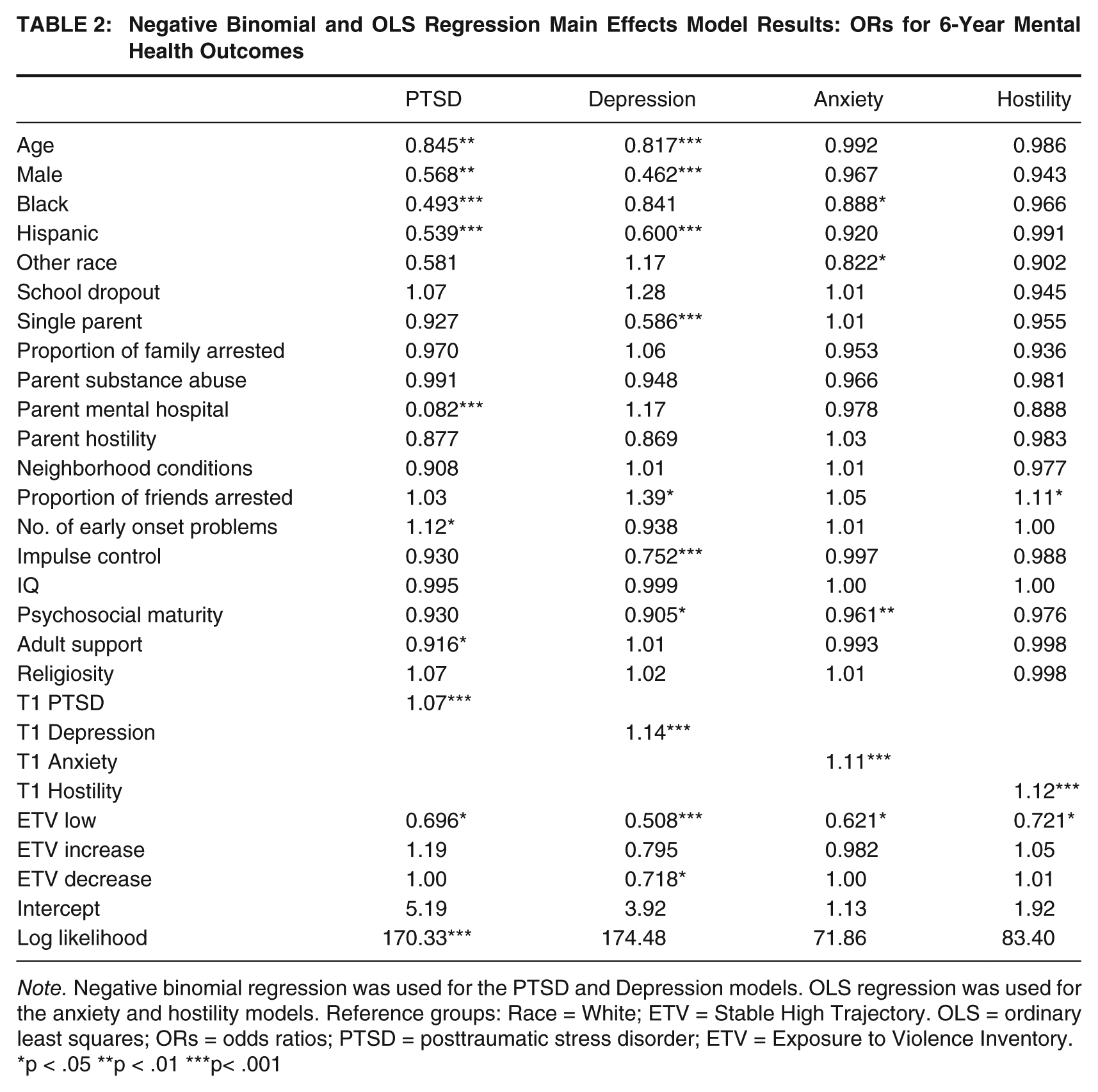
Note. Negative binomial regression was used for the PTSD and Depression models. OLS regression was used for the anxiety and hostility models. Reference groups: Race = White; ETV = Stable High Trajectory. OLS = ordinary least squares; ORs = odds ratios; PTSD = posttraumatic stress disorder; ETV = Exposure to Violence Inventory.
