
Abstract
Military veterans and their families face a multiplicity of challenges once they transition from service. Even though more American private and public-sector organizations are engaged in studying the needs of veterans and their families through need assessments, few assessments are comprehensive analyses of the challenges they face. This systematic review of 61 need assessments from 2007-2018 in the United States summarizes findings on 18 veterans issues. While most studies addressed issues relating to accessing U.S. Department of Veterans Affairs health and benefit services, mental health, employment, and homelessness, gaps in the literature emerged, particularly regarding ethnic and sexual minority, rural and elderly veterans, and National Guard/Reserve servicemembers. Large cities and states with varying degrees of military presence were frequent regions of study, with national think tanks, nonprofit organizations, and public universities conducting most need assessments. Future assessments should address persistent inequities in coverage among communities and topics of study using mixed-method research and survey design.
Keywords
Military veterans and their families in the United States are facing myriad challenges upon transition from service, from employment to family support and mental health. Current efforts by federal agencies reach thousands of veterans annually with their programs, in addition to state veterans’ affairs agencies and local collaborative support and service delivery. Using theoretical frameworks for organizing and conducting mixed-method need assessments codified by Stufflebeam, McCormick, Brinkerhoff, and Nelson (1985) and Sleezer, Russ-Eft, and Gupta (2014), think tanks, universities, state and local governments, and nonprofit organizations across the United States have conducted need assessment studies for the purposes of understanding gaps in service delivery and unmet needs of community members and recommending action-oriented steps to address these gaps in delivery. However, there has been no holistic assessment of these needs of veterans and their families, which distill common themes and gaps in need within the literature to inform future scholarship and practice. Our systematic review synthesizes consistently studied veterans’ issues, reveals gaps within the literature, and recommends key best practices for future needs assessments. Our study is organized as follows. We first provide an overview of the existing literature of veterans’ needs assessments to determine the landscape of locations studied, sponsoring organizations, and issues discussed. We then discuss our methods for a systematic review of the literature using guidelines from the PRISMA system. In the third section, we report our findings from the qualitative analysis of commonly studied issues and gaps within the literature. Finally, we provide recommendations on best practices for future need assessments, including those pertaining to veterans.
Method
We used a systematic review process to provide a comprehensive overview and analysis of the current scholarship in the field of veterans studies because of its explicit, rigorous, and transparent methods (Cooper, Hedges, & Valentine, 2009; Lipsey & Wilson, 2001; Tranfield, Denver & Smart, 2003). To our knowledge, only one other literature review has examined veterans’ need assessments (Perkins, Aronson, & Olson, 2017). While valuable, this work covers less than half the number of studies covered herein, and it neither presents nor appears to have been conducted using formal systematic literature review methods. As a result, the veterans and military family health literature lacks a structured and comprehensive accounting of research on the needs of veterans and their families throughout the United States. We outline below the criteria and steps taken to collect current scholarship within the literature.
Eligibility Criteria
Studies that analyzed the needs and issues facing veterans and their families using qualitative and quantitative data were included in our study. Based off of established definitions of need (Sleezer, Russ-Eft, & Gupta, 2014), we defined needs assessments as having three components: (a) discussion of need, (b) aimed at solving or improving a current problem, provide learning and development, and take advantage of future opportunities, and (c) rely on data collection and analysis to “identify and understand gaps in learning and performance to determine future action.” Restrictions imposed on the search included publication date (March 2007 to January 2018) and publication status. Eligible studies were published by academic think tanks and institutes; universities in the United States written by faculty members and published by a university-affiliated organization; government agencies and departments at the state, county, and local level; nonprofit organizations in the United States, including foundations; and peer-reviewed academic journals.
Information Sources and Search Terms
Studies were identified by searching electronic databases and search engines, scanning reference lists of articles and consultation with experts in the field of veteran and military family policy and scholarship. We restricted our search to English-language reports and journal articles within the United States which addressed “need assessment.” We applied these criteria to the following scholarly and U.S. Federal Government databases: ISI Web of Science, ProQuest Periodical Online, ProQuest Government Periodical Index, Scopus, JSTOR, Google, and from the U.S. Departments of Defense, Labor, Veterans Affairs (VA), and the Small Business Administration. Within these sources, we used combinations of “veteran,” “military,” “servicemember,” “need,” and “assessment.” 1 We used the search term “military” to target our searches for uniformed military veterans. We used “need” and “assessment” to reflect the specific literature in which we are studying in this systematic review.
Study Selection
Eligibility assessment for inclusion into the review was performed by evaluating the relevance of each study’s title, abstract, and key words to the search criteria. We used the system for selection according to guidelines of the PRISMA Statement (Liberati et al., 2009), which is shown in Figure 1. To separate needs assessments of veterans and their families from current scholarship on veterans issues in academic journals, we determined that studies which did not conform to the eligibility criteria of “need” and “needs assessment” would not be eligible for inclusion. From our survey of the existing literature, we identified 61 reports to be included in our analysis.

PRISMA Framework and Study Selection Procedure.
Topic Identification
To code the literature of need assessments, we employed three different strategies to determine the topics assessed in our review. We first conducted a comprehensive scan of the academic and policy literature on veterans’ issues. This resulted in a distillation of nine most frequent topics: military-to-civilian transition, access to U.S. Department of VA and Veterans Health Administration (VHA) care and services, employment, service provider coordination, women veterans, education, families, and mental health. Since the literature reviewed did not include every area of need for veterans and their families, our second strategy involved consulting with military community–focused service-delivery networks across the United States and state Departments of VA and to identify other key topics not covered in the initial literature scan (Armstrong et al., in press; Armstrong, Van Slyke, Isbester, & Chapman, 2016). This step resulted in the inclusion of five additional topics: homelessness, poverty, legal support, financial support, and behavioral health. Finally, we created a feedback loop in our coding process, whereby we could assess new topics for each study in our sample. Through this feedback loop, we identified four more topics: rural veterans, elderly veterans, National Guard and Reserve service members, and minority veterans. In total, these steps generated 18 topics that we applied to code the need assessments in our sample. To ensure the validity of these topics, peer reviewers from the community engagement and academic scholarship disciplines provided critical feedback, which we used to strengthen the categorization of our topics.
