
Abstract
Youth in juvenile justice facilities are at high risk of self-directed violence (SDV; suicide attempts and self-harm). Research shows that positive youth perceptions of adults are preventive against SDV among community youth, yet it is unknown whether this extends to detained youth. Using a large national dataset, the present study examines whether, at the facility level, youth perceptions of staff are associated with rates of youth SDV over time. Results from a multilevel mixed-effects negative binomial model suggest that after accounting for various juvenile facility characteristics and practices, youth perceptions of staff are marginally associated with decreased rates of SDV over time. The results from the present study hold implications for research, policy, and practice. Importantly, the results imply a need for facility-wide and evidence-based staff training on SDV among detained youth that emphasizes building positive interpersonal relationships between staff and youth.
In the United States, suicide is the second leading cause of death for youth aged 10 to 14 and the third leading cause for persons aged 15 to 24 (Centers for Disease Control and Prevention [CDC], 2022), with youth suicide rates increasing over time (Kim et al., 2021; Plemmons et al., 2018). An estimated 17% of youth experience suicidal ideation (thoughts or plans of suicide) and 7.4% attempt suicide (Kann et al., 2018). There is also a strong relationship between self-harm and suicide ideation and attempts (Klonsky et al., 2013; Paul et al., 2015); an estimated 21.2% of youth report engaging in lifetime intentional self-harm (Brausch & Gutierrez, 2009). The CDC defines both suicidal and non-suicidal behaviors, including suicide, suicide attempts, and self-harm as self-directed violence (SDV; Crosby et al., 2011).
Juvenile justice-involved youth have high rates of complex traumas and mental health needs that put them at increased risk of SDV (S. L. Brown et al., 2021; Kim et al., 2021). In juvenile residential facilities, suicide is the most common cause of death (Hockenberry & Sladky, 2020). It is therefore imperative to understand the mechanisms through which juvenile justice facilities can prevent youth SDV. Among community youth, trusted adults are generally considered key to preventing SDV (Asarnow & Mehlum, 2019); however, the adults with whom detained youth have regular contact are facility staff. By nature of their position, facility staff may have a different relationship with youth than a community youth would expect to experience. Using national data, the present study tests the extent to which detained youths’ positive perceptions of juvenile justice facility staff are associated with reduced youth injuries related to SDV.
Youth Suicidal Behavior in Juvenile Justice Facilities
Juvenile justice-involved youth are generally at higher risk for SDV than youth who are not justice-involved (Katsman & Jeglic, 2021; Teplin et al., 2015). Research estimates that up to 34% of justice-involved youth report suicidal ideation (Conrad et al., 2024), and up to 25.5% report attempting suicide (Heirigs et al., 2019). Similarly, approximately one-quarter of justice-involved youth report a history of self-harm (Conrad et al., 2024; Jin et al., 2021). Several factors help explain the elevated risk of SDV among justice-involved youth.
First, risk factors for SDV include many dimensions of emotional dysregulation common among justice-involved youth, such as negative self-concept, impulsivity, hopelessness, and hostility (Ford & Hawke, 2012). Second, justice-involved adolescents experience high rates of trauma (Dierkhising et al., 2013) and adverse childhood experiences (ACES; Baglivio et al., 2014), with as many as 98% of justice-involved youth reporting at least one traumatic experience (Johnson, 2017, 2018). Research finds a strong predictive relationship between trauma and suicide risk among justice-involved youth (Kim et al., 2021), including a dose–response relationship between cumulative ACEs and SDV (Bhatta et al., 2014; Johnson, 2017). Placement in juvenile justice facilities often contributes to traumatic childhood experiences, with 56% of youth reporting some form of violent victimization while in custody (Evans-Chase, 2014).
Finally, youth who are detained in juvenile justice facilities may have mental health needs that place them at increased risk of SDV. An estimated 60% to 75% of detained youth have at least one diagnosable psychiatric disorder (Colins et al., 2010; Teplin et al., 2002), compared with an estimated 20% of community adolescents (Merikangas et al., 2010). Research suggests that youth detained in juvenile justice facilities are at an even greater risk of SDV than justice-involved youth who remain in the community (Stokes et al., 2015; Teplin et al., 2015). Rates of suicidal ideation among detained youth range from 10% to approximately 40%, and between 9% and 34% of detained youth report attempting suicide (Abram et al., 2014; Hatcher et al., 2018). Fewer studies have explored self-harm among detained youth, although one self-report survey of juveniles entering secure juvenile facilities found that 25.7% of detained youth report a history of self-harm (McReynolds et al., 2017). Given that mental health treatment is not the primary mandate of the juvenile justice system, juvenile justice programs and facilities are often ill-equipped to meet the needs of mentally ill youth (Cavanagh et al., 2019), resulting in a strikingly underserved population. For example, a large-scale study of detained youth found that only 16% of youth needing mental health treatment received it during detention (Aalsma et al., 2015).
Factors Associated With Detained Youth SDV
SDV is not evenly distributed among detained youth. First, gender, race, and ethnicity are robust predictors of SDV in juvenile confinement. Detained girls are consistently more likely to report SDV in juvenile justice facilities than boys (Heirigs et al., 2019; Jin et al., 2021), and facilities with higher populations of males generally have lower rates of suicide attempts (Gallagher & Dobrin, 2006). Yet, most suicide deaths in juvenile confinement are male (Hayes, 2005, 2009; Ruch et al., 2019), consistent with non-justice-involved youth (Fontanella et al., 2015), suggesting that although females have higher rates of non-fatal suicide ideation and SDV in juvenile detention, male SDV may be more commonly fatal.
