
Abstract
This study aimed to explore the effects of standardized mindfulness-based cognitive therapy (MBCT) and MBCT training without practice on the negative mood of women in custody. Eighty participants were assigned to the standard MBCT group, theoretical learning group, or waitlist control group. We assessed participants’ mindfulness, stress, depression, and anxiety before and after the interventions. The results showed that, compared with controls, participants in the standard MBCT course showed significant improvement in depression and state anxiety; they also showed significant improvement in perceived stress. Although similar effects on depression were observed in the theoretical learning group, this group did not show decreased anxiety. These findings suggest that practice plays a crucial role in MBCT’s effects on female prisoners’ mental health. This study provides important insights into the application of mindfulness-based interventions (MBIs) as promising treatments for improving responsivity factors of the risk–need–responsivity model for female incarcerated populations.
Keywords
Incarceration, as the main form of criminal correction, results in drastic changes in individuals’ basic way of life, creating much stress. For instance, while in custody, people live close to each other, must abide by strict rules, lose the ability to create value in their own way, and are exposed to social tension, such as bullying and social isolation (Ashkar & Kenny, 2008; Haney, 2012; Yardley & Wilson, 2013). Therefore, it is not surprising that imprisonment experiences are characterized by psychological symptoms, such as depression and anxiety (Ashkar & Kenny, 2008; Haney, 2012). Compared with men, women in custody appear to be more vulnerable to mental health issues. For example, several studies have shown that depression, anxiety, and self-mutilation are more common in women in custody than men in custody (Belknap & Holsinger, 2006; Bloom et al., 2003; Kessler, 1998).
The evidence-based risk–need–responsivity (RNR) model was proposed based on general personality and social learning perspectives and was developed to build treatment principles that pursue rehabilitation rather than punishment for individuals who are incarcerated (Andrews et al., 1990). According to the RNR model, effective treatment incorporates three factors: (a) risk: high-risk people who have committed crimes should be prioritized for treatment; (b) needs: the correction goal addresses criminogenic need; and (c) responsivity: selecting individualized strategies to reduce criminal behavior. Programs that adhere to the RNR model have been shown to reduce recidivism by up to 35% (Andrews & Bonta, 2010). Although mental health factors such as depression and anxiety are noncriminogenic needs, they are responsivity factors that affect the individuals’ motivation to engage in treatment, regulate their ability to learn, and have humanitarian meaning (Bonta & Andrews, 2017; Bonta et al., 1995; McCormick et al., 2017).
The present study focused on the potential for mindfulness-based cognitive therapy (MBCT) as an intervention to improve female incarcerated populations’ mental health. Given the unique experience-based learning style of mindfulness-based interventions (MBIs; Creswell, 2016), an active control group was included that received the same MBCT training; however, for this group, the learning mode was based on a classical teaching paradigm and on reflection rather than practice. This active control group was included to clarify the need for integrity when implementing MBIs in prisons.
Female Incarcerated Populations’ Mental Health and Its Relevance to the RNR Model
Although men and women have similar criminogenic needs, their mental health backgrounds are often different (Dye & Aday, 2013). Many studies have shown that women in custody often have serious mental health problems that require intervention (Leigey & Reed, 2010; Marzano et al., 2011a). Compared with men, women who are incarcerated have a higher history of mental disorders, physical and sexual violence, and past suicide attempts (Leigey & Reed, 2010). In addition, the relatively small number and limited distribution of women’s prisons reduces the possibility of visits, making it more difficult for women to obtain family support while in custody (Marzano et al., 2011b). Compared with men’s prisons, female prisons provide fewer educational, medical, and vocational services (Themeli, 2006), which increases the risk of more serious mental disorders. Previous studies have reported that women sentenced to life imprisonment often experience shock, denial, and numbness (George, 2010), leading to increased negative emotions, mental health problems, or social withdrawal (Kruttschnitt et al., 2000).
In this study, mental health is considered an RNR model responsivity factor. Although risks and needs are the primary salient factors in the design of a qualified correctional treatment plan, responsivity factors are also important. Studies have found that responsivity variables can predict treatment plan completion in adults who have committed sex offences, suggesting that focusing on responsivity in treatment can improve intervention outcomes (Beyko & Wong, 2005). Specific responsivity factors have been found to moderate the effect of intervention (Bonta et al., 1995), and successfully addressing responsivity factors (including mental health factors) can improve intervention effectiveness regarding criminogenic needs (McCormick et al., 2017).
Mental health is not only a responsivity factor, it is also relevant to gender-specific correctional treatment. Many studies have shown that corrective programs implemented according to the RNR model can reduce recidivism. However, most of these studies either focused on men in custody or did not classify the results according to gender (Gobeil et al., 2016). Although gender-neutral disciplinary methods insist that gender will not affect the implementation of correction strategies, subsequent studies have shown that common factors in female incarcerated populations, such as parenting pressure, trauma history, adverse social conditions, and mental health problems, influence their response to correction (Blanchette & Brown, 2006; Rettinger & Andrews, 2010; Van Voorhis et al., 2010). Gobeil et al.’s (2016) meta-analysis showed that when high-quality research with good control conditions was assessed, the gender-informed intervention was more beneficial than the gender-neutral intervention. Other researchers found that when incarcerated young women have a history of trauma, or mental or physical health problems, they require gender-informed interventions (Day et al., 2014).