Coding Process
We used the 18 topics to qualitatively code the need assessments in the sample. The coding process, including corresponding topic identification, was predetermined by a team of researchers to ensure the validity and consistency of coding rules and practice. The team of researchers also developed a coding data extraction form following Brown, Upchurch, and Acton (2003) and Brown et al. (2013), to define methodological and substantive features (e.g., sponsoring organization, geographic focus, publication year), quality metrics of the study (e.g., number of topics addressed, methods employed, and detail for each topic), and focus areas (i.e., 18 defined topics).
Validity and Reliability
To ensure the validity of the systematic review and the coding process, two reviewers independently implemented the selection and coding criteria using the PRISMA Statement, predefined requirements for study selection, and the coding data extraction form. Discrepancies between process and results among the two reviewers were discussed and settled with input from research team leads.
Results
The study collected 61 articles that met our inclusion criteria (for a complete list of included articles, see Appendix A). Most publications were published between 2012 and 2015 (n = 40); however, fewer reports have been published since 2016 (n = 12). The needs of veterans and their families related to accessing the VHA (n = 47), mental health (n = 40), the U.S. Department of VA’s services (n = 37), and employment (n = 34) were the most frequently studied topic areas in the literature, with over half of the studies included addressing these topics. Less than half of the studies included addressed the remaining 12 topic areas including on transition (n = 30), housing and homelessness (n = 29), and women veterans (n = 27). Six topic areas were addressed in fewer than 10 studies, from rural (n = 9) and minority (n = 7) veterans to behavioral health (n = 4).
Within the needs assessments literature, scholars and policy makers studied predominantly metropolitan areas and states with large veteran populations (see Figure 2). Twenty-one large U.S. cities and metropolitan areas were frequent study environments for the challenges facing veterans (n = 21), with multiple studies being conducted in cities like Seattle, Los Angeles, and Boston. The studies included showed wide geographic breadth, with the majority of the states in the United States having at least one study done on its respective veteran population (n = 32). Many states had multiple reports conducted on its veteran population, particularly California and Michigan (n = 7 each), Texas (n = 5), and Massachusetts and Washington (n = 4 each). While states and large metro areas were the main focus of many reports, counties (n = 13) and smaller cities’ (n = 3) veteran populations were also studied in the included literature.
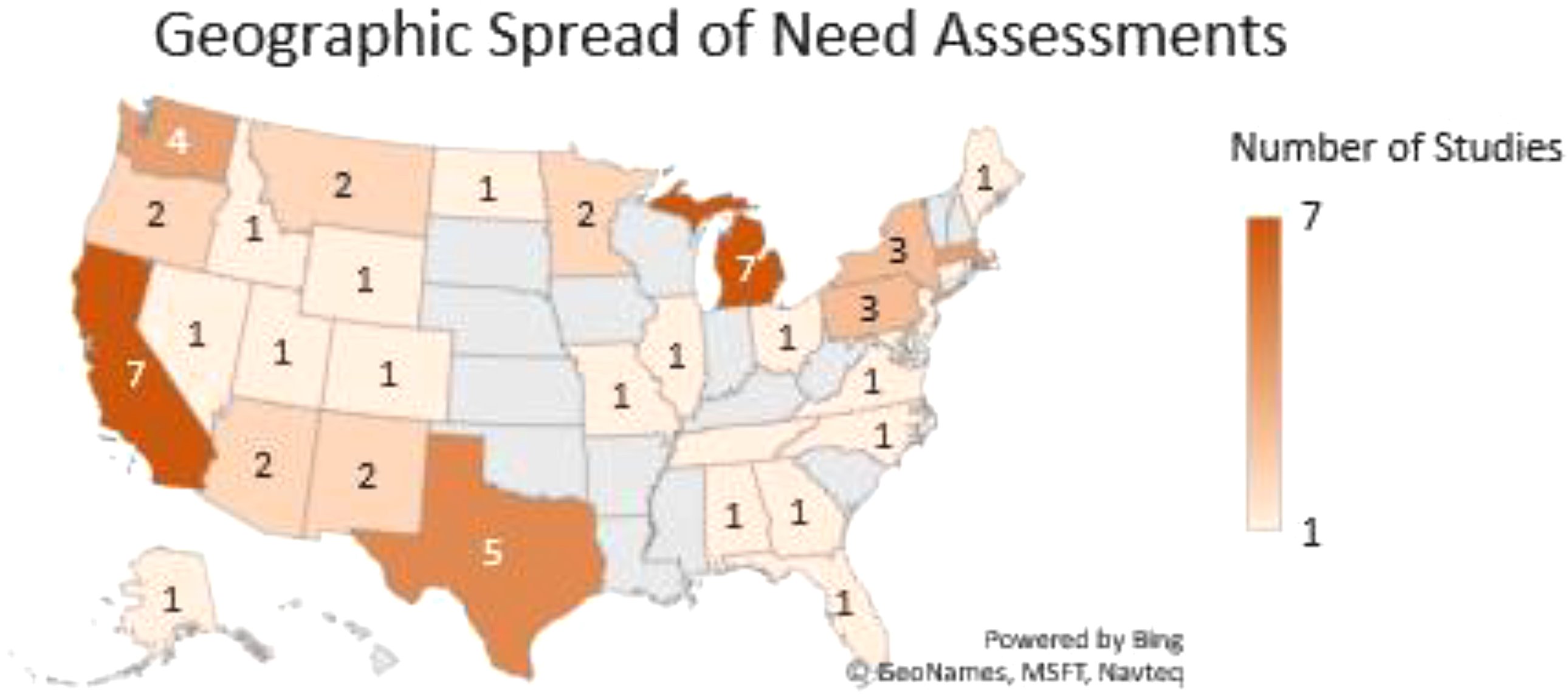
Geographic Distribution of Published Veterans' Need Assessments.
The needs assessment literature on veterans and their families is driven by five main categories of actors. Most needs assessments have been conducted by national nonprofit think tanks and organizations (n = 22), with two organizations publishing more than five studies each and seven organizations each publishing a need assessment. Universities published 14 needs assessments on veteran populations within their own states, with the majority of reports published by public universities (n = 10). State and local government agencies and local nonprofits (n = 7) commissioned and published multiple studies for their specific geographic and demographic areas. Finally, relatively few need assessments have been published in peer-reviewed academic journals (n = 7), with most those studies being published in 2012 and 2013 (n = 4).
