
Abstract
Most health care services in the United States are delivered by private providers. The Veterans Health Administration (VHA) serves as one major exception. However, over the past decade, various new policies have expanded veterans’ access to community providers, opening an ongoing debate over how far privatization should go. We fielded a national survey (N = 5,852, including 772 veterans) in early 2022 on four privatization proposals of varying scope. Americans broadly supported limited expansions of Community Care but were sharply divided on proposals to replace the VHA through private contracting or private insurance. Conservatives were the most consistent supporters. Veterans who received VHA care were less supportive, and veterans who received Community Care more supportive, of the more far-reaching proposals. Contrary to expectations, veterans satisfied with Community Care were not more supportive of unrestricted privatization. Future reform beyond existing Community Care arrangements may face public resistance, though opinion remains malleable.
Keywords
Introduction
The Veterans Health Administration (VHA), the operational health arm of the U.S. Department of Veterans Affairs, is the largest integrated health care system in the United States, delivering comprehensive primary and specialty medical care, behavioral health services, and related social support to roughly 9.2 million enrolled veterans through more than 170 medical centers and 1,100 outpatient facilities (U.S. Department of Veterans Affairs, 2024c, 2024d). Veterans are generally eligible for VHA care if they “served in the active military, naval, or air service and didn’t receive a dishonorable discharge” (U.S. Department of Veterans Affairs, 2026a). For most of its postwar history, the VHA has operated as a government-owned, government-operated system staffed by salaried federal clinicians. This organizational model sits uneasily alongside the otherwise privately delivered American health care system and has been the subject of recurring political debate over the proper balance between public provision and private contracting (Wu, 2025).
That policy debate over the VHA has intensified substantially over the past decade under presidencies from both parties and policy changes have increasingly introduced private components. The Veterans Access, Choice, and Accountability Act of 2014 (Choice Act), enacted under the Obama administration in the wake of the Phoenix wait-time scandal, established the first comprehensive mechanism for veterans to seek care from non-VHA providers at veterans affairs expense (Bass et al., 2021; Sterling et al., 2022). The Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of 2018, signed by President Trump, consolidated and substantially expanded that mechanism through the Veterans Community Care Program (Massarweh et al., 2020; Mattocks et al., 2021). The program consolidated multiple prior authorities and allowed veterans meeting specific criteria to receive care from non-VHA providers at VA expense under the Veterans Community Care Program. More recent policy developments have accelerated the trajectory further (Levin, 2025; Marshall-Chalmers, 2025). As a result, the VHA’s private care option now accounts for roughly 40% of all VA health care appointments, up from 20% a decade ago, with more growth on the horizon (Wu, 2025).
Given these developments, the VHA offers an interesting opportunity to study privatization, which encompasses a range of policy arrangements that differ in how far they shift health care delivery from public to private actors (Savas, 2005; Starr, 1991). At one end, contracting out maintains the government’s financing role while purchasing services from private providers. At the other, full privatization entails a complete transfer of ownership and management to private entities. Community Care, as established under the Choice and MISSION Acts, represents the former (i.e., public financing of privately produced services). However, critics have argued that the steady expansion of contracting out can function as incremental privatization, gradually eroding the capacity of the public system and shifting the institutional center of gravity (as well as funding) toward private provision (Gordon, 2017; Gordon & Early, 2024), a dynamic that has also been documented in the United Kingdom’s National Health Service (Pollock, 2004).
As successive policy changes reshape veterans’ health care, a striking gap remains in what we know about the views of the constituencies policymakers invoke when pursuing them. Policymakers across the political spectrum frame privatization proposals as responses to the preferences of American voters, conservative citizens, and veterans themselves. However, we know little about whether Americans in general, and veterans in particular, support the trajectory of VA privatization that policymakers are pursuing. And do those attitudes differ depending on how far a proposal would go? And do veterans who have directly experienced the VHA or Community Care hold systematically different views from those who have not?
To address these questions, we fielded a large national survey (N = 5,852, including 772 veterans) from January to April 2022 that asked respondents about four distinct privatization proposals ranging from modest expansions of Community Care to full-scale contracting and private insurance. Relying on the literature related to policy feedback, ideology, and elite cue-taking, we find that Americans broadly support limited expansions of Community Care, but that the more far-reaching proposals that most closely resemble current legislative and budgetary trajectories face substantial public resistance, particularly among veterans with direct VHA experience. Conservatives are the most consistent supporters of privatization. Contrary to expectations drawn from simple feedback logic, veterans satisfied with Community Care are not more supportive of broad privatization. Yet, a sizable share of Americans remains undecided on the more expansive proposals, indicating that public opinion in this domain is malleable and that the policy trajectory is not yet settled.
The remainder of the paper proceeds as follows. We next provide a brief overview of the VHA, the access challenges veterans have faced, and efforts to mitigate them, organized around three drivers of policy change including veteran needs, political scandal, and ideological positioning. We then develop our theoretical framework and hypotheses. Subsequent sections present our data and methodology, report our results, and discuss their implications for the ongoing debate over veterans’ health care.
The Veterans Health Administration, Access Challenges, and Privatization
The VHA has evolved substantially since its post-World War II consolidation, and the direction of that evolution has been shaped by three interacting forces, including persistent access gaps rooted in the geographic and clinical heterogeneity of the veteran population, crisis events that have repeatedly restructured the political terrain, and shifting ideological currents around public versus private provision of medical care. First, access gaps and veteran needs have served as the most consistent driver of change. VHA patients have higher rates of serious health conditions than both non-veterans and veterans who do not use VA care, including traumatic brain injury, posttraumatic stress disorder, military sexual trauma, exposure to environmental toxins, and chronic conditions such as diabetes, hypertension, and service-connected cancers (Eibner et al., 2016; Rasmussen & Farmer, 2023). These conditions often require long-term, coordinated treatment informed by familiarity with military service exposures and veteran culture, referred to as military-competent care (Lucier-Greer et al., 2025). Importantly, community providers may lack the training or institutional context to deliver such care (Farmer et al., 2016; Rasmussen & Farmer, 2023). Moreover, a substantial share of enrolled veterans also live in rural areas, often hours from the nearest VA medical center (Hahn et al., 2023; Rasmussen & Farmer, 2023). Although 99% of veterans lived within 40 miles of some VHA facility as of 2015, only 45% were that close to a VHA medical center offering comprehensive services, and only 46% lived within 40 miles of a medical center with full specialty care (Hussey et al., 2016). Others live in urban areas but require specialty services including to treat complex health care needs. At the same time, wait times for primary and specialty care have long been uneven across facilities, reflecting local staffing, case mix, and referral patterns (Feyman et al., 2022). Travel time, wait time, and specialty availability have therefore been ongoing sources of pressure on the system and, correspondingly, on Congress. The VA has responded to these pressures over decades by expanding access to telehealth, mobile clinic, and other policies seeking to improve access (U.S. Department of Veterans Affairs, 2024b).
Scandal has repeatedly supplied the second driver, converting chronic access pressure into acute political crisis. The most prominent was the 2014 Phoenix wait-time scandal, in which whistleblowers alleged that Phoenix VA administrators had maintained off-the-books waitlists to mask delays, and that as many as 40 veterans had died while awaiting care (Duhaney, 2020; Feyman et al., 2022; Mueller, 2020). These scandals open political windows favoring privatization-focused reforms that would face sharper resistance under ordinary conditions, and they shifted the burden of proof on institutional design from reformers to defenders of the VHA. The Veterans Access, Choice, and Accountability Act of 2014 passed bipartisan majorities in Congress and was signed by President Obama within that post-scandal window. The implementation of its 30-day-or-40-mile access standard represented a larger step toward community provision than would likely have been politically feasible in the absence of the Phoenix revelations (Gordon, 2017; Sterling et al., 2022). Similar dynamics have accompanied later episodes involving electronic health records implementation, toxic exposure claims processing, and wait-time reporting practices.