Second, race and ethnicity may be associated with SDV. Non-Hispanic White youth generally report a higher rate of suicide ideation and SDV compared with Latine/Hispanic and Black youth in juvenile facilities (Heirigs et al., 2019; Joshi & Billick, 2017), and the majority of victims of suicide in juvenile confinement are White (Hayes, 2005, 2009; Ruch et al., 2019). Yet, such findings are mixed (e.g., Abram et al., 2014). For example, a higher population of Black youth in juvenile justice facilities is associated with both increased rates of suicide attempts and risk of suicide deaths (Gallagher & Dobrin, 2006).
Finally, various facility characteristics are associated with increased risk of SDV in juvenile justice settings. These risks include larger detainee population sizes; private (vs. public) ownership; type of facility; facility urbanicity and region; use of restraints; lack of mental health care onsite; lack of programming; longer sentences; locked sleeping rooms; and the absence of suicide screening for youth within 24 hours of intake (Barkan et al., 2013, 2014; Casiano et al., 2016; Fontanella et al., 2015; Gallagher & Dobrin, 2006; Hayes, 2009; Huey & Mcnulty, 2005; Rossen et al., 2018). Given the high prevalence of SDV within juvenile detention facilities, it is important that researchers continue to explore both individual- and facility-level characteristics that may be associated with rates of SDV to guide suicide prevention strategies. For this reason, the present study considers gender, race and ethnicity, average length of stay, crowding, restraint use, and facility type in analyses.
Positive Adult–Youth Relationships and Suicidal Behavior Prevention
Positive adult–youth relationships are a key component of many SDV prevention strategies, which often include helping suicidal youth identify supportive adults inside and outside of the family they can turn to in moments of crisis (Diamond et al., 2019; Pisani et al., 2013). Family- and parent-based interventions have been shown to reduce SDV (see review by Glenn et al., 2015), yet positive adult relationships outside of the family can also be impactful. For example, a study of 38 high schools in the U.S. found that the density of trusted adult–child relationships in schools predicted fewer suicide attempts among students (Wyman et al., 2019). Likewise, a recent review highlighted the importance of trusted adults in preventing suicide ideation and suicide among young people (Asarnow & Mehlum, 2019).
The adults with whom detained youth spend the greatest amount of time are correctional staff (Anderson et al., 2020), and the primary source of adult–youth socialization and social learning in juvenile detention is staff (Feierman & Ford, 2016; Galardi & Settersten, 2018). Frontline staff are responsible for monitoring youth and enforcing facility policies (Ford & Blaustein, 2013) but also for the daily care and safety of detained youth (Pederson et al., 2021). Staff must balance their punitive role with their protective and rehabilitative roles (Inderbitzin, 2006, 2007) yet are more frequently trained in discipline, behavioral management, and rule enforcement than interpersonal techniques, mental health, and trauma (Ford & Blaustein, 2013).
A 2006 survey of juvenile correctional facility administrators and staff from juvenile justice facilities in the United States found that 100% of administrators report that rehabilitation is one of their facility’s goals, and 98% of staff reported their goal for dealing with juveniles focused on rehabilitation (Marsh & Evans, 2009). Yet, 50% of administrators and 83% of staff reported their goals also focused on deterrence, with 33% of administrators and 14% of staff also reporting a focus on incapacitation (Marsh & Evans, 2009). Similarly, an ethnographic study examining rehabilitative practices in a mid-sized juvenile detention center found that while intentional rehabilitative practices were common during both staff-led group activities and routine staff-youth contacts, some staff members believed that “detained youth were incapable of making positive change and/or that rehabilitative is an ineffective or inappropriate goal for detention” (Walden & Allen, 2019, p. 317). These studies suggest that while rehabilitation is a focus of many facilities and facility staff, punitive approaches are still prevalent in juvenile facilities. As such, relationships between staff and youth within juvenile justice facilities have a higher-magnitude power differential and more acrimonious tone than adult–youth relationships outside detention contexts (Cox, 2021). In fact, researchers argue that detained youth often have ambivalent and distrustful attitudes toward adults, particularly those with authority, and tend to react negatively to adults who hold punitive power over them (Ford et al., 2012).
Although less is known about how positive adult–youth relationships as a means of SDV prevention in non-detained samples may translate to juvenile facilities, there is evidence that positive staff–youth relationships and positive youth perceptions of staff are associated with positive outcomes for detained youth. A longitudinal study of male youth incarcerated in a secure juvenile facility in California found that positive perceptions of correctional staff are associated with reductions in institutional violence (C. Brown et al., 2019). In addition, a survey of 519 formerly detained youth across 100 facilities in the United States revealed that positive perceptions related to staff lead to a healthier adjustment for youth (Schubert et al., 2012). Similarly, a survey of 137 detained male youth found that perceptions of staff fairness were associated with well-being (i.e., feelings associated with their experience in detention, such as how stressful it has been) but not adjustment internalizing (Cesaroni & Peterson-Badali, 2016). In a study of detained youth who reported suicidal ideation in the past 6 months, 46.1% had disclosed it to another person, although it is not clear if that person was a staff member at the facility (Abram et al., 2008), suggesting the importance of approachable adult figures.