Discussion
The following discussion identifies the key needs of veterans and their families across the 18 topic areas and the trends of change and continuity on these issues in national, state, and local geographic contexts. While many of the studies were focused on unique veteran and military family populations, and thus have their own inherent value for local study, much of the commentary provided by these local-level studies connected to larger national-level trends and needs of the broader U.S. veteran and military family populations. We present first the most commonly addressed topic areas in the literature and their component issues and conclude the Discussion section with the analysis of less frequently studied topic areas.
Frequently Studied Topic Areas
Access to U.S. Department of VA and VHA Resources
Veterans from all over the United States experienced and reported difficulties and barriers to accessing health benefits and resources from the U.S. Department of VA and the VHA. The most common barrier to access for veterans was transportation. Both in rural areas (southern Alabama, Rensselaer County, NY, and in parts of Michigan and Tennessee) to large metropolitan cities like Boston, Detroit, Dallas–Fort Worth, and Houston, many veterans expressed difficulty getting to VA Medical Centers for care. This was a particularly difficult barrier for homeless, older, and rural veterans.
These inabilities to access services also extended to the navigation of VA services; veterans in all locations noted a general lack of information and education on the VA and health resources available to them through the VHA. For example, many Pennsylvania veterans who filed claims by themselves had a general lack of confidence in navigating the VA system and subsequently believed they were “taking away from other veterans” by using VA benefits. Women veterans faced similar challenges with accessing VA resources, except that they experienced difficulty in learning and accessing gender-specific services within the VA (Disabled American Veterans, 2014). As a result, many veterans were inclined to use private and non-VA health care due to the perceived ease of use or stop looking for care within the VA (Castro, Kintzle, & Hassan, 2013; Institute of Medicine, 2013). Finally, veterans from around the country reported that dealing with the bureaucracy and paperwork required to apply for and submit benefits claims were major burdens to their lives. Needs assessments across the country noted that military benefits generally had a lag and backlogs of pension and benefits claims were often incredibly lengthy. For example, San Mateo County, CA, veterans experienced wait times of 320 days for rating claims and 486 days for nonrating claims in 2014 (Stevens & Brutschy, 2014). Even the Montana State Bar noted that veterans faced legal and VA barriers to accessing their service-related disabilities benefits (Blaskovich, Reed, Redden, & Doggett, 2012).
Veterans reported several other issues with accessing VA services and benefits, ranging from cultural incompetency within the VA to mixed quality of VHA care. Older veterans were most likely to feel alienated and disrespected through their interactions with the VA due to their perspective of “cultural incompetency,” where VA employees—many of them civilians—did not seem to understand military culture, exhibit proficiency in working with military and veteran populations (e.g., loud noises sometimes scared patients into trauma), or know how to appropriately communicate with veteran patients (Tanielian et al., 2014; Wilder Research, 2015). 2 Due to this perceived cultural incompetence by patients, many Virginia veterans, for example, noted that they did not see the benefit of pursuing mental and behavioral services offered through the VA system (Dunkenberger et al., 2010). 3 In multiple studies, inadequate care was provided to veterans of all ages on issues ranging from mental health and substance abuse (Institute of Medicine, 2013), post-traumatic stress disorder (PTSD) and depression (National Council for Behavioral Health, 2012), and women’s health (Morris, 2012; Northeast Florida Women Veterans, 2015). For example, a 2014 study noted that a third of all VA Medical Centers do not have a gynecologist on staff for women veterans, even as demand continues to increase for gender-specific preventative screening, breast care, and prenatal and obstetrical care (Disabled American Veterans, 2014). Student veterans in the Nevada higher education system noted that of the three quarters who received medical care for a military-connected injury, a third of those students rated VHA care as inadequate (Elliott, Gonzalez, & Larsen, 2012).
Behavioral and Mental Health Needs
While the mental health needs of veterans were a commonly addressed theme in most of the studies, two common topics emerged: stigmas within the U.S. military against mental health disorders and high proportions of veterans with mental health issues. In the Washington Post’s 2014 survey of veterans across the United States, almost a third of respondents noted that the state of their emotional and mental health was worse off post-service than it was pre-service (The Washington Post & Kaiser Family Foundation, 2014). Veterans across the United States feel stigmatized and discouraged from seeking help for their mental health issues because of military culture, which considered them “weak” and posed risks to their promotions and military careers (Institute of Medicine, 2013). Thus, these studies noted a low willingness of veterans to report their illnesses to the VA; for example, a 2011 study in New York state found that 20% of New York state veterans who needed mental health services did not seek them out or obtain them (Schell & Tanielian, 2011).
Even within a very diverse veteran population in experience and health conditions, many studies in the literature reported high proportions of veterans studied with mental health issues. The National Council for Behavioral Health (2012) noted that in 10 states, 25,000–65,000 veterans had any type of mental health disorder, with 6 having over 15,000 veterans with PTSD or major depression and 5 having over 10,000 veterans whose needs were underserved. These trends of mental illness are also found at the city and local levels, where over 30% of the veteran populations in cities like Chicago, Los Angeles, Pittsburgh, and San Diego have a mental illness (Carter & Kidder, 2013, 2015; Castro et al., 2013; Kintzle, Rasheed, & Castro, 2016). The risk for veterans with mental illnesses is not reaching out or getting help; in studies of Connecticut, Massachusetts, Michigan, Minnesota, and Tennessee veterans, veterans with mental illnesses reported that they faced barriers to accessing VA resources from the lack of information available about the VA’s mental health services (Altarum Institute, 2014a; Dynia, 2009; Farmer et al., 2017; Hardy, 2013; Wilder Research, 2015).