MBIs, MBCT, and Mindfulness Practice
Contemporary MBIs combine training derived from Eastern meditation traditions with modern group psychotherapy. This approach has been shown to be effective for treating physical pain, depression, anxiety, addiction, and other physical and mental symptoms, and has received substantial support from empirical research over the past 30 years (Creswell, 2016). MBIs’ positive effects on judicial correction have been reported in several studies. For example, a study conducted in a British prison found that a 10-week mindfulness-based course improved incarcerated populations’ behavioral control, reduced their psychological distress, and increased their subjective well-being (Bilderbeck et al., 2013). A randomized controlled trial on female detainees at a detention center in Virginia, USA, found that after 7 weeks of mindfulness training, participants experienced fewer sleeping difficulties, a reduced desire to throw things or hit others, reduced nail or cuticle biting, and felt more hopeful about their future (Sumter et al., 2009). Another study found that mindfulness training reduced incarcerated populations’ postrelease risky behaviors (Malouf et al., 2017).
MBCT, the most evidence-based MBI, was developed by Teasdale and colleagues (2000) and specifically targets the psychological mechanisms of depression relapse. In particular, it integrates cognitive behavioral therapy with mindfulness-based stress reduction to benefit from both. A 60-week follow-up study found that, compared with traditional depression treatments, the standard 8-week MBCT course reduced depression patients’ relapse rate by 44% (Eisendrath et al., 2016).
As with other MBIs, the most important element in MBCT is mindfulness practice, which is usually conceptualized as a form of psychological training (Tang et al., 2015) that aims to cultivate an experiential awareness in the present moment (Hawley et al., 2014). Through practice, participants learn to deal with their own physical and mental experiences in an engaging and decentering manner, thus cultivating awareness of their internal state with an open, allowing, and accepting attitude. The intentional control of attention and the metacognitive processes during practice are reported to establish an alternative information-processing configuration, or cognitive mode, which is incompatible with a dysfunctional interlock configuration and therefore contributes to mental health (Bernstein et al., 2015, 2019; Shapiro et al., 2006). Mindfulness practice includes formal practice (such as body scan, sitting meditation, and other audio-guided meditations) and informal practice (intentionally paying attention to routine activities in daily life), which are equally important for cultivating mindfulness capacity.
Just as with physical training, greater mindfulness practice brings greater benefits. MBIs require participants to practice mindfulness both in class and as homework. Carmody and Baer (2008) found that the amount of formal practice during an 8-week mindfulness intervention was associated with depression symptom improvement, well-being, and increased mindfulness traits. Pradhan et al. (2007) found that depressive symptom improvement was positively correlated with practice frequency in patients with rheumatoid arthritis. Shapiro and colleagues (2003) conducted MBI with breast cancer patients and found that the amount of informal practice participants engaged in was associated with improved sleep.
Implementing mindfulness practice in prisons has other potential effects. The stress of incarceration may increase individuals’ risk of mental disorders (Yardley & Wilson, 2013). Despite this, if individuals in custody can learn to face their negative experiences with awareness and acceptance, the stress and pain associated with incarceration can become more manageable. That is to say, by becoming aware and accepting both the pleasant and unpleasant experiences without judgment, the habitual negative thoughts and reactions could be changed. These ideas were considered in mindfulness training. In other words, these characteristics of mindfulness training may prompt individuals to make more meaningful use of their incarceration time by improving psychological well-being. This could lead to smoother prison management, allowing staff to focus on correction treatment rather than maintaining order (Sumter et al., 2009).
Practical Concerns of MBI Prison Implementation
Several issues need to be considered when implementing MBIs in prison settings. The most prominent of these is whether the unique nature of mindfulness-based teaching can be implemented with integrity within the context of traditional prison management. All mindfulness courses are experienced-based and embodied learning through practice, where course topics are taught by mindfulness practitioners and based on direct practice experience in the classroom, with post-class practice being recognized as an important component of the course (Del Re et al., 2013). Although the practice aspects have been widely acknowledged as key elements of mindfulness teaching, few studies have verified their necessity for mindfulness learning effectiveness. Implementing mindfulness-based courses in correctional facilities may prove difficult, given that traditional prison education focuses on the transfer of knowledge through lectures rather than practice. This poses a practical implementation challenge not only for China’s correctional system but for that of other countries as well.
The Current Study
The purpose of this study was to test whether MBCT courses can alleviate negative emotions in female incarcerated populations and to examine whether practice-based mindfulness learning is necessary for mindfulness courses to exert positive effects. We applied a mental health intervention program for female incarcerated populations, adopting a quasi-random trial design, whereby an 8-week internationally standardized MBCT course was implemented in the experimental group; a well-matched 8-week course explaining the theory of MBCT served as the active control; and a wait-list control group served as the blank control. We systematically compared differences in perceived stress, depression, and anxiety in the three groups, before and after the 8-week interventions. We hypothesized that in-class and post-class practice are necessary conditions for mindfulness group courses to exert positive effects on stress and emotions. Therefore, compared with the theoretical learning and wait-list control groups, standard MBCT was expected to alleviate depression, anxiety, and stress to a greater extent.
Method
Participants
Participants were recruited from a women’s prison in China and were serving sentences of more than 15 years. After conducting a mindfulness lecture for all individuals in prison, 80 women enrolled voluntarily. The classroom used to conduct the standard MBCT intervention using yoga mats could only host a maximum of 25 people at once. Therefore, 80 participants were randomly assigned to one of three groups: the standard MBCT group (n = 25), the theoretical MBCT group (n = 30), and the wait-list control group (n = 25). Fourteen participants were excluded from the analyses because they were taking psychotropic drugs during the intervention period (six from the standard MBCT group, three from the theoretical MBCT group, and five from the wait-list control group), resulting in a total of 66 participants with valid data.
There were no between-group differences in age, education level, or distribution of crime types, χ2(6) = 0.87, p = .99. We also investigated between-group differences in the 12 dimensions of the Chinese Offender Psychological Assessment–Personality Inventory (COPA-PI, Y. Zhou, 2007). 1 Only the extraversion dimension showed significant group differences, F(2, 63) = 3.91, p = .03, where the standard MBCT group and theoretical learning group had lower scores than the wait-list control group. Participant characteristics and crime type distribution are shown in Table 1.