Ideology has acted as the third driver of change and the one that perhaps most clearly explains the ebb and flow of privatization acceptance over time. The United States has long combined public financing of health care with private production, and the VHA, as one of the few fully integrated public delivery systems in the country, has always sat uneasily with that dominant arrangement. Support for privatization has waxed and waned with political administrations, as has the political and policy salience of the VA. Moreover, organized interests have been active on both sides of the debate. As a result, both parties have advanced legislation expanding Community Care, but with distinguishable motivations. For the Obama administration, the Choice Act served primarily as a crisis response to the Phoenix scandal, aimed at expanding access within the existing system while preserving the VHA’s role as the primary provider of veterans’ care (Sterling et al., 2022). The first Trump administration, by contrast, framed the MISSION Act of 2018 and its implementing regulations in more explicitly market-oriented terms, emphasizing consumer choice, competition, and the reduction of government-operated health care (Apaydin et al., 2023; Arnsdorf, 2018; Massarweh et al., 2020; Rieselbach et al., 2019; U.S. Department of Veterans Affairs, 2024a). This framing aligned with the agenda of organizations such as the Concerned Veterans for America, which has advocated for converting the VHA into a government-chartered nonprofit and routing veterans into private provider networks (Arnsdorf, 2018), and has been carried forward legislatively by successive Republican chairs of the congressional veterans’ affairs committees, most recently Representative Mike Bost and Senator Jerry Moran, whose ACCESS Act would codify and expand Community Care eligibility standards (Marshall-Chalmers, 2025). On the other side, most major veterans’ service organizations, including the Veterans of Foreign Wars, the American Legion, and Paralyzed Veterans of America, have consistently opposed full privatization while accepting targeted expansions of Community Care, arguing that the integrated VA model delivers veteran-specific care that private providers cannot replicate (Shulkin, 2023). Subsequent regulatory implementation has continued to expand Community Care’s share of veteran encounters, with VA leadership under successive administrations walking a contested line between operational expansion and rhetorical restraint.
The evidence on whether expanded Community Care has produced its intended effects remains mixed. Veterans accessing Community Care often report improved geographic access and shorter wait times for particular services, but also consistently report care-coordination friction such as inconvenient appointment locations, scheduling delays, communication gaps, and confusing billing (Sayre et al., 2018; Stroupe et al., 2019). Comparative analyses find veterans generally more satisfied with VHA-delivered outpatient care overall, with Community Care showing advantages for specialty services in particular (Vanneman et al., 2020). At the same time, the cost and quality implications of expanding Community Care have become clearer over time. Community Care spending grew from US$7.9 billion in 2014 to US$18.5 billion in 2021, nearly doubling its share of the VHA medical care budget from 12% to 20% over that period (Bass et al., 2021; Rasmussen & Farmer, 2023). For Fiscal Year 2026, appropriations amounted to almost $35 billion (USAspending.gov, 2026). Beyond funding, an analysis of wait times for outpatient specialty care found that by 2018, Community Care wait times were longer than VHA wait times, suggesting that Community Care may not resolve the access problems it was designed to address (Gurewich et al., 2021) while a comparison of outcomes for dually eligible veterans found that VA care reduced 28-day mortality by 46% and spending by 21% relative to private hospitals (Chan et al., 2023). Moreover, only a small proportion of Community Care providers have completed VHA’s military and veteran cultural competency training, raising questions about their ability to fully serve veterans (Rasmussen & Farmer, 2023). However, advocates of expanded Community Care argue that competition, choice, and efficiency gains justify continued expansion (Fulton & Brooks, 2018; Gordon, 2017; Shulkin, 2019). This compares to most major veterans’ service organizations, which take the opposite view, arguing that the integrated VA model delivers care tailored to veterans’ unique needs that cannot be replicated in community settings (Shulkin, 2023). A recent high-level VA advisory panel warned that continued outsourcing threatens to materially erode VA’s direct-care capacity (Gordon & Early, 2024; Kizer et al., 2024), and systematic assessments document meaningful gains in access alongside meaningful losses in coordination and veteran-specific clinical expertise (Farmer et al., 2016; Rasmussen & Farmer, 2023). The result is a policy domain in which the relevant question has shifted from whether Community Care should exist to how far it should go, with the answer depending heavily on how the three drivers align at any given moment.
Theory and Hypotheses
Public Opinion, Voting, and VA Privatization Policy
Public and veteran attitudes toward VA Community Care matter not only as outcomes of the expansion of private provision but also as inputs into future policy. The most direct mechanism by which such attitudes translate into policy is electoral. Members of Congress who set VA authorization and appropriations, and presidents who sign the relevant statutes and direct their implementation, face voters for whom veterans’ health care may be a salient and sympathetic issue (Saad, 2014). The trajectory of VA Community Care expansion illustrates both the bipartisan character of this politics and the role of elite credit-claiming. The Veterans Access, Choice, and Accountability Act was enacted in 2014 under the Obama administration in response to the Phoenix wait-time scandal and represented a substantial expansion of veterans’ access to non-VA providers (Bass et al., 2021; Sterling et al., 2022). The MISSION Act of 2018 further extended that trajectory during the first Trump administration, consolidating multiple Community Care authorities and loosening access standards, and was accompanied by prominent executive credit-claiming (Massarweh et al., 2020; Yoon et al., 2024). Subsequent implementation has continued under administrations of both parties, with sustained advocacy for further expansion from segments of the veterans’ policy community and sustained opposition from most major veterans’ service organizations. The substantive policy question, how much of veterans’ care should be provided outside the VHA, on what terms, and with what safeguards, is therefore a political question whose resolution depends in part on where public and veteran opinion settles.
Although systematic public opinion data on VA privatization specifically are limited, two adjacent bodies of evidence inform expectations. First, Gallup has periodically polled Americans on the public or private provision of health care more generally. The Gallup results show consistent but not overwhelming support for an expanded private role, with substantial partisan cleavage (Jones, 2024). Second, commentary from veterans’ advocates including op-eds has characterized expanded Community Care as a threat to the integrated, veteran-specific model of VA care, emphasizing care-coordination costs and the loss of cultural competence that specialized VA providers develop (Lee, 2023; Williams, 2024). That is, Community Care can shorten travel times and reduce wait times for certain services but introduces fragmentation, quality-measurement gaps, and an additional burden on veterans who must navigate two systems (Farmer et al., 2016; Rasmussen & Farmer, 2023). The hypotheses developed below thus treat public and veteran attitudes as jointly shaped by ideology, elite cues, direct experience with VHA and Community Care, and trust in the institutions responsible for the policy.
Ideology
The private sector has long played an important role in the provision of government services in the United States in general (Smith & Lipsky, 1992). Market competition is at the heart of the privatization argument (Smith & Lipsky, 1992; Van Slyke & Hammonds, 2003) and proponents of privatization often cite alleged government inefficiency as a reason for their efforts (Smith & Lipsky, 1992; Van Slyke & Hammonds, 2003). While privatization serves as an umbrella term for a slew of policies that shift functions from the state to private entities, one of the most common forms is contracting out (Savas, 2005; Seidenstat, 1999; Starr, 1991). Contracting out maintains the public financing function while increasing the reliance on private production of services (Johnston & Romzek, 1999; Light, 1999; Niskanen, 1971). Contracting out fits particularly well with the American understanding of their political system and the realities of the American political environment because it combines public and private means (Crawford & Krahn, 1998; Salamon, 1999).
