
Abstract
Military suicide prevention efforts would benefit from population-based research documenting patterns in risk factors among service members who die from suicide. We use latent class analysis to analyze patterns in identified risk factors among the population of 2660 active-duty military service members that the Department of Defense Suicide Event Report (DoDSER) system indicates died by suicide between 2008 and 2017. The largest of five empirically derived latent classes was primarily characterized by the dissolution of an intimate relationship in the past year. Relationship dissolution was common in the other four latent classes, but those classes were also characterized by job, administrative, or legal problems, or mental health factors. Distinct demographic and military-status differences were apparent across the latent classes. Results point to the need to increase awareness among mental health service providers and others that suicide among military service members often involves a constellation of potentially interrelated risk factors.
Background
Although the military generally selects young, healthy individuals, the suicide rate among active-duty military service members has recently increased and is now equivalent to the suicide rate in the general population (Pruitt et al., 2019). Most research documenting this trend has focused on the Army, the largest branch of the US military. The suicide rate among active-duty Army personnel was below that of the general population and stable until 2004; but exceeded the suicide rate in the general population by 2008 (Black et al., 2011; Bryan et al., 2012; Bush et al., 2013; Kuehn, 2009; Logan et al., 2012; Nock et al., 2013). Over time, the suicide rate in the Army has consistently been higher than that in the Air Force, Marines, and Navy (Pruitt et al., 2018; Ramchand et al., 2011).
In the general population, the predominant risk factors for suicide include: mental health, alcohol, and substance abuse problems; interpersonal/family relationship issues; legal concerns; financial difficulties; and physical health challenges (Ertl et al., 2019; Nock et al., 2008, 2013; Stone et al., 2018). In part, suicide risk factors in the active-duty military population are similar (Black et al., 2011; Bush et al., 2013; Ghahramanlou-Holloway et al., 2017; Hyman et al., 2012; Logan et al., 2012; Maguen et al., 2015; Nock et al., 2013). Additionally, service members face a distinct set of service-connected risk factors since military service entails exposure to a set of occupational hazards (e.g., frequent deployments, exposure to military training exercises, and/or combat) that can lead to the disruption of relationships and the development of physical and mental health problems (Ardelt et al., 2010; Black et al., 2011; Bryan et al., 2012; Wilmoth et al., 2019). Other military-related risk factors include: military administrative issues, such as demotion, separation, and discharge (Ghahramanlou-Holloway et al., 2017); job problems related to a chosen or assigned military occupational specialty (Logan et al., 2012); and service-connected problems with sleep (Hyman et al., 2012). Reports from the Department of Defense Suicide Event Report (DoDSER) system between 2008 and 2017 confirm these findings (Psychological Health Center of Excellence, 2019; Pruitt et al., 2019). In each year, the most frequently identified risk factor was a failed intimate relationship, which was documented in almost half of all suicides among active-duty service members. Other prominent risk factors identified in each year include mental health concerns, job-related problems, military administrative issues, and civilian legal challenges.
In response to these empirical findings, suicide prevention materials published by the Defense Suicide Prevention Office (DSPO, 2019), an agency within the Department of Defense (DoD), identify three domains of potential suicide risk factors for service members: failed relationships; administrative or legal problems; and mental health concerns. Dissemination of this information is an extremely important response to the high and increasing rate of suicide among active-duty service members. Raising awareness of suicide risk factors may help improve risk recognition, increase effective intervention, and reduce suicides among military personnel. However, identification of these three domains of potential suicide risk may not sufficiently account for the possibility that service members who die by suicide can have multiple, potentially interrelated risk factors across different areas of life (Logan et al., 2011). For this reason, understanding patterns among risk factors across multiple domains can help improve suicide prevention efforts.
Extant studies do not sufficiently account for patterns in the broad array of risk factors that contribute to military suicides across multiple branches of the military. One study used DoDSER data and examined risk factors among suicide attempters and persons who died by suicide (i.e., decedents) in the US Army, but limited analysis to seven risk factors (Skopp et al., 2016). It identified three patterns among decedents: external and antisocial risk factors, including legal/administrative and work problems, and a history of substance abuse (12%); psychiatric diagnoses, prior self-injurious behavior, and a failed intimate relationship in the last 90 days (25%); and very low prevalence of identified suicide risk factors (63%). In order to expand our understanding of the factors that contribute to US military suicide deaths, and inform military suicide prevention efforts, we build on this earlier effort by using latent class analysis (LCA) to empirically distinguish patterns among 33 event-level risk factors reported by posthumous forensic autopsy for all US military suicide deaths from 2008 to 2017. Our expectation is that, similar to patterns observed in the general population (Logan et al., 2011), the majority of military suicide decedents will have multiple risk factors present at the time of their suicide, and that there will be empirically discernible patterns of risk that characterize subgroups of suicides.
