
Abstract
The present study examined the psychopathy-substance abuse nexus in a diverse Canadian sample of 420 justice-involved youth. The Psychopathy Checklist Youth: Version (PCL: YV) and a series of clinical and criminogenic substance abuse variables—assembled into a composite score that was corrected for missing indicators—were rated from court and treatment files and community recidivism was captured from criminal records. PCL: YV total, lifestyle, and antisocial facet scores showed strong convergence with clinical and criminogenic substance abuse indicators. Cox regression survival analyses demonstrated that certain indicators and the corrected composite incrementally predicted violent and general recidivism, controlling for PCL: YV total score across gender and ethnoracial groups. Kaplan–Meier survival analyses demonstrated that high psychopathy youth with medium or high substance-related concerns had steeper recidivism trajectories than low psychopathy youth with similar substance concerns. Results underscore the clinical and risk relevance of substance abuse and its intersection with juvenile psychopathy.
Drug and alcohol problems are well-established catalysts for youth justice system involvement, with survey research throughout Canada and the United States identifying youth justice populations to have particularly high base rates of substance use concerns (US Bureau of Justice Statistics, 2023; Vingilis et al., 2020). For instance, a large-scale survey by the US Bureau of Justice Statistics across juvenile justice facilities (2008–2018) revealed that 76% of youth in custody reported having ever used alcohol, 84% having ever used drugs, and that 60% met the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5; American Psychiatric Association, 2013) criteria for a substance use disorder 12 months prior to custody. Furthermore, meta-analytic findings consistently demonstrate substance use concerns to be a strong predictor of future crime and violence in justice-involved youth (Olver et al., 2014), yielding a small to medium effect (r = .20, k = 54, n = 97,511). Effects are particularly pronounced for female (r = .25, k = 19, n = 11,249) versus male samples (r = .19, k = 36, n = 41,311), suggesting substance concerns may have gender salience. Finally, national survey data also demonstrate that youth with substance-related concerns present an elevated risk for subsequently developing a substance use disorder in adulthood (McCabe et al., 2022); these youth also have high comorbidity with a range of internalizing and externalizing mental health concerns (Hemphälä & Tengström, 2010).
Psychopathy and Substance Abuse
Psychopathy is a serious personality disorder characterized by a constellation of interpersonal, affective, and lifestyle behavioral features that make it a clinically relevant criminal justice construct (Hare, 1996, 1999). Even in youth populations, the symptoms of psychopathy are extreme and maladaptive variants of personality, emotional, and behavioral functioning (e.g., egocentrism, lying, impulsivity, poor anger control) (Forth et al., 2003). Scores on a clinical rating scale prominently used to assess juvenile psychopathy, the Hare Psychopathy Checklist: Youth Version (PCL: YV; Forth et al., 2003), have demonstrated strong links to future crime and violence, with broadly medium effects for differentiating recidivist from nonrecidivist youth, particularly for violent and general recidivism (Olver et al., 2009). Moreover, confirmatory factor analytic research demonstrates that PCL: YV item scores can each be arranged into two factors or four narrower facets. Factor 1 subsumes the interpersonal (e.g., superficial, grandiose, deceitful) and affective (e.g., remorseless, callous, shallow affect) facets, while Factor 2 subsumes the lifestyle (e.g., impulsivity, irresponsibility, need for stimulation) and antisocial (e.g., poor behavior controls, release failure, criminal versatility) facets. With some exceptions, meta-analytic research has demonstrated that Factor 2 and its lifestyle and antisocial facets have particular relevance in predicting general and violent recidivism.
Psychopathy in general is associated with higher risks and needs in correctional samples (Simourd & Hoge, 2000), and specifically so within the juvenile literature in which high psychopathy youth are at higher risk and have a greater density of criminogenic needs (e.g., Lovatt et al., 2025; Stockdale et al., 2010). One such key domain is substance abuse and extant research supports the psychopathy-substance abuse link. In an early psychopathy-substance abuse study in a Canadian sample of 200 incarcerated men, Hemphill et al. (1994) found that Psychopathy Checklist-Revised (PCL-R; Hare, 1991, 2003) total scores and Factor 2 specifically had strong associations with drug abuse/dependence diagnoses (r = .35), number of substances tried (r = .34), and was inversely associated with age at first alcohol intoxication (r = −.25); psychopathy diagnoses, however, had low comorbidity with substance-related diagnoses. A meta-analysis of four studies (n = 759) demonstrated that PCL total score and particularly Factor 2, had moderate associations with alcohol abuse/dependence (r = .27) and drug abuse/dependence (r = .38), while Factor 1 had small associations with these criteria (r = .09 and .12, respectively).
In subsequent years, reliable links have been found between PCL-measured psychopathy and substance use concerns. For instance, in a U.S. jail sample of 399 incarcerated persons, Walsh et al. (2007) found that PCL-R scores, and particularly its lifestyle and antisocial dimensions, were significantly correlated with symptom criteria across alcohol and drug use categories (r = .11 to .27). Moreover, PCL-R total score and Factor 2 associations were invariant across White and Black subgroups for alcohol and cannabis symptoms, but the association held only for White individuals with respect to opioid or cocaine symptoms. Moreover, in a large British community dwelling sample (N = 638), Coid, Yang, Ullrich, Roberts and Hare (2009) found that the Psychopathy Checklist: Screening Version (PCL: SV; Hart et al., 1995) total score and its antisociality domain had significant associations with drug dependence, heroin, and amphetamine use, while associations with alcohol abuse criteria were not significant. In a British prison sample (N = 496), Coid, Yang, Ullrich, Roberts and Moran (2009) found that PCL-R total, lifestyle, and antisocial facet scores had significant associations with use of seven different categories of substances (including alcohol); interpersonal and affective facet scores also had associations with sedative and cocaine use but not other substances. Finally, in an adult community sample (N = 318), Schulz et al. (2016) found that PCL: SV measured Factor 1 yielded inverse associations with drug use and dependence in women (possibly representing the inconsistent and varied association of the interpersonal and affective features with substance use), while Factor 2 yielded positive associations across gender groups.
Research elsewhere has established the psychopathy-substance use connection beyond the PCL measures and across samples. For instance, in a large U.S. multisite study of correctional, forensic, and two university samples, total scores from various self-report measures of psychopathy including the Psychopathic Personality Inventory (PPI; Lilienfeld & Andrews, 1996), Hare Self-Report Psychopathy (SRP-III; Paulhus et al., 2016), and Levenson Self-Report Psychopathy (LSRP; Levenson et al., 1995), had broadly medium-range correlations (r = .21 to .43) with self-reported indicators of problematic substance use (Sellbom et al., 2017). Within each sample, and per previous lines of research, scores on the impulsive antisocial features of psychopathy demonstrated stronger associations with substance abuse criteria (r = .17 to .45) than measures of the interpersonal and affective features (r = −.12 to .30); none of the associations were moderated by gender (Sellbom et al., 2017).
Psychopathy and Substance Abuse in Youth Samples
Subsequent lines of research extended to youth populations have examined the psychopathy-substance abuse nexus. For instance, in a Swedish sample of 180 youth (99 girls, 81 boys) outpatient substance abuse referrals, PCL: YV total score and specifically, its antisocial and lifestyle features, were significantly correlated with alcohol and drug abuse diagnoses across genders (rs = .30 to .50) (Hemphälä & Tengström, 2010). Although the interpersonal and affective features were also associated with diagnoses among boys only, in regression analyses, only the lifestyle and antisocial features uniquely predicted diagnosis across gender groups (Hemphälä & Tengström, 2010). In a Dutch community school sample of 387 girls and 341 boys, Youth Psychopathic Traits Inventory (YPI) total scores and its grandiose-manipulative and impulsive-irresponsible domains had significant small to medium correlations with self-report measures of drug and alcohol problems (rs = .13–.35); for boys, the callous unemotional domain was also associated with both sets of substance-related concerns (Hillege et al., 2010). In a U.S. custodial sample of 373 justice-involved youth, Kimonis et al. (2012) found that YPI scores were significantly correlated with pre-incarceration substance use (r = .21) and institutional substance use (r = .17). Moreover, a juvenile psychopathy variant characterized by particularly prominent antisocial lifestyle features had the highest rates of both sets of substance use concerns.
However, the psychopathy-substance abuse links have not necessarily been a fait accompli, as samples elsewhere have demonstrated less consistency in yielding the above associations. For instance, in a small Japanese custodial sample of 57 youth, PCL: YV score was not significantly associated with self-reported drug or alcohol problems (Matsumoto et al., 2006). Moreover, in a U.S. sample of 64 male adolescents referred to substance abuse treatment, PCL: YV scores were not significantly related to age at first drug use or number of drugs used, although the total score and Factor 2 score had small positive associations with drug trafficking arrests (r =.16 and .15, respectively; O’Neill et al., 2003a). Finally, in a U.S. custodial sample of 94 justice-involved girls, Vaughn et al. (2008) found Impulsivity scores from the Antisocial Process Screening Device (APSD; Frick & Hare, 2002) to be significantly correlated with past year drug use severity (r = .26) as were Blame-External scores from the PPI-Short Form (r = .21); however, no other subscales from these measures were significantly correlated with drug abuse.