Participant Characteristics by Group (N = 66)
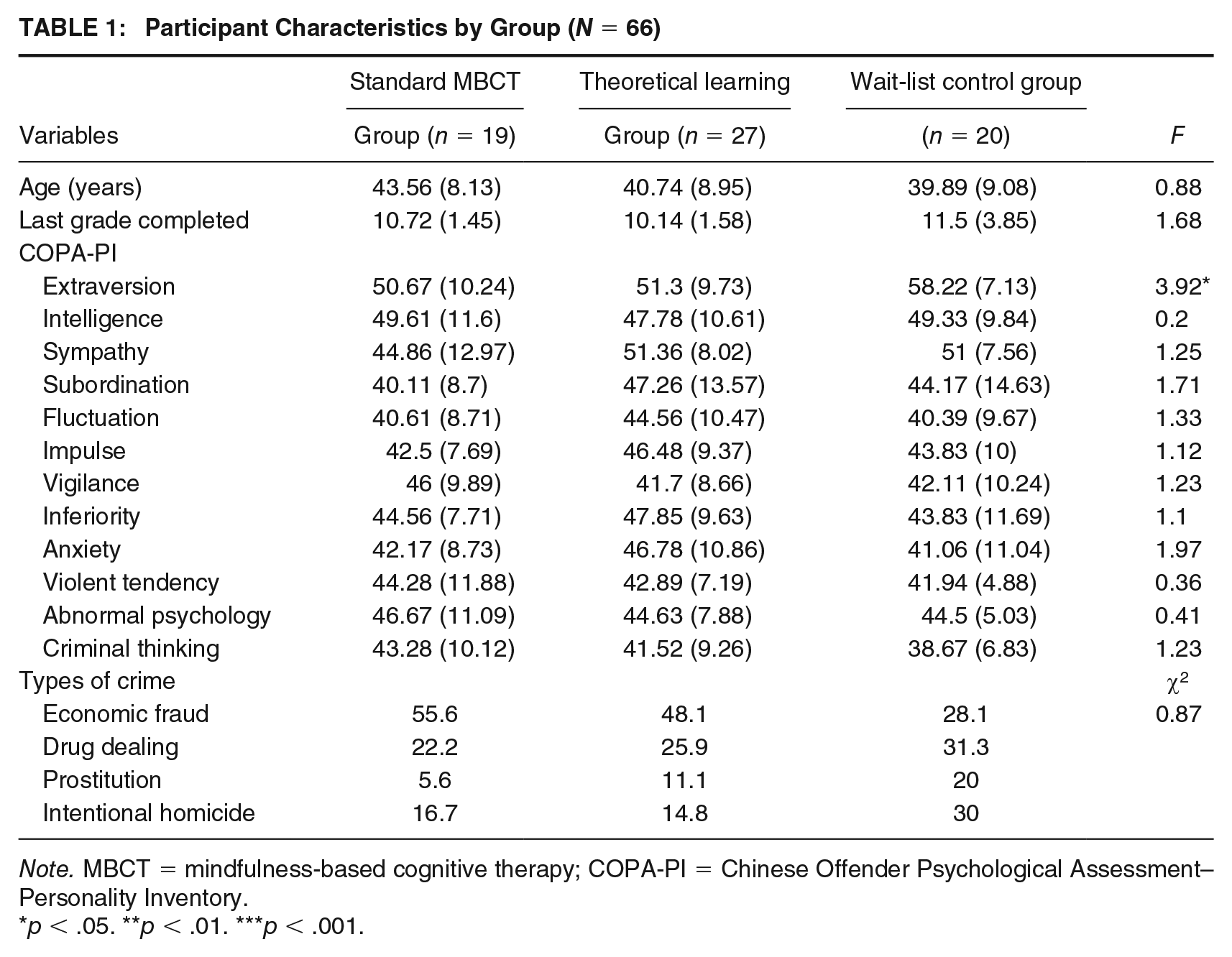
Note. MBCT = mindfulness-based cognitive therapy; COPA-PI = Chinese Offender Psychological Assessment–Personality Inventory.
p < .05. **p < .01. ***p < .001.
Research Procedure
Participants completed paper-based questionnaires in a prison area. To eliminate the effects of experimenter bias, neither the tester (research assistant) nor the participants were aware of group assignments. After completing the pretest, the standard MBCT group participated in the standard 8-week MBCT course with associated in-class and homework practice; those in the theoretical learning group participated in a well-matched 8-week mindfulness theoretical learning course without in-class or homework practice, and the wait-list control group carried on with their usual routine. The teachers for the standard mindfulness and theoretical learning groups were MBCT-qualified and had completed M1 to M4 teacher training approved by the Oxford Mindfulness Centre. After the 8-week courses, questionnaires were administered to all participants, with the practice questionnaire being administered only to the standard MBCT group. The standard MBCT and theoretical learning groups took part in the courses at the same time and believed that they had participated in the same mindfulness intervention. After the study completion, the theoretical learning and wait-list control groups were given the opportunity to complete the full MBCT course.
Intervention Methods
Standard 8-Week MBCT Course
The standard MBCT group followed the standardized teaching plan in the MBCT workbook, which included a 2-hr weekly session and 30 to 40 min of daily post-class mindfulness practice (Segal et al., 2002). During the actual implementation, paper-based practice instructions were given to the participants because audio playback devices were prohibited.
The classroom teaching structure of the standard MBCT group included 30 min of lecture-based teaching, about 30 min of group sharing and inquiry-based on practice experiences, and 30 to 40 min of mindfulness practice. Four sessions also included cognitive practices based on cognitive behavioural therapy.