p < .05 **p < .01 ***p< .001
Psychosocial maturity and social support had significant negative effects on symptomatology. Higher levels of psychosocial maturity decreased the likelihood of depression and anxiety symptoms. Higher social support was associated with fewer PTSD symptoms. However, there were no significant main effects for religiosity. In addition, female respondents were more likely to have higher levels of PTSD and depression symptoms, and White sample members had significantly higher levels of PTSD and anxiety symptoms. The early onset of behavioral problems was associated significantly with a greater number of PTSD symptoms.
Finally, in light of the fact that the overwhelming majority of respondents did not report any PTSD (72.8%) or depression (77.4%) symptoms from baseline to the 6-year follow-up, we ran logistic regression models (not shown) comparing the no-symptom groups with the symptoms group. Juveniles in the PTSD symptoms group had higher levels of exposure to violence (odds ratio [OR] = 1.05, p < .001), lower levels of psychosocial maturity (OR = 0.831, p < .010), and were less likely to be male (OR = 0.461, p < .001). More specifically, participants in the stable low-ETV (OR = 0.641, p < .050) and decreasing-ETV (OR = 0.665, p < .050) groups were less likely to have PTSD symptoms. Respondents who endorsed depression symptoms had higher levels of exposure to violence (OR = 1.06, p < .001), had lower levels of psychosocial maturity (OR = 0.866, p < .001), were less likely to be male (OR = .0321, p < .001), were more likely to have a biological parent with mental health problems (OR = 2.14, p < .050), and had parents with greater hostility (OR = 1.59, p < .050). Similar to the PTSD results, youth in the stable low-ETV (OR = 0.580, p < .050) and decreasing-ETV (OR = 0.578, p < .050) groups were less likely to have depression symptoms.
Overall, the main effects results indicated that exposure to violence predicts significantly higher levels of mental health symptoms at the Year 6 follow-up interview. Importantly, the effects of exposure to violence on mental health outcomes were most pronounced for sample members who had a stable high number of exposures to violence.
The direct effects exposure to violence on mental health symptoms may be moderated by certain conditioning variables. To test this, the analyses included interactions of exposure to violence with psychosocial maturity, social support, and religiosity. Specifically, a single interaction term between exposure and a conditioning measure was added to the overall regression model. Each interaction effect was modeled in a separate regression. The results for all interaction effects analyzed are shown in Table 3. The most consistent results were the interactions between the decreasing-ETV trajectory group and psychosocial maturity and social support. Decreasing levels of exposure to community violence combined with higher levels of psychosocial maturity and social support significantly decreased the level of mental health symptomatology. The results also indicated that PTSD symptoms were reduced for the interaction between the stable low-ETV group and higher levels of psychosocial maturity. For certain subgroups of youth, these results suggest that the negative mental health consequences of exposure to violence can be mitigated through psychosocial development and support. As respondents aged into more responsibility and developed adult social bonds, the odds of having higher levels of symptoms decreased with low and decreasing levels of ETV.