The military is a highly diverse population (Office of the Under Secretary of Defense, 2018). Given that suicide varies in the general population in relation to demographic characteristics (Denney et al., 2009; Hawton, 2000; Kubrin & Wadsworth, 2009; Kuehn, 2009; Qin et al., 2003), we expect that heterogeneity in the demographic characteristics of active-duty service members translates into dissimilar service experiences and suicide risk-factor profiles. Such variation might be evident by age, biological sex, race-ethnicity, marital status, and level of education. Thus, our first set of hypotheses is based on a general expectation that the prevalence of identified risk factors among military service members who died by suicide will vary by demographic characteristics. Specifically, given that an increased amount of time in the military may be associated with cumulative exposure to hazards (Wilmoth et al., 2019) and that those who join or serve in the military later in life may experience a greater amount of life-course disruption (Elder, 1986; Wilmoth & London, 2013), we hypothesize that increased age will be associated with differential identified risk-factor patterns among suicide decedents. Recognizing that research on suicide and social integration provides conflicting evidence regarding the effects of over- or under-integration into a social system (Braswell & Kushner, 2012; Kushner & Sterk, 2005; Tsai et al., 2015), we hypothesize that, among military service members who died by suicide, those with historically lower levels of integration into the military environment (i.e., women, racial-ethnic minorities) will have identified risk-factor patterns that are distinct from those with historically higher levels of integration into the military environment (i.e., men, Whites). Though included in the analysis, we do not make predictions regarding level of education.
Our second set of hypotheses focuses on the military status and experiences of those who died by suicide. We expect that military status and experiences—branch, rank, and number of deployments—will be associated with differential identified risk-factor patterns. We hypothesize that an increase in the number of deployments will be associated with patterns reflecting a higher prevalence of identified risk factors because deployment is likely associated with cumulative exposure to military hazards. Recognizing that higher rank in the military may be associated with more or different risk factors, such as job-related stress or cumulative exposure to hazardous conditions, but also may be associated with countervailing resources that reduce risk, such as higher socioeconomic status and different access to social support, we predict that identified risk-factor patterns will not vary by rank. Given the fact that the Army has outperformed other branches of the US military in integrating behavioral health care into primary care settings (Ramchand et al., 2011; Ursano et al., 2018), we predict differences in mental health risk factors among Army personnel compared to other branches.
Methods
Data
As part of the 2001 US National Strategy for Suicide Prevention, the Department of Defense created the Suicide Event Report (DoDSER) system to consolidate disparate systems within each military branch (Pruitt et al., 2019). Within 60 days of a suicide event, trained professionals collect and submit information on risk factors potentially related to the event to the DoDSER system. Reports include the service member’s demographic characteristics, suicide event details, and information pertaining to potentially contributing risk factors for which there is evidence (Bush et al., 2013; Gahm et al., 2012; Kemp & Bossarte, 2012; Pruitt et al., 2019). We analyzed data from the DoDSER system for the population of 2660 active-duty military service members who died by suicide between 2008 and 2017.