Emerging practices regarding suicide prevention in juvenile justice facilities encourage youth to turn to facility staff for help and focus on fostering supportive relationships between youth and staff. For example, the Safety Planning Intervention (SPI), originally designed to be implemented in emergency departments, has recently been modified for use in juvenile detention facilities. SPI includes instructions to help suicidal individuals identify support persons (Stanley & Brown, 2012). In juvenile justice facilities, staff are instructed to help youth identify staff whom they can ask for help (Rudd et al., 2021). In addition, the Youth Mental Health First-Aid (YMHFA) training is designed to educate and train frontline adults (e.g., teachers, health and human service workers) how to respond to youth with mental health challenges or who are in crisis (Ross et al., 2023). Adults are encouraged to listen to youth non-judgmentally, give reassurance and information, and encourage self-help and other support strategies. Juvenile justice facility staff who have been trained on YMHFA have reported that the skills they learned are relevant to their work and enable them to better recognize and respond to concerning behaviors that could turn into a crisis (Anderson et al., 2020). However, it is important that any change in policy or new programming instituted in youth detention facilities to reduce SDV be evidence-based. To this end, the present study investigates the extent to which positive youth perceptions of correctional staff protect against youth SDV in juvenile justice facilities.
Present Study
SDV prevention is a pressing issue in juvenile justice facilities, as juvenile justice-involved youth often have complex traumas and mental health needs and are at increased risk of SDV. However, facility staff may serve as supportive adults for youth who are detained and at risk of SDV, just as other adults are protective against suicidal and self-harm injuries among non-detained youth. Furthermore, research suggests that both youth characteristics and juvenile justice facility characteristics are associated with youth SDV. Yet, to date, little research has examined the correlates of youth SDV while detained, let alone longitudinally. We use a longitudinal national dataset of juvenile justice facilities to examine whether, at the facility level, youth perceptions of staff are associated with rates of youth SDV over time. We hypothesize that positive youth perceptions of staff will be inversely related to rates of SDV, operationalized as suicidal and self-harm injuries, accounting for facility characteristics such as facility demographics, location, and practices. In other words, we expect that facilities with higher average youth perceptions of staff will report less SDV over time.
Method
Data for the present study were obtained from the Performance-based Standards (PbS) Database for Researchers. PbS was launched in 1995 by the U.S. Office of Juvenile Justice and Delinquency Prevention to improve conditions of juvenile confinement and is now operated by the Center for Improving Youth Justice. The PbS database includes data from more than 300 U.S. juvenile correctional, detention, and assessment facilities. Facilities volunteer to participate in PbS and complete a 1-year candidacy and post-candidacy program under the guidance of a PbS Coach prior to their data being included in the PbS database. Beginning in October 2010, data was collected twice annually in April and October. Our analytic sample includes data over 23 collection periods between 2012 and 2017, with a total of 3,269 facility-level observations. We used data from April 2012 through April 2017 for two reasons. First, data collection instruments changed over time, and these collection periods included the necessary data. Second, we avoided analyzing data collected during the COVID-19 pandemic, as beginning in March 2020 the operation of juvenile justice facilities changed drastically (Barnert, 2020; Buchanan et al., 2020) and the average daily population in juvenile facilities decreased substantially (Godfrey Lovett, 2021) to protect the health of youth and staff.
Data were obtained from four PbS sources: the Administrative Form, Incident Report Form, Youth Climate Survey, and Staff Climate Survey. The Administrative Form includes facility-level data for each 6-month collection period (e.g., geographic location). The Incident Report Form includes incident-level data on all incidents and injuries in the facility during the collection period. The Youth and Staff Climate Surveys include individual-level information from a random selection of at least 30 youth and 30 staff in the facility during the month of data collection, respectively. As facilities, not youth, were measured repeatedly over time, all incident- and individual-level data were aggregated to the facility, and analyses were conducted at the facility level. A total of 206 facilities contributed data to PbS between April 2012 and April 2017. Out of 11 total collection periods, facilities contributed data for an average of 9.35 (SD = 2.67) collection periods, ranging from 1 to 11, for a total of 1,545 observations.
Measures
Self-Directed Violence
On the Incident Report Form, staff reported the number of injuries recorded in the collection period, defined as “any instance in which a youth or staff member is hurt even if treatment is not provided” (PbS Glossary: A Glossary of Critical Terminology for the PbS Program, p. 15), and the cause of each injury, including self-harm and suicidal behavior. Self-harm is defined as “behavior that causes harm” such as “self-laceration, self-battering, taking overdoses, or exhibiting deliberate recklessness” (PbS Glossary: A Glossary of Critical Terminology for the PbS Program, 2022, pp. 25–26). Suicidal behavior is defined as “attempted suicides, suicidal gestures, self-mutilations, intentional injuries to self, and developing a plan or strategy for committing suicide. . .suicidal behavior usually involves some overt action by youths, indicating intent to injure or kill themselves” (PbS Glossary: A Glossary of Critical Terminology for the PbS Program, 2022, p. 29).
These definitions overlap with one another. The definition of self-harm does not differentiate between suicidal and non-suicidal self-harm, and PbS paradoxically states that “instances of self-mutilation and of suicidal gestures must be classified as ‘suicidal behavior’ because it is impossible for facility staff to know the youth’s true motivation” (PbS Glossary: A Glossary of Critical Terminology for the PbS Program, 2022, p. 29). This likely results in inaccurate representations of self-harm and suicidal behavior and any measurement of one behavior in isolation from the other would be confounded. Therefore, our dependent variable, SDV, combines the two categories of injuries. Keeping in line with the CDC’s definition of SDV (Crosby et al., 2011), our dependent variable is operationalized as the total number of injuries reported to be caused by suicidal behavior or self-harm in each facility per collection period.