While veterans’ mental health was a common topic throughout the literature, few studies analyzed mental health among minority groups, particularly racial/ethnic, gender, and sexual minorities. The Institute of Medicine (2013) study found that Operation Iraqi Freedom/Operation Enduring Freedom (OIF/OEF) women veterans had higher needs for mental health care than in previous conflicts, and subsequent assessments found women veterans are more likely to have a combination of mental and physical health disorders than men, particularly among those who served in OEF/OIF engagements. Need assessments in both South Texas and Northeast Florida noted mental health services were critical health needs for women veterans; in the Northeast Florida study, almost half of the women veteran respondents reported suffering from either depression or anxiety, with almost a third reporting suffering from PTSD (Kotarba, Wivagg, Pierson, Martinez, & Kappler, 2016; Northeast Florida Women Veterans, 2015; Wivagg, Martinez-Ramos, & Pierson, 2016). However, while women veterans faced unique mental and behavioral health issues, the VA had only three women’s stress disorder teams for the entire country, supporting additional reporting on limited access for women veterans to PTSD treatments in military treatment facilities in 2014 (Disabled American Veterans, 2014). In addition to women veterans having specific mental health-care needs, the Institute of Medicine noted that African American veterans were less likely to receive mental health services for PTSD than non-Latino Whites (Institute of Medicine, 2013). The Nevada Higher Education System’s study of Nevada student veterans found that almost one fifth of student veterans met criteria for PTSD, with common symptoms including super attentiveness, trouble falling asleep, and difficulty concentrating in class (Elliott et al., 2012). While traditional minority populations were studied in the needs assessments, no study included in the sample addressed the specific needs or situations of sexual minorities, which includes LGBTQ service members and veterans.
Employment and Broader Workforce Needs
The needs assessment literature supported the findings from the abundance of scholarship conducted on veteran employment and self-employment (e.g., Boldon, Maury, Armstrong, & Van Slyke, 2016; Humensky, Jordan, Stroupe, & Hynes, 2013; Keeling, Ozuna, Kintzle, & Castro, 2018; Perkins et al., 2019; Schulker, 2017). A large majority of the literature reported veteran needs for employment, particularly the pre-interview stages. While some movements have aimed to improve the employment experiences of veterans, many veterans still reported that employers held stigmas against them, from misconceptions of mental health to misunderstandings of their skills (Guettabi & Frazier, 2015; Kintzle et al., 2016; Prudential Financial, 2012). This misunderstanding of skills could have come from the challenge that many veterans face translating their skills into civilian lexicon, particularly regarding resumes and cover letters. Job fairs were often difficult for veterans to derive benefit from due to these translation issues with civilian recruiters. The difficulty in accessing VA resources also extended to employment, where veterans in virtually all the studies reported an unawareness of available VA employment, rehabilitation, and training services and benefits (Albright, Hammer, & Currier, 2017; Pryor & DiNisco, 2008; Pryor & Pryor, 2010). These barriers to employment have been seen to lead to long-term unemployment among veterans, which often makes it more difficult for them to reenter the civilian sector without changing their primary functional area (Georgia Center for Nonprofits, 2012; McCarthy, 2014; Morris, 2012).
Women Veterans and Sexual Health
Fewer studies within the needs assessment literature addressed the common challenges women veterans face (n = 27); however, studies that did address women veterans’ issues described difficulties accessing VHA services, specific military sexual trauma (MST) resources, and disparities in income and employment. Female separation from the military and reintegration into civilian life is often more difficult than men’s experiences due to physical and sexual health needs, the demands and stresses of family life, and their own transitional periods. Both national and local needs assessments found that in some cases, women veterans do not have access to the same kinds of resources men have when they transition, from lacking safe spaces and inclusion into veteran service organizations and veteran support groups to being less likely to receive disability compensation for PTSD and TBI than male veterans—even though a higher proportion of women veterans receive total VA disability benefits than men (Disabled American Veterans, 2014; Morris, 2012). In a similar way, women veterans across the country noted frequent difficulties accessing health resources through the VHA due to a lack of awareness of available resources and challenges accessing health-care specialists (Douds et al., 2014; Haynes & Tavares, 2010; Kidder, Schafer, & Carter, 2016). The National Housing Conference paralleled these findings, noting that women veterans are more likely than men to live in poverty, and young female veterans, particularly African Americans, are at the greatest risk for homelessness among veterans (Sturtevant, Brennan, Viverios, & Handelman, 2015).
With rising rates of sexual harassment and sexual assault against post–9/11 women veterans across the United States, MST and its impacts are becoming even more important to the mental and physical well-being of women veterans (Castro & Kintzle, 2017; Kintzle et al., 2016; Wivagg et al., 2016). This increase could be partially due to growing confidence in the Department of Defense (DOD) among women service members to respond to these issues effectively. The Institute of Medicine (2013) notes that MST and the long-term impacts of potential marital problems can lead to a host of mental, physical, and sexual health problems in the future, including higher burden of medical illness, and increased risk for experiencing PTSD. Long-term effects of inequities between male and female veterans can also be seen in the disparities of income and employment. Studies from both Charlotte and San Mateo County, CA, show that women veterans earned less per year than male veterans and were more likely to have higher unemployment rates (Morris, 2012; Stevens & Brutschy, 2014). Women veterans in Houston perhaps summed the issues they face up the best: Women veterans have a very difficult time making their concerns and needs known to policy makers and community providers (Harris County TX Veteran Services Office, 2017).
Coordination
To the extent that the needs assessment literature examines the coordination of service delivery, most studies across the country noted low levels of communication and referral between veterans organizations. Due to limited budgets and available resources, many of these veterans organizations were not able to provide outreach and coordination resources for veterans and experienced difficulties integrating services either bilaterally or through a collaborative (Altarum Institute, 2015a, 2015d; Georgia Center for Nonprofits, 2012). Integration of services through a community collaborative was most frequent in cities with large veteran populations (i.e., Seattle, Los Angeles, and Charlotte). However, this was not true across the country; for example, even though Atlanta has a large veteran population, the region has been unable to create a collaborative to integrate these services. However, these are the exceptions to the trend of limited communication and integration of services found in the needs assessment literature, like urban areas of Boston, Pittsburgh, and Rochester, NY (Carter & Kidder, 2015; Ellison et al., 2012; Pryor & DiNisco, 2008).