Theoretical MBCT Course
The theoretical MBCT group received a theoretical learning course adapted from the standard MBCT course. The theme, duration, and the number of the weekly sessions corresponded exactly to the standard MBCT course, and the cognitive behavioural therapy session was also maintained. During each session, the teacher explained the psychological mechanisms underlying each theme, analyzed each theme using real-life examples, and encouraged students to reflect and discuss the themes based on their actual experiences. After each session, students were given the relevant chapters in the well-known book Full Catastrophe Living by the founder of contemporary mindfulness-based courses, Jon Kabat-Zinn, as post-class reading for self-learning. The teaching format was similar to the weekly mental health education courses in prisons, in which lectures and discussions are the main teaching forms.
Detailed descriptions of the two courses are presented in Supplemental Table S1 (available in the online version of this article).
Instruments
Mindful Attention Awareness Scale (MAAS)
The MAAS was developed by Brown and Ryan (2003), and a Chinese version was used for this study (Chen et al., 2012). The MAAS scale contains 15 questions, each scored on a scale of 1 to 6, where higher scores indicate a higher level of mindful awareness. Previous research demonstrated that the MAAS has good internal consistency (Cronbach’s α = .89) and good test–retest reliability (r = .87; Chen et al., 2012). In the current sample, MAAS scores showed moderate internal consistency (Cronbach’s α = .84).
Beck Depression Inventory (BDI)
Depression severity was measured using the Beck Depression Inventory–Second Edition (BDI-II). Each of the 21 questions was scored on a 4-point scale from 0 to 3, with higher scores indicating a higher degree of depression. Previous research demonstrated that the BDI-II has good internal consistency (Cronbach’s α = .91) and good test–retest reliability (r = .93; Zheng & Lin, 1991). Cronbach’s alpha in this study was .90.
Chinese Perceived Stress Scale (CPSS)
The Perceived Stress Scale (PSS) was developed by Cohen (1983), and the Chinese version used in this study was translated by Professor Yang Tingzhong. The scale consists of 14 items scored on a scale of 1 to 5, where higher scores indicate higher levels of stress in daily life. Previous studies have shown that the CPSS has moderate internal consistency (Cronbach’s α = .78) and moderate retest reliability (r = .78; Yang & Huang, 2003). Cronbach’s alpha in this study was .81.
State-Trait Anxiety Inventory (STAI)
The STAI was developed by Charles D. Spielberger (Spielberger et al., 1970). The scale consists of 40 items, each of which is rated on a 4-point scale, and items concerning positive emotions are reverse scored. Items 1 to 20 make up the State Anxiety Inventory (SAI), and Items 21 to 40 make up the Trait Anxiety Inventory (TAI). The Chinese version of this scale was obtained from the Handbook of Rating Scales for Mental Health (Wang, 1999). Higher scores indicate more severe state or trait anxiety. In previous studies, both the SAI and TAI have shown good internal consistency (Cronbach’s α: SAI = .92, TAI = .91; Li & Qian, 1995). Cronbach’s alpha for state anxiety was .92 and for trait anxiety was .88.
Participants’ Practice Questionnaire
We developed questions to investigate the status of the standard MBCT group’s mindfulness practice for this study. The items measured the frequency, length, and type of formal practice, the intention of informal practice, and the specific ways in which mindfulness was helpful to the participants.
Results
Common Method Bias Test
The data in this study were subjective self-reports, which are subject to common method bias. Based on the suggestions of similar studies (H. Zhou & Long, 2004), Harman’s single-factor test was employed to test for common method bias in the individual variables. Exploratory factor analysis was performed on the 90 pretest items, which had 26 factors with eigenvalues >1, the largest of which explained 22.81% of the total variance. The posttest had 24 factors with eigenvalues >1, the largest of which explained 26.28% of the total variance. This implies that the data did not show serious common method bias.
Negative Mood Improvement
At baseline, the groups showed significant differences in the level of perceived stress, F(2, 63) = 3.45, p = .04. The post hoc test found that perceived stress in the wait-list control group was significantly lower than that in the theoretical MBCT group (t = 2.41, p = .05, d = 0.53). There were no differences in baseline levels on the other scales.
Analysis of covariance (ANCOVA) analysis was conducted on the posttest scores of each questionnaire with the pretest as the covariate (Table 2). After 8 weeks of the course, there were significant between-group differences in state anxiety and depression (F[2, 63] = 3.28, p = .04; F[2,63] = 6.37, p < .001). The post hoc test found that the standard MBCT group state anxiety level was significantly lower than that of the theoretical MBCT group (t = 2.55, p = .04, d = 0.67). The results also showed that the depression score in the standard MBCT group was significantly lower than that of the wait-list control group (t = 3.57, p = .002, d = 0.84).