This project was approved as “Not Human Subjects Research” by the Defense Health Agency, COD#: CDO-18-2038, and by the Syracuse University Institutional Review Board, IRB #18-137. Fully de-identified data were provided by the Psychological Health Center of Excellence.
Measures
Distribution of Risk Factors Across Population, 2008–2017 DoDSER System, N = 2660.
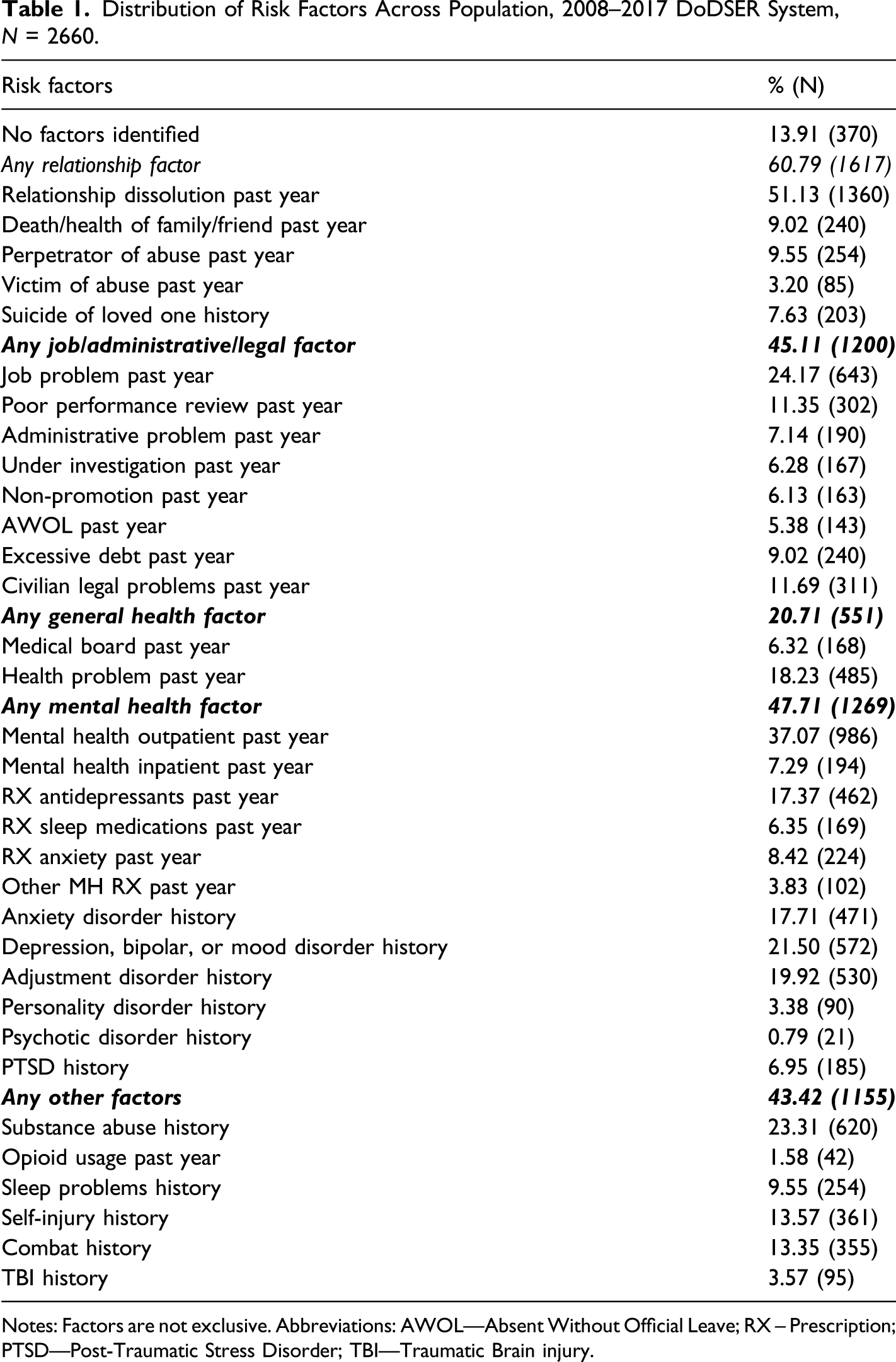
Notes: Factors are not exclusive. Abbreviations: AWOL—Absent Without Official Leave; RX – Prescription; PTSD—Post-Traumatic Stress Disorder; TBI—Traumatic Brain injury.
Analytic Strategy
We describe the prevalence of all identified risk factors for the population of military suicide decedents. To increase understanding of suicide decedents with no identified risk factors, we specified a logistic regression model to identify associations with demographic and military-status characteristics. Subsequent analysis focused on decedents with one or more identified risk factor. After examining the distribution of the number of identified risk factors recorded for these decedents, we used LCA to delineate patterns among them. LCA, which has been used to examine patterns among suicide-related factors in the general population (Logan et al., 2011) and active-duty U.S. Army personnel who attempted or died by suicide (Skopp et al., 2016), allows for identification of classes of cases or events using non-mutually exclusive variables (Hagenaars & McCutcheon, 2002). Evaluation of the Bayesian information criteria indicated that a five-class model best fit the data (see Appendix 1). We examined the probabilities of each risk factor within and across classes to describe the characteristics of the five latent classes. Finally, we specified logistic regression models to determine associations between demographic and military-status characteristics and membership in each of the five latent classes. Because there was a limited amount of missing data for age and race-ethnicity, we employed a complete case strategy for the logistic regression models. All analyses were conducted using STATA 16.0 (College Station, TX).
Results
Distribution of Identified Risk Factors
Table 1 presents the distribution of all identified risk factors, grouped by domain, among the 2660 military suicide decedents from 2008 to 2017. In this population, 370 suicide decedents (13.9%) did not have any of the 33 identified risk factors. Logistic regression analysis revealed that decedents with no identified risk factor were younger and had never been deployed, which may be indicative of lesser integration in the Armed Forces (Appendix 2). Regarding the multi-factor domains: a relationship risk factor was identified for 60.8% of suicide events; a job/administrative/legal risk factor was identified for 45.1%; a general health risk factor was identified for 20.7%; a mental health risk factor was identified for 47.7%; and at least one of the other risk factors was identified for 43.4%. Notably, among the specific identified risk factors, the most prevalent was a relationship dissolution in the past year, which was identified in 51.1% of military suicide events between 2008 and 2017.
