
Abstract
In recent years, there has been a surge in research that examines the relationship between traumatic brain injury (TBI) and involvement in the criminal justice system. However, the bulk of this research has been largely retrospective and descriptive, comparing rates of TBI in the offending population with the rates of TBI in the general population. Although findings from these studies indicate a higher prevalence of TBI in the offending population, virtually no studies have examined whether those with TBI are more likely to recidivate. To address this gap, the present study examined rearrest post release from prison among a cohort sample of Indiana inmates who were screened using the Ohio State University Traumatic Brain Injury Identification (OSU-TBI-ID) instrument. Findings indicate that, net of control variables, those with TBI were more likely to recidivate sooner than those without TBI. Policy implications and directions for future research are discussed.
In recent years, traumatic brain injury (TBI) has been the subject of increasing scholarly attention. Although there have been many definitions of TBI proposed over the years, the most recent consensus suggests it is an alteration in brain function caused by an external force to the head (Menon, Schwab, Wright, Maas, & Demographics and Clinical Assessment Working Group of the International and Interagency Initiative Toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Health, 2010). Thus, TBI refers to disruptions to the normal function of the brain caused by blows or jolts to the head. Moreover, recent definitions recognize that not all head injuries result in TBI but also that the severity of TBI can range from mild (a brief change in mental status or consciousness) to severe (a sustained period of unconsciousness or amnesia). In the United States, an estimated 1.7 million people sustain TBI each year (Faul, Xu, Wald, & Coronado, 2010). As a result of this large number, TBIs have been referred to as a “silent epidemic” as there is little public awareness and because the symptoms of TBI are not always readily evident (Goldstein, 1990). Most adults, at some point in their lives, experience a bump on the head but never experience adverse psychological or behavioral changes from the injury; however, for some individuals, TBI might result in impairments (Ferguson, Pickelsimer, Corrigan, Bogner, & Wald, 2012). Unless these individuals are identified early on, and diverted into appropriate treatment programs, the TBI can lead to a host of negative outcomes such as attention problems, increased aggression, hypersexual behavior, and a lack of impulse control, all of which are particularly salient if the injury occurs during childhood (Eghwrudjakpor & Essien, 2008; Fazel, Lichtenstein, Grann, & Langstrom, 2011; Leon-Carrion & Ramos, 2003; Turkstra, Jones, & Toler, 2003).
Involvement in the criminal justice system is another potentially negative outcome from TBIs that has received attention among researchers. However, much of this research consists of case studies or descriptive samples comparing the offending population with the general population. For example, the rate of TBI in the general population is estimated to be at about 8.5% (Silver, Kramer, Greenwald, & Weissman, 2001) while studies of offending populations have found rates between 25% and 87% (Barnfield & Leathem, 1998; DelBello et al., 1999; Langevin, 2006). Although these results illustrate higher rates of TBI among criminally involved populations, they are not able to assess a causal relationship between offending or reoffending rates as a function of TBI. Moreover, it is possible that offenders with TBI have repeated experiences with the criminal justice system, and so understanding how to screen for TBI is important in helping to deliver appropriate treatment while incarcerated and post release.
The Ohio State University Traumatic Brain Injury Identification (OSU-TBI-ID) instrument was designed for clinical purposes to capture the prevalence and severity of TBI and has been utilized in numerous studies and across a variety of populations, including military personnel, veterans, and prisoners (Bogner & Corrigan, 2009; Corrigan & Bogner, 2007a, 2007b; Corrigan, Bogner, & Holloman, 2012; Ferguson et al., 2012). However, although extant research suggests that the OSU-TBI-ID accurately captures the presence of TBI, it has not been used to determine whether having TBI is associated with subsequent involvement in the criminal justice system.
In this study, we examine data from a statewide cohort of adult male inmates who were screened for TBI, using the OSU-TBI-ID, over a 1-month period in 2012. From this cohort, we follow up a subsample of inmates who were released and returned to the same county (N = 150) to examine whether those with TBI were more likely to recidivate than those without.
TBI and Criminal Behavior
Much of the research establishing a relationship between TBI and criminal behavior comes from descriptive studies that compare rates of TBI in offender populations with those in the general population. Meta-analyses estimate that approximately 60% of adult offenders (Farrer & Hedges, 2011; Frost, Farrer, Primosch, & Hedges, 2013; Shiroma, Ferguson, & Pickelsimer, 2012) and 30% of juvenile offenders (Farrer, Frost, & Hedges, 2013) have TBI compared with 8.5% of the general population (Silver et al., 2001). However, many of these studies have targeted specific populations—homicide offenders (Blake, Pincus, & Buckner, 1995; Freedman & Hemenway, 2000; Lewis, Pincus, Feldman, Jackson, & Bard, 1986), sex offenders (Langevin, 2006), or those with mental health or a substance abuse problem (DelBello et al., 1999; Hawley & Maden, 2003; Martell, 1992; Walker, Staton, & Leukefeld, 2001)—rather than the general offender population. Moreover, sampling strategies have varied considerably with most relying on convenience samples (Blake et al., 1995; DelBello et al., 1999; Diamond, Harzke, Magaletta, Cummins, & Frankowski, 2007; Freedman & Hemenway, 2000; Lewis et al., 1986; Turkstra et al., 2003; Williams, Cordan, Mewse, Tonks, & Burgess, 2010).