By and large, efforts to privatize governmental services have been driven by conservatives (Hacker, 2002, 2004; Ikenberry, 1990; Savas, 2002), and privatization serves as a crucial component of the conservative consumer choice movement (Enthoven et al., 2001; Minow, 2002; Smith & Lipsky, 1992), as well as efforts to devolve and decentralize government responsibilities (Kelleher & Yackee, 2004). Privatization also aligns with other conservative goals such as reducing union influence (Van Slyke & Roch, 2004; Wolch, 1990), reducing regulation (Kerwin & Furlong, 2018), and reducing public bureaucracy (Van Slyke & Roch, 2004; Wolch, 1990). Ideologically, privatization also matches conservatives’ distrust of government (Huntington, 1981; Sundquist, 1984), their emphasis on individual choice and rights (Savas, 1982), and their long-standing efforts to reduce the size and scope of the federal state (Niskanen, 2006). These commitments have a particularly direct application to the VHA, which is among the most fully “socialized” components of American medicine: a government-owned, government-operated, integrated delivery system staffed by salaried federal physicians. Conservative elites from Goldwater onward have opposed socialized medicine as a general matter (Arnsdorf, 2018), and the VHA represents its clearest domestic institution. To the extent that ordinary citizens take cues from co-partisan elites and adopt the issue positions associated with their ideological identification (Levendusky, 2009; Slothuus & De Vreese, 2010; Zaller, 1992), we should expect conservatives in the mass public to express greater support for privatization of VHA services than moderates or liberals, even as veterans and their advocates may complicate that alignment in practice.
Feedback Effects
Policy feedback theory holds that policies, once implemented, reshape the political environment in which subsequent policy choices are made, including the attitudes of beneficiaries toward the program itself (Béland, 2010; Béland et al., 2022; Campbell, 2011; Lerman & McCabe, 2017; Mettler & Soss, 2004; Pierson, 1993). Three features of a policy condition the strength and direction of feedback effects: the tangibility of the benefits conveyed (Campbell, 2011; Kelly, 2016; Mettler, 2010), the visibility of those benefits to the beneficiary (Campbell, 2012; Patashnik & Zelizer, 2013), and the traceability of the benefits to the program as their source (Béland et al., 2022; Pierson, 1994). Where benefits are tangible, visible, and traceable, beneficiaries tend to develop supportive attitudes toward the program and to resist changes perceived as threatening to it. These conditions are reinforced by a broader political science literature showing that direct material experience with government programs meaningfully shapes political attitudes (Bechtel & Liesch, 2020; Hansford & Gomez, 2015; Kinder & Kiewiet, 1981). It is important to note that the attachment that veterans develop toward the VHA may not be purely material. Research on veteran identity suggests that for many veterans, their status as veterans is central to their self-concept, and that this identity shapes how they engage with systems of care (Adams et al., 2019; Harada et al., 2002). Veterans with stronger veteran identity are significantly more likely to use VA health care services, even when alternatives are available, and report stronger feelings of belonging within the VA system (Adams et al., 2019; Di Leone et al., 2016). VHA facilities and the veterans’ service organizations that have long complemented them serve not only as sites of clinical care but also as spaces of social connection and shared identity, reinforcing a sense of earned entitlement rooted in military service and the government’s reciprocal obligation to provide for those who served (Burtin, 2020). This normative dimension means that proposals to restructure or replace the VHA may be perceived not merely as a change in care delivery but as a breach of an institutional and societal commitment. Notably, this dynamic creates a potential tension with ideology as veterans as a population lean more conservative than the general public. This suggests that they would tend to favor privatization. Yet, their institutional attachment to the VHA and the identity-based bonds it sustains may pull in the opposite direction. VHA health care meets all three conditions to an unusually high degree. Benefits are tangible (medical care), visible (direct provision by identifiable VA clinicians at identifiable VA facilities), and highly traceable to the program and, by extension, to the government that funds it. We therefore expect policy feedback to operate strongly among veterans who use the VHA, generating institutional attachment and resistance to proposals perceived as threatening the existing model.
At the same time, feedback effects operate primarily to shape attitudes toward the program itself rather than to produce reflexive opposition to any and all related reforms. As a result, proposals that expand options without displacing the existing program may not trigger the same defensive response. With this framework, and given that most veterans have historically been supportive of the VHA as an institution (Shulkin, 2023), we expect:
The strength of policy feedback effects should vary systematically with direct exposure to the program. Veterans who have recently received care through the VHA have had the most concrete opportunity for the program’s benefits to shape their attitudes toward the institution. They received tangible medical care, they experienced VA clinicians and facilities, and they can trace those benefits to the government program that funded them. This is the mechanism the feedback literature identifies as operating most reliably, that is, through direct, material, identifiable benefits delivered by the program itself (Campbell, 2011; Mettler, 2010). Veterans with recent VHA care experience should therefore have developed the kind of institutional attachment that predicts resistance to policy changes perceived as threatening the existing model. On the other hand, veterans who have recently received care outside the VHA occupy the mirror position. Their recent care experience has been mediated by private providers, with the VA’s role as financier rendered comparatively less visible than the private clinician providing the care. If feedback effects operate symmetrically, exposure to Community Care should generate attitudes somewhat more favorable to continued or expanded reliance on private provision, and correspondingly less protective of the existing VHA model.
We note two important caveats to this framing. First, care receipt is an imperfect proxy for experience. The set of veterans who received VHA care in the past year includes both those who found the system effective and those who navigated it despite its well-documented access and coordination difficulties (Sayre et al., 2018; Stroupe et al., 2019). The same ambiguity applies in reverse to veterans who received Community Care as some encountered the fragmentation the literature documents (Farmer et al., 2016; Rasmussen & Farmer, 2023), while others did not. Second, recent exposure to one system does not preclude past exposure to the other. Many veterans have experience with both, and we cannot fully separate these populations with our cross-sectional data. Care receipt nonetheless remains the most directly observable indicator of sustained program exposure available to us, and the dichotomy between VHA and community-care receipt captures the most policy-relevant distinction. Nonetheless, we expect:
Satisfaction with that care provides a more demanding test of the feedback mechanism and one that more closely tracks the theoretical specification in the literature. Campbell (2011) and Mettler (2010) both emphasize that positive experience with a program is translated into durable program support more reliably than neutral or negative experience. Dissatisfying encounters can, on the margin, produce the opposite effect, even for beneficiaries of ostensibly generous programs. Satisfaction thus isolates the subset of recipients for whom the feedback mechanism should operate most strongly. At the same time, two limits to this expectation bear noting. A positive experience with a specific instance of Community Care may not generalize into support for broad privatization of the VHA as a system, as veterans whose community-care experience has been positive may still value the integrated VHA model for the complex, longitudinal, service-connected care they receive there. Conversely, veterans satisfied with VHA care may still recognize that Community Care serves as an important complement for specific access gaps without preferring it as a wholesale replacement. We expect satisfaction-conditioned effects to be directionally consistent but potentially more muted than a simple feedback logic would predict:
The Role of President Trump
Elite positioning provides another potential driver of mass attitudes toward VHA privatization, distinct from underlying ideological commitments. The first Trump administration supported privatization across a range of domains and treated reducing the size and scope of government as a central organizing principle (Gordon, 2017; Konnoth, 2021). On VHA policy specifically, President Trump has been an unusually vocal advocate for expanded private involvement in veterans’ health care across both of his presidential terms (Arnsdorf, 2018; Lawrence, 2019; Trump, 2021; Williams, 2024). Although the statutory expansion of Community Care began in 2014 with the Choice Act under President Obama, the MISSION Act of 2018 was signed by President Trump, and the implementing regulations issued during his first administration were notably pro-privatization (Apaydin et al., 2023; Arnsdorf, 2018). President Trump also has repeatedly claimed public credit for this trajectory and has made expanded choice for veterans a recurring campaign theme, including during the 2024 presidential campaign (Kheel, 2024; Trump, 2024).