Factor Patterns Among Suicide Decedents with at Least One Identified Risk Factor
Overall, 81.6% of suicide decedents had two or more risk factors reported (Figure 1). The mean of the distribution was 4.7 identified risk factors, which demonstrates that military suicide risk factors are typically co-occurring. Distribution of number of risk factors for decedents with at least one factor identified, 2008–2017 DoDSER System, N = 2290.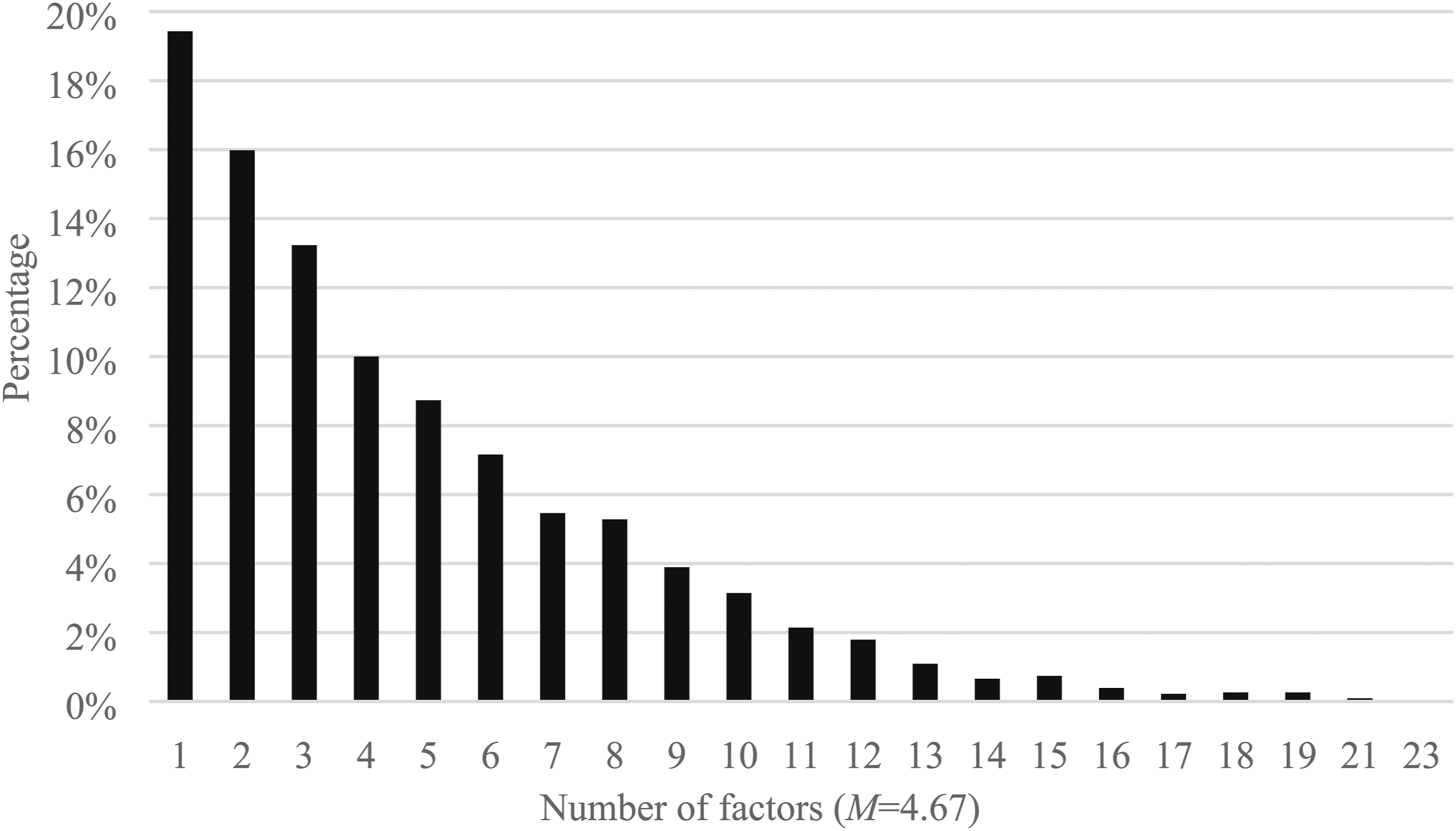
Latent Class Analysis, Probabilities for Identified Risk Factors, 2008–2017 DoDSER System.
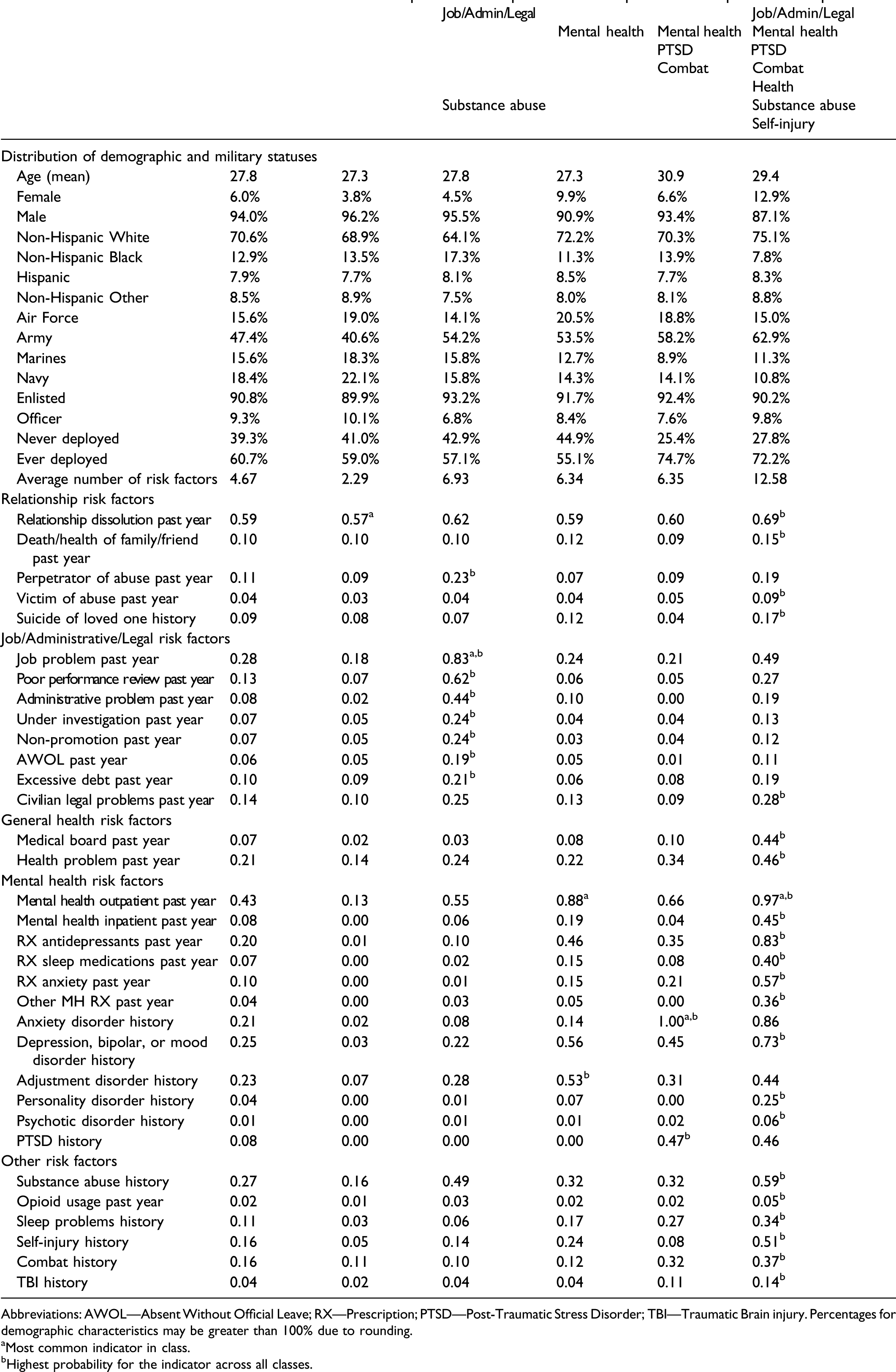
Abbreviations: AWOL—Absent Without Official Leave; RX—Prescription; PTSD—Post-Traumatic Stress Disorder; TBI—Traumatic Brain injury. Percentages for demographic characteristics may be greater than 100% due to rounding.
aMost common indicator in class.
bHighest probability for the indicator across all classes.
Classes 1 and 2 were characterized primarily by dynamic risk factors. For the largest latent class, Class 1 (N = 1272; 55.5%), the most common identified risk factor was past-year relationship dissolution (55%). It is important to note that in Class 1 the probabilities for all other identified risk factors were at or near their lowest levels relative to the other four latent classes, with no other risk factor having a probability over 18%.
Classes 2–5 each had probabilities of relationship dissolution and past-year mental health outpatient visit over 50%. In addition, Class 2 (N = 177; 7.7%) was characterized by decedents who had job-related, administrative, or legal problems, with the highest probability of past-year job problems and, relative to the other latent classes, the highest probabilities of all but one of the identified risk factors in the job/administrative/legal factors domain. Notably, a high probability of lifetime history of substance abuse (49%) also characterized Class 2.
