
Abstract
Black girls bear a higher burden of juvenile justice involvement in the United States, relative to other racial/ethnic female groups. Emerging evidence suggests that system involvement is related to trauma histories and post-traumatic stress disorder (PTSD). This study investigated the associations between individual, family, and peer factors, and their relationship to PTSD among Black girls with juvenile justice involvement. Cross-sectional data were collected from 188 Black girls in detention. Measures assessed were history of abuse, negative peer norms, future orientation, caregiver support, self-esteem, age, and PTSD symptoms. Major regression findings indicated that higher rates of caregiver support, higher negative peer norms, lower self-esteem rates, and lower future orientation rates were correlated with greater PTSD symptoms. Treatment programs for this population warrant a multisystemic approach, which includes caregivers and peers, and bolstering important constructs such as self-esteem and hopefulness.
Girls are the fastest growing group in the United States juvenile justice system, accounting for a third of all juvenile arrests (Kerig, 2018; Tam et al., 2019), and Black girls are overrepresented in the juvenile justice system when compared with their other racial/ethnic female counterparts (Hockenberry & Puzzanchera, 2017; Office of Juvenile Justice and Delinquency Prevention [OJJDP], 2019). Black girls aged below 18 years accounted for about 35% of all justice-involved girls although they comprise only 14% of the national population of American girls (OJJDP, 2019; Sickmund et al., 2020; Vafa et al., 2018). Justice-involved youth are disproportionately affected by post-traumatic stress disorder (PTSD), compared with youth with no such histories (Abram et al., 2013; H. J. Rosenberg et al., 2014). In addition, the association between abuse and/or polyvictimization (i.e., multiple forms of abuse) and PTSD has been more pronounced for adolescent females than males (Kerig, 2018).
Little information exists related to trauma experiences and sequelae for Black juvenile justice–involved girls. Establishing correlates of PTSD is a first step to inform and develop prevention and intervention strategies and services within and outside the justice system to address their criminogenic needs (Andrews & Bonta, 2010b). This study addresses this gap in the extant literature by examining the degree to which history of abuse, negative peer norms, future orientation, caregiver support, and self-esteem correlate with PTSD symptoms among Black girls with juvenile justice involvement. The selection of these variables was informed by the extant literature and theoretical considerations.
History of Abuse and PTSD
High numbers of girls in the juvenile justice system self-disclose trauma and victimization, putting them at risk for PTSD and psychosocial and behavioral problems, especially those who have been polyvictimized (Charak et al., 2019; Ford et al., 2013; Kalu et al., 2020; Kerig, 2018). According to the Survey of Youth in Residential Placement, 42% of girls versus 22% of boys in juvenile custody reported previous physical abuse. Similarly, 35% of girls versus 8% of boys reported past sexual abuse (Sedlak & McPherson, 2010). Moreover, approximately 40% of Black females report experiencing coercive sexual contact by the age of 18 years, reflecting a high rate of sexual trauma among girls of color (Women of Color Network, 2006).
There is an established link between victimization and juvenile justice involvement among girls (Ford et al., 2013; Kerig, 2018; Yoder et al., 2019). In addition, childhood sexual and physical abuse and neglect often precede and are strongly correlated with offending behavior (Ryan et al., 2013). Croysdale & colleagues (2008) found that girls were polyvictimized at a much higher rate (39%) than boys (19%) in their study. In addition, Pereda & colleagues (2017) noted that girls reported that they were more victimized by their caregivers in the previous year versus the boys in the sample (47.4% and 18.3%, respectively). Furthermore, girls reported psychological/emotional victimization (31.6%) and sexual abuse (42.1%) more than boys who were either psychologically (or emotionally) abused (11.0%) or sexually abused (9.8%). In a latent class analysis conducted by Charak and colleagues (2019), there were more girls than boys in the polyvictimization class, who reported multiple forms of victimization and violence exposures across physical, psychological, family, and sexual domains. Participants in this class also indicated high levels of emotional dysregulation, PTSD symptoms as per the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994), and other mental health symptoms such as depression, anxiety, somatic complaints, and suicidality. Although abuse and polyvictimization are closely related to youth delinquency, few studies have investigated the correlates of PTSD among Black girls with juvenile justice involvement.
PTSD symptoms are also positively associated with poor physical and mental health outcomes and multiple traumas, and these symptoms are commonly experienced by girls who are overrepresented within the juvenile justice system (Bennett et al., 2016; Gagnon et al., 2017; Kerig & Becker, 2012; Walsh et al., 2012). Different forms of victimization are associated with coping and survival strategies, such as aggression, substance abuse, self-harm, running away, sex trafficking, and associating with antisocial peers for survival, which can lead to juvenile justice involvement (Feiring et al., 2013). Moreover, survival coping, which in turn results in self-defense as a response to their trauma, could be misinterpreted by law enforcement or other authority figures as nonconforming behavior that is threatening to others. This misinterpretation is influenced by culture, social stigma, gender, and racial stereotypes, which disproportionately affects Black girls (Morris, 2016).