If voters take cues from co-partisan elites on issues that elites have made salient, and if those cues translate into policy preferences (Levendusky, 2009; Slothuus & De Vreese, 2010; Zaller, 1992), we would expect Trump voters to be more supportive of VHA privatization than non-Trump voters, above and beyond any effect of ideology. Whether an elite cue of this intensity actually moves voter-level preferences on a relatively technical and bipartisan policy question is, however, an empirical question. A positive association would indicate that rhetorical credit-claiming and voter preferences are aligned; a null result would suggest that, despite the intensity of elite positioning, VA privatization has not become an issue on which voters map elite cues onto their own preferences.
Data and Methods
Data
To assess public attitudes about privatization of VHA services in general and attitudes of veterans in particular, we fielded a large national survey using Lucid from January to April of 2022. Lucid relies on quota sampling to achieve nationally representative samples that closely mirror national benchmarks on a variety of demographic factors such as age, race, gender, education, and income. Lucid is a sample aggregator that brokers respondents across a large network of third-party supplier panels. Supplier panelists are recruited through a mix of channels including email invitations, in-app banners, push notifications, messaging on community sites, and loyalty program integrations and are typically compensated with small monetary or points-based incentives calibrated to expected survey length. Lucid’s data has been vetted and validated. Moreover, recent comparative work across nine contemporary online panels finds that Lucid performs well compared to alternative vendors on representativeness and attentiveness once standard quality controls are applied (Coppock & McClellan, 2019; Stagnaro et al., 2024). It has been frequently used in survey research related to health and social policy.
Our invitation was distributed across the Lucid supplier network with demographic quotas applied on age, gender, race and ethnicity, education, and income to approximate U.S. adult population benchmarks. Overall, 53,517 U.S. adults opted into the survey. Consistent with standard practice for online panel research, we embedded multiple attention checks to screen out inattentive or low-effort respondents (Ternovski et al., 2022). As a result, 16,461 respondents completed it (31%). Of the 16,461 respondents, 5,852 respondents received questions related to the privatization of the VHA, while the remainder were asked questions about a different, unrelated topic (see Online Appendices 1–3). Unweighted results closely matched population benchmarks and we further improved fit by post-stratification weighting for gender, education, race, age, and income to further approximate the U.S. population.
Dependent Variables
To assess public attitudes about different degrees of privatization of VHA services, we queried respondents about four distinct policy proposals. Before exposing respondents to our questions, we briefly introduced them to the topic. Subsequently, we asked about policy options that (a) allow veterans to seek care outside the VHA if access within the VHA is too limited, (b) allow veterans to seek care outside the VHA without any restrictions, (c) fully contracting out VHA services with private medical providers, and (d) governmental purchase of insurance for veterans from private insurers (see Online Appendix 4 for details). Each proposal offered respondents a 5-point scale from strongly agree to strongly disagree with a neutral midpoint option. These policy proposals offer different degrees of privatization that maintain the public provision of care, ranging from the existing approaches focused on contracting out to more expansive proposals that would solely rely on the federal government to finance such services.
Independent Variables
Several of our key independent variables are related to veteran status and veterans’ experience with health care. To identify veterans, we asked respondents whether they had “ever served on active duty in the U.S. Armed Forces, military Reserves, or National Guard?,” a standard question used for this purpose. We subsequently asked veterans whether they had received any medical care “provided or paid for by the VA” over the last year or so. For those who responded that they had received care, we then asked them about the amount of care they received “directly from the VA in a VHA facility?” and offered them a standard 5-point scale from “none at all” to “a great deal.” We also asked veterans about “how much of your care did you receive through private medical providers but paid for by the VA” and offered them the same scale. We dichotomized the answers into whether any care was received via both options because of the low number of responses in certain categories. In both cases, we also asked veterans about their degree of satisfaction with the care they received. The 5-point scale we offered ranged from “extremely dissatisfied” to “extremely satisfied” with a neutral midpoint. In our analyses below, we combine the respective “extremely” and “somewhat” options and generate a 3-point scale because of the low number of responses in some categories.
A second set of variables captured the political and ideological leanings of respondents. We included indicators for both liberals and conservatives in our models. We combined both “extreme liberals” and “liberals” in the former and both “extreme conservatives” and “conservatives” in the latter as well as a binary indicator for respondents who had voted for President Trump in the 2020 elections.
Finally, we included standard demographic controls for age, income (up to US$14,999; US$15,000 to US$24,999; US$25,000 to US$34,999; US$35,000 to US$49,999; US$50,000 to US$74,999; U$75,000 and more), gender, education (High School Graduation or less, Some College, or College Graduation, with graduate education as the reference), health status (a 5-point scale from “poor” to “excellent”), race and ethnicity (Non-Hispanic White, Non-Hispanic Black, Non-Hispanic Asian, Hispanic, Other Race/Ethnicity with Non-Hispanic Whites serving as the reference category), rural residence (rural, suburban, urban, with suburban as the reference), insurance status (employer-sponsored insurance [ESI], Medicare, Medicaid, individual coverage, other coverage, or uninsured with ESI as the reference). We also control for respondents’ trust in Congress (4-point scale from “no confidence at all” to “a great deal”) and trust in the president (4-point scale from “no confidence at all” to “a great deal”).
Methods
To assess public attitudes about the various privatization options for the VHA, we estimated a series of weighted least-squares models. Weighted least squares models are substantially easier to interpret than ordered models, which showed analogous results (omitted). For all four policies, we estimated three models using all respondents as well as an additional four models focused solely on veterans. The three models among all respondents utilize different indicators related to veterans to assess their attitudes toward VHA privatization. Model 1 simply contains an indicator for veteran status, whereas Model 2 contains this indicator as well as an indicator for whether or not the individual received any care from the VHA in the past year. Model 3 then contained the veteran indicator as well as indicators for whether respondents received care directly from the VHA or via private providers. We estimated analogous models for models 2 and 3 for veterans only, as well (Models 4 and 5). Finally, we estimated independent models for veterans and included the aforementioned measure of satisfaction for those who received direct VHA care (Model 6) as well as private care (Model 7). We conducted standard measures to assess model assumptions and fit. We considered a p-value lower than .05 as statistically significant throughout our analyses.
Results
Descriptive Overview of Support for the Four Policies
What does the American public think about the four policy proposals seeking to privatize the VHA (Figure 1)? Overall, Americans are broadly supportive of existing and more limited efforts to privatize the VHA. 67.3% (95% CI [65.6%, 68.9%]) strongly agreed and 21.1% (95% CI [19.8%, 22.6%]) somewhat agreed with the proposal to allow veterans to seek care outside the VHA if access within the VHA is too limited. This compared to 1.6% (95% CI [1.2%, 2.1%] respondents who strongly disagreed with the proposal and 1.8% (95% CI [1.4%, 2.3%]) somewhat disagreed with the remaining 8.3% (95% CI [7.3%, 9.3%]) being undecided. Respondents also supported the second proposal to allow veterans to seek care outside the VHA without any restrictions. Nonetheless, 56.6% (95% CI [54.9%, 58.3%]) strongly agreed and 25.8% (95% CI [24.4%, 27.3%]) somewhat agreed with the proposal, while 10.9% (95% CI [9.9%, 12.0%]) were undecided. This left 1.5% (95% CI [1.1%, 1.9%]) of respondents strongly disagreed with the proposal and 5.2% (95% CI [4.5%, 6.1%]) somewhat disagreed with it.