In addition to high probabilities of relationship dissolution and mental health outpatient visits, Classes 3–5 were characterized by relatively high probabilities of both dynamic and static mental health risk factors. However, the predominant mental health factors varied across these latent classes. Class 3 (N = 434; 19%) was characterized by relatively high lifetime probabilities of several mental health factors, but a 0% probability of PTSD and a low probability of combat history. Of note, relative to the other latent classes, Class 3 had the highest probability of adjustment disorder history (53%). Probabilities for depression/bipolar/mood disorder history (56%) and prescribed antidepressants (46%) were also relatively high.
Similar to Class 3, Classes 4 and 5 had relatively high probabilities of several mental health risk factors. However, the risk factor patterns were different than in Class 3. Specifically, Classes 4 and 5 were the only latent classes with a probability of PTSD above 0% (47% in Class 4, 46% in Class 5). They also had moderate, but distinctly higher, probabilities of combat history (32% in Class 4, 37% in Class 5). Class 4 (N = 213; 9.3%) was additionally characterized by a 100% probability of anxiety disorder. Class 5 (N = 194; 8.5%) was additionally characterized by decedents with systemic risk factors across all six domains. Specifically, relative to the other four latent classes, Class 5 had the highest probabilities for 22 of the 33 identified risk factors, including civilian legal problems, all of the mental health treatment risk factors, health problem in the last year, substance abuse history, self-injury history, and combat history.
Results From Logistic Regression Models Analyzing Demographic and Military Status Associations with LCA Class Membership, 2008–2017 DoDSER System, N = 2202.