Pre- and Posttest Comparisons After Covariance Adjustment
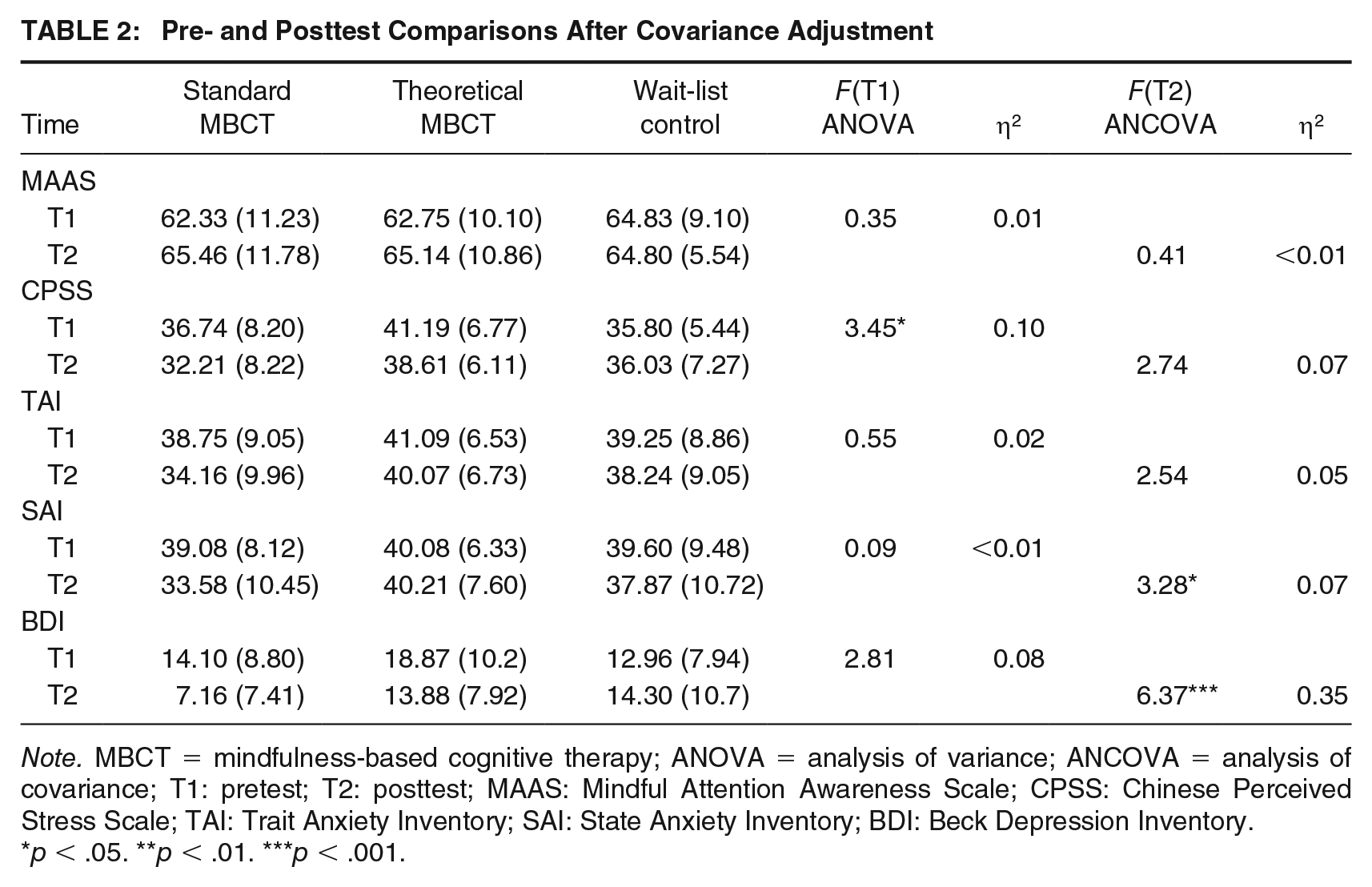
Note. MBCT = mindfulness-based cognitive therapy; ANOVA = analysis of variance; ANCOVA = analysis of covariance; T1: pretest; T2: posttest; MAAS: Mindful Attention Awareness Scale; CPSS: Chinese Perceived Stress Scale; TAI: Trait Anxiety Inventory; SAI: State Anxiety Inventory; BDI: Beck Depression Inventory.
p < .05. **p < .01. ***p < .001.
Further paired t tests showed that, compared with baseline, perceived stress in the standard MBCT group decreased significantly over time (t = 2.81, p = .01, d = 0.65) with a moderate effect size, and depression levels decreased (t = 3.57, p = .002, d = 0.82) with a large effect size. The state anxiety level decreased significantly over time (t = 2.55, p = .02, d = 0.59) with a moderate degree of effect; however, decreases in trait anxiety were not significant (t = 2.09, p = .02, d = 0.48) with only a small degree of effect. Depression levels in the theoretical learning group decreased significantly (t = 4.25, p = .001, d = 0.82), with a large effect size. The level of perceived stress decreased slightly (t = 1.77, p = .09, d = 0.34), with only a small effect size, and changes in state and trait anxiety were not significant (t = 0.10, p = .92, d = 0.02; t = 0.84, p = .42, d = 0.16). This suggests that both standard MBCT courses and mindfulness theory learning can alleviate learners’ depression and stress levels, but only standard MBCT interventions have a significant effect on state and trait anxiety (Figure 1 and Table 3).