Youth Perceptions of Staff
Youth were asked 14 questions on the Youth Climate Survey gauging their perceptions of facility staff, such as whether staff respect their traditions, beliefs, and cultures, whether they trust the staff at their facilities, and whether staff are interested in what youth have to say. Youth were not instructed to consider staff with specific roles (e.g., frontline staff, frontline staff supervisors, counselors, etc.), but rather facility staff overall. Eight questions were not included in this study because they were not incorporated into the Youth Climate survey until October 2013 (two questions) or April 2014 (six questions). We, therefore, used variables measuring whether staff (a) seem to genuinely care about the residents; (b) are fair about discipline issues; (c) use force only when needed; (d) make more positive than negative comments to youth; (e) show residents respect; and (f) are good role models. Individual-level Spearman correlations indicated all six items were moderately correlated with one another (ρmin = 0.43, p < .001; ρmax = 0.70, p < .001).
For all youth who responded to at least 75% of the items, individual responses, coded on a scale from 1 to 3 (1 = No; 2 = Sometimes; 3 = Yes), were averaged into an individual-level mean score. Responses were then aggregated to the facility level. The responses of youth who responded to less than 75% of the items (5.1% of all youth) were not included in the aggregated scores. 45.30% of facility observations (N = 698) had no youth excluded from the facility score, with an average of 1.37 (SD = 2.23) youth excluded per facility observation. The resulting variable is a facility-level mean score ranging from 1 to 3, with higher values corresponding to more positive perceptions of staff. The measure displayed excellent reliability (α = .90).
Facility Characteristics
Facility demographics
The Administrative Form captured individual characteristics of the youth population, counting each youth once. Each facility reported the number of individual youths by gender (male; female) and race/ethnicity (White non-Hispanic; Black non-Hispanic; American Indian; Asian; Pacific Islander; White Hispanic; Black Hispanic; Other Hispanic; and Other). The proportion of females is measured by dividing the total number of female youth by the total number of youth in the facility during the collection period, and the proportion of White non-Hispanic is measured by dividing the total number of White non-Hispanic youth by the total number of youth in the facility during the collection period.
Facility type, urbanicity, and region
The type of facility (assessment, detention, or corrections) was recorded on the Administrative Form. PbS defines assessment facilities as short-term facilities that provide diagnostic and assessment tests for the purpose of placement, services, and/or treatment decisions and hold youth both pre- and post-adjudication; detention facilities as temporary custody facilities designed primarily for youth pending legal action; and corrections facilities as training schools, treatment facilities, and residential programs for adjudicated youth. Corrections facilities were measured as the reference category. Facility urbanicity (urban, suburban, or rural), and region of the United States (Western, South, Northeast, or Midwest) were recorded on the Administrative Form. Rural facilities were measured as the reference category for facility urbanicity, and West as the reference category for facility region.
Youth perceptions of facility
On the Youth Climate Survey, youth reported their perceptions of the conditions of the facility in four items: whether (a) the facility is clean; (b) everything functions in their unit; (c) the food is good; and (d) they have been given required clothing, shoes, sheets, towels, and toiletries (0 = No; 1 = Yes). Individual-level Spearman correlations indicated the four items were significantly correlated with one another (ρmin = 0.18, p < .001; ρmax = 0.39, p < .001). For all youth who responded to at least 75% of the items, responses were averaged into an individual-level score ranging from 0 to 1 and subsequently aggregated to the facility level. The responses of youth who responded to less than 75% of the items (2.3% of all youth) were not included in the aggregated scores. 63.50% of facility observations (N = 979) had no youth excluded from the facility score, with an average of 0.61 (SD = 1.09) youth excluded per facility observation. The resulting variable is a facility-level score ranging from 0 to 1, with higher values corresponding to more positive perceptions of the facility. The measure displayed acceptable reliability (α = .60).
Facility Practices
Facility length of stay, number of youth, and crowding
The Administrative Form included the average length of stay in days for youth released during the collection period, the average number of youths in each facility per day during the collection period, and the facility’s capacity. A proportion measuring facility crowding was created by dividing the average number of youth in each facility per day by the facility capacity. A value of 1 indicates that the facility was at full capacity during the collection period, whereas a value of less than or greater than 1 indicates that the facility was under or over capacity, respectively.
Facility restraint use
The total number of incidents that involved restraint use for reasons other than suicidal behavior was collected on the Incident Report Form. A binary measure was created that indicates whether each facility reported using restraints for non-suicide-related reasons during the collection period (0 = No; 1 = Yes). This measure does combine facilities with infrequent use with those that regularly restrain their residents, yet we consider it a baseline for restraint use, as any use may increase perceptions of punitiveness.
Staff rating of training on suicide
On the Staff Climate Survey, staff were asked to rate “training, daily communications, and follow through” at their facility regarding suicide prevention. Responses to the question were measured on a four-point scale from 1 (poor) to 4 (excellent). Individual-level responses were aggregated to the facility level, resulting in a mean score ranging from 1 to 4.
Analytic Plan
Four facility observations were removed due to missing data, resulting in 1,541 observations for analysis. Collinearity diagnostics between all variables were explored and indicated no evidence of multicollinearity (VIFmin = 1.16; VIFmax = 2.70). We first conducted descriptive statistics to describe facility characteristics, followed by bivariate correlations. Next, as facilities had multiple observations over time, we used a multilevel mixed-effects negative binomial model to determine whether positive youth perceptions of staff were associated with SDV, controlling for other facility characteristics. The model’s random effects are used with longitudinal data to model intra-cluster correlation (the correlation between a facility’s observations over time). This model is used with over-dispersed count data, and just over half (54.64%) of the 1,541 facility observations had zero instances of SDV. Analyses were conducted in Stata using the menbreg command (StataCorp, 2023). As we do not own the data, materials and code for the present study are not available.