Given that the above studies were cross-sectional and descriptive, they are unable to determine a direct causal relationship between TBI and involvement in the criminal justice system leading researchers to speculate about how TBIs lead otherwise law-abiding people to engage in criminal behavior. Biological explanations suggest that damages to certain parts of the brain—namely, the frontal lobe, prefrontal cortex, and temporal lobes 1 —can impair judgment, reasoning, and impulse control, which might contribute to criminal behaviors (Chayer & Freedman, 2001). Damage to this area has been associated with changes in personality traits, attention deficits, short-term memory loss, and impaired learning, speech, and language functions (Barkley, Grodzinsky, & Dupaul, 1992; Bechara & Van der Linden, 2005; Fellows, 2006; Grafman et al., 1996; Pardini et al., 2011). Similarly, damage to the prefrontal cortex has been associated with violence, aggression, and antisocial behavior (Fabian, 2010; Martell, 1996; Raine, 2002), whereas damage to the temporal lobe is linked to unprovoked anger, memory problems, intellectual impairment, and the regulation of responses to cues that indicate threat (Fabian, 2010).
Despite the behavioral changes that can result from TBI, the causal relationship between TBI and crime is likely complex with multiple causal pathways. For example, several studies have found high co-occurring rates of TBI and substance abuse among juvenile and adult offenders (Barnfield & Leathem, 1998; Perron & Howard, 2008; Sacks et al., 2009; Walker, Hiller, Staton, & Leukefeld, 2003; Williams et al., 2010) as well as nonoffender adolescent populations (Ilie, Boak, Adlaf, Asbridge, & Cusimano, 2013). Also, a recent retrospective study among inmates found that TBI early in life was associated with earlier onset of substance abuse and the severity of drug use (Fishbein, Dariotis, Ferguson, & Pickelsimer, 2014). However, such studies are unable to determine a causal relationship, and so it is still unclear whether substance abuse is the result of TBI or, as other studies have suggested, substance abuse is what places one at a higher risk for TBI (Kolakowsky-Hayner et al., 2002; Vickery et al., 2008). A similar line of research which explores a potentially indirect mechanism in the relationship between TBI and crime focuses on mental illness following brain injury. These studies suggest that those with TBI, including both adolescents and adults, are more likely to have symptoms of a psychiatric disorder (e.g., attention deficit hyperactivity disorder [ADHD], bipolar disorder, major depression, panic disorder, depression) as well as increased aggressive behaviors at follow-up (Bloom et al., 2001; Cole et al., 2008; Dinn, Gansler, Moczynski, & Fulwiler, 2009; Gerring et al., 2009; Hesdorffer, Rauch, & Tamminga, 2009; Koponen, 2005; Max, Castillo, Lindgren, & Arndt, 1998; Max, Robertson, & Lansing, 2001; McKinlay, Grace, Horwood, Fergusson, & MacFarlane, 2009; Van Reekum, Bolago, Finlayson, Garner, & Links, 1996). Thus, having TBI might also result in symptoms of mental illness, substance abuse, or violence, which could exacerbate the likelihood of arrest.
TBI and Recidivism
The above studies have documented higher rates of TBI among inmates than the general population and established that TBIs are associated with behaviors that could lead to involvement in the criminal justice system (i.e., violence and substance abuse). However, there have been few prospective studies that examine the likelihood of criminal justice involvement following TBI. The only studies to prospectively look at arrest following TBI use Finnish birth cohort data and find that adolescents with TBI, based on hospital diagnosis, were significantly more likely to have been arrested than those without (Luukkainen, Riala, Laukkanen, Hakko, & Rasanen, 2012; Rantakallio, Koiranen, & Möttönen, 1992; Timonen et al., 2002). Thus, further research is needed to determine not only whether TBI is associated with the initial involvement in the criminal justice system but also whether TBI is associated with subsequent recidivism.
The present research seeks to advance the TBI crime literature by providing the first study to prospectively examine whether inmates with TBI are more likely to be rearrested post release than those without TBI. We used the OSU-TBI-ID—a well-established and validated instrument—to measure the presence of TBI among a cohort of male inmates and link this to follow-up data to assess rearrest post release. Although we are unable to determine whether TBI was associated with initial involvement in the criminal justice system, our study examines an equally important question regarding barriers to prisoners reentering their community, which is the association between TBI and subsequent involvement in the criminal justice system.