The Psychopathy-Substance Abuse Nexus and Rationale for the Current Study
The extant literature demonstrates an association between psychopathy, particularly its lifestyle and antisocial features, with substance abuse across samples, measures, gender and ethnoracial groups. The link has been most heavily examined in adult criminal justice samples. Similar findings have emerged in youth samples, particularly juvenile justice populations, although the association appears to vary somewhat, with inconsistency observed in substance abuse associations with the interpersonal and affective domains of psychopathy. Although some preliminary lines of research have demonstrated that psychopathy may moderate the relationship of substance abuse to violent criminal charges (Vincent et al., 2024), to our knowledge, this has only been examined in adult samples in a postdictive fashion (i.e., with prior criminal history vs community recidivism), and without interrogating this joint association as a function of gender or ethnoracial heritage. Finally, previous studies have used limited indicators of substance-related concerns (e.g., history of use, symptom count, self-report measures), versus a multimethod approach that includes both clinical and criminogenic indicators of substance-related concerns.
The psychopathy-substance abuse nexus has implications for forensic assessment, risk management, and the prevention of future crime and violence per the principles of risk (matching treatment intensity with risk level), need (prioritizing dynamic risk factors for treatment), and responsivity (individualizing service delivery using cognitive behavioral methods of change) (Bonta & Andrews, 2024). The present study aimed to redress gaps in the extant literature with implications for service delivery through examining the psychopathy-substance abuse nexus with links to recidivism in a large and diverse justice-involved sample of youth. Using a set of clinical and criminogenic indictors of substance-related concerns we hypothesized that: (1) PCL: YV scores, particularly its lifestyle and antisocial facets, would be significantly correlated with measures of substance abuse; (2) Substance abuse indicators and a composite measure would predict violent and general recidivism; (3) Substance abuse measures would predict recidivism in an additive and incremental manner over and above PCL: YV score, and that youth scoring high on both domains would have higher and faster rates of recidivism than youth scoring lower on either one or both domains; and (4) that the above associations by and large would emerge across gender (male vs female) and ethnoracial (Indigenous vs non-Indigenous White majority) groups.
Method
Sample
The present study sample consists of 420 court-adjudicated youth referred for forensic assessment and/or intervention services at an urban community mental health outpatient facility in the Canadian prairie province of Saskatchewan between 1996 and 2013. The sample was extracted from two previous samples in published studies (Lovatt et al., 2025; Stockdale et al., 2010) that featured an examination of dynamic violence risk and need that prioritized youth with violent offense histories. As the present study is archivally based, the availability of information on participant characteristics and program involvement varied considerably and is reported accordingly. At the time of referral, the youth were 16.4 years of age (SD = 1.5, range age 12–20, n = 420), and about two thirds (68.3%, n = 287) were male, and one third, female (31.7, n = 133). Ethnoracial data were not consistently reported in file documents but were available for 88.3% (372/420) of youth; most youth were Indigenous (73.9%, n = 275/372) and 26.1% (n = 97/372) were non-Indigenous (White majority). Intersectionally, this was broken down into 46.5% (173/372) Indigenous male, 21.0% (78/372) non-Indigenous male, 27.4% (102/372) Indigenous female, and 5.1% (19/372) non-Indigenous female.
Most of the sample (66.8%, n = 250/374) had a conviction history prior to their index offense, and approximately half had a previous charge or conviction for a violent offense (51.1%, n = 191/374). As a court-referred sample to a specialized set of forensic community services, these youth were generally higher risk-need than the general youth justice population. Accordingly, most youth had an index conviction for a violent offense (79.1%, 317/401), which included both sexual and nonsexual violent offenses. At the time of referral, about one-half of the youth (56.1%, n = 210/374) were not attending school, and most (83.1%, n = 301/362) had a history of suspension or expulsion. Most youth were residing with one or more parental figures (45.8%, n = 184/402), followed by youth custody (20.4%, n = 82/402), group home/foster care (12.7%, n = 51/402), other relatives (12.2%, 49/402), and 9.0% other living arrangement (e.g., friends, supported living, independent, transient).
Measures
PCL: YV
The Psychopathy Checklist: Youth Version (PCL: YV; Forth et al., 2003) is a 20-item symptom construct clinical rating scale designed to assess the features of psychopathy in youth. Items are rated on a 3-point ordinal scale representing the extent to which the item applies in whole (2), partially (1), or not at all (0) for the youth evaluated. Possible scores range from 0 to 40, representing the density and severity of psychopathic features. Confirmatory factor analytic research demonstrates the items can be arranged into two factors subdivided into four facets: Factor 1, which subsumes the interpersonal (e.g., impression management, grandiose, deceitful) and affective (e.g., lacks remorse, callous/lack of empathy, shallow emotion) facets, and Factor 2, which subsumes the lifestyle (e.g., proneness to boredom/need for stimulation, impulsivity, irresponsibility) and antisocial (e.g., poor anger controls, serious criminality, criminal versatility) facets. The PCL: YV does not have an item pertaining specifically to substance abuse, although youth substance use involvement may contribute to higher ratings on certain items (e.g., proneness to boredom/need for stimulation, impulsivity). The interrater reliability of PCL: YV scores was examined in each of the samples comprising the current study sample, and was reported to be generally high as follows: Stockdale et al. (2010; 25 double coded cases) PCL: YV total ICCA1 = .91, interpersonal ICCA1 = .60, affective ICCA1 = .66, lifestyle ICCA1 = .89, antisocial ICCA1 = .84; Lovatt et al. (2025; 27 double coded cases) PCL: YV total ICCA1 = .96, interpersonal ICCA1 = .86, affective ICCA1 = .84, lifestyle ICCA1 = .78, antisocial ICCA1 = .90.
Substance Abuse Variables
Five substance abuse indicators, three clinical and two criminogenic, were extracted from file and integrated to generate a composite variable to examine psychopathy outcome relations.
Diagnosis
Referred to any Diagnostic and Statistical Manual of Mental Disorders IV or IV-TR (APA, 1994, 2000) diagnosis of a substance-related disorder coded yes-no (1–0) as documented on file, provided by a pediatric psychiatrist or registered psychologist.
APS-SF clinical concern rating
The Adolescent Psychopathology Scale-Short Form (APS-SF; Reynolds, 2000) is a 115-item multidimensional measure of youth mental health concerns comprising 12 scales; it is the abbreviated version of the full-length APS proper. Item ratings are converted to T-scores and are interpreted as no concern (T = < 60), subclinical (T = 60–64), mild clinical (T = 65–69), moderate clinical (T = 70–79), and severe clinical symptom range (T ≤ 80). Clinical concern severity ratings were rescaled from 0 (no concern) to 4 (severe). For the present study, the APS-SF substance abuse scale was employed.
Intake substance abuse severity rating
Upon intake, clinicians completed a substance abuse severity rating scored on a 5-point Likert-type scale (1 none to 5 severe) based on the youth’s current and previous substance use history. This was part of a routine inhouse intake procedure introduced in Lovatt et al. (2025) to prioritize services and had yet to be empirically validated.
YLS/LSI-Sk substance abuse need domain
The Youth Level of Service/Case Management Inventory (YLS/CMI; Hoge & Andrews, 2003) was rated archivally on a subsample of youth from a previous investigation (Olver et al., 2012), while Level of Service Inventory-Youth Saskatchewan Edition (LSI-Sk; Andrews et al., 2001) risk and need ratings were extracted from presentence reports on the other subsample as reported in Prince et al. (2021). Each measure is a youth-adapted general-risk need measure derived from the family of Level of Service Inventory measures, specifically, the Level of Service/Case Management Inventory (Andrews et al., 2004). The item content of each measure is arranged into eight risk-need domains; for the present study, the substance abuse domain was examined, specifically whether it was identified as moderate or high need (coded 1), versus low or no need (coded 0).
VRS-YV substance abuse dynamic item
The Violence Risk Scale-Youth Version (VRS-YV; Wong et al., 2004-2011) is a dynamic violence risk assessment tool for youth comprising four stable and 19 dynamic items. Items are scored on a four-point ordinal scale (0, 1, 2, 3), with higher ratings scores representing a link to increased violence risk; items with scores of 2 or 3 are considered criminogenic and are prioritized for services. For the present study, VRS-YV item D12 Substance Abuse (i.e., the link between substance abuse and violence) was examined.
Substance abuse composite variable (residualized)
The five indicators were dichotomized and integrated to create a substance abuse composite variable reflecting clinical and criminogenic problems with substance abuse: DSM diagnosis present (1 yes, 0 no); Clinical intake rating 4 or 5 (yes 1, no 0); APS-SF substance abuse clinical concern rating moderate or severe (yes 1, no 0); YLS/LSI-Sk substance abuse rating moderate or high (yes 1, no 0); and VRS-YV D12 substance abuse dynamic factor rating of 2 or 3 (yes 1, no 0). Listwise deletion of a large amount of missing data (e.g., all cases without complete information across all measures) wastes valuable data, can introduce severe bias, and result in a massive loss of statistical power, increasing type II errors (Allison, 2002; van Ginkel et al., 2020); however, use of multiple imputation to estimate missing data for certain variables become unstable when missingness exceeds 50% (Junaid et al., 2025). To account for and minimize the influence of missing data that varied across measures we employed a three-step strategy to generate a three-level composite variable controlling for missing data; (1) evidence of any criminogenic issue with substance abuse from either the LSI-Sk or VRS-YV rating; (2) evidence for a clinical problem with substance abuse from any of the intake rating, APS-SF scale, or DSM diagnosis; and (3) generating a corrected substance abuse composite variable for analysis by statistically controlling for the number of missing indicators.
