
Abstract
The story of medical marijuana implementation in the states provides researchers an opportunity for a unique study of the relationship between political culture and policy implementation. This paper tests the relationship between the utilization of medical marijuana at the county level, estimated supply, institutional design, and the political culture of each jurisdiction. The paper draws on the Institutional Analysis and Design framework and social construction theory. This model supports the conclusion that political culture is a significant part of the policy implementation story.
Introduction
The present decade has seen a significant change in the direction of drug policy in the United States. The 40th anniversary of the “declaration” of the War on Drugs in 2011 precipitated a national discussion of drug policy at the same time that Colorado and Washington became the first states to legalize marijuana and other states moved toward becoming new medical marijuana states. Medical marijuana has long been a complex subset of the overall drug policy issue. The political struggle between competing interest groups—public health officials, law enforcement, patients’ advocates—and the diversity of implementation strategies make medical marijuana an interesting subject area for a variety of public policy and public administration concepts.
This paper tests the concept of political culture as a proxy for social construction and the relationship that public attitudes have on the implementation of medical marijuana laws. Political culture in this context refers to the social standing of medical marijuana users within the wider community as measured by voting behavior. While the relationship between ideology, voter attitudes, and voting behavior is frequently studied in political science, the connection between social construction, voting behavior, and policy implementation is less well-defined in public administration. Consequently, the theoretical importance of social construction as a policy implementation problem is defined and discussed in the section “Theoretical Foundations.”
After this, I present and test a model for measuring social construction by using presidential voting as a proxy measure of political culture. I explain and elaborate the basis for this proxy measure using existing literature that connects values and voting behavior. I conclude that political culture, as an attribute of the wider target community and not merely the ideology of political elites and administrators, is an essential factor in predicting the success of policy outcomes.
Theoretical Foundations
In general, the medical marijuana debate has been driven by the debate over the palliative benefits of tetrahydrocannabinol (THC), the psychoactive substance in marijuana. A growing body of research demonstrates that THC has genuine benefits for alleviating glaucoma and neuropathy, among, perhaps, other chronic ailments (Ellis et al., 2008; Nurmikko et al., 2007). Advocates support the use of the drug for pain relief and appetite stimulation for patients with, among others, HIV/AIDS, cancer, Crohn’s disease, cachexia, and severe and consistent pain and muscle spasms (MPP, 2011). One drug made from THC, Sativex, has recently (as of the time of this writing) been approved and released onto the market in the United Kingdom, Spain, and Denmark (PBR Staff Writer, 2011). Opponents counter with competing evidence that highlights the negative side effects of ingestion through inhalation and of marijuana use in general (National Institutes of Health, 2011).
Despite this medical debate, medical marijuana has not been rigorously studied as a complex policy implementation problem. This neglect is unfortunate given the level of conflict, the ongoing variation in implementation strategies, and the simple fact that drug policy is a social issue that has been highly divisive for at least half a century. In addition to the many policy dimensions involved concerning the design of medical marijuana laws, one important prospect for studying this important issue is the role that cultural norms play in the implementation of these laws.
Those who have studied the design and implementation of governance regimes have sought to more accurately understand the processes by which cooperation and negotiation are achieved to produce consensus-based rules (Ostrom, 2007). The Institutional Analysis and Design (IAD) framework offers a useful conceptual tool for shaping a study of this particular aspect of policy implementation. The research used to develop the IAD has organized and developed empirical findings on the design and management of collective governance regimes overseeing a wide range of collective action problems. In each of these governance problems, the attributes of the wider community—usually operationalized as norms, traditions, and values of a given political community—are key variables that can intervene between the design of institutions and the achievement of a given set of intended policy outcomes (Ostrom, 2005).
Other public administration research offers important organizational context for the role of norms and values in policy implementation. It has become more common to use culture, norms, values, and social capital as explanations for variations in the management of policies that have been constructed at a “higher” policy level (Putnam & Feldman, 2003; Riccucci, 2005). This type of research demonstrates that the meaning of political symbols and rhetoric is more critical to policy outcomes at the “bottom–up” level of ordinary citizens, local leaders, and county officials than the rhetoric of governors or presidents (Elmore, 1979-1980). Some studies have begun to provide effective measurements of norms and values in public management contexts (e.g., May & Winter, 2007, 2009).