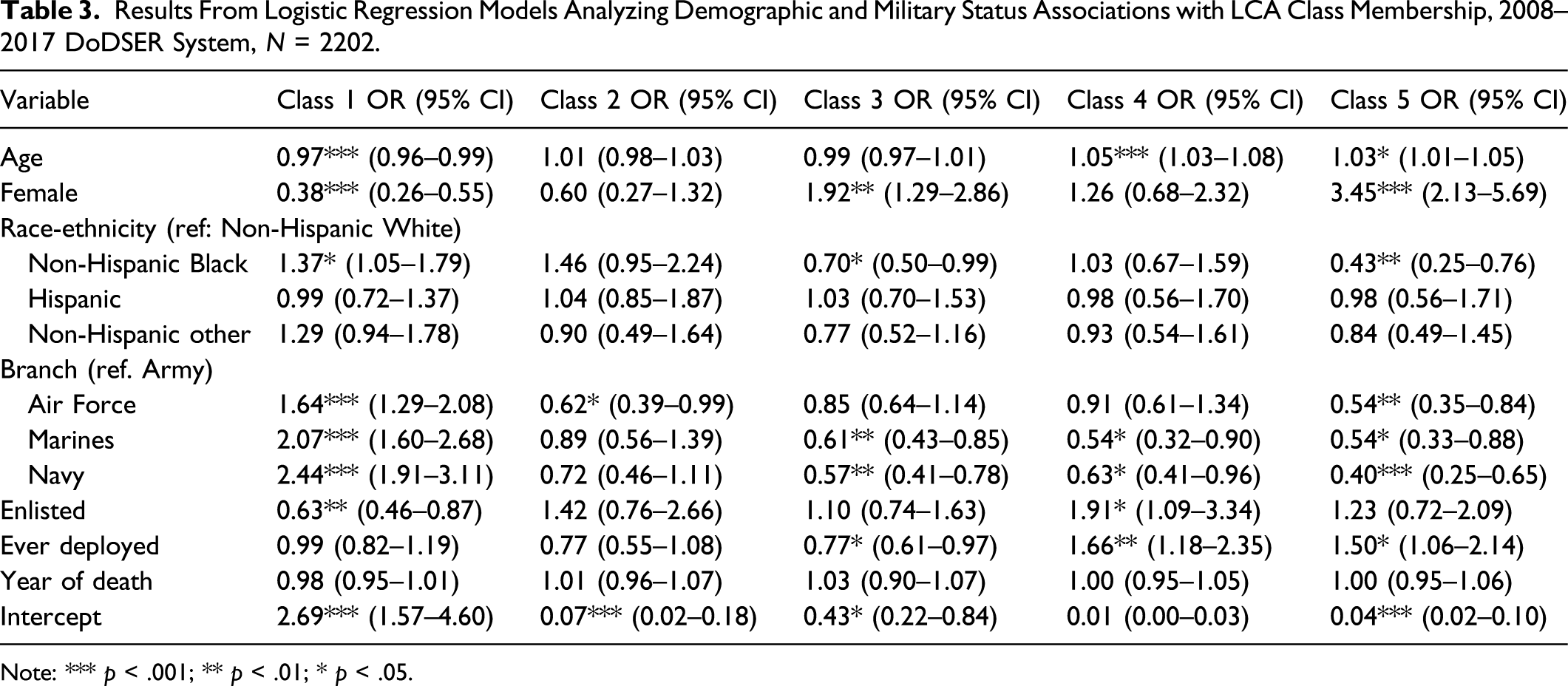
Note: *** p < .001; ** p < .01; * p < .05.
Discussion
This study yields novel findings, as well as some that are consistent with those reported in the literature. Likely because we analyzed a broader array of risk factors, we document that 13.9% of military suicide decedents had no identified risk factor—much lower than reported in Skopp et al. (2016). This was more common among younger military service members and those who had never been deployed. While it may be that some of these suicide decedents actually did not experience any of the 33 risk factors examined in this study, it is also possible that such factors existed in the lives of these service members but were not discovered during the posthumous investigation of the suicide. Recently enacted quality control procedures in the DoDSER program centered on post-suicide data collection may result in a reduction in the percentage of decedents without an identified risk factor in future data (Skopp et al., 2016).
It is probable that interventions enacted by the DoD will not be able to prevent all suicides among military personnel (Sisti & Joffe, 2018; Stein et al., 2019). However, in an effort to reduce military suicide as much as possible, the DoD is taking a multi-pronged approach to prevention, which includes efforts to teach coping and problem-solving skills to young military service members early in their careers (Department of Defense, 2019). Results from this study support enhancement of this programmatic initiative. The results also indicate the need for the DoD to increase attention to the overlapping, compounding influences of coexisting risk factors and the emphasis on particular aspects of single risk factors.
First and foremost, it is important that suicide prevention efforts aimed at military personnel account for the fact that risk factors are often co-occurring: among military suicide decedents from 2008–2017, 81.6% with any identified risk factor had two or more risk factors recorded, with a mean of 4.7 risk factors. Thus, while it is important for mental health providers and others to be aware of singular risk factors (as discussed below), it is also imperative to realize that deaths by suicide often result from a constellation of potentially interrelated risk factors (Stanley et al., 2016; Van Orden et al., 2010). Findings from this study indicate the need for mental health providers and others in the military chain of command to pay particular attention to military service members with relationship problems with or without co-occurring risk factors. When relationship problems are co-occurring, providers should especially be attentive to service members who are experiencing: (1) job, administrative, or legal problems with/without accompanying substance abuse history; (2) adjustment disorders and/or depression; (3) PTSD and/or combat history with/without an accompanying anxiety disorder; and (4) PTSD and/or combat history with accompanying systemic risk factors across multiple domains.