Caregiver Support and PTSD
Caregiver figures—partly through the provision of support—exert strong influence in the lives of their youth (Miller-Graff, 2016). In addition, the mental health and well-being of children and youth’s caregivers is an important factor in their overall functioning (Hagan et al., 2017). Such supports are even more central when youth are troubled, distressed, or reside in economically disadvantaged neighborhoods (Kiser et al., 2010). Black families generally encourage stronger parent–child attachment (Arbona & Power, 2003). Prior studies involving Black girls suggest that lack of parental social support might correlate with poorer overall youth well-being (Bradley & Corwyn, 2000; Sun et al., 2020). In a study of girls from a national sample of adolescents and their parents, Black girls were less likely to display externalizing behavior if they also reported high rates of parental attachment (Kalu et al., 2020). Children and youth with histories of abuse—especially sexual abuse—who have supportive caregivers may show decreased levels of symptoms despite the abuse severity compared with those who have less supportive caregivers (Wamser-Nanney et al., 2020). However, support is not always positive; caregivers’ reactions to trauma (especially those who have histories of high trauma exposure) may be most important to youth symptom presentation (Lieberman et al., 2005). Furthermore, youth who are recipients of caregiver support (e.g., emotional, financial, or informational) might be pressed upon by caregivers to conform to certain behaviors or standards that might engender strife and emotional distress on the part of adolescents. Moreover, the more distraught and diminished the coping of the parents or caregivers, the greater the chance for adverse outcomes in children and youth exposed to trauma and/or abuse (Cicero et al., 2011). Consequently, girls who experience problematic caregiver support could have increased PTSD symptoms. Another possible hypothesis is that during times of stress, youth might come to depend on and expect support from caregivers. However, when stressors exceed existing caregiver supports, youth might display more PTSD symptoms (Patterson, 2002).
Negative Peer Norms and PTSD
A plethora of research has consistently shown that negative peer norms are associated with a wide range of negative youth behavioral and psychological outcomes (Janssen et al., 2016; Kerig & Becker, 2010; Voisin & Kim, 2018). Participation in deviant or antisocial peer groups has been associated with rejection from society and further affiliation with negative peer groups (Kerig & Becker, 2010; Voisin & Kim, 2018). Youth who are involved with a network of peers who endorse negative norms are more likely to be engaged in risky behaviors (Voisin & Neilands, 2010).
Youth who affiliate with others who are gang involved may experience more violent episodes resulting in PTSD symptoms (Harris et al., 2013). McGee and Foriest (2009) identified a direct relationship between negative peer affiliation and delinquency among African American female youth, and those who reported delinquent behaviors were more likely to have female peers who had been suspended and/or arrested. Their relationships with delinquent girls resulted in a greater influence on their views about criminal behavior and led to escalated disorderly behavior. Similar to other research study findings, some girls sought out these peers for protection during a fight or other illegal activity (Jones, 2009). This further indicates a direct relationship between victimization (abuse/trauma) and offending among this population (McGee & Foriest, 2009; Yoder et al., 2019). Consequently, girls with trauma histories are more likely than their counterparts without such violent exposures to socialize with antisocial peer groups (Adams & East, 1999), thereby further exacerbating dangerous behaviors leading to trauma exposures and PTSD symptoms.
Self-Esteem, Future Orientation, and PTSD
Psychological factors, such as self-esteem (i.e., internal self-beliefs) and perceived life chances (i.e., hope for the future), have generally been correlated with more positive mental health outcomes (McDade et al., 2011). Future orientation—a common proxy term for perceived life chances—are thoughts, expectations, and dreams that people possess for their future that produce motivation and hope (McDade et al., 2011). The concept of a positive future could foster behaviors focused on positive goal attainment (Oyserman et al., 2004).
A study of low-income Black youth residing in violent neighborhoods found that higher levels of future orientation were correlated with lower psychosocial risk distress factors. Within the same sample, youth who reported greater future orientation—even in the presence of economic and social disadvantage—had better mental health outcomes (So et al., 2016). Similarly, other research has corroborated this finding and has shown that higher levels of perceived life chances and self-esteem are positively associated with better mental health outcomes (Mann et al., 2004). It is plausible that youth who display high levels of self-esteem and future orientation might engage in more mental filtering that could circumvent higher levels of mental distress and curtail PTSD symptoms.
Purpose of This Study
Few studies have explored individual, peer, and family constructs and their relationship to PTSD symptoms across a single sample of Black girls with histories of juvenile justice involvement. These constructs are significant for all youth; however, they have particular cultural and social significance for Black girls with histories of juvenile justice system involvement. These youth often reside in high-need, under-resourced communities and, as we have shown in the above summary, these factors have particular relevance to PTSD symptoms, indicating a push for rehabilitation and treatment based on the criminogenic needs of this underserved and understudied population.
This study examines the correlates of trauma among Black, juvenile justice–involved girls. It also investigates a novel potential correlate, future orientation. We hypothesized that future orientation, self-esteem, and caregiver social supports would be associated with lower PTSD symptoms. Similarly, higher levels of negative peer norms and abuse history would correlate with greater PTSD symptoms. Age is highly correlated with many of the variables in this study and would be controlled for in all analyses (Kerig et al., 2016; So et al., 2016).