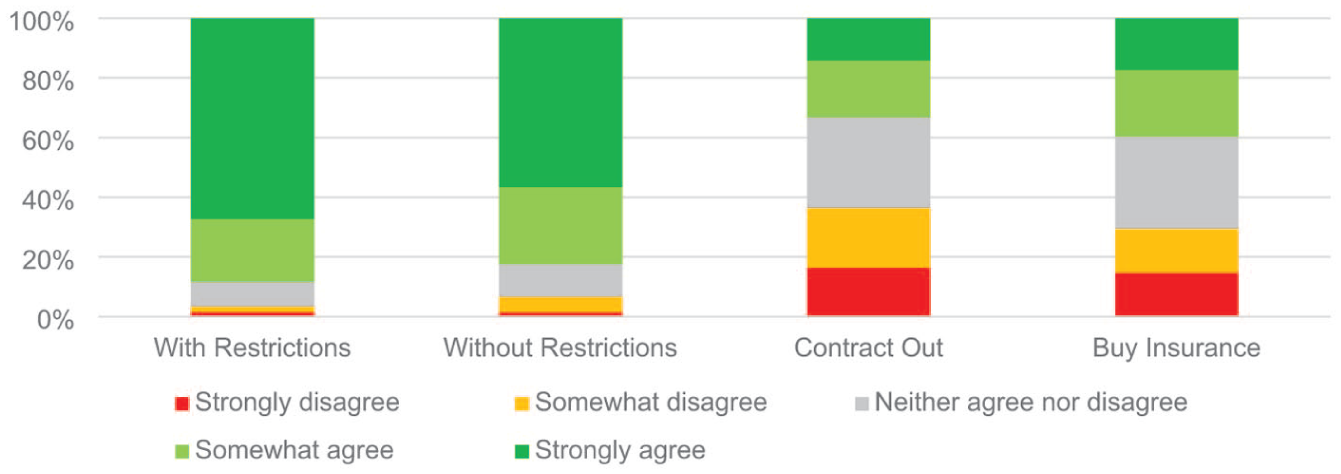
Distribution of support for the various privatization proposal for veterans health administration.
Public attitudes toward the more expansive privatization proposals were more muted with respondents slightly favoring the governmental purchase of insurance for veterans from private insurers over fully contracting out VHA services with private medical providers. For the former, only 14.7% strongly agreed (95% CI [13.6%, 15.9%]) and 14.7% somewhat agreed (95% CI [13.6, 16.0]) with the proposal, while 22.2% (95% CI [20.9%, 23.7%]) somewhat disagreed and 17.4% (95% CI [16.1%, 18.8%]) strongly disagreed. At the same time, 3 out of 10 respondents (30.9%, 95% CI [29.4%, 32.5%]) neither agreed nor disagreed. Full-scale contracting was supported strongly by 16.4% (95% CI [15.2%, 17.7%]) and somewhat by 20.0% (95% CI [18.7%, 21.4%]) of respondents. This compared to 19.0% (95% CI [17.7%, 20.4%]) who somewhat disagreed and an additional 14.2% (95% CI [13.0%, 15.5%]) who strongly disagreed; 30.3% (95% CI [28.8%, 31.9%]) were neutral.
Correlates of Support for the Four Privatization Policies
Private Care With Restrictions
We found no evidence that veterans differed from non-veterans with regard to the proposal focused on private care with certain restrictions (Table 1), whether defined by veteran status alone (Table 1, Model 1), by receipt of VA-paid care in the past year (Table 1, Model 2), or by the site of that care (Table 1, Model 3). As a result, H2, H3a, and H3b were not supported. In the models estimated among veterans only, neither care receipt nor satisfaction with care reached conventional levels of significance, and H4a and H4b were likewise not supported. However, conservatives were more supportive of this limited privatization proposal than moderates across all three all-respondent specifications (0.154, p < .001), supporting H1. Self-identified liberals were also somewhat more supportive than moderates in two of the three models (0.075, p < .050), indicating that support for this modest expansion of choice extends across the ideological spectrum. At the same time, Trump voters were slightly more supportive than non-Trump voters (0.091, p < .025), providing limited support for H5.
Regression Results for Attitudes About Privatized Care With Restrictions.
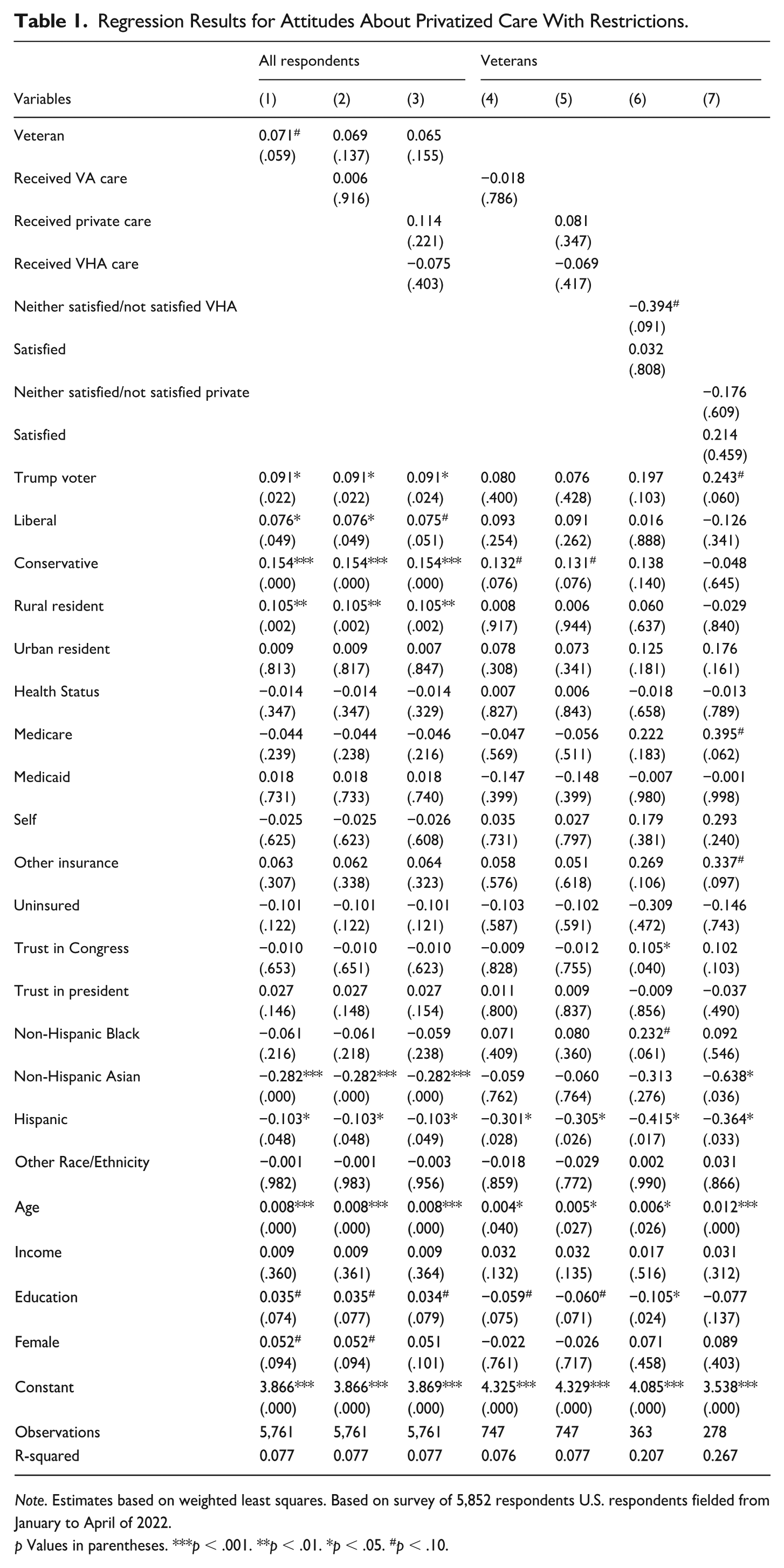
Note. Estimates based on weighted least squares. Based on survey of 5,852 respondents U.S. respondents fielded from January to April of 2022.
p Values in parentheses. ***p < .001. **p < .01. *p < .05. #p < .10.