Method
Setting
The short version of the OSU-TBI-ID was employed as a screening instrument for all incoming male inmates in Indiana for approximately 1 month. This instrument was designed to provide both a valid and reliable method to assess lifetime exposure to TBI. Indeed, prior research has shown acceptable to high levels of reliability, including both interrater and test/retest reliability (Bogner & Corrigan, 2009; Corrigan & Bogner, 2007a, 2007b; Corrigan et al., 2012; Ferguson et al., 2012). Similar levels of predictive validity have been demonstrated by examining the relationship between lifetime history of TBI and effects that are commonly associated with TBI, including cognitive performance, interpersonal functioning, and violence and aggression (Bogner & Corrigan, 2009; Corrigan & Bogner, 2007a, 2007b; Corrigan et al., 2012; Ferguson et al., 2012). In addition, the OSU-TBI-ID is becoming a widely recognized valid instrument as evidenced by its adoption in a variety of research and clinical practices such as the “TBI Model Systems National Database Syllabus” (National Data and Statistical Center, 2016) and the National Institutes of Health’s “National Institute of Neurological Disorders and Stroke Common Data Elements” (NINDS; 2016). Thus, there is considerable evidence that the OSU-TBI-ID instrument is a reliable and valid method to assess lifetime exposure to TBI.
The instrument is administered through a structured interview lasting approximately 10 min. Individuals are asked to recall injuries involving the head or neck that resulted in altered consciousness or a loss of consciousness. For example, questions include the following: “Have you ever been hospitalized or treated in an emergency room following an injury to your head or neck?”; “Have you ever injured your head or neck in a car accident or from some other moving vehicle accident?”; “Have you ever injured your head or neck in a fall or from being hit by something?”; “Have you ever been injured playing sports or on the playground?”; “Have you ever injured your head or neck in a fight, from being hit by someone, or from being shaken violently?”; “Have you ever been shot in the head?”; and “Have you ever been nearby when an explosion or a blast occurred?” “If you served in the military, think about any combat-related incidents.” For each of the instances, the respondent is also asked how long they were unconscious and at what age the injury occurred. Based on the age of the first injury, number of injuries, severity (i.e., a loss of consciousness), and the length of time unconsciousness, the OSU-TBI-ID places respondents in one of five TBI categories: improbable, possible, mild, moderate, or severe. TBIs that resulted in losing consciousness (excluding, for example, loss of consciousness due to drug overdose) for greater than 30 min are classified as “severe,” while those resulting in periods of unconsciousness lasting less than 30 min are coded as “mild.”
For approximately 1 month, all male inmates entering the Indiana state prison system were screened for TBI at the Reception Diagnostic Center prior to incarceration. Intake specialists gather information on criminal history and medical needs. Based on this information, inmates are then placed into one of several Indiana Department of Corrections (hereafter IDOC) facilities. All intake specialists were trained on how to administer the short version of the OSU-TBI-ID. The instrument was then incorporated into the electronic IDOC intake data collection system from November 5, 2012, to December 3, 2012, in an attempt to determine the overall rate of TBI among 831 male inmates.
In this study, we examine data from a subsample of 155 who were released to Marion County (Indianapolis), Indiana, within 18 months (June 2014) following the OSU-TBI-ID intake survey. Indiana does not have a statewide jail database system so we were only able to capture reliable jail data from Marion County; therefore, for this subsample, we collected prior and follow-up data on all arrests that resulted in jail in Marion County. After listwise deletion of missing cases, our final sample included 151 inmates.
Analytic Procedure
Follow-up incarceration data for the subsample released by June 2014 (N = 151) were collected the following year in August 2015. Our sample, then, had a minimum of 12 months at risk for recidivism. However, most inmates were released earlier than that with the earliest being 2 months following intake screening. Thus, inmates’ risk period for rearrest ranged from 12 to 29 months with an average of 19.9 months (SD = 6.6). We examined time to recidivism using Cox regression survival analysis. One of the strengths of survival analysis techniques is the management of censored data: Left censoring occurs when data on the starting point are not available and right censoring when there are no data on the ending point, which often occurs when studying recidivism. In short, survival analysis methods are able to correct for the unequal distribution of follow-up time by using censored and uncensored (i.e., those that did recidivate) cases to calculate the probability of surviving (i.e., not recidivating) for each time point (Box-Steffensmeier & Jones, 2004). Therefore, it is able to examine both the likelihood of and time to recidivism while also being able to control for the effect of covariates on these outcomes. All analyses were conducted using IBM SPSS 21.
Measures
The dependent variable used in this study was recidivism, which was operationalized as any rearrest that resulted in jail, following discharge from the IDOC. The OSU-TBI-ID screening instrument provided data on the presence and severity of TBI (improbable, possible, mild, moderate, or severe), the likely age of the first TBI injury, and the source of the injury (accident, hit by an object, violence, or explosion). IDOC also provided sociodemographic information on offenders, including age at intake, race/ethnicity categories, and education level. Offense type (person, property, controlled substance, or other) and the presence of a psychiatric disorder (1 = yes, 0 = no) were also provided; unfortunately, additional information on diagnosis was not available nor were data on substance abuse. Inmates were given a mental health screening prior to being sent to a prison facility. This determined whether the inmate had a psychiatric disorder that required additional services and whether this disorder caused functional impairment at the time of intake. Data were only available on whether the inmate had a psychiatric disorder, not on the specific diagnosis. Finally, the criminal history data also provided a total number of lifetime arrests in Marion County as well as a total number of incarceration in IDOC.