Cases that were missing information across all indicators for either domain were excluded; of the 352 included cases 14.8% (n = 52) had no missing indicators, 47.2% (n = 166) 1/5 missing, 35.5% (n = 125) 2/5 missing, and 2.6% (n = 9) 3/5 missing. Each case had presence/absence information available from at least one indicator on each of the criminogenic and clinical domains, coded across 3 points (0, 1, 2): evidence of no criminogenic or clinical substance-related concerns (0); evidence for one substance-related concern, either criminogenic or clinical (1); and evidence that substance abuse is both criminogenic and clinically relevant (2). Given that 85% of cases still had missing information from at least one or more indicators, this would have the net effect of underestimating the number of substance-related concerns on clinical and/or criminogenic domains. To correct for missing data, we regressed the substance abuse composite variable on the number of original missing indicators and saved the unstandardized residual; the resulting residualized substance abuse composite variable score (i.e., actual composite variable score—predicted composite variable score) represents the level of substance-related concerns across clinical and criminogenic domains independent of the original number of missing indicators. This serves as a more reliable and corrected index of substance-related concerns independent of the number of missing values.
Recidivism
Recidivism information was coded from official criminal records obtained from the Canadian Police Information Centre (CPIC), a comprehensive national criminal record database maintained by the Royal Canadian Mounted Police (RCMP). Recidivism was defined as any new criminal conviction for an offense incurred following referral for services; for youth in custody at the time of services, this would entail offenses committed post-release. Violent recidivism included any offense against the person with the potential for physical, verbal, or psychological harm (e.g., assault, homicide, robbery), including sexual offenses. General recidivism included any new offense committed be it violence as operationalized above or nonviolent (e.g., property offenses, drug offenses, breaches). Recidivism was coded in binary manner (1 yes, no 0) along with the date of first disposition for a given offense category to permit computation of time to first conviction for survival analysis. All recidivism data were coded following the completion of ratings or other data capture on all other study measures.
Procedure
The present study was conducted as part of a larger dynamic violence risk youth project and involved combining two samples to increase sample size and, therefore, statistical power, and to expand the inclusion of new variables that would permit addressing new research questions not previously examined on smaller independent samples. Specifically, the substance abuse variables detailed above represent novel data collected across two samples, and the generation of a substance abuse composite variable is a new measure developed to comprehensively capture the substance abuse construct that is the focus of the present study. Each study received ethical approval from the university research ethics board, operational approval from the Saskatchewan Health Authority, and legal approval from a Youth Court Judge of the Saskatchewan Law Courts. The present study received ethical approval (certificate no. 5872) from the University of Saskatchewan Behavioural Research Ethics Board to combine the datasets from these two studies for analysis. The data gathered for the present study included demographic information, clinician-rated measures, self-report and outcome data, briefly described below. The present study features the use of protected or copyrighted materials to collect highly sensitive data on a vulnerable population; the authors do not have ethical, legal, or operational jurisdiction to release these data, and as a result, these data, as well as most study measures, are not publicly available; they can be obtained by consulting the test publisher of each measure. This study was not preregistered.
The PCL: YV was rated archivally from Court and treatment files in Lovatt et al. (2025) and Stockdale et al. (2010); the former also included a smaller subset of PCL: YV ratings completed on actual cases in the field. This also applied to the YLS/CMI and VRS-YV ratings (including the substance abuse item content on each measure) while the LSI-Sk ratings were extracted from youth presentence reports located on file. In Stockdale et al. (2010), Dr. Adelle Forth trained the team, which included a doctoral-level psychologist, a senior clinical psychology doctoral student, and a registered clinical social worker, on the PCL: YV; the doctoral psychologist, in turn, trained the group on the other risk measures, completing a set of randomly selected files to calibrate ratings prior to commencing independent coding. In Lovatt et al. (2025), a senior clinical psychology doctoral student and a senior undergraduate honors student completed ratings on the study measures from file, and they were trained and supervised by two of the personnel (both doctoral-level psychologists) from Stockdale et al. (2010) using the same calibration methodology.
The remaining substance abuse measures, as noted above, were culled from a set of routine clinical intake procedures or incorporated from measures obtained from forensic assessments. DSM IV or IV-TR diagnoses were frequently assigned by a court-ordered pediatric psychiatrist and/or a registered psychologist providing services on referral, while substance abuse intake severity ratings were similarly completed by the referred clinician as noted above. The APS-SF was frequently administered across samples described in Stockdale et al. (2010) and Lovatt et al. (2025)—in the former, T scores were recorded from files for APS-SF scales, while for the latter, clinical concern categories had been extracted—and as such, all APS-SF ratings were retained as, or converted to, clinical concern categories to permit analysis. As noted previously, recidivism data were coded via CPIC following the coding and capture of all other study measures.
Data Analytic Strategy
The analyses proceeded in several stages using SPSS v.31 and were linked explicitly to study hypotheses, representing a common set of recidivism prediction metrics to examine predictive validity (Hanson, 2022). The residualized substance abuse composite variable was used for all analyses, with the exception of basic descriptives, which employed the raw uncorrected composite variable for descriptive purposes. For these initial analyses, we also conducted gender and Indigenous group comparisons across each substance abuse measure via standardized mean difference (Cohen’s d) in which d magnitudes of .20, .50, and .80 correspond to small, medium, and large effects, respectively (Cohen, 1992).
Second, to examine the convergence of psychopathy and its dimensions with substance abuse, we computed Pearson correlations between PCL: YV total and facet scores with substance abuse measures in the aggregate sample and among gender and ethnoracial subgroups. Bivariate correlations between two sets of continuous variables were interpreted as .10 small, .30 medium, and .50 large (Cohen, 1992). Third, to examine the criminogenic relevance of the substance abuse measures, we conducted receiver operator characteristic (ROC) curve analyses for fixed 3- and 5-year violent and general recidivism; the two follow-ups were intended to represent shorter versus longer term periods in the life of a youth. ROCs generate an area under the curve (AUC) value ranging from 0 to 1, representing the probability that a randomly selected recidivist has a higher score than a randomly selected nonrecidivist. With .50 representing chance level predictive accuracy, values of .56, .64, and .71, respectively, represent small, medium, and large effects (Rice & Harris, 2005). ROCs were conducted in the aggregate sample and across demographic groups.
Fourth, to examine the extent to which substance abuse, clinically or criminogenically, is additive and incremental beyond individual levels of juvenile psychopathy (i.e., youth scoring high on both substance abuse and psychopathy would have higher and faster rates of recidivism than youth scoring lower on either one or both domains), we conducted a series of Cox regression survival analyses. The analyses simultaneously entered PCL: YV total score followed by the residualized substance abuse composite score to examine incremental predictive associations of violent and general recidivism over time. Taking an intersectional approach, the analyses were conducted for Indigenous and non-Indigenous male youth, female Indigenous youth, and for the aggregate sample, including youth with known versus unknown ethnoracial heritage; these analyses would ascertain to what extent a psychopathy-substance abuse nexus exists in the sample as a whole, and among specific gender x ethnoracial groups. As a survival analytic technique, Cox regression adjusts and controls for individual differences in follow-up time and generates a hazard ratio (eB) representing the percent change in hazard for an unwanted outcome (i.e., recidivism), per one unit change in the predictor. Incremental validity is demonstrated when a given predictor is significantly associated with a given outcome, controlling for other predictors; significant associations for both psychopathy and substance abuse measures indicate that each contributes unique risk-relevant information in the prediction of outcome.
The Cox regressions were then extended to include all six sets of substance abuse indicators across broad gender and ethnoracial groups to extend the incremental validity findings. Each indicator was examined given that associations for each of the individual indicators have relevance for the psychopathy-substance abuse nexus, beyond the residualized composite variable. To examine gender and ethnoracial invariance of observed effects, we employed meta-analysis (Comprehensive Meta-Analysis 3.0; Borenstein et al., 2015) to examine the incremental predictive validity of substance abuse in two ways: (1) between groups meta-analysis of hazard ratios across independent gender and ethnoracial groups; measures of effect size heterogeneity (Q and I2 statistics) would indicate if there is a significant difference in hazard ratios between groups—no difference would represent gender or ethnoracial invariance of observed effects—while the aggregate hazard ratio would represent whether a significant incremental effect exists across groups; and (2) within-groups meta-analysis of dependent incremental effects across the five substance abuse indicators within a given gender or ethnoracial group, compared to the incremental effects of the composite variable in the same group. The latter is a conservative strategy that generates a weighted overall effect controlling for dependency, so that each effect for a given measure is not treated as a separate effect when aggregating (which would shrink standard errors and increase type 1 error).
Finally, we conducted a set of Kaplan–Meier survival analyses on the aggregate sample on psychopathy and the residualized substance abuse composite variable. A PCL: YV score of 20, representing both the mean and median score for the sample, was employed to create high and low psychopathy groups, while the substance abuse composite variable was examined at three levels (based on the residualized composite score and its convergence with the 0, 1, 2 scaling of the raw composite variable) to create six comparison groups of high vs low psychopathy with low, medium, or high substance-related concerns, respectively. These analyses using categorical predictors aid interpretation of the Cox regressions which employ continuous predictors and have more complex interpretation; youth scoring higher on both measures should have higher and faster rates of recidivism than youth scoring lower on either measure.