Results
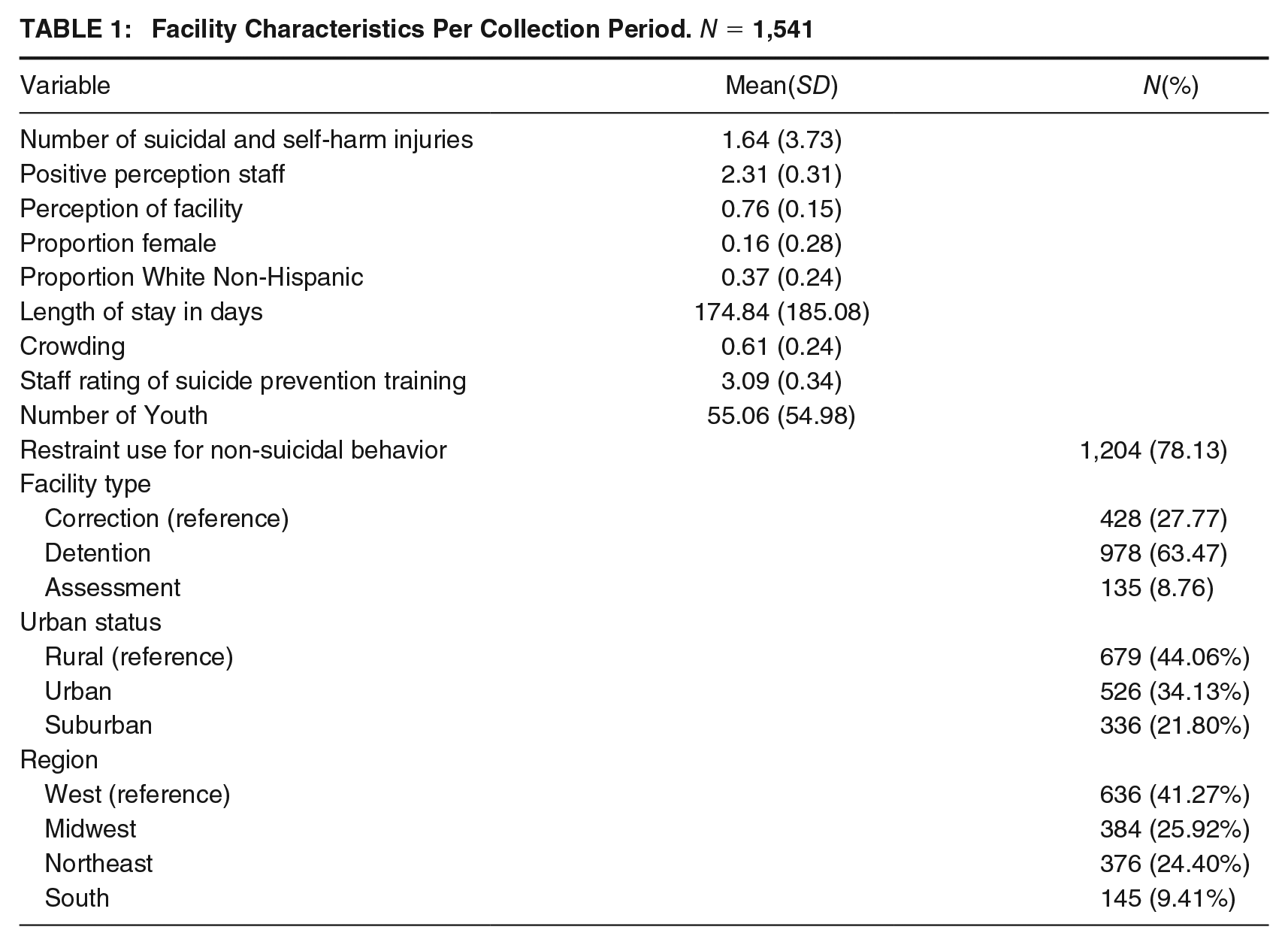
Descriptive statistics across all facilities and time periods are presented in Table 1. Facilities reported between 0 and 81 SDV injuries per 30-day reporting period, with an average of 1.64 injuries (SD = 3.73) per reporting period. On a scale of 1 to 3, youth detainees rated their perceptions of staff an average of 2.31. Within facilities, the proportion of youth detainees that were female (M = 0.16, SD = 0.28) and non-Hispanic White (M = 0.37, SD = 0.24) was low. Most facilities were located in rural areas (44.06%) and in the West (41.27%), and the majority (78.13%) used restraints for non-suicidal behavior. On average, youth were detained for 174.84 days (SD = 185.08) and facilities were under capacity (M = 0.61, SD = 0.24). Staff rated their training, daily communications, and follow-through on suicide prevention highly (M = 3.09; SD = 0.34). At the bivariate level, SDV was negatively correlated with youth perceptions of staff (ρ = −.22, p < .001; correlations table available upon request 1 ) and significantly correlated with all covariates but urbanicity (Urban: rpb = .01, p = .68; Suburban: rpb = −.02, p = .46; Rural: rpb = .01, p = .83) and facilities in the Midwest (rpb = .02, p = .48).