Results
Sample Description
The descriptive characteristics are provided in Table 1. All of the participants in this study are males, and the average age at release was 31.2 (SD = 10.0). More than half (60.26%) of the population was identified as Black, 36.42% was White, and 3.1% was Hispanic. However, given the overall small sample size, the small number of individuals identified by IDOC as Hispanic, and well-documented race/ethnic disparities in the criminal justice system, we dichotomized the race/ethnicity categories into “White” and “race/ethnicity minority status” for subsequent analysis. Over half of the sample (53.64%) had either a high school (HS) diploma or General Educational Development (GED) at the time of intake, with 41.72% not having completed HS and 4.64% having some secondary education beyond HS; however, because of the small sample size for the purposes of statistical analysis, we dichotomized the education variable (1 = HS degree or more, 0 = no HS degree). The most common offense type among this cohort was property crimes (41.72%), followed by person crimes (24.50%), controlled substances (16.56%), and other (17.22%). Lifetime prior arrests ranged from 0 to 39 with an average of 6.56 (SD = 6.93). Approximately half (51.66%) of the sample had five or fewer arrests (11.26% had no prior arrest and 4.6% had one arrest). A psychiatric diagnosis was present in 14.57% of the population which is consistent with studies on the prevalence of mental illness among prisoners (Fazel & Danesh, 2002; Steadman, Osher, Robbins, Case, & Samuels, 2009). Finally, over half (53.64%) of the sample had an arrest that resulted in jail following release from prison.
Sample Characteristics (N = 151)
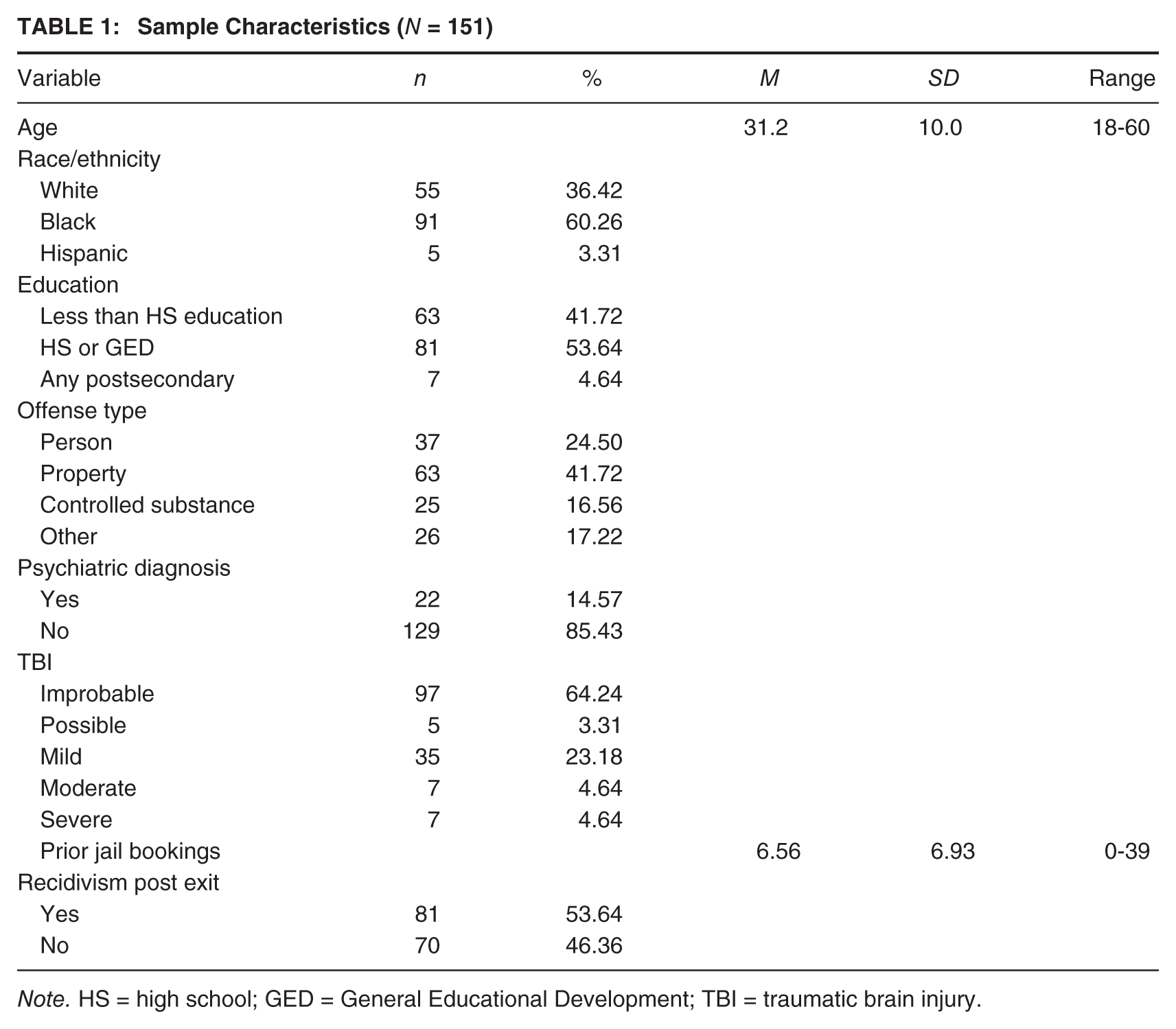
Note. HS = high school; GED = General Educational Development; TBI = traumatic brain injury.