In the context of medical marijuana implementation, the formal characteristics of state medical marijuana regimes are worthy of study in their own right. However, this paper argues that the variation in the (informal) attributes of the political communities that have adopted and implemented medical marijuana laws is at least equally significant to the achievement of the policy goal of increasing palliative care for chronic conditions. The following section provides a theoretical basis for my hypothesis that the negative or positive construction of medical marijuana users in a given political community has a statistically significant relationship to the rate of registered users in that community.
Social construction theory (e.g., Ingram, Schneider, & Deleon, 2007; A. Schneider & Ingram, 1993; A. L. Schneider & Ingram, 1997) is a powerful tool for explaining the connection between informal “attributes of the wider community” and the successful achievement of policy outcomes in the context of divisive social issues in well-established political communities. The theoretical connection rests in the wider society’s larger views of the target population of a given policy. Drug policy has been driven by the construction of roles that have deeply emotional and culturally significant meanings. One consistent set of drug policy roles asserts that “America’s youth” must be protected from “users” and “dealers” (Whitford & Yates, 2009). Despite the significant overlap in these demographics (i.e., many a hapless “youth” is actually a “user” or “dealer”), policy has been shaped around the mental images relating to these groups and the perceived social standing of these groups within society (Houston & Richardson, 2004). While other community “attributes,” such as norms about rule compliance, honoring contracts, and the like may matter more in resource-governance regimes, my assumption for this paper is that constructions of social roles are the most critical community “attribute” in the design and implementation of social policies.
The medical marijuana issue has been motivated by an attempt to build a political space for the severely ill that mitigates the otherwise negative stigma surrounding marijuana use among the general public. In other words, the qualifier “medical” offers a socially accepted, generally positive concept that communicates that many marijuana users self-medicate due to legitimate medical concerns and legitimate medical benefits. This phenomenon was documented early in the medical marijuana movement by a meta-analysis of public opinion surveys published in the Journal of the American Medical Association (Blendon & Young, 1998). In this survey data, the authors documented the emergence of a dichotomy in public opinion: a general opposition to marijuana legalization but general support for allowing physicians to prescribe marijuana for palliative purposes. Long-term CBS News polling (2012) documents a steady growth in support for medical marijuana with 83% in favor in 2012 versus 62% in 1997 (the year after California became the first medical marijuana state). In contrast, last year marked the highest level of documented support for legalization with 47% in favor and 47% opposed. In summary, the term “medical” has been used to counteract well-entrenched social perceptions of marijuana users. This strategy has apparently been effective when measured by the adoption of medical marijuana laws. The contrast in California makes the case most clearly. While California became the first medical marijuana state in 1996 by popular vote, a full legalization referendum was rejected in 2010 despite the consistent migration of public opinion toward a more favorable view of marijuana use in general. In addition, historically conservative states such as Arkansas have come close to adopting medical marijuana laws, while states perceived to be socially liberal, such as Oregon and Nevada, have rejected complete legalization.
Despite the success of policy adoption, deep social divisions inevitably continue to exist in the implementation process. Many implementation rules delegate power to local and county authorities, potentially intensifying the social and political divisions between would-be users and those charged with interpreting and enforcing the law. There are several possible causal mechanisms to support a relationship between the ongoing social construction of medical marijuana users and the number of registered medical marijuana patients.
First, the effects of social construction are arguably most tangible in regard to the issue of stigma (cf. Granberg & Holmberg, 2010; Triandis, 1989). Medical marijuana is a rare issue where social, medical, and political stigmas intersect. There is solid research that stigma (Corrigan, 2004), social pressures, and support networks (Lomas, 1998) affect patients’ medical choices as much as, if not more than, the efficacy of medicines themselves. Medical marijuana laws are themselves a form of social acceptance that create the opportunity for new directions in patient–doctor relationships (Bonenfant, 2010). Unlike most medical issues, however, the politicized nature of the medical marijuana debate makes marijuana possession, growth and distribution a public issue, subject to the formal and informal judgments of others.