Similar to other evidence (Pruitt et al., 2017, 2019), our results emphasize the importance of a continued focus on relationships in military suicide prevention efforts. The largest latent class, containing 55.5% of suicide decedents with at least one identified risk factor, was primarily characterized by the dissolution of an intimate relationship in the past year. Furthermore, 59% or more of suicide decedents in the other four latent classes experienced a relationship dissolution in the year prior to their suicide.
Consistent with a risk factor pattern seen in prior research (Skopp et al., 2016), one of the five latent classes we found included job, legal, and/or administrative problems coupled with substance abuse problems. However, as the current study analyzed a broader array of risk factors relative to prior studies, we clarified that this latent class also included relationship dissolution in the prior year and receipt of outpatient mental health services. In our study, this latent class included 7.7% of the suicide events.
Unlike prior research (Skopp et al., 2016), we included separate indicators for a number of different psychiatric diagnoses and psychiatric treatment modalities. It is important to note that even after including this more expansive set of mental health risk factors in the analysis, less than half (47.7%) of suicide decedents had any mental health factor reported in the forensic autopsy. While mental health outpatient care was common in four of the five latent classes, our analytic strategy revealed important differences in three of the latent classes regarding other mental health risk factors. Importantly, PTSD and combat history were only predominant in two of the five identified latent classes, representing a total of 17.8% of suicide decedents with at least one identified risk factor. Thus, the majority (82.2%) of suicide decedents with at least one identified risk factor were part of latent classes in which PTSD was not reported as a contributing factor and levels of combat history were low. It is also worth noting that a prior history of self-injury was only prominent in the one latent class characterized by systemic risk factors inclusive of relationship dissolution, job/legal/administrative problems, mental health factors, and moderate levels of combat experience and PTSD. Army STARRS research on military service members who attempted suicide suggests that some service members have mental health disorders that are undetected and/or untreated (Naifeh et al., 2019; Nock et al., 2014; Ursano et al., 2018). We agree with the recommendations in these reports that there is a need to increase mental health screening and access to care for all service members. As is recognized by the DoD (Department of Defense, 2019), an increase in access to mental health services may reduce suicide attempts and events, while contributing to service members’ well-being more generally.
Turing our attention to the most prominent single risk factors, the DoD also recognizes that the dissolution of intimate relationships is a primary risk factor contributing to military suicide (Department of Defense, 2015, 2019). Its suicide prevention efforts include increasing awareness of suicide and potential avenues for supporting individual service members experiencing relationship difficulties. However, current DoD goals articulated in its Strategy for Suicide Prevention (2015) do not specifically focus on interventions for the relational dyad. Given that relationship dissolution in the prior year was the most common identified risk factor, was prominent across all five latent classes, and was the primary risk factor in the largest latent class, the results of this study suggest the need for couple-level intervention, inclusive of married and non-married personnel, at all stages of the relationship life-course (i.e., formation, stabilized, de-coupling, ended). Enhanced understanding of the timing and sequencing of relationship dissolution in relation to other risk factors might also enhance the efficacy of interventions. Thus, efforts to develop and strengthen coping and problem-solving skills should expand beyond the soldier to include the partner. Such interventions could aim to provide couples counseling to enhance intra- and inter-personal resilience, while also reinforcing help-seeking behaviors and critical skills, such as communication, decision-making, parenting, conflict resolution, and coping with physical and mental health issues. Interventions might also help military personnel develop the needed skills for ending relationships, including but not limited to effective processing of grief and adjustment to relational transitions. While the dissolution of intimate relationships among military personnel will continue, knowledge that this factor is primary among suicide decedents, and often co-occurs with other risk factors, should compel the DoD to explore all possible avenues to strengthen relationships and ensure that soldiers have the skills and resources to constructively resolve relational issues when needed.
It is noteworthy that current DoD suicide prevention literature does not provide any mention of job problems (Department of Defense, 2015; 2019; DSPO, 2019). Yet, a job problem in the year prior to their suicide was identified as a risk factor in just under a quarter (24.2%) of military suicide events recorded in the DoDSER system between 2008 and 2017. Notably, this factor was prominent in four out of the five latent classes described in this study. Thus, our results suggest that the DoD’s focus on teaching problem-solving skills to military personnel should include an actual application or performance aspect of these particular skills when facing job, legal, and/or administrative problems. Organization-level initiatives aimed at training supervisors on how to approach and assist employees dealing with work related challenges could be beneficial. As in any organization, military personnel will experience job-related problems that may possibly result in salient role loss and identity change. Since this risk factor is common among military suicide decedents, DoD programs that teach problem-solving and coping skills should proactively address job-related challenges. In addition, avenues should be available for military personnel to receive support in instances when they are struggling with their job performance or have military- or civilian-related administrative legal issues.
While reasonable to provide these suggested resources partly through the mental health service structure, less than half of suicide decedents have a mental health risk factor reported on forensic autopsy. Thus, it would be strategic to provide suicide prevention resources outside of the mental health service delivery structure to members of the chain of command who could serve as an additional layer of risk monitoring. Another way to do so would be through the use of peer support, a facet of prevention recognized, but not fully developed, by the DoD (Department of Defense, 2015). Psychological resilience and preparedness are often nurtured by teaching individuals crucial skills to proactively anticipate, address, and adapt to career-related challenges (Vuori et al., 2012). The inclusion of a fully-developed peer component—inclusive of peers trained as gatekeepers and/or mentors (Goldsmith et al., 2002; Ramchand et al., 2011)—may help create a network of support throughout the military that reinforces empowerment and mastery of relationship and job-related skills among service members and extends suicide prevention services beyond the immediate mental health service delivery infrastructure.