Military-to-Civilian Transition
Consistent with academic scholarship on military-to-civilian transition and reintegration, 4 the needs assessments in our sample affirm that recently transitioned veterans often feel socially and culturally isolated in their new communities. Hardy (2013) notes that veterans across the country experience a loss of identity upon separation from military culture, which makes it difficult for many to find a sense of purpose for their post-service life. Many veterans transition into communities that do not understand them, their experiences, or their challenges. Compounded with work and employment barriers, changes in civilian lifestyle, and difficulties accessing military and government assistance, veterans may feel isolated and struggle to adjust to a new way of life (The Washington Post & Kaiser Family Foundation, 2014). Need assessments of veterans in Alabama, New York, and Virginia found that difficulties with transition can also lead to worsening mental health statuses and heighten the risk of substance abuse, driving their needs for private and VA health care (Albright et al., 2017; Dunkenberger et al., 2010; Schell & Tanielian, 2011). However, transitioning veterans in multiple states, particularly those with large veteran populations like Michigan, Pennsylvania, Texas, and Washington, still were uncertain with how to access VA, VHA, and community resources (Altarum Institute, 2015a; Douds et al., 2014; Kotarba et al., 2016; Lachman & Laing, 2008; United Way of King County, 2009). Finally, only a few studies looked at the transition experiences of minority groups including women and ethnic minorities. The Southern Alabama study found that minority veterans, predominately African American and Latino, were less likely to have a job upon separation than White veterans (Albright et al., 2017). It is clear that transition challenges affect all veterans but are commonly misunderstood by the civilian communities in which they live.
Homelessness
Homelessness is one of the hidden crises facing many veterans around the United States due to the confluence of increasing home prices, unemployment, mental illnesses, food insecurity, and a lack of housing assistance infrastructure in many major cities and urban areas. Across the country, veterans who faced homelessness were likely to be Caucasian males between 36 and 65 years old, lack health insurance, face substance abuse issues, and were commonly Army veterans from the Vietnam or Gulf War era (Georgia Center for Nonprofits, 2012; Knopf, 2013; Pryor & Pryor, 2010; Stevens & Brutschy, 2014). Of the sixty-one needs assessments collected, most communities saw an increase in homelessness rates for veterans, particularly in large cities like Chicago, Dallas–Fort Worth, Denver, San Francisco, and Seattle; notable cases of declining homeless rates were in Los Angeles, Orange County, CA, Phoenix, and San Antonio, along with the state of Massachusetts. The studies noted that many of these counties, municipalities, and cities, particularly in California, Connecticut, Georgia, and Michigan, often lack the infrastructure and resources needed to help homeless veterans.
Within the homeless veteran population, many veterans do not know about potential housing resources available to them until they are out on the street or in an emergency. Sturtevant, Brennan, Viverios, and Handelman (2015) noted that post–9/11 veterans could only afford to buy a median-priced home in 5 of the 50 largest metro areas in the United States; veterans in the San Francisco and Seattle areas faced particularly high costs of living (Carter & Kidder, 2013; Sturtevant et al., 2015; United Way of King County, 2009). One option available to veterans is the HUD-VASH program, administered by the U.S. Department of Housing and Urban Development, where veterans can receive housing vouchers to rent housing. In some communities where housing is becoming more expensive, like San Francisco and San Mateo County, CA, VA housing benefits, allowances, and HUD-VASH vouchers often do not cover the costs of housing rentals for veterans (Stevens & Brutschy, 2014).
A report by the Disabled Veterans of America (2014) noted that women veterans across the United States were 2 times more prone to homelessness than male veterans, with women veterans representing 8% of all homeless veterans in 2013; of these homeless women veterans, African American women are particularly at risk of homelessness. These veterans often faced transportation barriers to accessing services and sometimes faced issues relating to food insecurity, as was the case with homeless veterans in Chicago (Kintzle et al., 2016). It is clear that common health and mental issues veterans face might be risk factors to chronic homelessness among veterans.
Less Frequently Studied Topic Areas
Poverty Among Veterans
Out of the current literature on veterans’ needs, only a few (n = 7) discussed poverty among veterans. Multiple need assessments reported noted the general lack of social safety nets provided by state and local governments for citizens, particularly for veterans, which could be integral to addressing health issues such as depression, PTSD, alcohol and substance abuse, and relationships and divorce (Albright et al., 2017; Dunkenberger et al., 2010; Kidder et al., 2016). The need assessment from Southern Alabama noted that more than 46% of veterans who were in the enlisted ranks reported an annual income of less than US$24,000, which is under the federal poverty line for a family of four (Albright et al., 2017). Northeast Minnesota veterans were in a similar situation, with 12% of respondents reporting an annual income of less than US$20,000 (Wilder Research, 2015). Of particular concerns for the Southern Alabama veterans, especially for women and ethnic minority veterans, were food insecurity and food deserts (Albright et al., 2017). There are bound to be examples and situations like those that veterans in Alabama, Dallas–Fort Worth, Minnesota, and Virginia, thus requiring further scholarship on the issue of veteran poverty.
Veteran Subgroups: Ethnic Minorities and Rural Veterans
Surprisingly, the literature of veterans’ needs assessments underanalyzes these two populations, which experience some of the greatest challenges to accessing VA and VHA services and in gaining employment. Only nine needs assessments addressed specific needs of rural veterans, including barriers to accessing VA and VHA resources, transportation difficulties, and specific health needs. Since the unique needs of ethnic/minority veterans were only studied in seven need assessments, there were few common themes outside of minority veterans experiencing discrimination within the VA system. Even within other large themes of education, employment, women, and mental health, there were not specific discussions about how these themes affect minority veterans.
Legal Support
While legal support is a common service found in integrated veteran service networks and collaboratives around the country, one fourth of the needs assessment literature (n = 16) addressed the needs for legal support. Two statewide studies in Maine and Montana found that veterans often try to handle legal issues on their own, citing the high costs of hiring an attorney and low referral rates from social service providers to legal aid organizations (Blaskovich et al., 2012; Liscord & Elliott, 2013). The Maine study also found that veterans who lacked legal representation before courts were at a higher risk to become homeless than other veterans (Liscord & Elliott, 2013). Additional studies found that poor veterans in Texas and National Guard and Reserve service members in Massachusetts have a particularly great need for legal support (Farmer et al., 2017; Kotarba et al., 2016). These studies, in addition to the Altarum Michigan studies (2015a, 2015d), observed that common legal issues for veterans included criminal offenses, bankruptcy, housing, evictions, and substance abuse.