Results
Sample Descriptives, Gender, and Ethnoracial Comparisons on Substance Abuse Measures
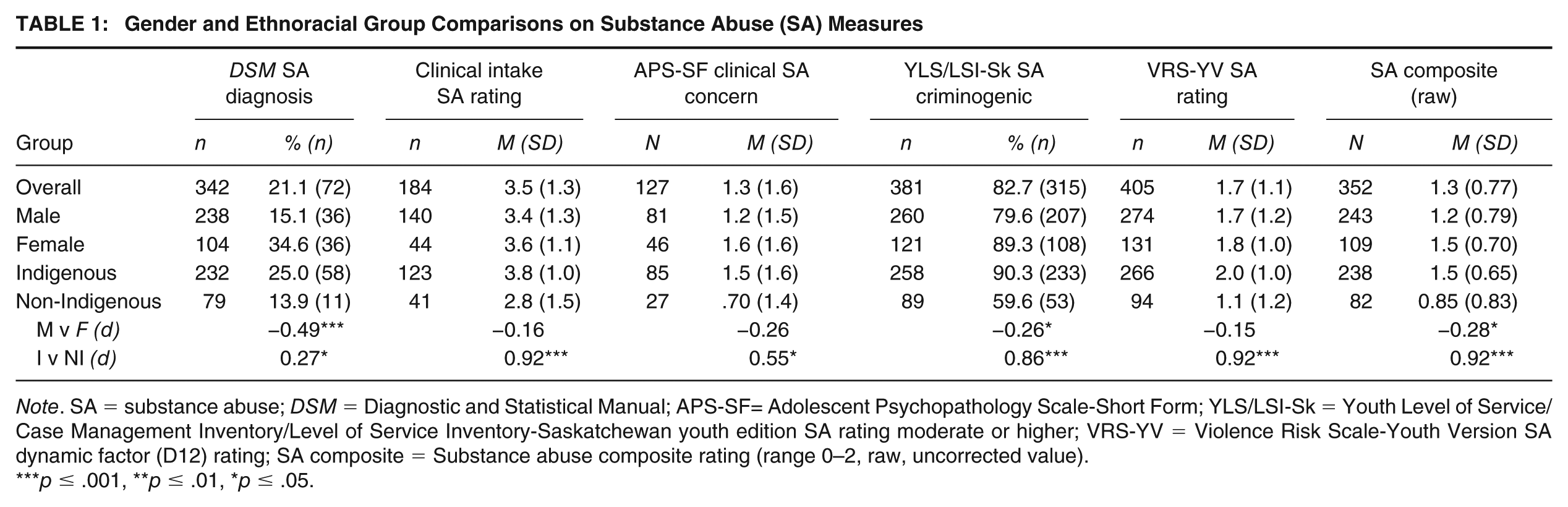
Table 1 reports descriptive statistics for the substance abuse measures in the aggregate sample and within broad gender and ethnoracial groups. Overall, one in five youth were identified as meeting symptom criteria for a DSM substance use diagnosis, with the rates being significantly higher in female and Indigenous youth. The clinical intake rating indicated at least moderate concerns in the sample overall (3.5/5, 58.2% scoring 4 or 5, n = 107/342), with Indigenous youth demonstrating a large effect for higher intake ratings compared to non-Indigenous youth. For the APS-SF substance abuse clinical concern rating, 31.5% of the sample (40/127) rated as moderate or severe, with Indigenous youth scoring significantly higher than non-Indigenous youth (medium effect). For the two sets of youth risk measures, related patterns emerged: a majority of the sample had substance abuse rated as criminogenic overall on the YLS/LSI-Sk substance abuse domain (82.7%, 351/381) or VRS-YV substance abuse item D12 (58.5% [237/405] scoring 2 or 3; M = 1.7, SD = 1.1). Indigenous youth had significantly higher criminogenic substance abuse ratings with large effects, while female youth had a significantly greater presence of substance abuse as a criminogenic need on the YLS/LSI-Sk domain.
Gender and Ethnoracial Group Comparisons on Substance Abuse (SA) Measures
Note. SA = substance abuse; DSM = Diagnostic and Statistical Manual; APS-SF= Adolescent Psychopathology Scale-Short Form; YLS/LSI-Sk = Youth Level of Service/Case Management Inventory/Level of Service Inventory-Saskatchewan youth edition SA rating moderate or higher; VRS-YV = Violence Risk Scale-Youth Version SA dynamic factor (D12) rating; SA composite = Substance abuse composite rating (range 0–2, raw, uncorrected value).
p ≤ .001, **p ≤ .01, *p ≤ .05.
On the raw substance abuse composite measure, 18.8% (66/352) of youth had a score of 0, 32.4% (114/352) a score of 1, and nearly half (48.9%; 172/352) had a score of 2; the overall mean was 1.3 (SD = 0.77) with Indigenous and female youth, respectively, scoring significantly higher than non-Indigenous (large effect) and male (small effect) youth. The residualized substance abuse composite generated via regression was a continuous variable; inspection of the distribution of unstandardized residuals (ranging from −1.589 to 1.098) enabled identification of cases where substance abuse problems were underestimated by the raw composite variable owing to a greater number of missing values. As would be expected, the number of missing indicators had a small negative correlation with composite score (r = −.22, p < .001), but was unrelated to Indigenous ancestry, gender, or any recidivism outcomes (rs = −.05 to .04, ns). Positive residual values represented the equivalence of a would be raw score of 2, values between 0 and −1 represented an equivalence of having at least one criminogenic concern, while residuals <−1.0 corresponded to the absence of substance-related concerns.
Convergent Associations With PCL: YV-Measured Youth Psychopathy
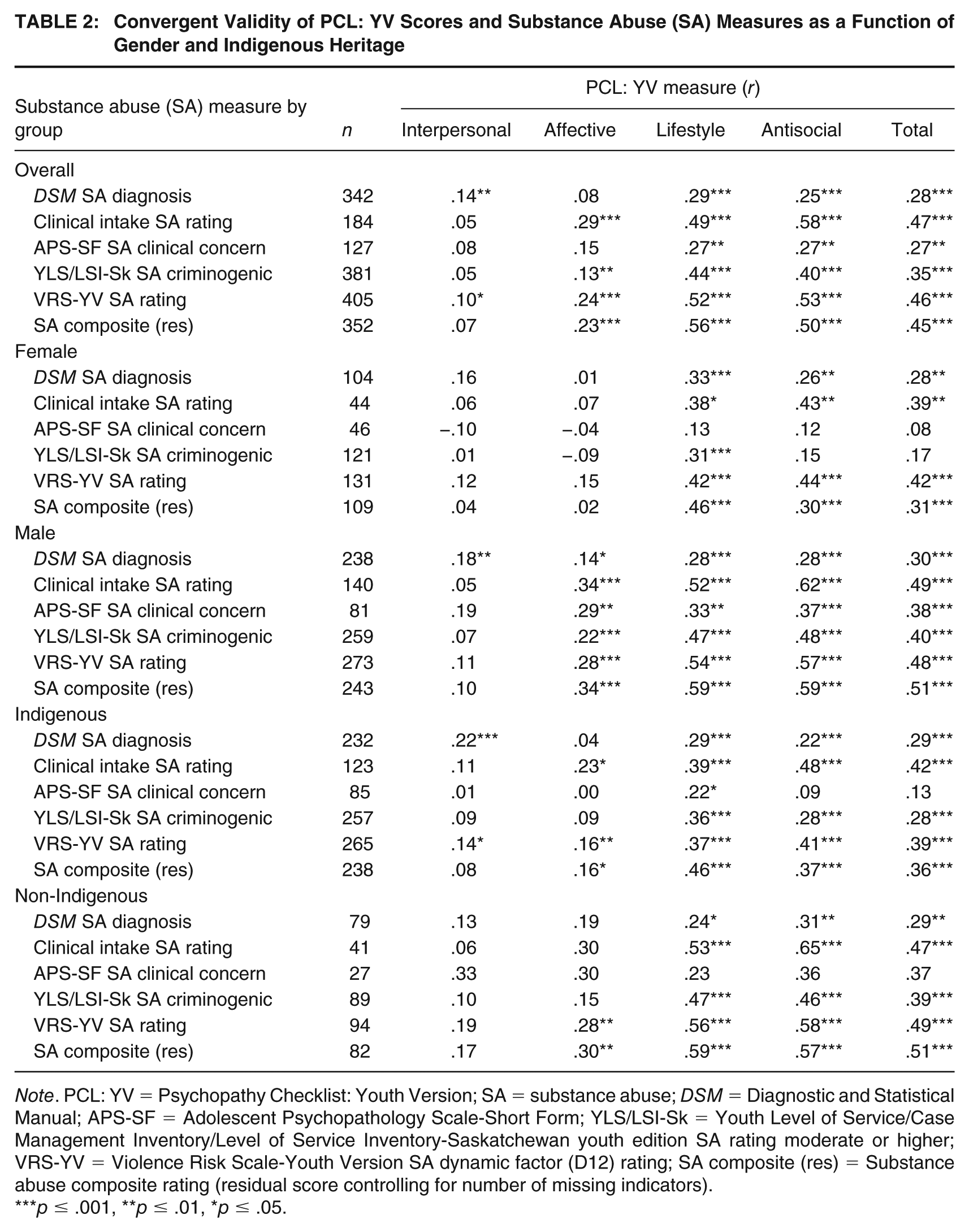
Table 2 presents the convergent validity correlation matrix for PCL: YV total and facet scores with the substance abuse measures, in the overall sample and within gender and ethnoracial groups. PCL: YV total, lifestyle, and antisocial facet scores had significant correlations across the substance abuse indicators, with the greatest variability seen in relations with the APS-SF substance abuse clinical concern rating. Small to medium in magnitude correlations were seen for female and Indigenous youth across these measures (r = .08 to .48) with PCL: YV total, lifestyle, and antisocial facet scores, while broadly medium to large correlations (r = .23 to .65) were observed for these associations with male and non-Indigenous youth. Affective facet scores were significantly correlated with all substance abuse indicators for male youth but none of these indicators for female youth; they had small to medium associations with clinical intake ratings, VRS-YV D12 scores, and the residualized substance abuse composite across ethnoracial groups. Interpersonal facet scores had the weakest associations, but had small and frequently significant effects with DSM substance use diagnosis.