Limitations
The primary limitations of this study are related to data. All investigations conducted for military suicide decedents are dependent on official military records and retrospective reporting by friends and family members of the service member who committed suicide. It is possible that these records do not capture information on risk factors that occurred outside of the official military service record or were not known to family or friends of more-isolated service members. Based upon this limitation, and the finding that 13.9% of service members did not have any identified risk factor, it is likely that the reported prevalence rates for risk factors encompassed within the official military service record are underestimated. In addition, we do not have comparative information about the prevalence of all risk factors included in this study in the overall military population. The DoD (Deployment Health Clinical Center, 2017) does provide information on the prevalence of diagnosis of a limited number of mental health conditions, but these data do not include lifetime diagnosis of chronic mental health conditions like those used in this study or measurement of risk factors outside of the mental health arena. Thus, we cannot discern whether the identified risk factors we describe are unique to suicide decedents or representative of the larger military population.
While this study reports that risk factors related to relationship, job, administrative, and legal problems are common among military suicide decedents, it is not possible to disentangle the timing and sequencing of factors with these data. Thus, we could not explore whether these social factors may have preceded and generated some of the reported mental health and substance use issues. Finally, it is worth noting that this study only focused on military suicide decedents, and thus does not provide clarification to the lingering question as to whether military suicide attempters and decedents have similar or dissimilar characteristics or risk factors (Schoenbaum et al., 2014; Skopp et al., 2016; Ursano et al., 2015). It also does not address the question of overlap in the risk factors associated with veteran suicide, which is an important direction for future comparative research. While we focus on military suicide decedents only in this study, in order to account for the detail involved in analysis of a broad array of risk factors, it would be beneficial for future research to provide a similar analysis among military suicide attempters and veterans, respectively. Despite these limitations, the thoroughness of the suicide factor data available for military service members who committed suicide between 2008 and 2017 allowed us to effectively describe patterns in the prevalence and coexistence of identified risk factors for military suicide events, which increases our understanding of the complexity surrounding suicide among active-duty service members. Though not testable with the data used in this study, future research should explore whether these patterns are also present among military veterans.
Conclusions
Results from this study demonstrate that there is a broad array of suicide risk factors among military suicide decedents and that they are often co-occurring. PTSD and mental health are risk factors for some, but not all, of military service members. Risk factors related to relationships, job, administrative, and legal problems are also common among military suicide decedents and point to the need to more fully take the social determinants of military suicide into account. For many military suicide decedents, their relationship problems are accompanied by job, administrative, or legal problems, substance abuse, PTSD and/or combat experience, and mental health risk factors. Continued emphasis in suicide prevention efforts on well-established suicide risk factors, such as relationship problems and mental health, is necessary. However, mental health providers should be aware that suicide among military service members often involves a constellation of risk factors. In addition, the DoD’s current emphasis on individual service members must be expanded to more directly involve spouses and intimate partners, and efforts must be made to ensure military personnel are equipped to successfully address problems they have with their job and/or military career. Such a re-orientation toward recognizing that suicide risk factors are often co-occurring, proactive relationship building, increased accessibility to mental health services for all service members, and the possible upstream social structural factors that drive suicide may provide new opportunities for intervention and increase the effectiveness of suicide prevention efforts.
Footnotes
Author Contributions
Scott Landes—Conceptualization, methodology, formal analysis, data curation. Janet Wilmoth—Conceptualization and writing. Andrew London—Conceptualization and writing. Ann Landes—Conceptualization and writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication benefited from NIA Center Grant P30AG066583, Center for Aging and Policy Studies. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix 1
Bayesian Information Criterion (BIC) by Model, 2008–2017 DoDSER System, N = 2502.
Model
BIC
2 classes
49,816.5
3 classes
49,436.5
4 classes
49,152.8
5 classes
6 classes
49,356.2
7 classes
49,319.7
8 classes
49,403.2
9 classes
49,497.6
Appendix 2
Results from logistic regression model analyzing demographic and military status associations with no risk factors, 2008–2017 DoDSER System, N = 2502. Note:*** p < .001.
Variable
OR (95% CI)
Age
0.96*** (0.94–0.98)
Female
0.55 (0.30–1.01)
Race-ethnicity (ref: Non-Hispanic White)
Non-Hispanic Black
1.17 (0.81–1.67)
Hispanic
0.83 (0.50–1.37)
Non-Hispanic Other
1.41 (0.95–2.09)
Branch (ref: Army)
Air Force
1.20 (0.87–1.67)
Marines
0.89 (0.61–1.30)
Navy
1.24 (0.89–1.72)
Enlisted
0.81 (0.52–1.26)
Ever deployed
0.61*** (0.47–0.79)
Year of death
1.00 (0.96–1.05)
Intercept
0.54 (0.25–1.16)