Financial Support
Many veterans across the United States face financial problems similar to civilians, from increasing debt limits on credit cards to having difficulties meeting rent, mortgage, and utility costs (The Washington Post & Kaiser Family Foundation, 2014). However, within the 15 assessments which addressed financial need, the most common need was for financial planning assistance. Upon transition from the military, many veterans do not have the tools necessary to be effective financial planners. Veterans in Massachusetts and Rensselaer County, NY discussed their difficulties finding and accessing credit counseling, financial guardianship, and financial planning resources; financial planning was also a challenge for veterans in Boston and throughout Michigan (Altarum Institute, 2015c; Ellison et al., 2012; Farmer et al., 2017; Pryor & Pryor, 2010). In addition to lacking financial planning skills, many veterans throughout the country expressed challenges with keeping up with monthly bills, from student veterans in Nevada with educational costs to credit card balances and debt; in some cases, these challenges can be exacerbated to large proportions, such as in Los Angeles, where one third of pre–9/11 and post–9/11 veterans were in financial trouble post-transition (Castro et al., 2013; Elliott et al., 2012). Only two reports addressed the financial needs of specific veteran subgroups: National Guard/Reserve veterans were reported to have the greatest financial difficulties among Massachusetts veterans, while financial needs were the second most common challenge facing women veterans in Jacksonville, FL (Farmer et al., 2017; Northeast Florida Women Veterans, 2015). While these are simply two case studies within the literature, they present a critical need in the scholarship to address the unique financial needs of veterans’ subgroups.
National Guard/Reserve
Due to a general lack of acknowledgment in the needs assessment literature (n = 6), the unique needs and challenges of National Guard and Armed Forces Reserves (NG/R) members are not well-documented or understood. For example, NG/R men and women are often left out of outreach efforts to veterans for any service, which shows often poor communication between NG/R service members, the VA, and community services and referral organizations. NG/R service members also face particular difficulties accessing VA resources and services, as reported in the Michigan studies (Altarum Institute, 2015c, 2015d). Finally, NG/R veterans experience many difficulties finding full-time employment because employers do not want to have to hire more people to cover for the NG/R service member when they are deployed or called into action (Farmer et al., 2017; Morris, 2012). To comprehensively study the American veteran, studies and scholarship need to include analysis of the NG/R experience.
Military Families
While academic literature in social work has been active in studying the experiences of military families, military spouses, and children (Bell, Reed, & Edwards, 2011; Blaisure, Saathoff-Wells, Pereira, MacDermid Wadsworth, & Dombro, 2012; Bradbard & Maury, 2014; Bradbard, Maury, & Armstrong, 2016; Dejoie Smith et al., 2011; Ebata, Pusateri, Knobloch, & McGlaughlin, 2015; Park, 2011; Segal & Clever, 2013), the same scholarly interest has not transferred to the needs assessment literature. Only 18 studies in the current needs assessment literature addressed the unique needs of military families. One of the most interesting observations from the literature was that the U.S. DOD and the VA do not consider the full spectrum of military families when delivering services, particularly with nontraditional families. The further contributes to the barriers military family members face in accessing VA services (Institute of Medicine, 2013). Common concerns and needs among families included childcare, legal assistance, counseling, and mental health. The unique needs of families, such as mental illnesses of military children, domestic violence risks, family services, childcare, and family-based interventions, are understudied in the needs assessment literature. This gap inhibits the VA and community organizations from providing these services in an effective and culturally sensitive manner.
Education
Similar to the subject of military families, veteran experiences with education are well-documented in the academic literature, with particular focus on attainment and assimilation in higher education and technical programs. However, the education needs of veterans in specific geographic areas were understudied in the needs assessment literature; only modest attention (n = 23) was given to these educational needs. Elliott, Gonzalez, and Larsen (2012) conducted the only statewide study of student veterans in higher education institutions through the University of Nevada system. The studies that did address education often cited the reoccurring theme that veterans across the country were generally unaware of, or unable to, access VA and GI Bill resources to help fund their education (Altarum Institute, 2015b; Castro, Kintzle, & Hassan, 2015; Disabled American Veterans, 2014; University of Arizona, 2012). Veterans in these studies often cited the burdensome and extensive paperwork for benefits claims as an inhibitor to their educational needs, in addition to general cultural isolation and discomfort from the civilian student population. However, these studies did find that OIF/OEF veterans have higher levels of education attainment than veterans from other wars. Women veterans had a higher completion rate of college education than male veterans and civilian women from 2000 to 2009 (Disabled American Veterans, 2014). Other studies, including those in Massachusetts, Minnesota, and Pennsylvania, found higher educational attainment among post–9/11 veterans as well (Douds et al., 2014; Farmer et al., 2017; Wilder Research, 2015). These studies also addressed the vocational programs of the VA and the U.S. Department of Labor but were often critical of their effectiveness since veterans noted that the programs were more about training than actually gaining employment or the skills required for employment.
Study Characteristics
Geographic coverage
The need assessment literature’s geographic coverage clearly points to inequities among states and communities in terms of study (see Figure 2). While this coverage was mentioned above, there are specific cities and regions of the country that receive more investigation than others. On the one hand, many of these assessments focused on cities with large veteran populations, including Charlotte, Dallas–Fort Worth, Los Angeles, Pittsburgh, and San Antonio. Organizations and local governments are most likely to study populations that require study, and in these cases, veterans are a large portion of the total population. However, as shown in Figure 2, over one third of the states within the United States did not have a study conducted on their veteran populations. Veterans within these states are likely to have different needs in accessing VA and VHA services, education, employment, homelessness, and legal services. Thus, another gap exists in the literature in understanding of veteran experiences in each state within the country.