Method
Participants
The secondary data for the current analysis came from a parent study called Imara that was a randomized controlled study designed to test the efficacy of a sexual risk reduction intervention. Specifically, the intervention intended to decrease the incidence of sexually transmitted infections, improve HIV-preventive behaviors, and enhance psychosocial outcomes for Black females in a juvenile detention center (Davis et al., 2016; DiClemente et al., 2014; Kim et al., 2020; Logan-Greene et al., 2018). The full efficacy study is described in detail elsewhere (DiClemente et al., 2014). Data for this study were drawn from the baseline data. Eligibility criteria for the study participants consisted of girls who self-identified as African American or Black, were aged 12 to 17 years, were currently residing in the local detention center, were not in steady relationships, were not pregnant or wanting to be pregnant, and who self-reported having vaginal intercourse prior to detention (Davis et al., 2016).
Procedures
In the Imara study, written informed assent for study participants was obtained from adolescents and verbal consent was obtained from parents prior to implementation of any study procedures. Data collection was completed while girls were still in detention. Subsequently, 93% (N = 188) of the eligible participants enrolled in the study. Participants completed surveys using audio computer-assisted self-interviewing (ACASI) technology, which has been proven to reduce selection bias and may help with literacy problems. ACASI is self-administered, enhances confidentiality, enhances accurate recall using timeline follow-back techniques, and identifies inconsistencies in the client’s self-report to prompt them to resolve the discrepant data (Kim et al., 2020; Kissinger et al., 1999; Logan-Greene et al., 2018). This study is a secondary analysis of exempt data, so no further IRB approval was required.
Measures
All study measures were selected based on the underlying theory and empirical evidence for their utility and satisfactory psychometric properties demonstrated in other studies with similar populations. All study measures were previously validated with this population (Wingood & DiClemente, 2002).
PTSD Symptoms
PTSD symptoms were measured using a modified self-report version of the PTSD Symptom Scale Self-Report Version (PSS-SR; Foa et al., 1993; Sun et al., 2020), which includes 17 items. To assess presence and severity of PTSD symptoms, participants responded to items, such as “Having bad dreams or nightmares about the trauma” and “Reliving the trauma, acting or feeling as if it was happening again,” describing the frequency and severity of problems (0 = not at all or only one time to 4 = 5 or more times per week/almost always; range = 17–68). Using a PSS-SR total score of 14 as a cutoff was considered clinically elevated (Coffey et al., 2006). The PSS-SR has been used with Black girls and demonstrated good psychometric properties (Gray et al., 2016). Cronbach’s alpha for the scale is .94.
History of Abuse
History of abuse was a measure of cumulative childhood abuse that is specific to abuse and does not include other forms (e.g., neglect) of victimization. This measure was created in the larger study to assess participants’ demographic and behavioral factors (So et al., 2016). The items have been used in prior research and measured three dichotomous variables: physical, emotional, and sexual abuse (Logan-Greene et al., 2018). Participants responded to questions, such as “Have you ever been emotionally abused?” “Have you ever been physically abused?” and “Has anyone ever forced you to have vaginal sex when you didn’t want to?” Response category was 1 (yes) or 0 (no). Responses were summed to a 3-point scale (range = 0.1–3.0) with higher scores indicating more abuse. The Cronbach’s alpha for this scale was .66.
Caregiver Support
Caregiver support was measured with 10 items. These items have been used in prior research (Logan-Greene et al., 2018; α = .858). Participants responded to items such as “I can count on my primary caregiver when I need to get something off my chest” and “Talking about my problems with my primary caregiver makes me feel ashamed or foolish.” Response categories ranged from 1 (never) to 5 (always), where higher scores indicated more caregiver support. Three items were negatively scored, so they were reversed scored. The Cronbach’s alpha for this scale was .86.
Negative Peer Norms
Negative peer norms were measured using a modified version of a 17-item scale (adapted from Elliott et al., 1985). The Items have been used in prior research (Logan-Greene et al., 2018; α = .918). Participants responded to questions like “How many of your friends engage in the following behaviors: skipping school, stealing, using drugs or alcohol, and hitting people?” Response categories for each question ranged from 0 to 3 (0 = none of them, 1 = some of them, 2 = most of them, 3 = all of them) and were summed into a final scale (range = 0–51). Higher scores indicated more support from deviant peers. The Cronbach’s alpha for this scale was .92.
Future Orientation
Future orientation was measured with a modified 10-item scale (Whitaker et al., 2000), with items derived from Coopersmith’s Self-Esteem Inventory (Coopersmith, 1967). Items from the modified scale have been adapted and used in prior research (So et al., 2016; α = .65). Examples of items were “You will graduate from high school” and “You will be respected in your community.” Response categories ranged from 1 (very low) to 4 (really high), where higher scores indicated higher future orientation (range = 6–40). The Cronbach’s alpha for this scale was .95.
Self-Esteem
The girls’ self-esteem was measured using 10 items of the Rosenberg Self-Esteem Scale (Logan-Greene et al., 2018; M. Rosenberg, 1965 α = .843). Examples of items were “I feel that I have a number of good qualities” and “I feel that I am a failure,” with response categories ranging from 1 (strongly disagree) to 4 (strongly agree), where higher scores indicated greater self-esteem (range = 13–40). The Cronbach’s alpha for this scale was .90.