Convergent Validity of PCL: YV Scores and Substance Abuse (SA) Measures as a Function of Gender and Indigenous Heritage
Note. PCL: YV = Psychopathy Checklist: Youth Version; SA = substance abuse; DSM = Diagnostic and Statistical Manual; APS-SF = Adolescent Psychopathology Scale-Short Form; YLS/LSI-Sk = Youth Level of Service/Case Management Inventory/Level of Service Inventory-Saskatchewan youth edition SA rating moderate or higher; VRS-YV = Violence Risk Scale-Youth Version SA dynamic factor (D12) rating; SA composite (res) = Substance abuse composite rating (residual score controlling for number of missing indicators).
p ≤ .001, **p ≤ .01, *p ≤ .05.
Predictive Associations of Substance Abuse Indicators With Community recidivism
The sample was followed up an average of 8.5 years (SD = 2.4) in the community, during which 56.4% (235/417) of youth incurred any new conviction after 3 years, 64.5% (263/408) after 5 years, and 70.3% (293/417) overall; the rates of violent reconviction were 35% (146/417) after 3 years, 44.4% (181/408) at 5 years, and 50.6% (211/417) overall. Three cases did not have recidivism information and an additional 11 cases did not have sufficient follow-up to be included in the 5-year fixed follow-up analyses. Higher overall rates of violent and general recidivism were found for Indigenous youth (59.1%, 162/274 and 77.4%, 212/274, respectively) relative to non-Indigenous youth (32.3%, 31/96 and 57.3%, 55/96, respectively) (χ2 = 20.51 and 14.27, respectively, ps < .001), as well as for male youth (54.9%, 156/284 and 75.4%, 214/284, respectively) relative to female youth (41.4%, 55/133 and 59.4%, 79/133, respectively) (χ2 = 6.68, p = .010 and 11.03, p < .001, respectively).
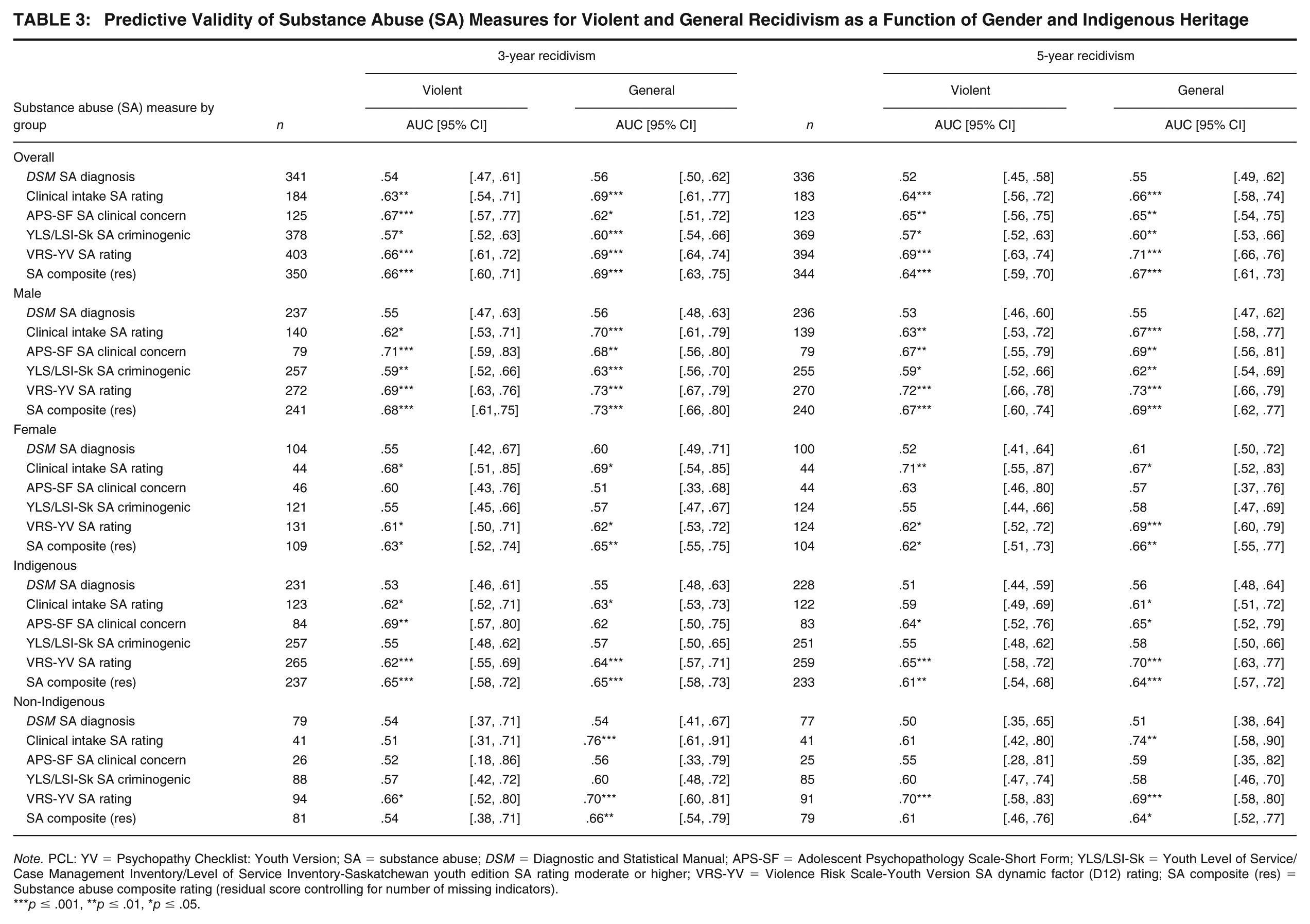
Table 3 reports bivariate associations (AUC) of the five substance abuse indicators and the substance abuse composite with 3- and 5-year violent and general community recidivism in the aggregate sample and among gender and ethnoracial subgroups. Several themes were apparent. First, scores on the residualized substance abuse composite predicted violent and general recidivism, irrespective of follow-up, across gender and ethnoracial subgroups. Medium effects (AUCs = .64 to .70) were most frequently observed in the aggregate sample and male and non-Indigenous youth subgroups, small and medium effects (for violent and general recidivism, respectively) were observed with female youth, and small effects were observed for Indigenous youth. Second, among the clinical predictors, DSM substance abuse diagnoses were a weak and nonsignificant predictor of all recidivism outcomes across groups and in the sample as a whole. APS-SF clinical substance abuse concerns and intake rating severity fared better, however, with broadly medium effects for both outcomes in the aggregate sample, although predictive associations varied by gender and ethnoracial subgroup. The male group demonstrated effects that broadly mirrored the findings from the aggregate sample; however, for the remaining groups, the clinical intake severity rating most consistently predicted violent and general recidivism, while APS-SF scores predicted outcome only among Indigenous youth. Third, criminogenic substance abuse ratings varied in their relation to outcome; while VRS-YV ratings consistently demonstrated medium effects in the prediction of both sets of recidivism outcomes across groups, YLS/LSI-Sk need ratings demonstrated small significant effects in the aggregate sample and among male youth, but weak and nonsignificant effects in the remaining groups.
Predictive Validity of Substance Abuse (SA) Measures for Violent and General Recidivism as a Function of Gender and Indigenous Heritage
Note. PCL: YV = Psychopathy Checklist: Youth Version; SA = substance abuse; DSM = Diagnostic and Statistical Manual; APS-SF = Adolescent Psychopathology Scale-Short Form; YLS/LSI-Sk = Youth Level of Service/Case Management Inventory/Level of Service Inventory-Saskatchewan youth edition SA rating moderate or higher; VRS-YV = Violence Risk Scale-Youth Version SA dynamic factor (D12) rating; SA composite (res) = Substance abuse composite rating (residual score controlling for number of missing indicators).
p ≤ .001, **p ≤ .01, *p ≤ .05.
Incremental Predictive Validity of Substance Abuse Indicators With Recidivism
The final set of analyses examined the youth psychopathy and substance abuse nexus via Cox regression survival analyses in the aggregate sample and among gender and ethnoracial subgroups. Visual inspection of partial residuals from Cox regression for model predictors plotted against survival time substantively met the proportional hazards assumption, although follow-up examination of the slopes through regression demonstrated marginal non-proportionality for criminogenic and composite predictors; no adjustments to the models were made, however, given that minor departures from proportionality have a negligible impact on discrimination and calibration of Cox regression models (Austin & Giardiello, 2025).