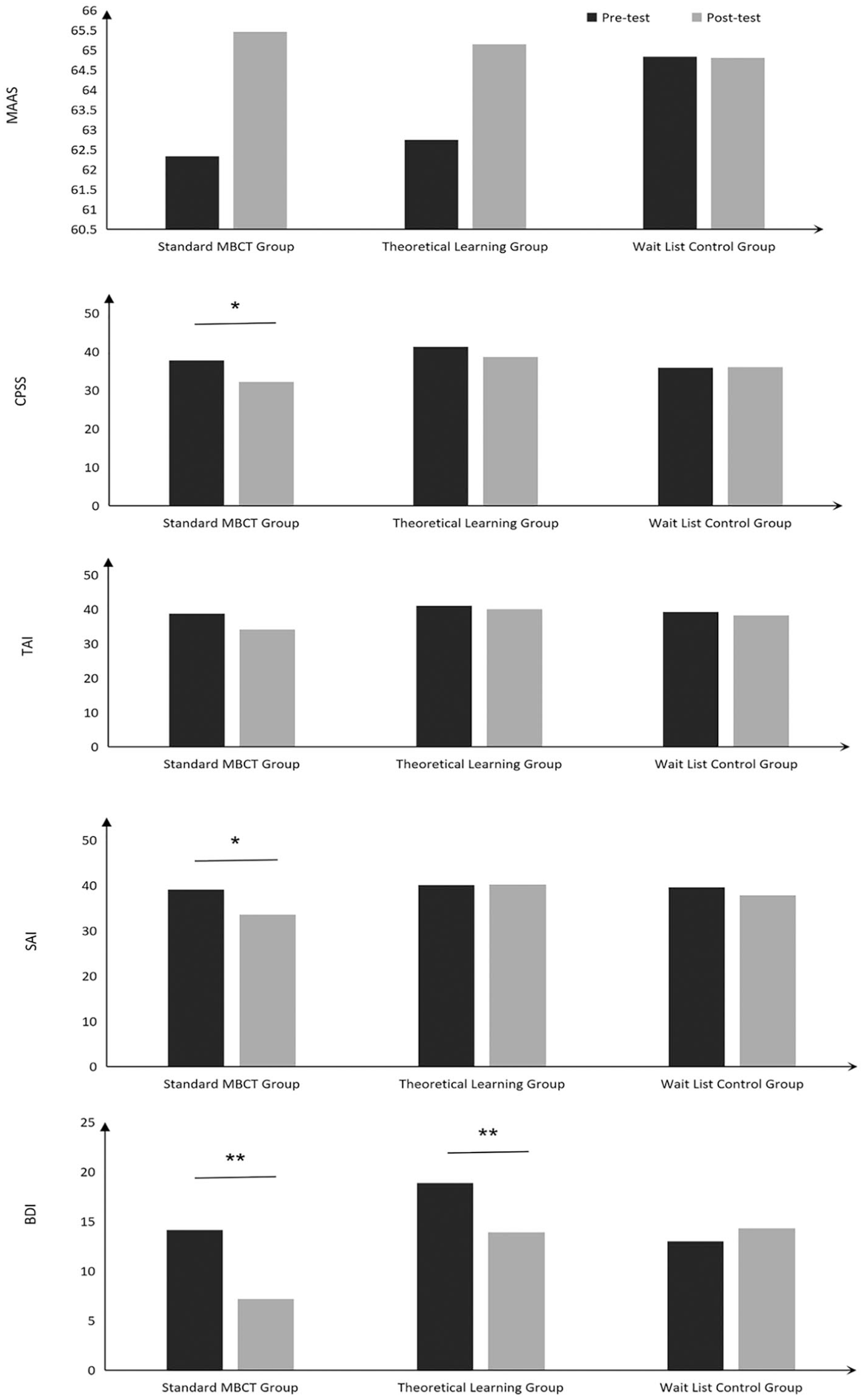
Pre- and Posttest Score Changes by Group
Pre- and Posttest Paired T Tests Across Groups
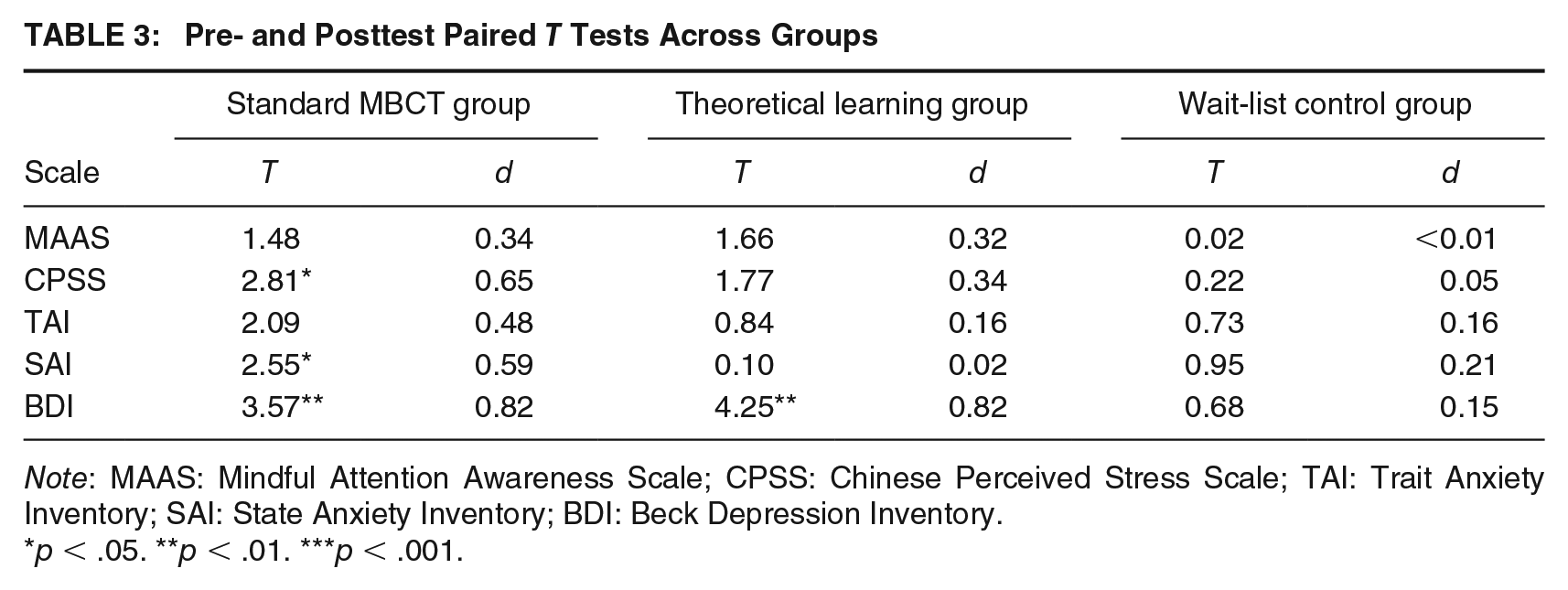
Note: MAAS: Mindful Attention Awareness Scale; CPSS: Chinese Perceived Stress Scale; TAI: Trait Anxiety Inventory; SAI: State Anxiety Inventory; BDI: Beck Depression Inventory.
p < .05. **p < .01. ***p < .001.