Age
Age was used as a continuous variable.
Data Analysis
Univariate analyses were computed to describe all study variables (see Table 1). Next, bivariate correlation analyses were conducted to examine the associations between all study variables: PTSD symptoms, history of abuse, caregiver support, negative peer norms, self-esteem, future orientation, and age (Table 2). Next, a multiple regression analysis was conducted where all independent variables (i.e., history of abuse, caregiver support, negative peer norms, self-esteem, future orientation, and age) were entered simultaneously into the model to determine their relationship to the dependent variable PTSD symptoms, controlling for the effects of age (Table 3). The regression model was conducted with the total score of PTSD symptoms as the outcome variable associated with the independent variables. Post estimation tests were conducted to assess for multicollinearity and the results indicated the absence of collinearity. All analyses were completed using Stata 15.
Descriptive Statistics (N = 188)
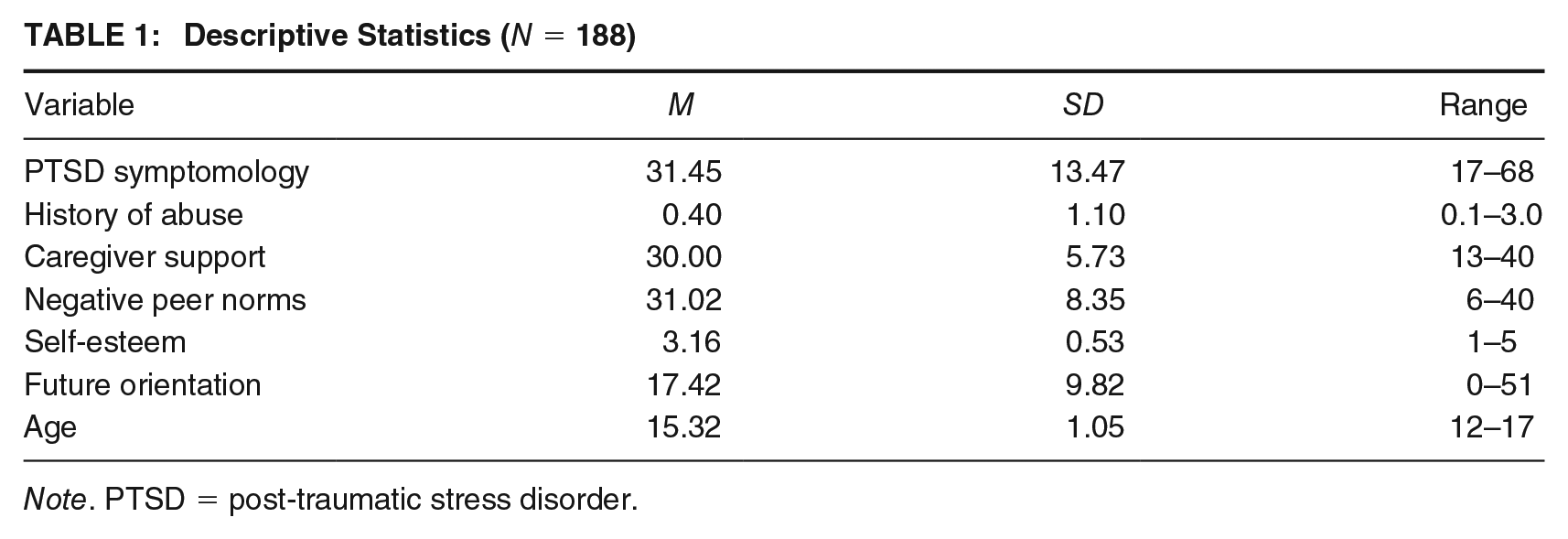
Note. PTSD = post-traumatic stress disorder.