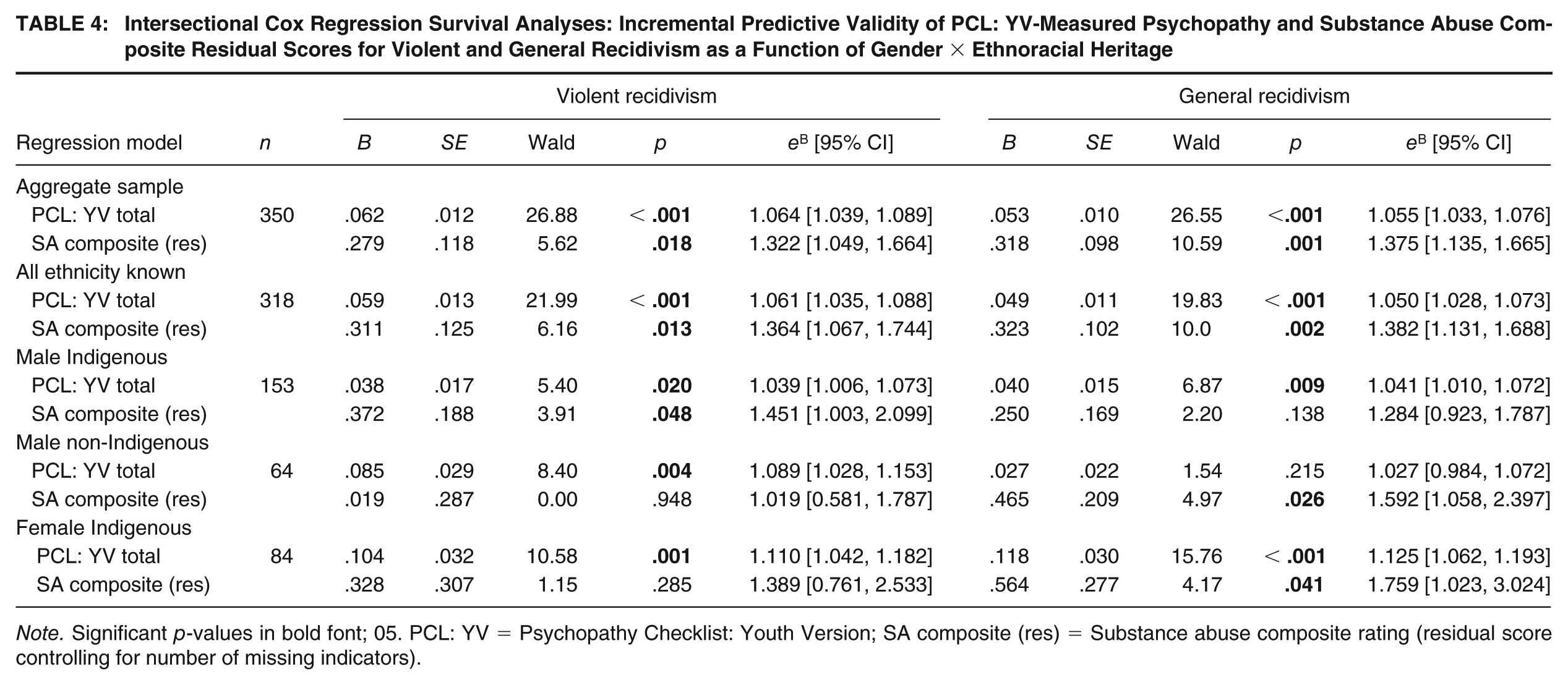
Table 4 presents a series of Cox regressions of the residualized substance abuse composite and PCL: YV scores conducted on the aggregate sample, including only those youth of known ethnoracial heritage, and intersectional gender x ethnoracial analyses. As expected, PCL: YV score incrementally predicted violent and general recidivism across all groups and subgroups. The substance abuse composite incrementally predicted increased violent and general recidivism, controlling for PCL: YV score in the aggregate sample and for those youth for whom ethnoracial heritage was known; hazard ratios improved slightly when youth of unknown heritage were excluded from analyses. The resulting hazard ratio represented more than a 30% increase in the hazard of future violence (eB = 1.322) or general recidivism (eB = 1.375), per one unit in substance-related concerns, after accounting for missing indicators and controlling for baseline psychopathy. Intersectional analyses demonstrated that residualized substance abuse composite ratings incrementally predicted violent recidivism for Indigenous male youth, and general recidivism for Indigenous female youth, and non-Indigenous male youth.
Intersectional Cox Regression Survival Analyses: Incremental Predictive Validity of PCL: YV-Measured Psychopathy and Substance Abuse Composite Residual Scores for Violent and General Recidivism as a Function of Gender × Ethnoracial Heritage
Note. Significant p-values in bold font; 05. PCL: YV = Psychopathy Checklist: Youth Version; SA composite (res) = Substance abuse composite rating (residual score controlling for number of missing indicators).
Table 5 reports the results of incremental predictive validity findings for the six substance abuse indicators within each of the four broad gender and ethnoracial subgroups; intersectional analyses were not conducted owing to the variability in cell numbers across the various measures and only the substance abuse predictor hazard ratios (controlling for PCL: YV total score) are reported for parsimony. Overall effects by gender and ethnoracial group are represented by between-groups and within-groups meta-analysis. One primary theme is that the residualized substance abuse composite variable more consistently significantly predicted outcome than the within-groups incremental validity meta-analyses (WG IV MA) of the five indicators; the composite uniquely predicted both outcomes among all male youth and all Indigenous youth. Results of between-groups incremental validity meta-analyses (BG IV MA) demonstrated that the residualized substance abuse composite uniquely predicted general recidivism across gender and ethnoracial groups, and violent recidivism across the gender groups; hazard ratio magnitudes were not significantly different between either gender or ethnoracial subgroup.
Incremental Predictive Validity Effect Size Invariance Testing: Meta-Analysis of Cox Regression Hazard Ratios of Substance Abuse Model Predictors Controlling for PCL: YV Total Score Across Gender and Ethnoracial Groups
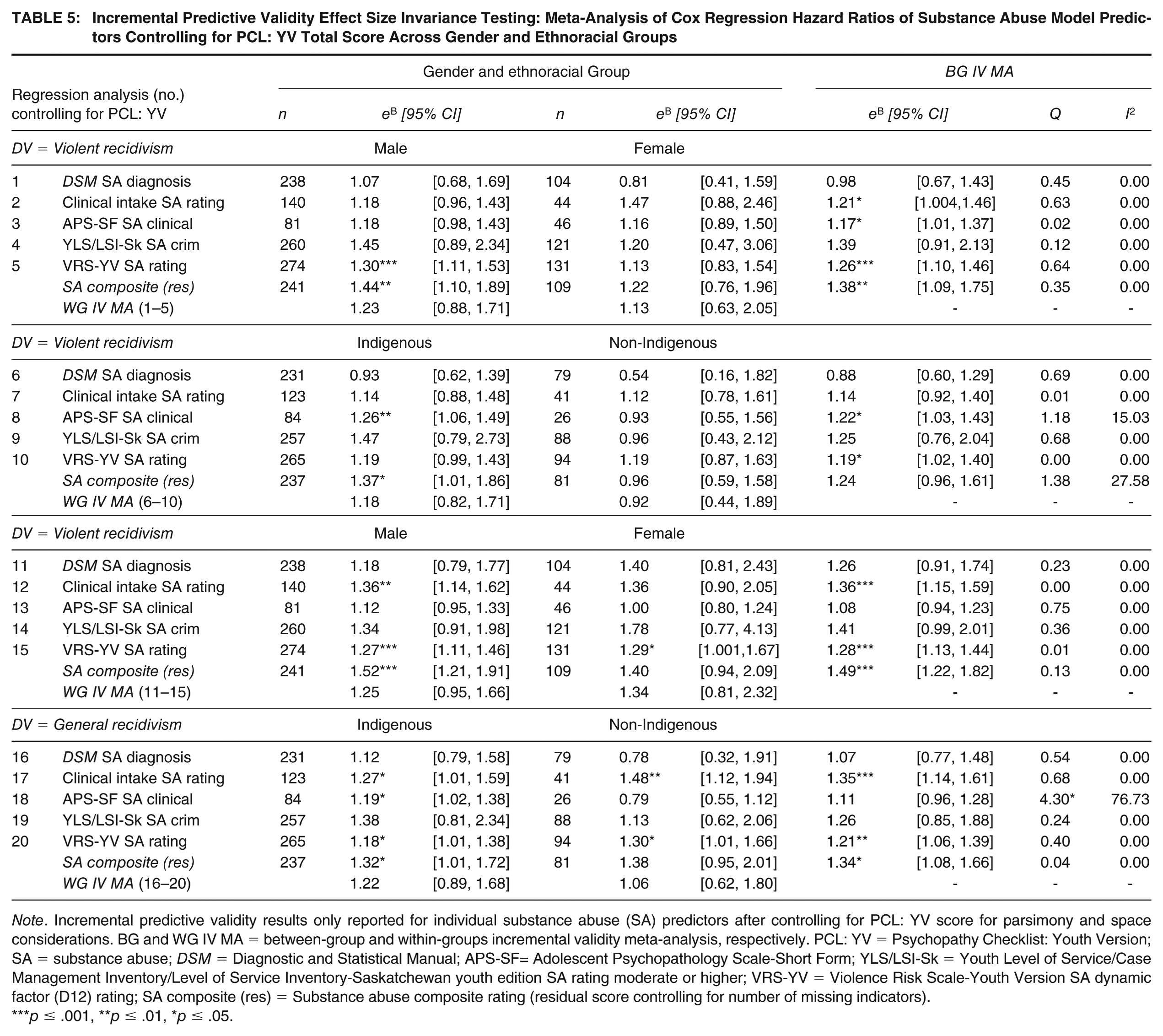
Note. Incremental predictive validity results only reported for individual substance abuse (SA) predictors after controlling for PCL: YV score for parsimony and space considerations. BG and WG IV MA = between-group and within-groups incremental validity meta-analysis, respectively. PCL: YV = Psychopathy Checklist: Youth Version; SA = substance abuse; DSM = Diagnostic and Statistical Manual; APS-SF= Adolescent Psychopathology Scale-Short Form; YLS/LSI-Sk = Youth Level of Service/Case Management Inventory/Level of Service Inventory-Saskatchewan youth edition SA rating moderate or higher; VRS-YV = Violence Risk Scale-Youth Version SA dynamic factor (D12) rating; SA composite (res) = Substance abuse composite rating (residual score controlling for number of missing indicators).
p ≤ .001, **p ≤ .01, *p ≤ .05.