Private Care Without Restrictions
Our findings from the first policy were largely a mirror for the second policy, private care without restrictions (Table 2). Across all respondent specifications, veterans did not differ systematically from non-veterans, and neither care receipt nor site of care reached significance. Hence, H2, H3a, and H3b were again not supported. However, veterans who received VHA care and were satisfied with it were less supportive of unrestricted private care than other veterans (–0.375, p = .030), supporting H4a. Unexpectedly, veterans who received Community Care and were satisfied with it were also less supportive of unrestricted privatization (–0.671, p < .001). H4b was therefore not supported, and the direction of the effect ran contrary to our expectations. Conservatives were again more supportive of unrestricted privatization than moderates across all respondent models (0.148 to 0.149, p < .002), supporting H1. However, H5, which focused on Trump voters, was not supported.
Regression Results for Attitudes About Privatized Care Without Restrictions.
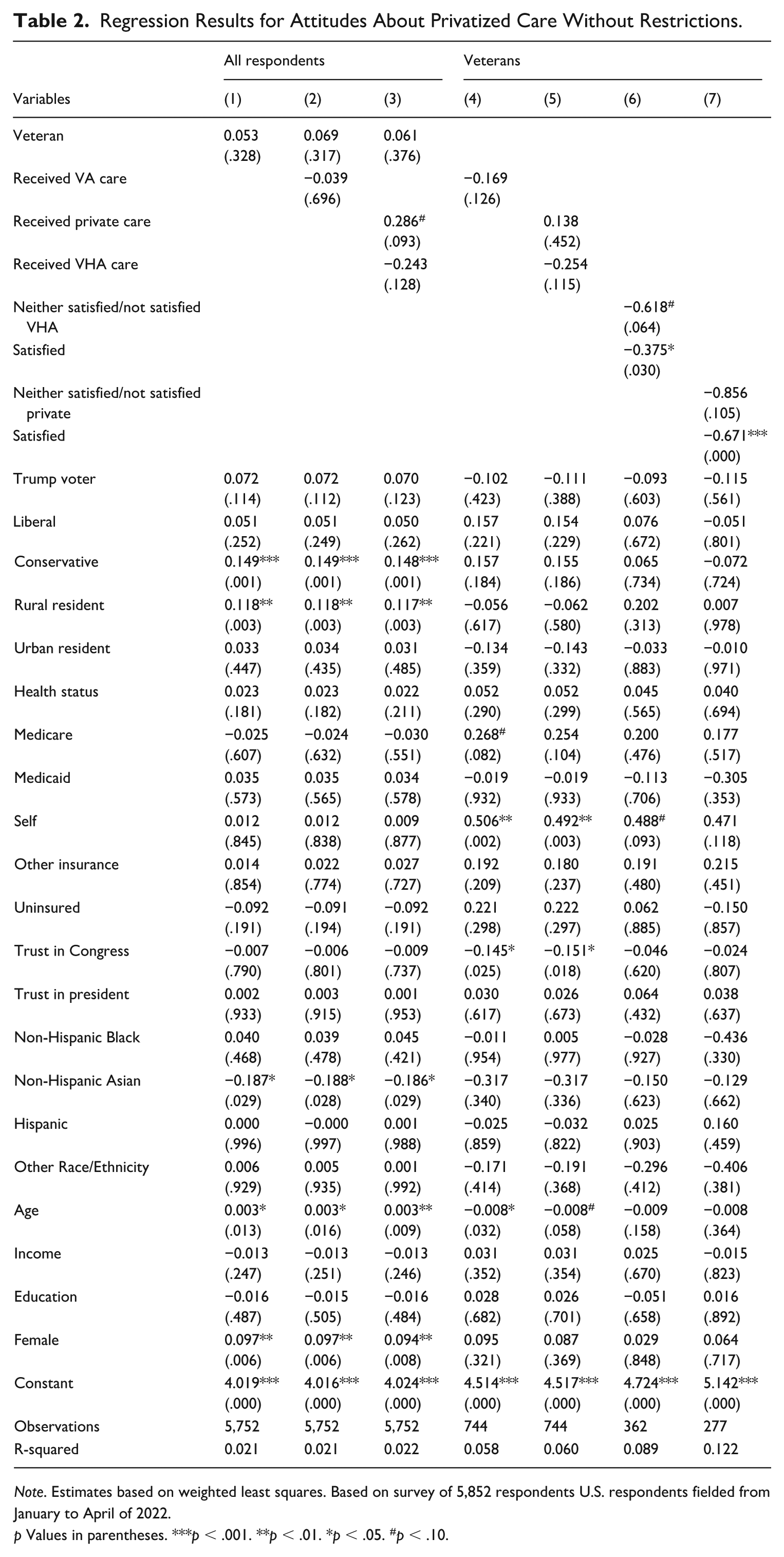
Note. Estimates based on weighted least squares. Based on survey of 5,852 respondents U.S. respondents fielded from January to April of 2022.
p Values in parentheses. ***p < .001. **p < .01. *p < .05. #p < .10.
Full Privatization
The third policy, fully contracting out VHA services to private medical providers, represents a substantially more far-reaching privatization proposal than the first two (Table 3). In the all-respondent models, veterans did not differ from non-veterans (Table 3, Model 1). H2 thus was not supported. When we disaggregate veterans by site of care received, however, the patterns predicted by policy feedback theory come into view. Veterans who received care directly from the VHA were substantially less supportive of full privatization than other respondents (–0.435, p = .029), supporting H3a. However, veterans who received Community Care were substantially more supportive (0.767, p < .001), supporting H3b. Moreover, conservatives were more supportive of full privatization than moderates across all specifications (0.153 to 0.156, p < .012), supporting H1, while H5, which focused on Trump voters, was not supported. In the veterans-only models, the site-of-care effects observed above did not separate veterans from one another once the sample was restricted to veterans alone, and the satisfaction-conditioned specifications do not reach significance. The corresponding hypotheses H4a and H4b were therefore not separately supported. Conservative veterans were more supportive of full privatization than non-conservative veterans in two of the three specifications (0.321, p = .032; 0.350, p = .041), indicating that the conservative effect documented in the all-respondent models operates within the veteran population as well.
Regression Results for Attitudes About Full Privatization.