Negative Binomial and OLS Regression Moderation Model Results: ORs for 6-Year Mental Health Outcomes
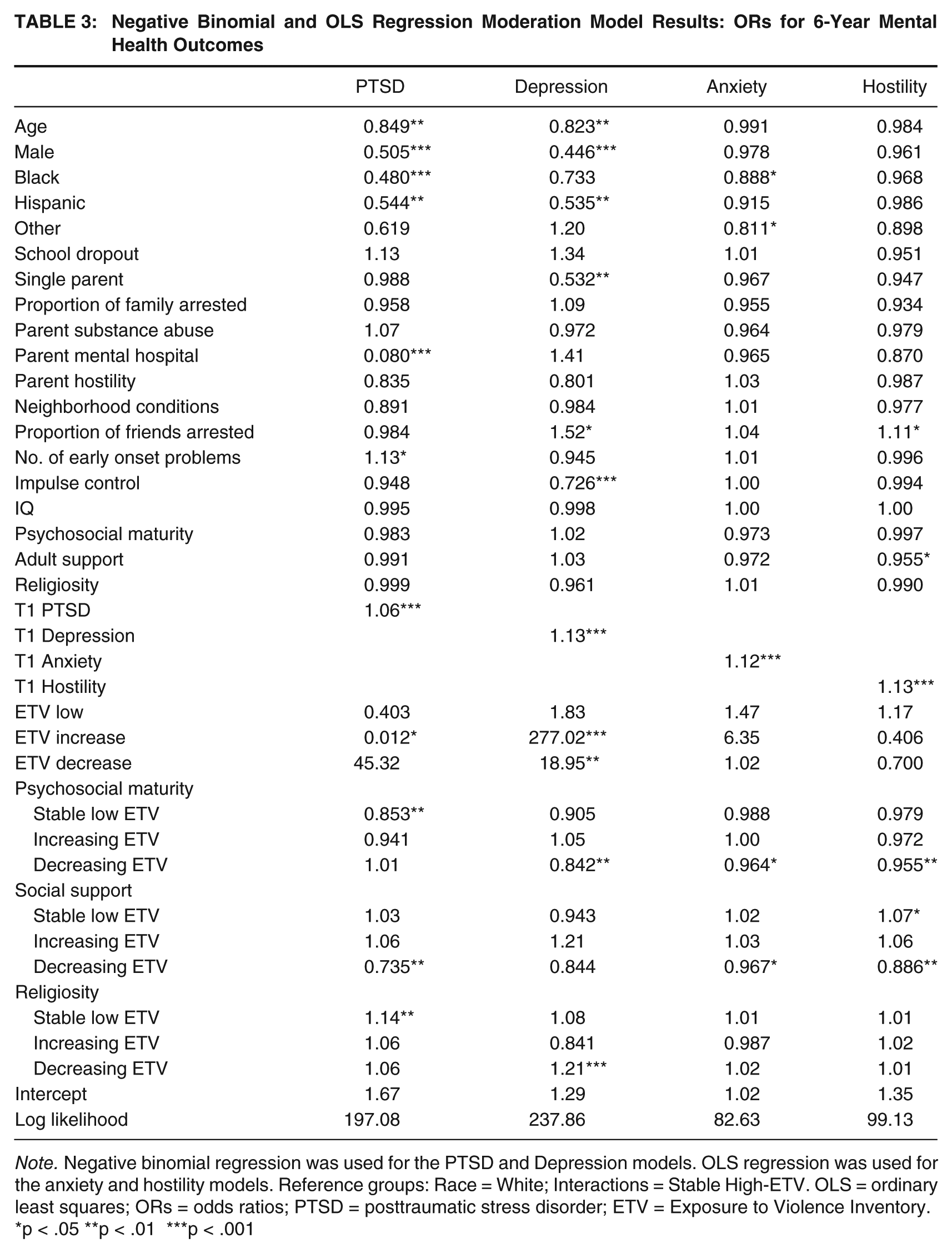
Note. Negative binomial regression was used for the PTSD and Depression models. OLS regression was used for the anxiety and hostility models. Reference groups: Race = White; Interactions = Stable High-ETV. OLS = ordinary least squares; ORs = odds ratios; PTSD = posttraumatic stress disorder; ETV = Exposure to Violence Inventory.
p < .05 **p < .01 ***p < .001
The findings also indicated that a greater number of early childhood problems increased the number of PTSD symptoms. Females had significantly more PTSD and depression symptoms than males; White participants had greater PTSD, depression, and anxiety symptoms than non-White respondents. The race finding is surprising because Black youth had significantly higher exposure to community violence and lived in more distressed neighborhoods than their White counterparts. However, White participants had significantly higher levels of conduct problems, which has been shown to be associated with mood and anxiety disorders (Barkley, 2006).