A second core theme was that substance abuse ratings from the VRS-YV, but not the YLS/LSI-Sk, uniquely predicted general recidivism across all subgroups, and violent recidivism among male youth; however, all between-subjects meta-analyses yielded significant incremental effects across groups. Third, among the clinical indicators, the intake severity rating uniquely predicted general, but not violent, recidivism within all but the female subgroup (although they had the same hazard ratio magnitude as male youth). By contrast, the APS-SF substance abuse clinical concern rating incrementally predicted both outcomes, but only among Indigenous youth; this was also the only instance in which hazard ratios were significantly different (Q < .05 and I2 > 75%) between Indigenous and non-Indigenous youth (general recidivism).
Kaplan–Meier survival analyses were conducted to help unpack the results of Cox regressions by dichotomizing PCL: YV ratings into high and low groups using mean/median splits, at each level of the residualized substance abuse composite measure arranged into low, medium, and high levels of severity as outlined in the Sample Descriptives section of Results; log rank chi-square statistics for pairwise comparison of survival curves are reported in full beneath Figure 1, along with percent recidivism (PR) for each outcome within a given category. High psychopathy youth with the equivalence of having both clinical and criminogenic substance abuse indicators (High P, High SA) had significantly higher and faster rates of violent and general recidivism than lower psychopathy youth with similarly severe substance-related concerns (Low P, High SA). The psychopathy-substance abuse nexus appeared even stronger for general recidivism, in which case, high psychopathy youth with medium or high substance-related concerns had significantly steeper trajectories of recidivism than either high psychopathy youth with no substance-related concerns (High P, Low SA) or lower psychopathy youth with any level of substance-related concern. Finally, high psychopathy youth without substance-related concerns on any set of indicators did not have significantly different rates of failure than any of the low psychopathy groups, irrespective of substance-related concerns.
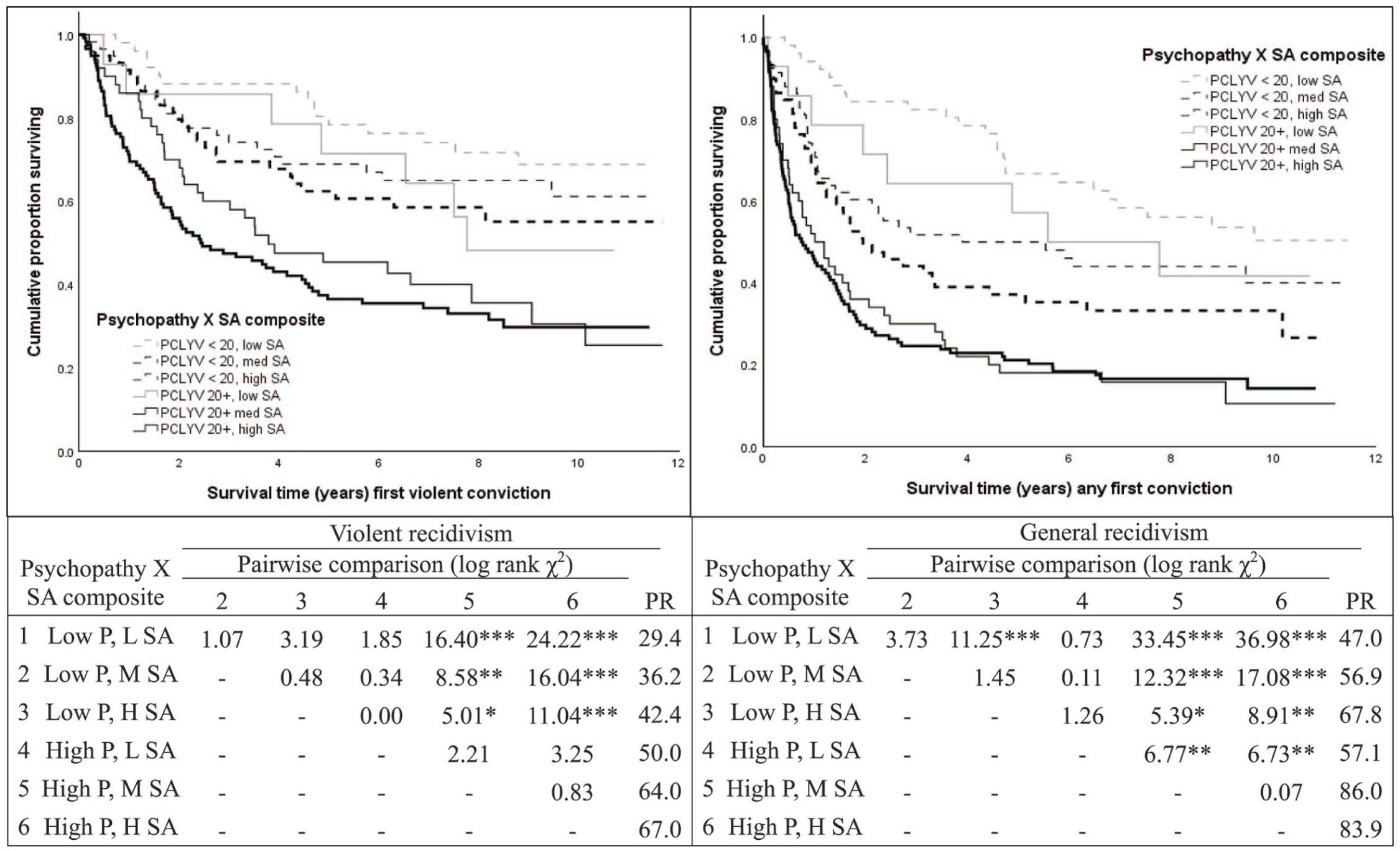
Kaplan-Meier Survival Analyses: Trajectories of Recidivism for Psychopathy-Substance Abuse Composite Groups
Discussion
The present study examined the intersection of juvenile psychopathy with the substance abuse construct in a diverse sample of more than 400 court-adjudicated youth, the majority of whom had violent conviction histories. Over 80% of youth had at least one criminogenic or clinical indicator of a substance-related concern, and approximately half the sample had such concerns across both domains, reflecting substance-related concerns that are both clinically significant and risk relevant; this was particularly evident for female and Indigenous youth, who scored higher on these key areas. The profiles of substance abuse indicators in tandem with a broad range of juvenile psychopathy traits have important empirical, conceptual, and service delivery implications regarding the intersection of these constructs.
Psychopathy-Substance Abuse Associations and Diversity Implications
PCL: YV scores showed moderate convergence with the substance abuse indicators, both clinical and criminogenic, with the strongest associations being shown with the lifestyle and antisocial features of psychopathy across gender and ethnoracial groups. The pattern of association indicates problematic substance use to reflect an impulsive, irresponsible, and chronically antisocial lifestyle, consistent with findings elsewhere in the youth (Hemphälä & Tengström, 2010) and adult literatures (Hemphill et al., 1994; Sellbom et al., 2017). Such traits may increase proneness for substance use (e.g., proneness to boredom/need for stimulation), reflect a lifestyle that promotes immersion in a drug and alcohol use subculture, and issues that may be exacerbated by substance use (e.g., anger problems, serious criminality). For instance, substance abuse may contribute to school absenteeism and conduct problems, serve as a motivator for criminal behavior (e.g., robbery to obtain money for drug use), or be a direct catalyst by way of loosening already weak inhibitions against crime and violence.
An interesting exception was stronger associations for male youth (compared with female youth) between affective facet scores and substance abuse indicators, a parallel that has also been observed with the PCL: YV and self-report measures of youth psychopathy across justice and community samples (Hemphälä & Tengström, 2010; Hillege et al., 2010). One possibility could be that female youth are more likely to use substance abuse to self-medicate trauma and related mental health concerns, representing a subset of youth for which callous and unemotional features are less prevalent or clinically relevant. A related possibility may be that the difference represents multiple gendered pathways into substance use for girls (Hudson et al., 2017).