Mean Values, Standard Deviations, and Bivariate Correlations of the Study Variables (N = 188)
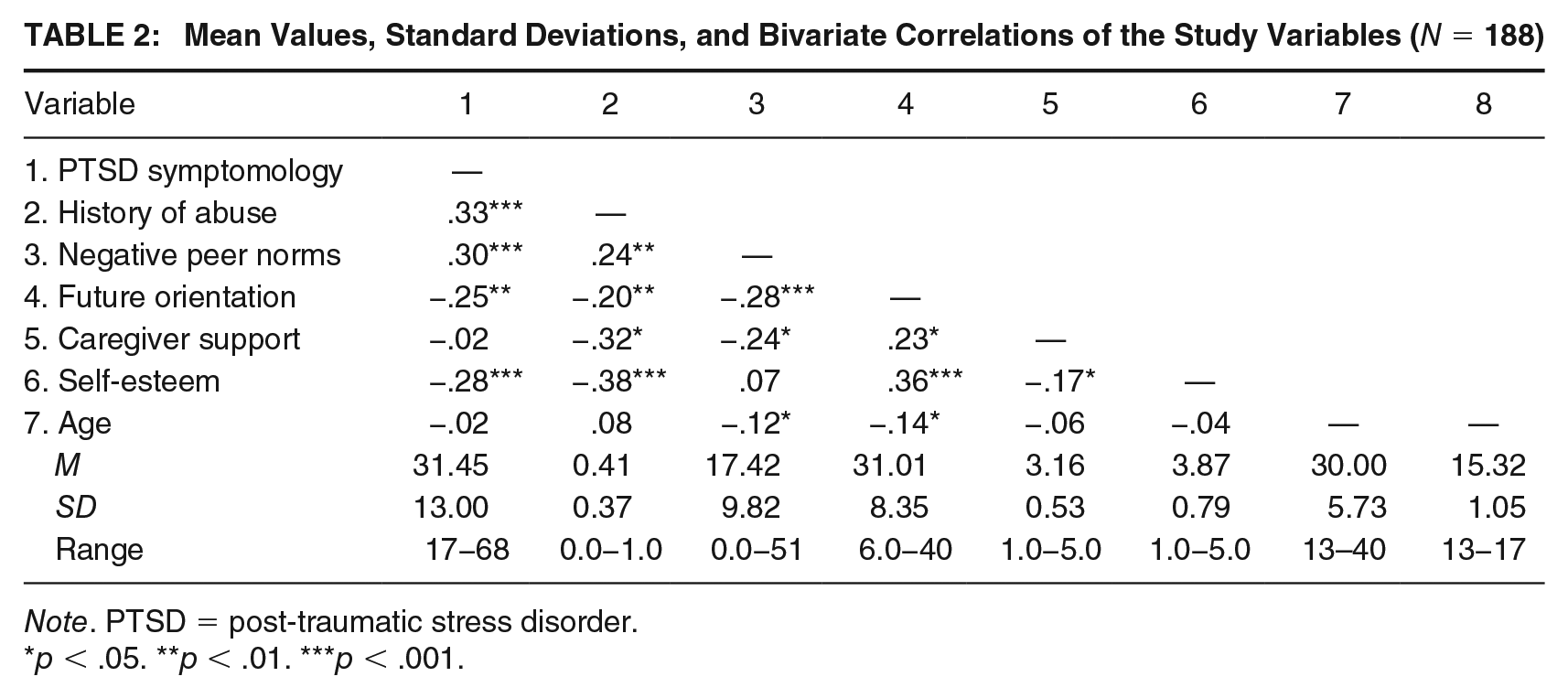
Note. PTSD = post-traumatic stress disorder.
p < .05. **p < .01. ***p < .001.
Multiple Regression Analysis on PTSD Among Black Girls (N = 188)
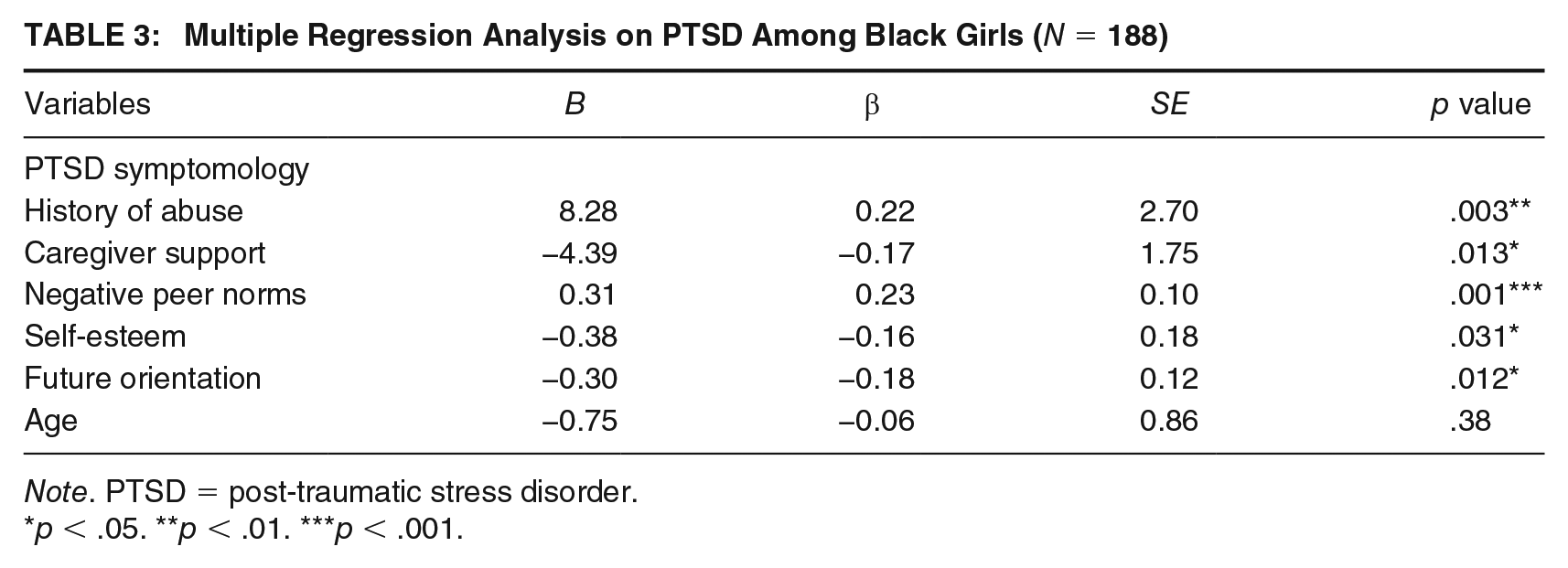
Note. PTSD = post-traumatic stress disorder.
p < .05. **p < .01. ***p < .001.