Discussion
The present study contributes to the ever-growing body of literature concerned with identifying possible mechanisms through which the effects of neighborhood disadvantage are transmitted to juveniles (Conger et al., 1994; Leventhal & Brooks-Gunn, 2004). Although most of the available research relies on samples of community youth, here we focus on a sample of serious juvenile offenders. This subgroup of juveniles is considered to be at high risk for both exposure and related adverse negative mental health and other consequences (Baskin & Sommers, 2013; Cuevas et al., 2007; Odgers, Moretti, Burnette, Chauhan, & Repucci, 2007). However, even within this group, we found substantial variation based on changes in exposure.
Overall, psychosocial maturity and social support did significantly moderate the effects of exposure to community violence on mental health symptomatology, but only for youth on decreasing or stable low trajectories of exposure. Surprisingly, neither religiosity nor neighborhood disorder moderated exposure to the violence–mental health symptomatology relationship. The data also show that youth with stable high exposure are more likely to have more PTSD, depression, and hostility symptoms as compared with youth in the stable low exposure group. Youth who experienced a decline in exposure to community violence over the course of the study also experienced a decrease in depression symptomatology as compared with the stable high exposure group. Importantly, there were no significant differences in mental health outcomes for youth with increasing exposure compared with those with stable high exposure.
The finding of worse outcomes for the stable high exposure group suggests important heterogeneity within this sample of serious youth offenders. Here, the fact that we were able to use a longitudinal approach permitted us to identify a subgroup whose chronic exposure put them at greatest risk for mental health problems. The significant differences in outcomes between the chronic exposure group and the low and decreasing exposure groups highlight the importance of the difference between proximal and distal exposures (Lynch, 2003).
Although, in general, the literature on exposure to community violence associates exposure with symptomatology, the vast majority of youth in the present study reported no or low levels of mental health symptoms. Instead, mental health symptoms were significantly more likely among youth who had both high and direct exposures. This group reported more symptoms related to depression, anxiety, PTSD, and hostility. We attempted to make sense of this finding and discovered that those youth with both the highest exposure to community violence and mental health symptomatology also had deficits in psychosocial maturity, were more impulsive, and were more likely to associate with deviant peers.
The importance of psychosocial maturity for adolescent development is well documented (Cauffman & Steinberg, 2000; Chassin et al., 2010; Monahan, Steinberg, Cauffman, & Mulvey, 2009). As evidenced by a growing body of literature, exposure can affect the timing of developmental processes (Aisenberg & Herrenkohl, 2008; Boney-McCoy & Finkelhor, 1995), leaving children with poorer socialization and self-regulation skills, more impulsive, and lacking in psychosocial maturity. As a result, children exposed to chronic community violence may not be able to complete age-graded developmental tasks that then leave them open to greater alienation from schools, prosocial peers, and adult social support.
Limitations
There are a number of limitations of the present research that are consistent with other studies that use data from the Pathways to Desistance Project. As the study was composed of serious offenders only, the sample is not representative of juvenile offenders as a whole, or of youth in disadvantaged neighborhoods in general. Other limitations of the study include the lack of early childhood measures of exposure to community violence, behavior, and symptomatology, and the absence of data on exposure to violence in the home. Future researchers should seek to disentangle the effects of exposure to violence in the community from exposure to family violence (i.e., abuse and neglect). For example, is abuse and neglect in childhood a precursor of exposure to violence in the community? It is important to note that both conduct and substance abuse disorders were excluded from the present study.