The Psychopathy-Substance Abuse Nexus: Criminogenic Relevance and RNR Implications
A strength and novel feature of the present study was the inclusion of recidivism outcome to extend examination of the psychopathy-substance abuse nexus. We were surprised not to find any previous studies in this area examining links to recidivism. First, the criminogenic relevance of the substance abuse measures was apparent, although there was some variability in the predictive validity of the individual indicators for recidivism outcome. Of the clinical indicators, DSM diagnoses were quite broad, did not reflect severity necessarily, and tended to be poor predictors; however, the clinical intake ratings and APS-SF scores both reflect frequency, chronicity, and severity of substance abuse, and these tended to be better outcome predictors in the aggregate sample and across gender and ethnoracial groups. The criminogenic indicators, which reflect the extent to which substance abuse is linked to crime and violence as a dynamic need, had greater risk relevance, especially dimensional scores on VRS-YV dynamic item D12; the smaller effect sizes for the binary YLS/LSI-Sk substance abuse domain and non-significance in gender and ethnoracial subgroups likely represent attenuation owing to a loss of variance. The pattern of findings, multifaceted nature of substance abuse concerns, and variability in data completeness across measures underscored the development of a residualized substance use composite variable, which consistently predicted recidivism across gender and ethnoracial groups.
The direct examination of the psychopathy-substance abuse nexus through a series of incremental validity analyses, in our view, generated the most informative findings. Three primary themes were evident. First, controlling for PCL: YV total score, residualized substance abuse composite ratings incrementally predicted violent and general recidivism, whether the analyses were conducted on the sample in aggregate or limited to youth with known ethnoracial background; intersectional subgroup analyses demonstrated that the substance abuse composite incrementally predicted violent recidivism among Indigenous male youth, and general recidivism for Indigenous female youth and non-Indigenous male youth. These intersectional findings are critical, as they demonstrate no single ethnodemographic group to be driving the observed findings, and they illustrate the additive and incremental relevance of the substance abuse construct beyond psychopathy in potentiating general and violence-specific risk. An exception seemed to be lower direct relevance to violence for non-Indigenous male youth, who tended to have lower base rates of this outcome compared to Indigenous youth. Moreover, given that incremental validity findings remained unchanged and improved slightly when limited to youth of known ethnoracial heritage, this may suggest that youth of unknown heritage were likely to be non-Indigenous (White majority) ancestry; perhaps when diversity is not meaningfully viewed as a factor in clinical service delivery, service providers are less inclined to document it.
Second, owing to smaller cell sizes for subgroup analyses for some indicators, this created power constraints such that some associations were not significant despite having the same effect size magnitude, potentially serving as type II errors; that is, the absence of statistical significance does not equate to the absence of an effect, as reaffirmed through the use of fixed effects meta-analysis demonstrating invariance across gender and ethnoracial groups. Third, the results of the between-groups meta-analysis demonstrated that the VRS-YV substance abuse item, substance abuse composite ratings, and the clinical intake rating incrementally predicted both outcomes across gender groups. Moreover, across ethnoracial groups, VRS-YV substance abuse rating incrementally predicted both outcomes, intake severity ratings incrementally predicted violent recidivism, and APS-SF clinical substance abuse ratings and the composite uniquely predicted general recidivism; however, the meta-analytic effect was significant for these two clinical indicators owing to their associations with outcomes for Indigenous youth.
Extending the convergent validity findings, the results would suggest the presence of both higher levels of psychopathy and substance abuse concerns, which elevate risk for future crime and violence. Stronger links to general recidivism across gender, particularly for Indigenous female youth, could represent the broader range of antisocial behavior concerns that a psychopathy-substance abuse tandem could contribute to, including property offenses (e.g., break and enter, theft), drug-related crimes, technical violations (e.g., abstention, curfews), or gendered classes of criminal behavior (e.g., prostitution), all of which could be motivators for and a direct product of substance use concerns. With respect to violence, substance abuse combined with psychopathic features may further elevate risk for substance-fueled crimes involving heated emotion or reduced inhibition (e.g., assault, homicide) or instrumentally motivated ones (e.g., robbery).
The use of five substance abuse indicators was intended to illustrate the risk relevance of clinical and criminogenic operationalizations of this construct among high psychopathy youth, particularly when the two are integrated; we would not necessarily expect any clinician to assess five different ways that a youth may have a substance abuse problem in their evaluations. We believe it may be prudent, however, to include an assessment of some reliable form of clinical and criminogenic indicator of a substance-related concern in tandem with administering the PCL: YV. Taken together, this can have useful service delivery implications. For instance, violence reduction treatment might include tailored interventions for youth with high psychopathy and substance use. Per the risk principle, high psychopathy youth with elevated substance use concerns are at a higher risk and merit a greater intensity and range of risk-reducing interventions. Per the need principle, substance abuse is criminogenic and predictive of future crime and violence across genders, ethnoracial groups, and different levels of psychopathy; thus, it is a domain that merits direct intervention. And per the responsivity principle, the very nature of both sets of clinical concerns places youth at risk for not engaging the very services they need most, particularly given the association of psychopathy with program attrition (Olver et al., 2011), including youth populations struggling with substance use (O’Neill et al., 2003b).
The results would suggest going beyond isolated drug and alcohol abuse counseling to a forensic substance management approach that treats substance-related concerns within a criminogenic context (i.e., links to crime and violence). The end goal of programming would not only be in reducing and managing use, but decreasing further antisocial behavior. Such interventions would be multimodal, addressing related areas of risk and need (e.g., school and leisure, attitudes, peer networks) and demonstrate responsiveness to gender (Gobeil et al., 2016), ethnoracial heritage (Gutierrez et al., 2018), and personality (Newton et al., 2022) to maximize treatment buy-in and gains, and to minimize attrition.
Strengths, Limitations, and Conclusions
The present study has several strengths and limitations with implications for future research and practice. First, some notable strengths of the present study are that it featured multimethod, multimodal data (i.e., clinician ratings, self-report), including multiple measures of substance use in particular. The creation of a simple substance abuse composite variable provided a means of integrating clinical and criminogenic concerns in this domain, and the generation of a residualized score controlling for missing indicators provided a means of correcting for missing data to provide a more reliable and valid representation of the totality of substance-related concerns. Second, the study contributes to a limited body of youth psychopathy and substance use research, and one that lacked data on diverse groups (female and Indigenous youth). The use of a diverse combined sample provided opportunity to examine the psychopathy and substance abuse link in female and Indigenous youth, both of whom are understudied in this literature. Third, the inclusion of comprehensive recidivism data enabled examining critical links to outcomes that have been notably absent from the extant literature: the psychopathy-substance abuse-recidivism link, with RNR implications to inform intervention planning (e.g., forensic substance use management) to manage risk and to decrease future crime and violence.
There were several limitations that limited the generalizability of conclusions that can be drawn from the present findings, with implications for future research. First, the retrospective archival nature of this study permitted only limited exploration of diversity and additional data, including an expanded sample size, would benefit further exploration of diversity, culture, and more exhaustive efforts at intersectionality. The exclusive use of file information also places constraints on the comprehensiveness and availability of quality information needed to rate clinical measures, such as the PCL: YV. The use of interviews and real-time follow-up can yield more comprehensive information for rating measures as well as add field validity to bolster conclusions. Moreover, future investigations could be strengthened by including information pertaining to youth identification with their ethnocultural heritage. For instance, “Indigenous” is an umbrella term conventionally referring to persons that are First Nations, Métis, or Inuit, each of which is a highly culturally, linguistically, and geographically diverse group within its own right; in Saskatchewan alone, there are 70 First Nations comprising 5 linguistic groups and the Métis peoples with separate languages (e.g., Michif; Indigenous Services Canada, 2021).
Second, there was a lack of consistent data on types of substances used and as such, this could not be examined. There is some evidence to suggest that the type of substance use during adolescence matters. For instance, the abuse of cocaine and opiates have been shown to be associated with greater adverse outcomes across youth and adult samples (Welty et al., 2025), and patterns of substance use have been found to change over historical time periods (e.g., among emerging adults, alcohol use has been decreasing while marijuana and hallucinogen use has been increasing; National Institute of Drug Abuse, 2022). Of note, many of the youth in this sample reported polysubstance use. Third, greater linkages of these data to appropriate treatment (substance use interventions) would help to inform assessment and intervention practices, as would the incorporation of a measure of protective factors (e.g., supportive relationships with prosocial adults, positive attitudes toward education, effective coping skills).
Finally, the only outcomes examined were legal in nature (i.e., criminal recidivism). The inclusion of clinical outcomes related to substance use (e.g., sobriety, relapse) along with treatment progress indicators (e.g., attendance, nonadherence) related to involvement in risk-reduction services (e.g., forensic substance management, violence reduction services) would enhance our understanding of the RNR implications for youth with high psychopathy and problematic substance use. Given the recidivism rates associated with this broadly high-risk-need subgroup, future research should prioritize youth presenting with these characteristics and also seek to better understand their pathways to offending (e.g., gendered pathways associated with substance use and interpersonal aggression). The collection of additional youth self-report data related to victimization and trauma is also recommended given these experiences may contribute to substance use and other mental health concerns, including juvenile psychopathy, in different ways (e.g., use of substances to cope with anger in boys, use of substances to cope with anger and anxiety in girls, development of callous/unemotional traits; Hudson et al., 2017).
Footnotes
Authors’ Note:
The views, opinions, and assumptions expressed in this paper are those of the authors and do not necessarily reflect the views or official positions of the Saskatchewan Health Authority, Correctional Service of Canada, or the University of Saskatchewan. The authors thank the Saskatchewan Health Authority; Saskatchewan Ministry of Justice: Corrections and Policing; and the Saskatchewan Law Courts for their support of this research. As the present study features the use of protected or copyrighted materials to collect highly sensitive data on a vulnerable population, the data, as well as most study measures, are not publicly available. This study was not preregistered.