TBI Status
The results of the OSU-TBI-ID screening instrument’s classifications are presented in Table 1 and show that approximately one third of the sample screened positive for TBI. Of those, 9.26% were coded as possible, 64.81% as mild, 12.96% as moderate, and 12.96% as severe. Among those who screened positive for TBI (n = 54), we were also able to examine the age, self-reported prior hospitalization, and indictors of the TBI injury from the OSU-TBI-ID instrument. The self-reported age of the first TBI incident ranged from 3 to 42 years old with an average age of 18.76 years (SD = 9.47); over a third (35.2%, n = 19) had the first TBI incident from age 14 or below. Over three quarters (77.80%, n = 42) reported that they had been hospitalized or seen in an emergency following an injury to the head or neck. For the sources of head- or neck-related TBIs, 45.10% reported being in a car accident; 46.30% reported being hit by something and/or injured playing sports; 33.30% reported being in a fight, being shaken, or shot; and 7.40% reported being in an explosion or blast. Although these were not mutually exclusive categories (respondents can identify multiple sources of injury), over two thirds (68.5%) identified only one, 22.2% identified two sources, and 9.26% three.
To examine potential differences in the sample by TBI status, we dichotomized the categories so that improbable indicated “No TBI” (64.2%, n = 97) and possible, mild, moderate, and severe indicated “TBI” (35.76%, n = 54). Means tests found no differences in TBI status by age, and chi-square tests found no significant differences by race/ethnicity minority status or education by TBI status. However, those with TBI were more likely to have a psychiatric diagnosis than those without TBI (24.1% and 9.3%, respectively, χ2 = 6.10, p = .014), had a greater number of prior lifetime arrests than those without (8.04 [SD = 6.63] and 5.73 [SD = 6.99], t = 2.67, p = .047), and had significantly different offense types. Specifically, those with TBI were more likely to have been incarcerated on person offense type than those without TBI (42.6% and 14.4%, respectively, χ2 = 21.24, p < .001).
Survival Analysis Predicting Recidivism
During the 12 to 30 months of the follow-up period, 46.36% (n = 70) of the sample remained out of the criminal justice system while slightly over half (53.64%, n = 81) of the sample was rearrested. The number of days to recidivism ranged from 9 to 700 days with an average of 221.70 days (SD = 166.75). Survival analyses were used to examine time to rearrest, which produces a life table that describes duration distributions for the full sample or by key variable levels. One way to describe the life table is to plot the cumulative proportion surviving at each time interval by a key covariate. Figure 1 shows the survival function for those with and without TBI, and illustrates that those without TBI went longer until recidivism event. For example, at 6 months, the cumulative proportion of those without TBI who had not yet recidivated (i.e., surviving) was 74.23% compared with 64.81% of those with TBI. Similarly, at 12 months, the survival rate for those without TBI was 62.89%, and among those with TBI, almost half (48.15%) had recidivated.