Our analyses included both female and male adolescent offenders; however, it is possible that the trajectories of exposure to community violence differ by sex. Unfortunately, the data set had only a marginally sufficient number of females in the sample (n = 184) to obtain a stable trajectory model for this group, alone (Nagin, 2005). In addition, future research should focus on differentiating neighborhoods by the levels of concentrated poverty and social organization. Research indicates that inner-city children have different patterns of co-occurrence of psychopathology symptoms and related outcomes and live under higher levels of stress, which translates to higher levels of psychopathology than their counterparts living in other urban poor communities (Hay, Hollister, Altheimer, & Schaible, 2006).
Conclusion
Overall, the two most notable findings from the study are as follows: (a) the moderating effect of psychosocial maturity and social support between exposure to community violence and adverse mental health consequences among this sample of serious youth offenders, and (b) the consistently worse outcomes suffered by those youth who experienced stable high exposure to violence. The former finding is not particularly surprising given the strong support in the literature for the moderating effects of psychosocial and social support resources on mental health symptomatology (see Hill, Kaplan, French, & Johnson, 2010, for a review of the literature). However, protective factors that were salient for the stable low exposure group members did not have an impact on our sample of adolescent offenders with stable high exposure. One possible explanation that receives increasing support in the literature is that such factors lose their strength under extreme circumstances and among those with multiple and chronic risk factors (Hammack et al., 2004; Kliewer et al., 2004). Clearly, the youth experiencing chronic exposure to community violence represent one such extreme group.
Findings from the present study are suggestive of important policy and intervention strategies. Key among them is the need to develop specific strategies that target what appear to be unique profiles. The present study also contributes to the development of empirically derived profiles of serious youth offenders. Consistent with the concerns expressed by Snyder (2004), this