Facility Characteristics Per Collection Period. N = 1,541
Results from the multilevel mixed-effects negative binomial regression model are presented in Table 2. After accounting for facility characteristics and practices, average youth perceptions of staff were associated with a decrease in SDV injuries incidence-rate ratio (IRR = 0.61), but this finding was not statistically significant at the .05 level (95% confidence interval [CI] = [0.37, 1.01], p = .053). Facilities with a higher proportion of females (IRR = 2.44, p = .03) and white non-Hispanic youth (IRR = 2.58, p = .04) reported higher rates of SDV over time. Compared with rural facilities, suburban facilities had significantly lower rates of SDV (IRR = 0.59, p = .04), but there were no significant differences between rural and urban facilities (IRR = 0.68, p = .09). Facilities located in the Northeast (IRR = 0.41, p = .001) and Midwest (IRR = 0.56, p = .03) had lower rates of SDV over time compared to Western facilities. Neither youth perceptions of the facility nor facility type were significantly associated with rates of SDV. Facilities that used restraints for reasons other than suicidal behavior reported significant increases in SDV over time (IRR = 2.52, p < .001). Average staff ratings of suicide training were associated with a significant decrease in SDV (IRR = 0.57, p = .003). Average length of stay (IRR = 1.00, p = .61) and crowding (IRR = 0.65; p = .10) were not statistically associated with SDV.
Characteristics Predicting Facility-Level Rates of SDV Injuries. N = 1,541
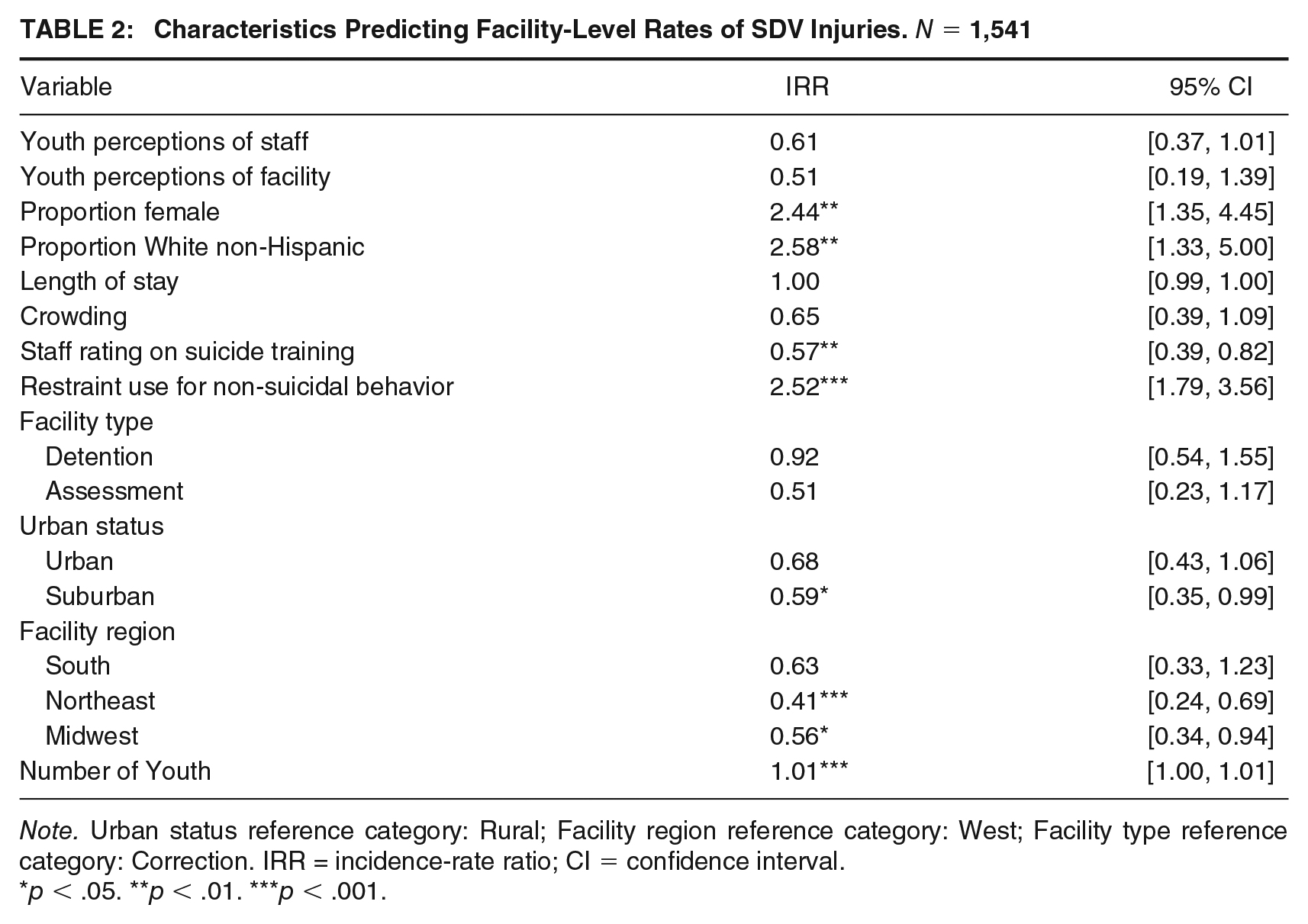
Note. Urban status reference category: Rural; Facility region reference category: West; Facility type reference category: Correction. IRR = incidence-rate ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
In a post hoc analysis (not pictured), we ran the multilevel mixed-effects negative binomial regression analysis separately by facility type and found that in detention facilities, positive staff–youth relationships were significantly associated with decreased self-harm and suicide events (IRR = 0.27, 95% CI: [0.11, 0.70], p = .007) and that in correction facilities, there was no significant relationship (IRR = 0.89, 95% CI: [0.49, 1.62], p = .71). The small sample size prevented a similar analysis for assessment facilities.