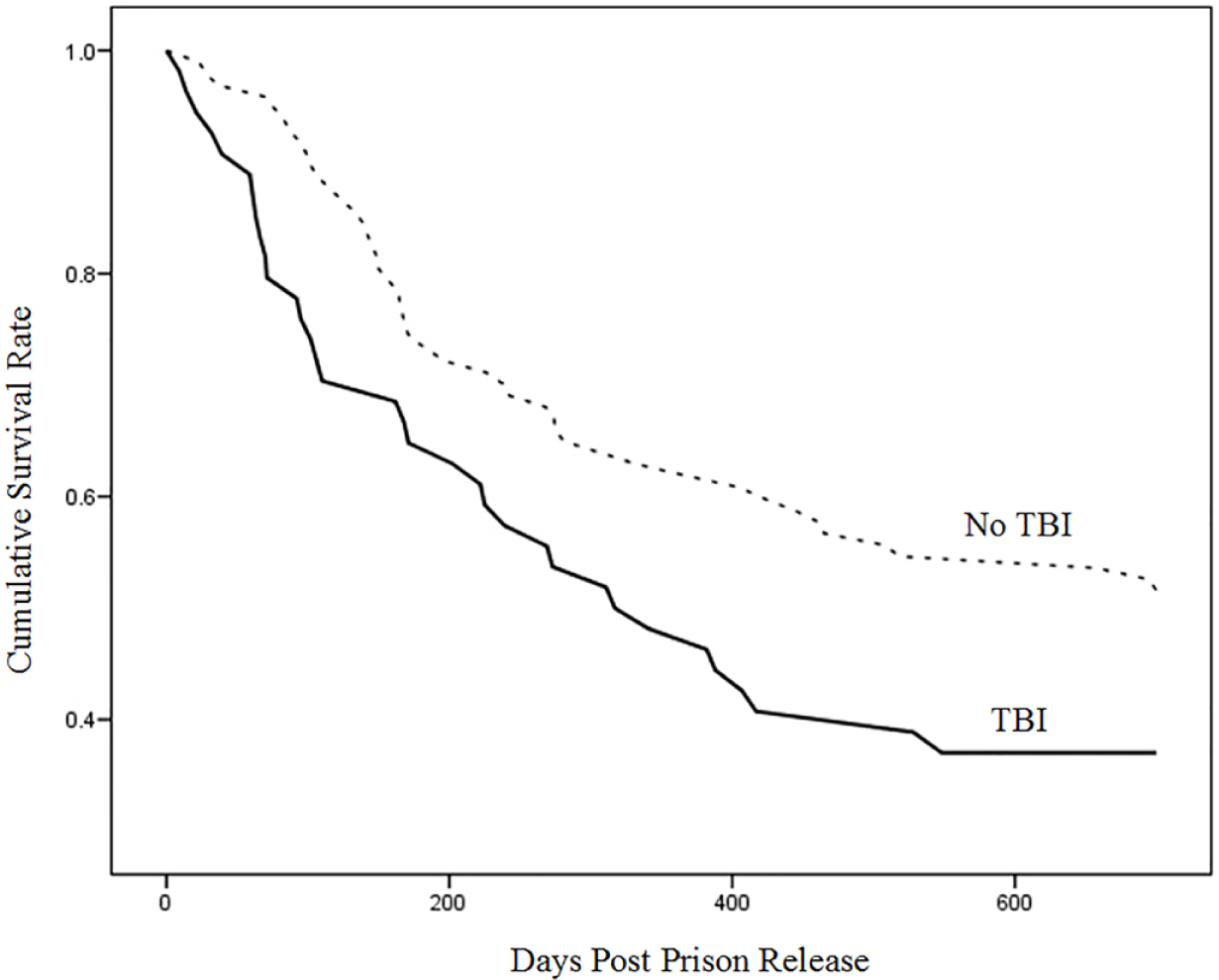
Time to Rearrest Post Prison Release by TBI Status
To assess the effect of TBI on criminal recidivism, while controlling for covariates, we used Cox regression survival analysis. Table 2 shows the results of Cox regression models predicting the time to recidivism. Model 1 includes only the dichotomous TBI variable and suggests that those returning inmates with TBI have a hazard rate of recidivism that is 1.57 times greater than those who did not have TBI (Exp(B) = 0.79). 2 However, we want to assess whether there is an association between TBI and recidivism after controlling for other theoretically important predictors of recidivism. To do this, we included additional measures in subsequent Cox regression models. Model 2 examines the effect of TBI on recidivism while controlling for several sociodemographic variables, including age, race/ethnicity minority status, and education. The results suggest that TBI status and minority status are associated with recidivism. Net of other factors, the hazard of recidivism increased about 69% for those with TBI. Whites were at a decrease hazard of recidivism when compared with minorities (Exp(B) = 0.63).
Cox Regression Predicting Recidivism Post Exit
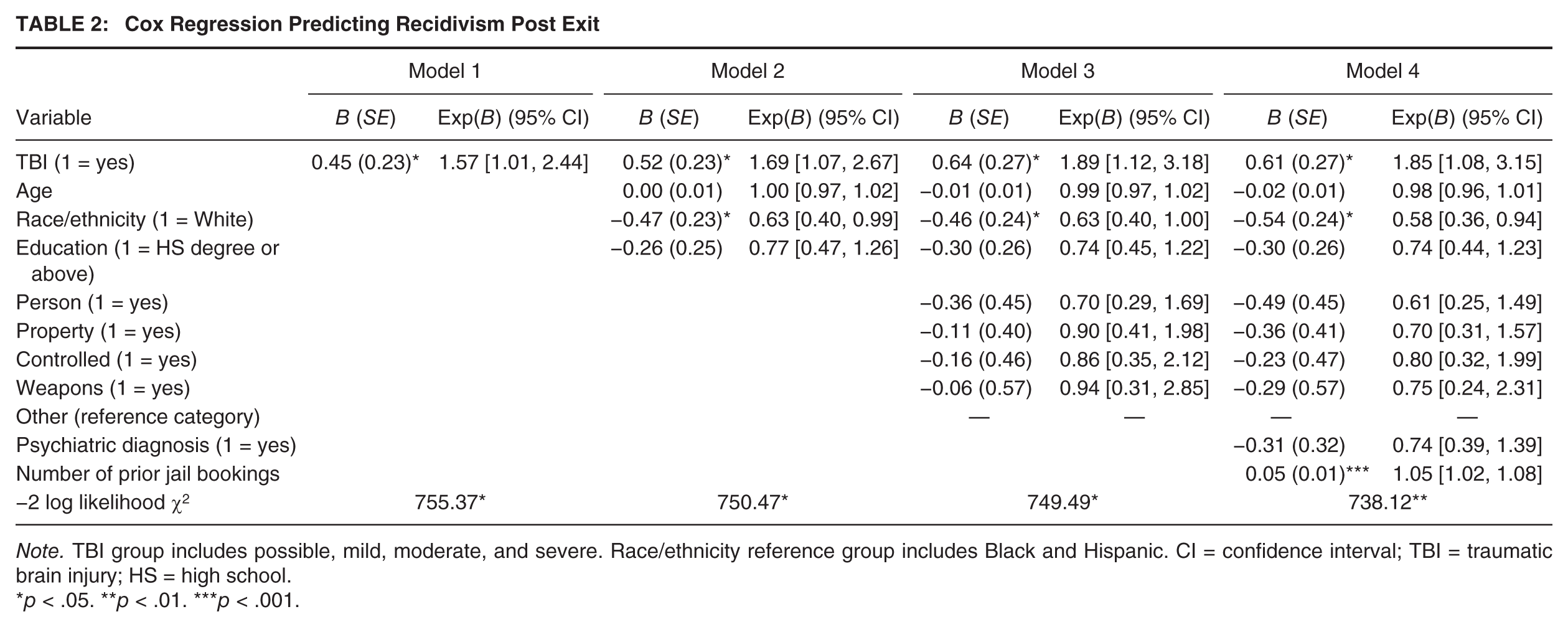
Note. TBI group includes possible, mild, moderate, and severe. Race/ethnicity reference group includes Black and Hispanic. CI = confidence interval; TBI = traumatic brain injury; HS = high school.
p < .05. **p < .01. ***p < .001.
Model 3 includes four additional dichotomous variables measuring each offense type: person, property, and controlled substance, with other offenses as the reference group. Although none of the offense type measures are significant, both TBI status and the dichotomous race/ethnicity variables remain significant. Moreover, adding these variables again increased the effect size of the TBI status variable. Finally, Model 4 includes a dichotomous variable measuring the presence of a psychiatric diagnosis as well as the number of prior arrests. In this final model, TBI status, minority status, and prior arrests are all associated with recidivism. Model 4 suggests that among this sample, controlling for the other variables in the model, the hazard of recidivism increases by 5.2% for each additional prior arrest, is 1.71 times greater for race/ethnicity minority groups and 1.85 times greater for those with TBI.
Discussion