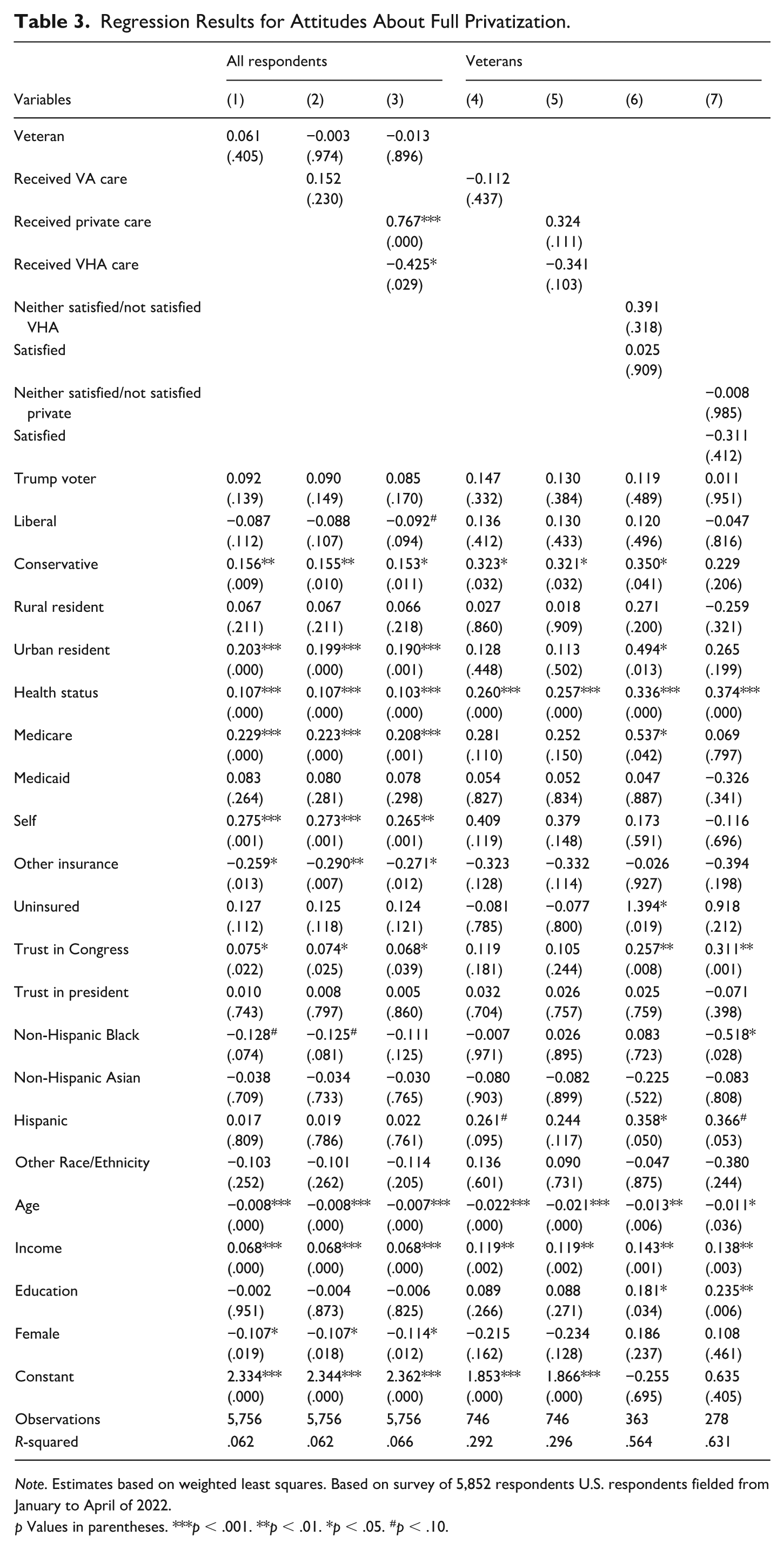
Note. Estimates based on weighted least squares. Based on survey of 5,852 respondents U.S. respondents fielded from January to April of 2022.
p Values in parentheses. ***p < .001. **p < .01. *p < .05. #p < .10.
Health Insurance Coverage
Finally, for the policy replacing VHA direct provision with government-purchased private insurance coverage for veterans, correlates of support generally echoed the full-privatization findings (Table 4). As with full privatization, the site-of-care findings emerge clearly in the all-respondent models. Veterans who received Community Care were more supportive of privately-purchased insurance than other respondents (0.864, p < .001), supporting H3b while veterans who received VHA care were less supportive (–0.565, p = .011), supporting H3a. The satisfaction-conditioned specifications in the veterans-only models did not reach significance, and H4a and H4b were therefore not separately supported. Moreover, veterans did not differ from non-veterans indicating that H2 was not supported. With regard to ideology, we found no effect of conservative identification on support for private insurance purchase. H1 was thus not supported in the all-respondent models. However, liberals were less supportive than moderates (–0.116 to –0.111, p < .047). In the veterans-only specifications, however, conservative veterans were more supportive of private insurance purchase than non-conservative veterans in two of three models (0.363, p = .032; 0.358, p = .034). Finally, H5 was not supported as Trump voters did not differ systematically from other respondents.
Regression Results for Attitudes About via Health Insurance Coverage.
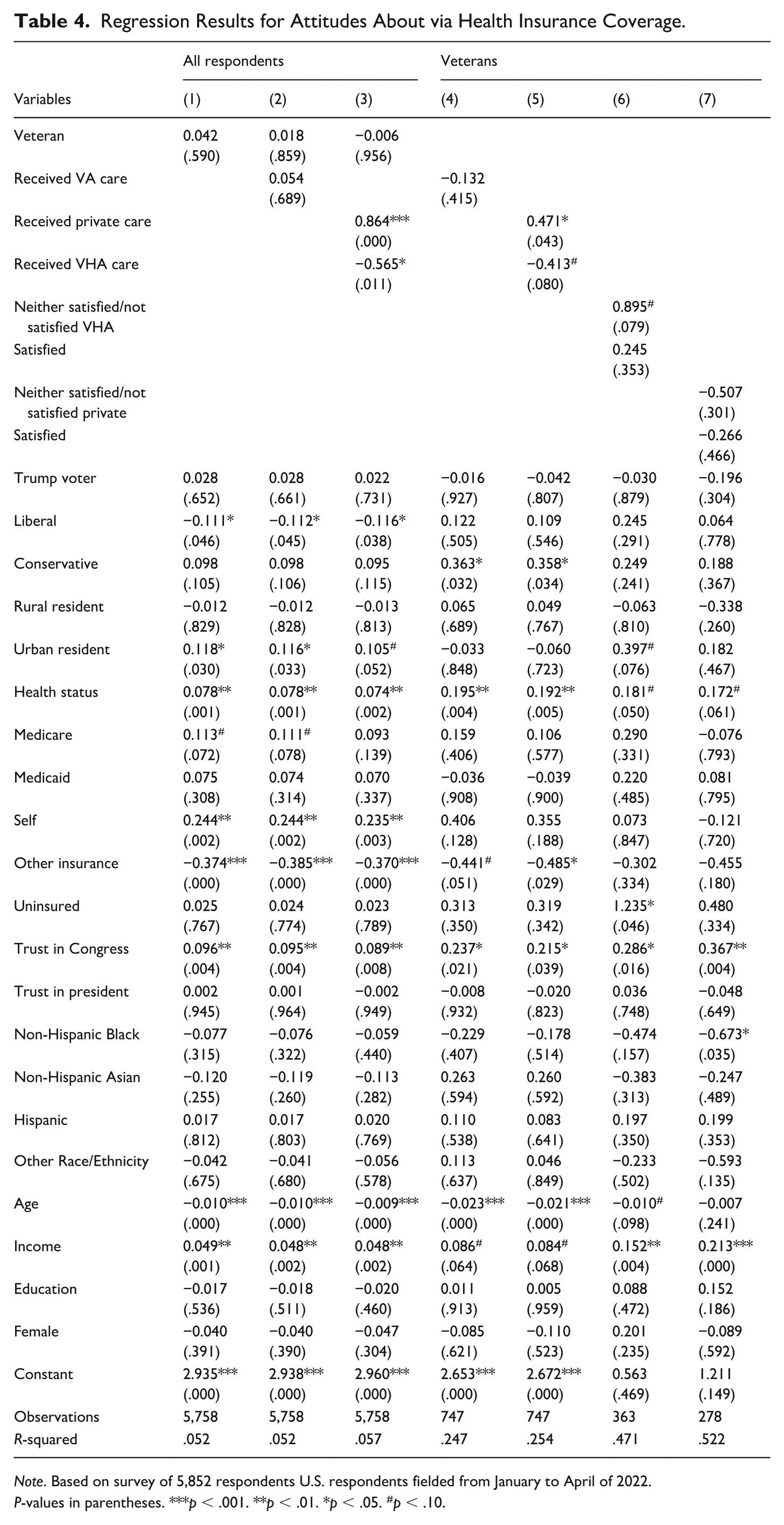
Note. Based on survey of 5,852 respondents U.S. respondents fielded from January to April of 2022.