Discussion
The present study explored whether aggregate youth perceptions of juvenile facility staff are associated with facility-level rates of youth self-directed violence over time, measured as suicide and self-harm behaviors. Although prior research has identified the importance of positive adult relationships in suicide prevention in community contexts (Asarnow & Mehlum, 2019; Wyman et al., 2019), the present study uniquely examines youth detention and incarceration, in which the risk of SDV is higher than among the general population (Stokes et al., 2015; Teplin et al., 2015). Although the results did not reach the level of statistical significance (p = .053), the results do suggest that over time, juvenile facilities in which youth report more positive perceptions of staff report decreased rates of youth self-directed violence, after accounting for facility characteristics and practices. Spearman correlations do support a statistically significant and negative bivariate relationship between youth perceptions of staff and SDV, and the effect size (IRR = 0.61) suggests this finding is practically significant, particularly given the upper end of the 95% confidence interval, [0.37, 1.01]. This finding adds to a growing body of literature calling for improvements in youth perceptions of staff and staff–youth relationships in juvenile settings (e.g., C. Brown et al., 2019) and holds direct implications for research, policy, and practice.
The results highlight key facility characteristics that are associated with rates of SDV within juvenile justice facilities. Facilities with a higher proportion of females have higher rates of SDV, reinforcing previous research indicating that girls are more likely to report suicidal ideation, suicide attempts, and self-harm in juvenile justice facilities (e.g., Jin et al., 2021; Joshi & Billick, 2017). Second, facilities with a higher proportion of White non-Hispanic youth have higher rates of SDV, in line with previous research (e.g., Joshi & Billick, 2017; McReynolds et al., 2017). However, this finding is contrary to facility-level research suggesting that higher populations of Black youth in juvenile facilities are associated with increased rates of suicide attempts and deaths (Gallagher & Dobrin, 2006).
Average youth perceptions of the facility (cleanliness, functionality, quality of food, whether youth had been given necessary clothing, sheets, towels, and toiletries) were not significantly associated with rates of SDV over time, yet the bivariate correlation between average youth perceptions of staff and facilities was relatively high (ρ = .73; p < .001). While this correlation could suggest that youth conflated facility and staff experiences with one another, exploratory factor analyses, reliability statistics, and collinearity diagnostics suggest otherwise. Rather, this supports prior arguments that staff–youth relationships and youth perceptions of staff contribute to the overall functionality of juvenile facilities (Pederson et al., 2021; Schubert et al., 2012). Furthermore, average youth perceptions of both staff and facilities were significantly and negatively correlated with SDV (staff: ρ = −.22, p < .001; facility: ρ = −.21, p < .001). It is possible that the independent effects of perceptions of staff and of facilities on rates of SDV wash one another out, such that an underlying interaction is present. Future individual-level research could better inform how youths’ perceptions of the facility and of staff interact.
Results regarding facility type, urbanicity, and region were mixed. First, facility type (assessment, detention, or correction) was not significantly associated with SDV after controlling for other factors. However, in the post hoc analyses, positive youth perceptions of staff were significantly associated with SDV in detention facilities but not in correction facilities. Youth profiles in each of these types of facilities (higher needs compared to lower needs) could be influencing the outcomes, and future research should explore how youth needs are associated with self-harm and suicide rates. Second, in line with previous findings regarding rates of suicide in the United States (e.g., Rossen et al., 2018), suburban facilities have significantly lower rates of SDV relative to rural facilities, and Western facilities report higher rates of SDV compared with Northeastern and Midwestern facilities. However, we found no significant differences between urban and rural facilities and between Western and Southern facilities. Even so, given the salience of racial, ethnic, and gender identities and the geographic location of facilities, future research must consider intersectional identities and geographic characteristics for a more complete understanding of the relationship between demographics and SDV in juvenile facilities.
As expected (see Gallagher & Dobrin, 2006), the use of restraints for reasons other than suicidal behaviors was associated with an increase in SDV even after controlling for youth perceptions of staff, facility characteristics, and facility practices. Although we are unable to determine the reasons for which restraints were used in each facility, their use may increase perceptions of facility punitiveness, which in turn may negatively affect youths’ perceptions of staff and facilities. After all, restraint use was significantly and negatively correlated with both perceptions of staff and facilities (perceptions of staff: ρ = −.33, p < .001; perceptions of facility: ρ = −.33, p < .001). Further supporting prior research (Gallagher & Dobrin, 2006; Hayes, 2009) we found that facility crowding was not significantly associated with rates of SDV.
We found that the average staff rating of suicide training at their facility was high (M = 3.09 on a scale from 1 to 4), consistent with prior research finding that most juvenile correctional staff agree that their training on suicide risk and mental health screenings are adequate (Gagnon & Swank, 2021; Swank & Gagnon, 2017). Encouragingly, we found that average staff ratings of suicide training is associated with decreased rates of SDV over time, controlling for youth perceptions of staff, facility characteristics, and facility practices. This finding provides support that, beyond improvements to staff mental health knowledge (Penn et al., 2005), staff suicide prevention training, communications, and follow-through can have direct and positive impacts on the safety and well-being of detained youth. This finding is also encouraging for the implementation of suicide prevention programs such as SPI (Stanley & Brown, 2012) and YMFHA (Ross et al., 2023) in juvenile justice facilities. We did not have access to data regarding the dosage or content of staff training, and therefore more research is needed to understand what trainings are effective, and how communications and protocols can be implemented effectively and with fidelity to prevent youth SDV in juvenile justice facilities.