Results
Descriptive Statistics
The analytic sample consisted of 188 Black girls aged between 12 and 17 years, and the mean age was 15.32 years (see Table 1). Using an established clinical cutoff (see the “Measures” section), the symptoms for PTSD exceeded the cutoff (M = 31.45, SD = 13.47; Coffey et al., 2006). In terms of the different types of abuse, 56% of girls experienced emotional abuse, 43% experienced physical abuse, and 24% experienced sexual abuse. Overall, Black girls experienced moderate levels of history of abuse (M = 0.40, SD = 1.10). Girls reported low levels of negative peer norms (M = 17.42, SD = 9.82) and moderate levels of future orientation (M = 31.02, SD = 8.35). They also reported moderate levels of caregiver support (M = 3.16, SD = 0.53). Among the overall sample, girls reported moderate self-esteem (M = 30.00, SD = 5.73).
Bivariate Analyses
Table 2 provides bivariate correlations between the primary study variables and the outcome variable of PTSD symptoms. The results of the Pearson correlation indicated that there was a significant positive association between history of abuse and PTSD symptoms (r = .33, p < .001). A positive correlation also existed between negative peer norms and PTSD symptoms (r = .30, p < .001), as well as negative peer norms and history of abuse (r = .24, p = .008). Results also indicated negative correlations between future orientation and PTSD symptoms (r = −.25, p = .005), history of abuse (r = −.20, p = .007), and negative peer norms (r = −.28, p < .001). Negative correlations were documented between caregiver support and PTSD symptoms (r = −.26, p < .001), history of abuse (r = −.32, p = .003), negative peer norms (r = −.24, p = .002), and future orientation (r = .23, p = .011). There were negative correlations between self-esteem and PTSD symptoms (r = −.28, p < .001), history of abuse (r = −.38, p < .001), future orientation (r = .36, p < .001), and caregiver support (r = .36, p = .014). Finally, there was a negative correlation between age and negative peer norms (r = −.12, p = .007), as well as with future orientation (r = −.14, p = .049).
Multiple Regression
Accounting for the effects of age, the overall regression model was statistically significant R2 = .20, F(6, 181) = 8.74, p < .001. A change in 1 SD in history of abuse was related to a .22 decrease in PTSD scores (β = .22, p = .003). Negative peer norms were statistically significant and positively associated with PTSD scores (β = .23, p = .001). Our results revealed a negative relationship between future orientation and PTSD scores (β = .23, p < .001). Caregiver support was statistically significant and negatively related, resulting in a .17 decrease in PTSD scores (β = −.18, p = .012). Finally, self-esteem was negative and correlated with a decrease in PTSD scores (β = −.16, p = .031) among girls.
Discussion
This study addressed a major gap in research by focusing on Black girls in the juvenile justice system—an understudied population—to explore future orientation and other factors associated with PTSD symptoms. Study findings suggest that girls who reported high abuse histories reported high rates of PTSD symptoms. Overall, the study findings corroborate and extend those of prior studies that have documented that girls who have suffered abuse are at greater risk for reporting PTSD. The mean PTSD score for this study sample was 31.45, which suggests that the girls showed high levels of PTSD. However, in a previous study with incarcerated girls, they did not report total PTSD scores—they assessed PTSD with a Psychiatric Diagnostic Interview to determine past and current PTSD diagnoses. They found that 65.3% of the sample reported PTSD symptoms at some time in their lives while 48.9% of the sample reported current PTSD symptoms (Cauffman et al., 1998). Given the strong presence of histories of abuse for those in correctional facilities, detention centers should adopt a response model that focuses on protective factors like future orientation to promote a shift away from approaches that focus primarily on risk versus those that are protective.
Like other studies of youth—including girls involved with the juvenile justice system—Black girls in this study with histories of abuse correlated with PTSD symptoms. Black girls in this study reported moderate rates of PTSD, but did not report moderate or high rates of abuse. Previous research studies with Black adolescents and incarcerated African American women suggest they are likely to underreport mental health correlates, including PTSD, depression, and so on (Lu et al., 2017). Moreover, Black girls’ ability to radiate strength to cope with past trauma and rebuff future victimization involves adopting a protective demeanor that has been noted with this population, something scholars call survival coping (Kerig, 2018; Morris, 2016). This could also be seen as their survival coping mechanism as it helps them avoid danger in situations of immediate threat and harm. However, Black girls tend to be punished and further victimized when they demonstrate these protective behaviors. Specifically, they are often viewed as threatening and their attempts to deal with their trauma histories have been formed by their gendered and racialized stereotypes, including the subtleties of their trauma responses (Epstein et al., 2017; Kerig, 2018; Morris, 2016). Consequently, the need to develop culturally sensitive approaches to both prevent future harm and intervene to treat and reduce abuse associated with their juvenile justice involvement is even more dire.