This study uses the OSU-TBI-ID to assess the relationship between TBI and recidivism among male offenders in Marion County, Indiana. Our findings suggest that those with TBI were more likely to recidivate post release than those without TBI. The results of our bivariate analysis indicate that those with TBI did not differ in terms of age, race/ethnicity minority status, or education. However, those with TBI did appear to be more likely to have a psychiatric diagnosis and a greater number of prior arrests than those without TBI. The majority of persons with TBI reported having been hospitalized or seen by a medical professional following their TBI. In addition, individuals with TBI experienced a larger number of arrests for person offenses. This is supported by prior research that suggests that brain injuries are associated with violence and aggression (e.g., Bufkin & Luttrell, 2005; Fabian, 2010; Martell, 1996; Raine, 2002). We then used survival analysis to adequately adjust for the right censored nature of our recidivism measure. Our results suggest that those with TBI were more likely to recidivate, and this relationship held when controlling for other theoretically relevant covariates, including age, race/ethnicity, education, and type of offense. Thus, those with TBI tended to experience an arrest sooner than those without TBI. In addition to TBI, race/ethnicity minority status and the total number of prior arrests were also associated with time to recidivism. These findings are consistent with much of the criminal justice research on recidivism. Prior criminal activity and involvement in the justice system are among the strongest predictors of future criminal behavior in the initial years following release (Gendreau, Little, & Goggin, 1996; Huebner & Berg, 2011; Langan & Levin, 2002; Ulmer, 2001); however, some studies suggest that the effect of prior arrests is no longer significant several years post release (Huebner & Berg, 2011; Kurlychek, Brame, & Bushway, 2007). Similarly, although research finds that recidivism is highest among African Americans (particularly males under the age of 18; see Beck & Shipley, 1989; Langan & Levin, 2002), more recent studies suggest that this pattern is the result of the social context and structural conditions (i.e., racial inequality and poverty rate) to which African American ex-prisoners return (Kaufman, 2005; Kubrin & Stewart, 2006; Reisig, Bales, Hay, & Wang, 2007; Visher & Travis, 2003). Unfortunately, the administrative data used in this study were limited and we were unable to look at long-term recidivism patterns or the social contextual factors to which inmates returned; however, it is important to note the potential explanations for these results.