Unlike previous research (Casiano et al., 2016), our results indicated that the average length of time youth were detained in facilities is not associated with rates of SDV. However, our finding is in line with prior research examining suicide and suicide attempts, a subset of SDV, in juvenile facilities, specifically (Gallagher & Dobrin, 2006; Hayes, 2005). It is possible that the disaggregation of our dependent variable into two separate measures of self-harm and suicidal injuries would result in findings more consistent with this prior research.
Strengths, Limitations, and Future Directions
The conclusions drawn from the present study are strengthened by several study characteristics. First, the study is highly ecologically valid, given that we used official records and reports from juvenile facilities and detained youth. Second, unlike much of the other research in this area, the present study is longitudinal, which allows us to more confidently understand the temporal ordering. Finally, we used a strengths-based approach to consider how positive staff–youth relationships may be associated with SDV reduction.
The findings from the present study are tempered by limitations. Primarily, the present study was conducted at an ecological level; facilities, rather than individuals, were measured over time. By aggregating individual-level responses to the facility level, statistical power is limited, we are unable to make individual-level inferences, and we are unable to detangle individual-level variations in perceptions of staff. It is possible that individual youth characteristics pertaining to mental health and suicidality may drive both individual and facility-level SDV more so than facility-level perceptions of staff and/or facility characteristics and practices. In the same vein, a small number of youth in any given facility may be responsible for the majority of that facility’s SDV incidents. In addition, perceptions of staff may change frequently in juvenile facilities because of both youth and staff turnover. After all, youth were detained for an average of 174 days across all facilities in the sample, and research suggests that juvenile facilities have average staff turnover rates of 20% to 25% per year (Minor et al., 2011). Researchers should expand the present research to consider these individual characteristics.
We were also unable to control for facility-level variables unmeasured by PbS, such as staff and/or facility orientation toward rehabilitation, suicide risk screening at intake, onsite mental health care, and facility specialization, that are likely to be associated with risk for and treatment of SDV (see Casiano et al., 2016). The omission of these variables tempers our results, as it is possible they confound the relationship between youth perceptions of staff and SDV. Finally, although internal reliability was high (α = .90), the measure of youth perceptions of staff used has not been previously validated, considered facility staff as a whole rather than specific staff roles, and only assessed whether staff seem to genuinely care about the residents, are fair about discipline issues, use force only when needed, make more positive than negative comments to youth, show residents respect, and are good role models. Although these items are highly face-valid, the abbreviated length of the scale likely does not fully capture a youth’s view of correctional staff (e.g., if the staff follows through on their promises) or the different types of affective relationships that youth may have with correctional staff (see Marsh & Evans, 2009).
Future research should use an individual-level approach to investigate the relation between a youth’s perception of staff and their risk of SDV, as doing so would better allow researchers to control for individual SDV risk and for tests of the mechanisms through which youth perceptions and staff–youth relationships can be improved. Future research could also examine whether the relationship between youth perceptions of staff and SDV varies depending on staff roles, such as through a comparison of frontline staff and mental health care staff. Particularly, future research can build from the findings in the present study by leveraging research-practice partnerships to access more complex data that both advance research and practice. Dyadic analyses and multi-method studies of individual youth–staff relationships over time would better reveal the causal mechanisms between relationship quality and SDV.
Implications
Juvenile justice facilities have an obligation to prevent SDV among the youth under their care. Due to the decentralized nature of juvenile justice administration in the United States, each state maintains its own standards for juvenile residential facilities, including suicide prevention (see National Institute of Corrections, 2022). However, federal guidance from the Department of Justice requires that “the facility director ensures the facility has a suicide prevention program that identifies and responds to juvenile detainees who express suicidal behaviors or ideations” (Department of Justice, 2011, p. 27), implying that the onus is on employees and structures within the facility to respond to and prevent youth SDV. This issue is all the more urgent given the contemporary rise in youth internalizing disorders and SDV, particularly in light of the COVID-19 pandemic. Pre-, peri-, and post-pandemic research on SDV prevention has found that mental ill-health and suicidality have increased among adolescents (Bridge et al., 2023; Thompson et al., 2021), including among justice-involved youth (Reid et al., 2022).
Even as developmental science clearly articulates the importance of positive adult–youth relationships during adolescence for healthy development, including crime desistance (Cavanagh, 2022), recommendations from state-level juvenile justice task forces lack focus on relationships between youth and legal actors generally, let alone in the context of reducing the risk of SDV among detained youth (e.g., Iowa Supreme Court Juvenile Justice Task Force, 2023). Researchers continue to reiterate a need for facility-wide mental health, suicide, and self-harm education, intervention, and prevention training among frontline staff in juvenile justice facilities (Whitley et al., 2022). Although average staff ratings of training were unrelated to SDV in the present study, staff ratings may not reflect the quality, fidelity, or evidence-based nature of the training used in a given facility. Importantly, youth suicide intervention and prevention programs such as SPI can and should be adapted for implementation in juvenile justice facilities (Meza et al., 2022). The alignment of state and federal policy and funding with science is necessary to integrate evidence-based SDV prevention in juvenile justice facilities. The results from the present study suggest that it is imperative for such evidence-based practices to focus on building strong, positive interpersonal staff–youth relationships, as youth perceptions of staff are associated with rates of injury resulting from SDV.
Footnotes
Authors’ Note:
We have no known conflicts of interest to disclose. The findings reported in this manuscript have not been previously published. This research was conducted with access to the PbS Researchers Dataset. The views expressed are those of the author and do not reflect the view of PbS. This work was supported by the Annie E. Casey Foundation. The authors do not own the data, therefore materials and analysis code for this study are not available. No aspect of the study was preregistered.
Notes
![]() .
.