Participants also reported having support from negative peer networks that may endorse risk norms, as well as having high levels of caregiver support correlated with PTSD symptoms. Specifically, for those with support from deviant peers, there was an increase in PTSD symptoms. This could be the result of girls who already display PTSD symptoms being drawn to or recruited to deviant peer networks; these peers may offer support because they have similar experiences and backgrounds. The timing of peer and caregiver support relative to experiences of PTSD symptoms are unknown, so the ability to indicate temporal ordering was not feasible. In addition, it is equally likely that youth who exhibit a stronger likelihood of PTSD or greater PTSD symptoms require greater levels of support, meaning they are more symptomatic and feel the need for greater caregiver support (Bradley & Corwyn, 2000). Given that these girls all resided in a local detention center at the time data were collected, they may have felt isolated, in the absence of support from caregivers, while they have access to both prosocial and deviant peers who are detained with them. In addition, nearly a quarter of the sample reported histories of sexual abuse, so they may feel increased PTSD symptoms in the absence of their caregivers, which is noteworthy as youth who have supportive caregivers may show decreased levels of symptoms (Wamser-Nanney et al., 2020).
Notably, the presence of structural violence in families, schools, communities, and systems (e.g., juvenile justice system, child welfare system) is an important link to maintaining systems of inequality that hinder child development and influence various behavioral problems among Black youth (McGee, 2014; Sokolower, 2011–2012). The results from this study suggest the need to confront the structures that foster violence through social domains, including associations with parents/caregivers, deviant peers, and their influence on PTSD symptoms. Specifically, other scholars have documented trauma and victimization within juvenile correctional facilities as an area of vital interest (Ford et al., 2013; Hodge & Yoder, 2017; Kerig, 2018; Yoder et al., 2019). Consequently, the trauma-offending link requires early and effective responses to trauma/victimization to halt future juvenile justice involvement (Yoder et al., 2019). Recent efforts by the Office of Juvenile Justice and Delinquency Prevention have focused on the need for a trauma-informed approach, noting the importance of collaborative treatment efforts across various child and family service organizations for youth who have experienced traumatic events (Olafson et al., 2016; Yoder et al., 2019). Scholars suggest a focus on matching treatment services with offender’s criminogenic needs (e.g., employment, education, substance misuse, and antisocial behavior) to change and reduce future criminal behavior (Andrews et al., 1990). Additional focus exclusively on Black girls is also warranted.
Higher self-esteem and future orientation were associated with lower PTSD scores. Prior studies have shown that high self-esteem is associated with lower rates of behavioral health risks (Harris-Britt et al., 2007). This study extends these findings by documenting that it is correlated with lower rates of PTSD symptoms. It is likely that high self-esteem might allow Black girls to engage in higher order self-regulation that might curtail the presentation of PTSD symptoms. As previously mentioned, Black girls’ coping skills (i.e., survival coping) and the need to present a tough exterior or attitude, coupled with descriptors like “Black girl magic” and being a “strong Black woman,” may also serve to promote high self-esteem despite the noted costs. Another point of consideration is the role of future orientation, which has not been a prominent factor in empirical studies with this population. In this study, future orientation in comparison with self-esteem had a stronger correlation to PTSD scores. This suggests that it is an important area of research to investigate protective mechanisms with justice-involved Black girls.
It is important to frame these findings within the context of this study population. Youth who often become involved with the juvenile justice system tend to reside in highly socially disadvantaged communities and in families where there are high levels of needs and stress (So et al., 2016). Although strong caregiver supports might be beneficial in some domains, strong supports and enmeshment with caregivers who are themselves troubled or with high need might also negatively impact the mental health of their youth. Larger samples are needed to better approximate mediating pathways accounting for PTSD symptoms among this population. In addition, identifying their perceptions of their future life chances—such as graduating from high school, going to college, or feeling like they will be respected in their community—all reflect their thoughts in an intersectional context that enhances future policy, research, and practice efforts.
Limitations and Implications
Our findings have significant implications for treatment, intervention, and future research. However, prior to discussing these implications, as with all studies, there are several limitations that warrant mention. The study design was cross-sectional and therefore all findings are correlational and do not suggest any causal or temporal inferences. For example, we could not establish the timing of caregiver and peer support relative to girls’ PTSD symptoms, so future work should consider this. Overall, the study findings are only generalizable to populations of Black girls with detention histories in Atlanta, Georgia, and similar settings. We assessed past PTSD as a self-reported measure, and it was not evaluated clinically. Clinical evaluations or a Structured Clinical Interview for the DSM-IV Axis I Disorders (SCID) is a widely used, structured clinical interview for psychiatric disorders that contains a PTSD-specific module with 19 items, which might serve to triangulate study findings (First et al., 1995). Although, prior research among urban youth is growing, other researchers have reported higher distress and impairment levels in traumatized youth with PTSD (Sartor et al., 2010) while other scholars note limits to PTSD, which omits the “complexity and ongoing nature of trauma commonly experienced by youth of color in urban communities” (Ginwright, 2015, p. 20). Future research studies with Black girls might also comprise mixed-methods studies to include both surveys of lifetime trauma and/or PTSD, that is, the UCLA post-traumatic stress disorder reaction index (PTSD-RI)—adolescent version for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) (Ford et al., 2018; Steinberg et al., 2013), including semi-structured interviews to understand how they make meaning of their histories of trauma and abuse. Furthermore, Ginwright (2015) suggested exploring Persistent Traumatic Stress Exposure, which may better describe the circumstances Black girls may experience dealing with ongoing chronic trauma in their families, schools, and communities.