P-values in parentheses. ***p < .001. **p < .01. *p < .05. #p < .10.
Discussion
Our analysis of public attitudes about VHA privatization proposals yielded a consistent set of findings. Americans broadly support limited expansions of Community Care policies. Support dropped substantially for the two more far-reaching proposals, with only about a third of respondents supporting full contracting or privately-purchased insurance and roughly 30% remaining undecided on each. Our analyses also indicate that conservatives were generally more supportive of privatization (H1) with the exception of the insurance-purchase proposal, where the conservative effect disappears in the all-respondent models but reappears among veterans. We found no support for our expectation that veterans in the aggregate would be less supportive of privatization than non-veterans (H2). The more nuanced expectations had mixed findings. That is, our hypothesis that veterans’ attitudes would vary by site of recent care (H3a and H3b) was not supported for the two more limited proposals but was strongly supported for the two more far-reaching proposals. However, the hypotheses focused on satisfaction with care (H4a and H4b) only found limited support. As such, H4a was only supported for the unrestricted-private-care proposal. H4b, that satisfaction with Community Care would amplify support for privatization, was not supported, and the direction of the effect ran contrary to our expectations. Finally, H5, that Trump voters would be more supportive of privatization above and beyond ideology, was supported only for the most modest of the four proposals.
Our findings have several broader implications. The pattern we identified related to the experience of veterans indicates that policy feedback operates most strongly when the proposal under consideration would materially displace the existing program rather than merely expand options around it. Veterans with recent VHA care were no different from non-veterans when asked about limited expansions of Community Care but were substantially less supportive of full contracting and insurance purchase (Campbell, 2011, 2012; Mettler, 2010). The mirror finding among veterans who received Community Care is similarly consistent with symmetric feedback logic, as direct experience with private provision may have shifted attitudes in the direction of continued reliance on it.
However, the finding that veterans who received Community Care and were satisfied with it were not more supportive of unrestricted privatization but less so ran in the opposite direction from the hypothesized effect. The most plausible interpretation is that satisfaction with a specific community-care encounter does not generalize into support for systemic privatization of the VHA. This may be because veterans navigating both care systems encounter frustrating care-coordination costs (Farmer et al., 2016; Rasmussen & Farmer, 2023; Sayre et al., 2018). A positive experience with a private provider may coexist with awareness that building an entire care system on that model would be costly. This reading is consistent with the persistent position of major veterans’ service organizations, which generally support targeted expansions of Community Care while opposing full privatization (Shulkin, 2023). It also suggests that the classical policy feedback literature’s emphasis on beneficiary experience as a source of program support needs to be qualified. That is, experience with individual encounters may not be equivalent to preference for systemic change.
The findings related to the fourth policy, replacing VHA direct provision with government-purchased private insurance coverage, are interesting because they produced an ideological pattern that differs instructively from the other three. Conservative identification was not associated with support in the all-respondent models, while conservative veterans showed a clear positive association. One plausible interpretation is that private insurance purchase retains substantial government financing rather than shifting genuinely toward market provision. For conservatives in the general public, the proposal may read as a reshuffling of federal health care expenditure rather than as a reduction in the government’s role. For veterans who might actually use the resulting coverage, the proposal’s choice and portability dimensions may dominate the financing dimension.
Finally, our findings suggest a public opinion environment in which limited expansions of Community Care find broad support, but more far-reaching proposals face substantial resistance, particularly among the veterans with direct VHA experience who are most directly affected. Ideology is the most consistent correlate of such support. However, the null finding for Trump voters, despite President Trump’s unusually vocal elite positioning on VA privatization, suggests that elite credit-claiming on this issue has not translated into a measurable voter-level signal. For policymakers, these findings imply that an aggressive push toward full privatization would likely face public opposition in the current opinion environment, while continued incremental expansion of Community Care would likely encounter little public resistance. The substantial share of undecided respondents on the more expansive proposals, however, indicates that current opinion is malleable.
Our study has several limitations. First, our data are cross-sectional and drawn from an online, non-probability panel. Although the Lucid panel has been extensively validated for social science research (Coppock & McClellan, 2019; Stagnaro et al., 2024) and we have applied standard quality controls and post-stratification weighting, cross-sectional data cannot establish causal relationships between care experience and attitudes. Second, our measures of care receipt and satisfaction capture recent experience but do not separate respondents who have used both VHA and Community Care from those who have used only one. In as far as veterans have experience with both systems, we cannot fully disentangle these populations. In addition, our data do not allow us to distinguish veterans by service era, and attitudes toward the VHA may differ meaningfully across generational cohorts. Vietnam-era veterans, who came of age alongside the VHA’s postwar expansion and comprise a large share of current VHA patients, may hold stronger institutional attachments than post-9/11 veterans, whose military experience coincided with the expansion of Community Care and who may have different expectations of and experiences with the system (Eibner et al., 2016). Future research should examine these nuances. Fourth, our survey was fielded in early 2022, before the PACT Act, the Elizabeth Dole Act, and the Veterans’ ACCESS Act reshaped Community Care eligibility and utilization. Attitudes measured today, in a materially different policy environment, could differ from those we report. Finally, our survey asked respondents about four privatization proposals described in brief summary form. Providing more detailed information about costs, care-coordination implications, or workforce effects might materially alter responses.
Conclusion
The provision of care to veterans will continue to be a public policy issue that requires ongoing attention and substantial commitment of resources. While providing some private-sector choice has become widely accepted, fully privatizing the VHA remains controversial because of concerns about fragmenting and undermining a health system tailored to veterans’ specific needs (Lee, 2023; Williams, 2024). Americans may continue to hesitate to support full-scale privatization out of concerns about costs (Lawrence, 2019), strain on the private health care system (Rose & Wagner, 2025), protection of veterans’ health, or the broader consequences of privatization as a policy form.
Developments since this survey was fielded have given these questions additional urgency. The second Trump administration has accelerated the pace of Community Care expansion along several tracks simultaneously. The Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act further expanded private care options for veterans. Other legislation currently in Congress would loosen eligibility thresholds for Community Care and establish a 3-year pilot program allowing veterans to access private mental health and substance use services without prior VA referral or preauthorization (Marshall-Chalmers, 2025). Moreover, the Trump administration’s fiscal 2026 VA budget proposal directs a majority of new medical care funding to Community Care rather than to direct VA provision (Levin, 2025). Staff reductions at VA facilities have proceeded in parallel. Community Care now accounts for roughly 40% of all VA health care appointments, up from 22% in 2014 (Wu, 2025).
These developments test the political calculus our findings describe. Our results suggest that the current trajectory with the incremental expansion of Community Care is politically sustainable, while more aggressive restructuring of the integrated VA model may not necessarily be, at least under current opinion conditions. Whether the accelerated expansion now underway moves opinion toward acceptance of more far-reaching change, or activates the resistance we document among veterans with direct VHA experience, is an open empirical question with substantial consequences for the future of the nation’s largest integrated public delivery system.
Supplemental Material
sj-docx-1-afs-10.1177_0095327X261459116 – Supplemental material for “To Care for Him Who Shall Have Borne the Battle”: Public Attitudes About Privatizing Veterans’ Health Care in the U.S
Supplemental material, sj-docx-1-afs-10.1177_0095327X261459116 for “To Care for Him Who Shall Have Borne the Battle”: Public Attitudes About Privatizing Veterans’ Health Care in the U.S by Anisha Aggarwal, Siddharth Srivastava and Simon F. Haeder in Armed Forces & Society
Footnotes
Authors Note
The phrase is drawn from Abraham Lincoln’s Second Inaugural Address (Lincoln, 1865) and serves as the official motto of the ![]() .
.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by the Robert Wood Johnson Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.