Topical breadth and inclusivity
The assessments included in this review are varied in topical breadth and scope. Some studies were generally comprehensive, covering more than 10 of the 18 topic areas (Douds et al., 2014; Dunkenberger et al., 2010; Harris County TX Veterans Service Office, 2017; Hoskins, 2013). Others singularly focused on one specific topic affecting veteran health or well-being (McInnes et al., 2015; Rede Group, 2014; Tanielan et al., 2014). Most of these needs assessments address at least 4 or more of the 18 topics included in this systematic review (n = 51). However, as a body of literature, the need assessments underrepresent certain veteran subgroups within the population, particularly the needs and current conditions of minority (ethnic and gender), poor, and rural veterans, military children, and National Guard and Reserve service members. The lack of study on ethnic minority veterans is particularly surprising, given that they often have different postservice experiences and needs than White, male veterans. Likewise, the academic literature on the experiences and needs of military families, particularly military children, is robust, especially in the field of social work. Even though there is academic interest in the needs of these children, only nine studies in the need assessment literature addressed specific concerns of children, such as transition difficulties and need for age-appropriate mental health services. While it is important that some need assessments focused on and addressed homeless, rural, and poor veterans, given little academic scholarship on their needs, they were not studied in even a majority of the need assessments. Their unique needs, particularly the comorbidity of PTSD and substance abuse which can lead to homelessness and poverty, should be better documented if scholars and practitioners are to understand how to effectively deliver services to these groups.
Sponsoring organizations of need assessments
Public universities, national and local nonprofits, and state and local governments were most likely to publish a need assessment for a specific geographic area. The goals for these types of studies were almost always to understand the needs of local veteran populations and to provide recommendations for policy formulation, service delivery, and future study. Many of the national organizations have been productive because they can marshal financial and project support from their own budgets and from partnerships with outside philanthropic donors. 5 These organizations also have a broader set of personnel and institutional resources in which they can employ to conduct in-depth and comprehensive studies of veteran populations in a specific geographic region. Compared to university publications, fewer academic peer-reviewed need assessments have been conducted on veterans’ issues because universities often collaborate with philanthropic partners or funders to self-publish reports. Additionally, those assessments which have been peer-reviewed and published in academic journals depend on rigorous data collection through randomized surveys and statistical analysis, which may not be readily available to many university institutes. However, the impact of universities and academic research in the veterans’ need assessment literature cannot be understated; if not for these studies, many geographic areas would not be represented or documented. Ultimately, the propensity to conduct a need assessment depends on two critical factors: access to sufficient government or philanthropic financial support to design and implement the study and an institutional investment in improving the quality of life for their local and regional population. Given that needs assessments were conducted across geographic areas and levels, all with different sizes of veteran and military family populations, size of military population is not the only factor that determines where these needs assessments are conducted. We anticipate that more communities will collaborate with local nonprofits, universities, and think tanks in the future to study their local veteran populations.
Recommendations for Future Scholarship and Practice
Two themes emerge from analysis of this literature which have direct application to future scholarship and practice by researchers and community members around the country. Our study finds that needs assessments are often designed and implemented by public and private organizations in a balance between analytical rigor and available budgets. Resource constraints on the part of both funders and researchers ultimately determine the methods for data collection employed and the scope of needs covered in the study. Just as the need assessment literature reviewed here suggests that veterans and their family members have co-occurring sets of needs, multiple stakeholder groups and organizations may have a shared interest in the design and findings of a need assessment to inform their own service delivery to veteran populations. Organizations that conduct needs assessments should consider engaging community stakeholders from across a set of issue areas in order to use marshalled resources from these partners to expand the scope of the study, drawing upon each organization’s expertise or interest areas. For example, the King Foundation in Dallas–Fort Worth, TX, successfully implemented this approach, bringing together six different major philanthropies in a consortium to support the Center for a New American Security’s comprehensive study of veterans in the region (Kidder et al., 2016). Future needs assessments for the U.S. veteran population will be strengthened in capacity and resources by sponsoring organizations seizing opportunities to collaborate with others within their communities to help fund these studies.
Future need assessments also must employ rigorous mixed-method procedures that address a wide scope of issue areas and needs in studying the U.S. veteran population. Three studies—Virginia Tech’s study of the state of Virginia (Dunkenberger et al., 2010), RAND’s study of the state of New York (Schnell & Tanielian, 2011), and the Institute of Medicine’s (2013) study of the U.S. OEF/OIF veteran population—exhibited many best practices in employing rigorous methods to their analysis. Each study used mixed-method study techniques, combining quantitative data collection through surveys (with random sampling) and qualitative data collection through interviews and focus groups, and they included an in-depth discussion on the methods employed, with a granular focus on detail that the study could be replicated. In their analysis of the findings, the authors of these three studies compared their samples to the national veteran population using publicly available data from the U.S. Census Bureau and the VA. These studies not only addressed more than 10 of the identified 17 topics, but they also provided recommendations for future practice and scholarship based on their findings. As the needs and experiences of a community’s veteran population are dynamic and ever evolving, we encourage researchers and both private and public organizations who are interested in conducting need assessments of any type, including those for veterans, to employ both informal and formal information and data gathering methods. This can be achieved through mixed-method research designs (e.g., the three above-mentioned studies) and through community engagement that fosters multisector collaboration and participation (e.g., pooled funding, data sharing, population access) to execute studies that will maximize rigor, validity, and public value.
Conclusion
The available literature on the needs of veterans throughout the United States provides critical qualitative and quantitative data on which service providers, collaboratives, policy makers, and philanthropies can use to augment the quality and efficacy of their service delivery to veterans. The 61 needs assessments published over the past 11 years reflect a rapidly growing interest and commitment to studying and serving veterans across the country. While counties and local governments with large veteran populations are studying how best to serve their veteran constituents, this interest is shared among states and regions with lower populations of veterans, such as in Alaska and North Dakota. This geographic breadth, however, does not greatly alter the experiences of veterans postservice because as national needs assessments detailed, veterans in every corner of the country noted common themes about their inability to access VA services, issues with transition and feeling culturally isolated from civilian society, and unique sexual health needs among women veterans (Carter & Kidder, 2013; Institute of Medicine, 2013; National Council for Behavioral Health, 2012). The results found in these needs assessments parallel discussions in academic scholarship of veterans’ issues, particularly mental and physical health.
However, these 61 studies do not provide a complete, holistic picture of all the needs of veterans across the country. Future needs assessments, regardless of sponsoring organization, should include either the whole range of needs veterans face or detailed and rigorous analysis of one or a few particularly salient issues for the veterans and their families in a given geographic area. Not only should state, county, and local governments invest in the time and resources to study their veteran populations and how best to serve them, but further attention should also be given to some of the understudied needs of veterans, including poverty, National Guard and Reserve service members and veterans, and behavioral health. Further research should be conducted on the unique experiences and set of challenges women and minority veterans face, particularly those of African American and Hispanic veterans and military families.