group of serious, violent juvenile inmates may have difficulty upon reentry. While all of the youth in this study may face the stigma of having been labeled as dangerous, some (particularly those on the increasing exposure trajectory) might find themselves in a situation where their psychological status may exacerbate an already tenuous situation: reentry. Therefore, reentry services should better target the specific needs of this returning subgroup of serious youth offenders, with emphasis on readjusting coping strategies so as to strengthen impulse control. Without such special care, the characteristics that distinguish them from their counterparts on other exposure trajectories may jeopardize their successful reintegration.
It is important to note that research emphasizes that “learned cognitions” (Bandura, 1986; Guerra, Huessmann, & Spindler, 2003) that support the continuation of maladaptive coping are resistant to change. This is suggestive of two strategies, one remedial and the other preventive. In terms of the former, research shows that early intervention to alter children’s cognitions with regard to how they respond can be very useful, especially for those with early signs of emotion dysregulation. Thus, people who work with youth at risk for exposure should routinely screen for such experiences. Second, and it should go without saying, strong efforts to reduce violence exposure, especially among the most vulnerable, would go a long way toward reducing adverse mental health consequences.
Footnotes
Appendix A
Distribution of Mental Health Symptom Scores (N = 1,354)
| Symptom Frequencies | PTSD (count)Baseline | 6-Year Follow-Up | ||
|---|---|---|---|---|
| 0 | 81.0% | 85.9% | ||
| 1-3 | 6.3% | 0.8% | ||
| 4-7 | 2.8% | 2.0% | ||
| 8-10 | 2.5% | 3.1% | ||
| >10 | 7.5% | 8.3% | ||
| Symptom Frequencies | Depression (count) Baseline | 6-Year Follow-Up | ||
| 0 | 88.1% | 85.7% | ||
| 1-3 | 0.2% | 0.2% | ||
| 4-6 | 3.2% | 3.8% | ||
| >6 | 11.6% | 10.4% | ||
| Symptom Frequencies | Anxiety (0-4 scale) | Hostility (0-4 scale) | ||
| Baseline | 6-Year Follow-up | Baseline | 6-Year Follow-up | |
| 0-.99 | 82.7% | 88.1% | 68.4% | 82.7% |
| 1-1.99 | 13.1% | 9.2% | 21.5% | 13.1% |
| 2-2.99 | 2.8% | 2.1% | 8.2% | 3.0% |
| 3-4 | 1.4% | 0.6% | 1.9% | 1.2% |
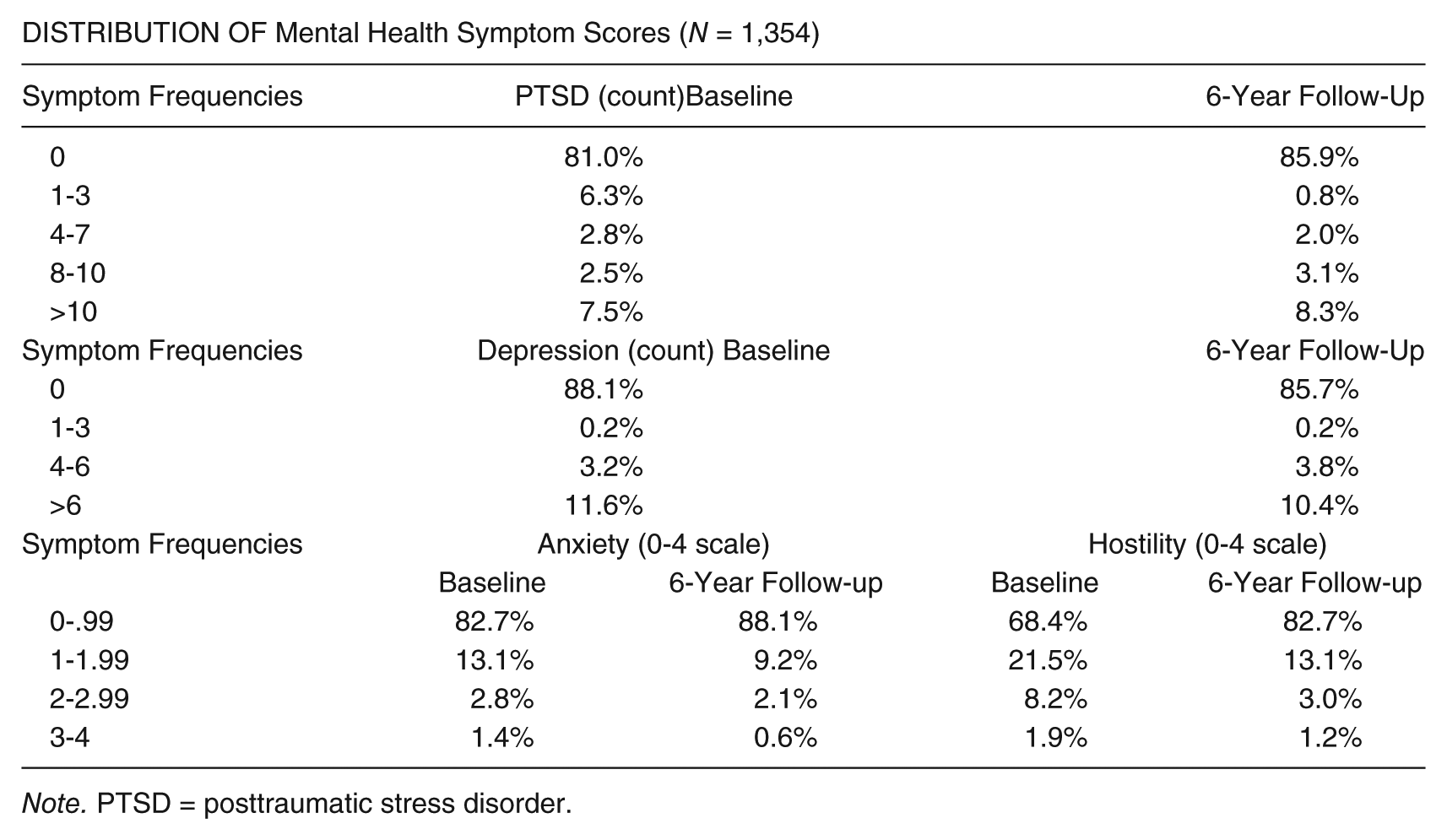
Note. PTSD = posttraumatic stress disorder.