Our study has several strengths over existing research investigating the association between TBI and involvement in the criminal justice system. First, we use prospective data which allow us to establish the temporal precedence of the variables. Prior research investigating the relationship between TBI and crime has largely been descriptive or retrospective, and compared rates of TBI in the offender population with rates of TBI in the general population. In this study, we were able to first assess the presence of TBI and then determine postincarceration recidivism. However, we were not able to determine whether the TBI occurred prior to their first criminal justice experience. In fact, those with TBI had a greater number of prior lifetime arrests than those without. Although it is possible that prior arrests is also a driving factor in the TBI and recidivism, we found that even when controlling for prior arrests in a multivariate model the presence of TBI was still associated with recidivism. Second, inmates in this study were screened using the OSU-TBI-ID, a validated clinical screening instrument (Bogner & Corrigan, 2009). Prior studies have typically used nonstandardized methods to obtain information on TBIs. Moreover, the OSU-TBI-ID was used as a screening instrument among all incoming inmates in this study. Thus, our study may be more generalizable to the incarcerated population given that much of the prior research has only examined TBI in specific offense types or used convenience samples. Finally, many of the prior studies failed to control for other well-known predictors of criminal behavior, including age, race/ethnicity, and prior criminal behavior.
Although there have been virtually no prospective studies examining the relationship between TBI and involvement in the criminal justice system, our study is consistent with many retrospective, descriptive studies (Barnfield & Leathem, 1998; Langevin, 2006; Ray, Sapp, & Kincaid, 2014; Shiroma et al., 2012) though adds to this body of literature by suggesting that there is a relationship between having TBI while incarcerated and involvement in the criminal justice system following release. However, it is important to note that this association could operate through several mechanisms not measured in this study. For example, recent biological theories have shown disruptions in key areas of the brain posthead injury are responsible for impulse control, the regulation of emotions, and planning and judgment (Raine, 2014). TBI can lead to disruptions in executive functioning such as impulse control affecting levels of self-control, which is a consistent predictor of antisocial behavior and crime (Gottfredson & Hirschi, 1990), or attachments that restrain individuals from engaging in criminal behavior (Hirschi, 1969; Sampson & Laub, 1993), neither of which were measured in the present study. It is also possible that those with TBI become involved in the criminal justice system, not directly because of their TBI but because their social background and TBI serve as barriers to prosocial activities with family and friends. This may lead to difficulties finding sufficient employment or may lead them to self-medicate with alcohol and drugs. On reentering the community, many inmates are ill-prepared for life outside an institution and too often return to disorganized, high-crime neighborhoods lacking supports for housing, employment, social activities, and mental health and substance abuse treatment where they resume antisocial behavior patterns (see Fisher et al., 2014; Hartwell, 2004). Moreover, it is also possible that offending patterns are similar across groups, but those without TBI are better at concealing crimes than those with TBI.
Although the current study fills an important gap in the literature, it is not without limitations. First, we do not have postrelease supervision data on the inmates. In other words, we do not know whether the offenders in our analysis had court-ordered supervisions upon their release from IDOC (i.e., parole), which would affect postrelease criminal behavior and the discovery of those behaviors. For those under supervision, their criminal behavior may be more easily discovered. Second, the sample used in this analysis only consisted of males who returned to Marion County, Indiana. Moreover, our measure of recidivism extended only to this county; while this might adjust for potential regional variations in recidivism, it limits the generalizability of our findings. Extending this study beyond Indiana and including female offenders could increase the generalizability of the findings. Third, while the OSU-TBI instrument is a reliable instrument, there is a potential for recall bias as it relies on retrospective reporting of TBIs from the inmates during the intake screening. There is also concern that inmates may self-report TBIs more or less often than those in the general population. However, recent research shows the validity of TBI self-reports to be fairly consistent when comparing self-reports in the incarcerated population with the general population (Bogner & Corrigan, 2009). Last, we were unable to directly test potential underlying causal mechanisms linking TBI to initial involvement in the criminal justice system or subsequent recidivism. For example, we were unable to measure personality traits or disorders (such as substance abuse, psychopathic traits, or other personality disorders) that might be associated with an increased risk of TBI, arrest, and recidivism. Future research should attempt to examine these specific mechanisms longitudinally to determine whether there is a direct or indirect relationship between TBIs and self-reported criminal behaviors as well as involvement in the criminal justice system.
Conclusion
Only recently have researchers started to examine TBI within a criminal justice context as studies consistently showed higher rates of TBI within incarcerated populations than the general population. Although the results of this study suggest a link between TBI and rearrest following incarceration, perhaps more importantly it highlights both the need and manner by which criminal justice institutions can screen for the presence of TBI. The short version of the OSU-TBI-ID can be easily implemented into existing screening instruments to detect the presence of TBI among inmates. Once inmates are identified, they can be placed into programs that address their individual needs and develop proper intervention strategies. If inmates get the appropriate treatment for brain injuries while incarcerated, they may be less likely to engage in criminal behavior after release. Moreover, detecting TBI as early as possible in the criminal justice process could reduce the burden of TBI on initial and repeat offending.
Footnotes
We would like to thank Brooke Hiltbold, Spencer Lawson, and Jennifer Lutz for their help in collecting and preparing the data for analysis.