Footnotes
Appendix A

| Article | Location(s) Studied | Number of Topic Areas Studied | Study Method |
|---|---|---|---|
| Albright, Hammer, and Currier (2017) | Eight counties in Alabama | 10 | Mixed method |
| Altarum Institute (2014a) | Metro Detroit, MI | 7 | Mixed method |
| Altarum Institute (2014b) | State of Michigan | 9 | Mixed method |
| Altarum Institute (2015a) | Eight counties in Michigan | 4 | Mixed method |
| Altarum Institute (2015b) | Seven counties in Michigan | 6 | Mixed method |
| Altarum Institute (2015c) | Three counties in Michigan | 10 | Mixed method |
| Altarum Institute (2015d) | Six counties in Michigan | 6 | Mixed method |
| Blaskovich, Reed, Redden, and Doggett (2012) | State of Montana | 3 | Quantitative |
| California Department of Veterans Affairs (2011) | State of California | 7 | Mixed method |
| Carlson, Stromwall, and Lietz (2013) | United States (National) | 5 | Qualitative |
| Carter and Kidder (2013) | Twelve states in the Western United States | 7 | Mixed method |
| Carter and Kidder (2015) | Thirteen counties in Pennsylvania | 5 | Mixed method |
| Castro and Kintzle (2017) | Metro San Francisco, CA | 8 | Quantitative |
| Castro, Kintzle, and Hassan (2015) | Orange County, CA | 6 | Quantitative |
| Castro, Kintzle, and Hassan (2013) | Los Angeles County, CA | 7 | Quantitative |
| Disabled Veterans of America (2014) | United States (National) | 10 | Qualitative |
| Douds et al. (2014) | State of Pennsylvania | 12 | Mixed method |
| Dunkenberger et al. (2010) | State of Virginia | 11 | Mixed method |
| Dynia (2009) | Middlesex County, CT | 9 | Qualitative |
| Elliott, Gonzalez, and Larsen (2012) | State of Nevada | 5 | Quantitative |
| Ellison et al. (2012) | Metro Boston, MA | 5 | Quantitative |
| Farmer et al. (2017) | State of Massachusetts | 9 | Mixed method |
| Gabrielian, Yuan, Rubenstein, Andersen, and Gelberg (2013) | States of Arizona, California, and New Mexico | 6 | Mixed method |
| Georgia Center for Nonprofits (2012) | Metro Atlanta, GA | 7 | Mixed method |
| Guettabi and Frazier (2015) | State of Alaska | 6 | Quantitative |
| Hardy (2013) | State of Tennessee | 4 | Qualitative |
| Harris County (TX) Veteran Service Office (2017) | Harris County, TX | 11 | Qualitative |
| Haynes and Tavares (2010) | State of Ohio | 5 | Qualitative |
| Hoskins (2013) | King County, WA | 11 | Quantitative |
| Institute of Medicine (2013) | United States (National) | 9 | Mixed method |
| Kidder, Schafer, and Carter (2016) | Metro Dallas–Fort Worth, TX | 7 | Mixed method |
| Kintzle, Rasheed, and Castro (2016) | Metro Chicago, IL | 6 | Quantitative |
| Knopf (2013) | United States (National) | 5 | Mixed method |
| Kotarba, Wivagg, Pierson, Martinez, and Kappler (2016) | State of Texas | 10 | Mixed method |
| Lachman and Laing (2008) | Pierce County, WA | 2 | Qualitative |
| Liscord and Elliott (2013) | State of Maine | 3 | Quantitative |
| McCarthy (2014) | Bristol County, MA | 5 | Quantitative |
| Miller, Finn, and Newman (2014) | United States (National) | 3 | Qualitative |
| Milliken, Auchterlonie, and Hoge (2007) | United States (National) | 4 | Quantitative |
| Morris (2012) | Metro Charlotte, NC | 10 | Mixed method |
| National Council for Behavioral Health (2012) | United States (National) | 3 | Mixed method |
| Northeast Florida Women Veterans (2015) | Metro Jacksonville, FL | 7 | Qualitative |
| Peterson (2014) | States of Minnesota, Montana, and North Dakota | 2 | Qualitative |
| Petri and Gee (2015) | State of Missouri | 7 | Mixed method |
| Prudential Financial (2012) | United States (National) | 4 | Quantitative |
| Pryor and DiNisco (2008) | Metro Rochester, NY | 6 | Qualitative |
| Pryor and Pryor (2010) | Rensselaer County, NY | 8 | Mixed method |
| Rede Group (2014) | State of Oregon | 1 | Mixed method |
| Schell and Tanielian (2011) | State of New York | 6 | Mixed method |
| Spelman, Hunt, Seal, and Burgo-Black (2012) | United States (National) | 5 | Mixed method |
| Stevens and Brutschy, 2014 | San Mateo County, CA | 7 | Mixed method |
| Sturtevant, Brennan, Viverios, and Handelman (2015) | United States (National) | 6 | Qualitative |
| Tanielian, Hansen, Martin, Grimm, and Ogletree (2016) | Metro Detroit, MI | 5 | Mixed method |
| Tanielian et al. (2014) | United States (National) | 1 | Quantitative |
| United Way of King County (2009) | King County, WA | 1 | Qualitative |
| The Washington Post and Kaiser Family Foundation (2014) | United States (National) | 6 | Quantitative |
| Wilder Research (2015) | Saint Louis and Itasca Counties, MN | 7 | Mixed method |
| Wivagg, Martinez-Ramos, and Pierson (2016) | Metro San Antonio, TX | 4 | Quantitative |
| Volunteer Lawyers for Justice (2014) | State of New Jersey | 4 | Quantitative |
Acknowledgments
We would like to thank participants at the Canadian Institute of Military and Veteran Health Research Forum 2018 in Regina, SK, David Albright, and Zachary Huitink for their feedback on this article and to Alex MacDonald and Nathaniel Birnbaum at Syracuse University for their research assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.