To further compare the differences between the standard MBCT and theoretical learning groups, the percent increases in scores from pretest to posttest were used to represent the degree of improvement in psychological indicators. The results of the independent-samples t test showed that there was a significant difference in the degree of improvement between the SAI scores of the standard MBCT group and the theoretical learning group (t = 2.27, p = .03, d = 0.68), with moderate effects. There was a slight difference in trait anxiety changes between the two groups, but only a small effect (t = 1.47, p = .15, d = 0.44). There was no significant difference between the two groups in depression and perceived stress levels (t = 0.99, p = .33, d = 0.30; t = 1.01, p = .32, d = 0.30). This shows that by the end of the 8-week course, state anxiety levels differed in the standard MBCT and theoretical learning groups, suggesting the crucial role of mindfulness practice for decreasing anxiety (Supplemental Table S3).
Mindfulness Practice as Homework
Participants’ homework practice in the standard MBCT group was measured using the practice questionnaire completed by 18 participants. Only four responders formally practised more than 3 times a week, and they showed more obvious changes in MAAS and perceived stress, as well as depression and anxiety levels (see Supplemental Figure S1, available in the online version of this article). However, we could not conduct inferential statistics because of the limited sample size.
In addition, 61.11% of the participants (n = 11) replied that they often engaged in informal practice, suggesting that the attitude of mindfulness was integrated into their lives. The types of formal mindfulness practice that participants frequently performed were mindful breathing (100% selected this option) and body scan (38.89% selected this option). The average length of each practice was about 8 min. The majority of participants believed that the effects of formal practice were mainly reflected in emotional control and concentration.
Finally, to investigate whether individuals with different personality traits obtain different benefits from MBCT courses, we examined correlations between the COPA-PI dimensions and the percent change between the pretest and posttest for each scale. Results did not show a significant relationship between the personality dimensions and the percent change between the pre- and posttests (see Supplemental Table S2).
Discussion
An active control design was employed in this study to test the efficacy of an MBCT course for improving the negative mood of female incarcerated populations. MBCT practice effects were investigated by comparing theoretical MBCT (without practice) with standard MBCT training (with practice). Despite the small sample size, our study has some valuable findings, with important implications for judicial correction.
First, our findings indicate that both 8-week mindfulness courses with matched themes (i.e., the standard MBCT group and theoretical learning group) resulted in decreased self-reported depression levels. However, only the standard MBCT group showed significant changes in the posttest scores for state anxiety; theoretical learning alone had no effect on anxiety. These results show MBCT’s feasibility in prisons and suggest that the experience-based nature of mindfulness practice may play a key role in improving mental health in female incarcerated populations.
The theoretical learning participants were taught by teachers with the same mindfulness teaching qualifications and covered the same learning topics as the standard MBCT group. Therefore, the explicit difference between the two groups was that one included mindfulness practice and the other did not. Consequently, we believe that the different outcomes between the two groups are attributed to mindfulness practice, both in the classroom and after class. The key to the difference may lie in mental operations that occur during practice.
Aversion and the habitual avoidance of unpleasant experiences underlie rumination, which is a key mechanism in depression relapse (Robinson & Alloy, 2003). Depression response style theory suggests that individuals who are prone to experience negative emotions often ruminate on negative events, in an attempt to resolve the issues causing the pain, leading to more negative emotions and more dissatisfaction with themselves (Nolen-Hoeksema, 2000). This mind-set is also common in normal populations (Piguet et al., 2014). MBIs may help dissolve this loop through mindfulness training, which works to establish a new mind-set that embraces facing experiences with openness and acceptance, regardless of their flavour (Hawley et al., 2014). These skills could be taught and understood to some degree by classical teaching and self-reflection, as shown by the positive effects on depression observed in the theoretical learning group. However, only the standardized MBCT group illustrated the broader positive effects on depression, perceived stress, and state anxiety. Only through mindfulness practice can one experience being with an internal state without reacting. By just observing physical sensations through formal and informal practice, individuals learn to experience emotional impulses in a safe way and realize that any experience can rise and fall like the tide and will not last forever (Shapiro et al., 2006). This insight could help liberate individuals from clinging to cravings, aversion, and automatic reactions by replacing them with skilful responses (Shapiro et al., 2006).
Given the limited number of practice questionnaire respondents, we cannot draw conclusions regarding the amount of practice needed to drive a significant positive effect, but the participants who indicated that they engaged in formal practice more than 3 times per week showed greater improvements in depression, anxiety, and perceived stress (see Supplemental Figure S1). Moreover, standardized MBCT participants were not allowed to use an audio player to practice under guidance after class, a common MBI practice, which may have resulted in lower measured effects. In fact, the hypothesis that more mindfulness practice equals better results has been supported in previous studies (Carmody & Baer, 2008; Pradhan et al., 2007). Future studies should work to clarify the relation between the amount of practice time and MBI benefits.