This study examined direct relationships when many of these factors might be interrelated and mediating pathways may exist accounting for PTSD among this population. The finding for future orientation is one example of a factor that may be mediated by other covariates, like trauma, age, race, or gender, so these factors need to be investigated in future research studies with this population. The R2, though respectable and significant, was low. It should be noted that statistically significant coefficients in these models represent the mean change in PTSD, given a one-unit shift in the independent variables in the study. Qualitative findings may provide some context for these quantitative findings. This information would help with the development of interventions that are culturally tailored and effective. In a meta-analysis of mindfulness-based interventions (MBIs) with incarcerated adults, findings offered preliminary support of the efficacy of MBIs in targeting psychological health in incarcerated populations (Per et al., 2020). Further controlled studies are required to examine criminogenic outcomes and recidivism rates after treatment, especially for youth and girls of color. Andrews and colleagues (2010a) noted the need to adapt treatment with cognitive behavioral and social learning approaches to increase favorable youth outcomes. In addition, future studies should include parents and/or caregivers to investigate their past experiences of abuse. Retrospective analysis of childhood sexual abuse of Black women in Grenada who also had histories of domestic violence noted that they never disclosed their childhood histories of abuse due to a culture of silence (Jeremiah et al., 2017). Exploring this phenomenon with Black girls and their parents/caregivers might highlight potential patterns of abuse and system involvement as well as barriers to intervention and prevention efforts.
Past research has established that Black girls are targeted and experience higher rates of arrest and sentencing than their White equivalents (Greenberger et al., 2014; Moore & Padavic, 2010). However, their differential treatment needs to be explored in terms of their trauma and abuse histories. Black girls experience higher rates of confinement for nonviolent status offenses (e.g., truancy, curfew violations, and running away) unlike their White peers (Kim et al., 2020). One explanation for the link between Black girls and their increased involvement with the juvenile justice system is the perception that they are more threatening, aggressive, and angry (Kerig, 2018; Morris, 2016). In a recent study of adults in the United States, findings suggest that adults view Black girls from the age of 5 to 14 years as adults unlike their White counterparts (Epstein et al., 2017). Consequently, Black girls were viewed as “needing less protection and nurturing than White girls” (Epstein et al., 2017, p. 11). Black girls in this study also reported high levels of PTSD, which suggests a need to prioritize them in policy, research, and in the collection, analysis, and dissemination of social and health care services, school discipline, and juvenile justice (and child welfare) system data to incorporate pathways to healing that may curtail future arrests, detainment, and incarceration (YWCA, 2017).
Future research should consider incorporating parent/caregiver/family-focused interventions as the role of the family in particular has been shown to be protective related to other health outcomes of Black youth like HIV testing (Boyd et al., 2020). Intersectional social determinants of health and historical trauma should also be included in future research to further inform culturally appropriate interventions (Logan-Greene et al., 2018; Quinn, 2018). Specifically, this should be done within a framework of healing justice, one that mandates oppression be seen as community and collective trauma, which involves an approach “that restores individuals and communities to a state of well-being” (Ginwright, 2015, p. 9). Finally, future research studies should also include academic outcomes for detained girls. In a study of dually system-involved (juvenile justice and child welfare) youth, Black youth who reported histories of involvement with the juvenile justice system alone experienced far worse academic outcomes than other groups, so intervention strategies are needed to address their educational needs (Kalu et al., 2020; Yoon et al., 2019).
Conclusion
Components such as positive caregiver and family support, close prosocial peers to promote a future orientation, and healthy environments need to be incorporated to help reduce Black girls’ PTSD symptoms and delinquent behavior, and address their criminogenic needs. Specifically, multisystemic treatment approaches are needed to reduce the impact of family stress, as well as enhance parent/caregiver/family functioning that is associated with their responses to girls’ trauma and abuse (Hagan et al., 2017; Patterson & Fisher, 2002). In addition, given the protective effects of self-esteem and future orientation, culturally sensitive initiatives that bolster positive internal self-images and hope are warranted. Clinical services that address untreated trauma and promote healing by highlighting possibilities for well-being to moderate and reduce the negative effects of trauma on health outcomes are critical to reduce future delinquent behavior (Carrión et al., 2007; Ginwright, 2018). The opportunity exists to develop and leverage innovative approaches to reduce the arrest, detainment, and incarceration, as well as the residual effects of other types of system involvement for Black girls, so they can successfully heal from their experiences and live lives that are healthy and free of suffering and violence.
Footnotes
Authors’ Note:
We would like to acknowledge Kayla Luttrell of The Ohio State University College of Social Work for her writing and editorial assistance. All authors have met the criteria for authorship through their substantial individual contributions of the conception and development of this article. The content is solely the responsibility of the authors.