Second, and more relevant to the RNR model, MBCT’s positive effects on female incarcerated populations’ mental health highlight the feasibility of structured MBIs as an effective way to address responsivity factors in the correctional justice system. As one of the responsivity factors, mental health can regulate individual learning motivation and reduce participants’ attrition in correction programs, functioning as an intermediate stage of risk factor correction (McCormick et al., 2017). Moreover, the capacities cultivated by MBIs—being with and not reacting—may help individuals be more engaged in correctional treatments. In the standardized MBCT group, several participants reported that when they concentrated on what they were doing in the present, through focusing and observing their bodily sensations, boring work became more interesting, so staying in the present was no longer difficult. The standard MBCT participants also shared experiences of regulating and transforming their emotional impulses during interpersonal conflicts by focusing on their breath and bodily sensations. The standardized MBCT facilitated thought-provoking sharing, all based on the participants’ firsthand practice experience. This suggests that MBIs can have positive benefits, not only on incarcerated populations’ mental health but also on their manner of being with themselves and the rest of the world. This is highly relevant to the intrinsic concept of the RNR model—to design and deliver crime prevention programming in an ethical, legal, decent, humane, and otherwise normative manner (Bonta & Andrews, 2017).
Third, according to the RNR model’s principle of responsivity, correctional treatment should be based on individuals’ characteristics (Andrews & Bonta, 2010). Women with long-term sentences live in prison for a long time and face the normal problems associated with aging. MBIs can improve incarcerated populations’ physical condition by increasing flexibility (Field, 2011). In addition, previous studies have shown that women in custody face higher levels of stress, leading to higher levels of cortisol, a hormone that can cause several health problems (De Kloet et al., 2005). MBIs may help reduce cortisol levels (Lindsay et al., 2018); therefore, MBIs may be an effective preventive health measure.
MBCT and other group MBIs can also work as gender-sensitive interventions to help women deal with gender identity problems, reduce stress, and alleviate the related psychological problems caused by premenstrual syndrome or menopause (Sumter et al., 2009). In particular, relationship theory asserts that breaking off relationships is an important source of psychological pain, and compared with men, women prefer to use social contact to relieve pressure (Anumba et al., 2012). As a group therapy, MBCT’s dynamic factors help individuals to obtain support through interpersonal relationships developed during the course.
Finally, the benefits of a mindfulness-based curriculum could be sustained and strengthened after course completion. MBIs were developed to increase individuals’ capacity to face both positive and negative life experiences with kindness and compassion, cultivating inner wisdom by just being with their own experience, and developing skillful responses, rather than reacting through habit (Shapiro et al., 2006). This capacity can be mastered through practice, and maintained and developed for as long as individuals continue to practice. Thus, the benefits of MBIs can continue to help individuals over time, which was supported by a study that collected follow-up data on practice perseverance and its benefits after the course was over (Kuyken et al., 2008). Other studies also indicated that mindfulness training can help individuals who are incarcerated maintain a positive outlook for the future and focus on goals, which are both essential for successful reintegration (Auty et al., 2017; Maruna, 2001).
Another finding that is worth noting is that compared with the wait-list control group, the standard MBCT and theoretical learning groups did not show significantly higher levels of mindful awareness at posttest compared with pretest, although the theoretical learning group showed a trend in this direction. This result might be attributable to the instrument used to measure mindfulness in this study, the MAAS, which is a unidimensional scale that mainly reflects the awareness dimension of mindfulness (i.e., consciousness). However, the mindfulness attitudes of acceptance and nonjudgment are not reflected in this scale. Although some early scholars believed that “clear consciousness of the present moment” was the only core tenet of mindfulness, as mindfulness developed into a formal scientific concept, more researchers began to view it as a complex, multidimensional system. For instance, it requires individuals to adopt a curious, open, and accepting attitude toward present experiences (Keng et al., 2011). The monitor and acceptance theory (MAT) divides mindfulness into two dimensions: monitor and acceptance (Lindsay & Creswell, 2017). Contemporary MBI systems are multifaceted; acceptance is also one of the important elements and practice goals. This implies that mindful awareness alone is not an adequate measure of the full mindfulness spectrum.
Limitations
This study has some limitations. First, the small sample size limits the results to preliminary inferences. We did not anticipate the high number of participants on psychotropic medication, which resulted in a loss of valid data. Second, retrospective reports of homework practice may have been influenced by individuals’ subjective bias; daily practice diaries would be more accurate. Third, there is a possibility that the standard MBCT participants and the theoretical learning participants discussed the course content, contaminating data from the two groups to some degree. However, we do not believe this was a serious problem because of the fact that in Chinese prisons, individuals tend to be very busy with their daily work and study schedules, leaving little time for free chat. This study was carried out in a large prison with 3,000 females; the participants came from different areas and different cells, which further reduced the possibility of individuals discussing course content; however, this cannot be completely ruled out.
Future Research Directions
Our results show that MBCT played an important role in alleviating female incarcerated populations’ negative emotions; however, these types of treatments for noncriminogenic needs should not replace those that address criminogenic needs. Future studies should, therefore, continue to evaluate whether incarcerated populations who have undergone MBIs perform better in correction programs aimed at criminogenic needs, so as to further reduce recidivism.
Supplemental Material
sj-pdf-1-cjb-10.1177_0093854820974409 – Supplemental material for Comparison of Mindfulness With and Without Practice Among Women in Custody
Supplemental material, sj-pdf-1-cjb-10.1177_0093854820974409 for Comparison of Mindfulness With and Without Practice Among Women in Custody by Xiaolan Song, Huiwen Zhao, Ting Lou, Yanming Wang and Ming Zheng in Criminal Justice and Behavior
Footnotes
Authors’ Note:
This work was supported by Open Research Fund of College of Teacher Education, Zhejiang Normal University (No. jykf20022); We thank Zeng Ling for her support during the study, as well as the authorities of Female Prison of Zhejiang Province for the organization of the course. And we would like to thank Editage (Supplemental Figures S1 and Supplemental Tables S1–S3 are available in the online version of this article at ![]() ) for English language editing.
) for English language editing.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.