It is plausibly more difficult for a conservative, religious Republican resident of a county to seek out medical marijuana as a medication even when it may, in the eyes of a physician, be medically appropriate. It may even be unlikely for such a citizen to engage socially and medically with a physician who would consider medical marijuana a legitimate treatment. Through this analysis, we come to a much-neglected point that the operational success of implementing a policy has as much to do with the culture of the target jurisdiction as it does with the policy acumen and administrative skill of the responsible agency (cf. Pressman & Wildavsky, 1989, for the bedrock analysis of this general point). Consequently, we come full circle to the importance of determining the attributes of the community within which a policy is being implemented.
If this proposition that medical marijuana is best seen as a social construction problem is correct, then variation in the adoption and implementation in medical marijuana laws should be influenced, at least in part, by the perception of medical marijuana users by others in their communities. The main purpose of this paper is to understand the degree to which the social construction of medical marijuana users influences the implementation of medical marijuana laws even after the laws have been passed and administration has been designed. As stated earlier, I predict that the negative or positive construction of medical marijuana users in a given political community has a statistically significant relationship to the rate of registered users in that community.
Research Design
Official information about the structure of programs and user data as of August 2012 have been derived from state medical marijuana program websites and phone conversations with two of the state programs (Vermont and New Mexico). The rapidly changing drug policy landscape makes it necessary to draw an arbitrary stop point for data collection. County-level data were also compiled from the 2010 Census Estimates and 2008 county election returns from the respective secretaries of state. Finally, dispensary data were compiled from medical marijuana program websites.
The dependent variable in this model is the percentage of county residents registered as medical marijuana patients. This provides a standardized measure of the relevant target group across counties of all sizes. County-level patient registration data are available from Arizona, Colorado, Maine, Montana, New Mexico, Rhode Island, Oregon, and Vermont. These medical marijuana states now require yearly patient registrations. Each state is on equal footing because of the use of 2011 data, a year that is available for each jurisdiction. The percentage was calculated using the most recent county patient numbers and 2010 county census data. This was the closest possible measurement. As a result, the sample size is 312 counties.
Two states do not maintain registries (Alaska and Washington), and California’s registry is voluntary. In addition, Michigan and Hawaii (as of the time of writing) do not make county-level data available to the public, even on request. Also, Vermont does not track data by county, but the small size of the state makes it feasible to treat the state as a single county. Finally, because of legal delays, New Jersey and Washington, D.C., have not yet released to the public (as of early 2012) the number of applications they have received for their start-up medical marijuana programs. Despite the limitation in the number of states available, the use of county-level data within the available states overcomes the small sample size problem that would exist if we looked only at the state level.
The key county-level explanatory variable is political culture. The following model uses county results from the 2008 presidential election to measure political culture. The history of the drug war in general can be defined as the implementation of competing values in agencies and programs divided along the lines of law enforcement and treatment. These competing perspectives can roughly be mapped as “conservative” and “liberal,” as discussed in detail in the following sections.
The connection between voting behavior and the political culture of a jurisdiction is well-documented in political science. Developing the use of voting behavior measures in public administration could serve many purposes beyond the scope of this paper. For example, votes and other pronouncements have been used as a measure of the policy preferences of legislators (Carroll Lewis, Lo, Poole, & Rosenthal, 2013) and, more recently, executive cabinet members (Bertelli & Grose, 2007, 2011). In general, political science scholars have argued for a reliable association between voting behavior and a wider set of voter beliefs on social and economic issues despite disagreements about many specifics (Abramowitz & Saunders, 2005; Fiorina, 2005; Jacoby, 2010; McCarty, Poole, & Rosenthal, 2006; Palfrey & Poole, 1987). These arguments relate to the foundational work of Daniel Elazar, who documented the broader connection between political behavior and the cultural characteristics of a given jurisdiction. In particular, his works on Jewish communities in Canada (Elazar, Brown, & Robinson, 2003) and Swiss democracy (Elazar, 2001) emphasize the relationship between the cultural dimensions of a political community and its support of political positions.
One remaining question is whether or not “political culture,” as measured in voting behavior, is an adequate proxy for the social construction of medical marijuana users. Relevant to this question is the observation that some scholars have strengthened the empirical connection between general cultural cues, such as shopping and vehicle ownership, and political alignments (Jacobs, 2013; Marschall & Rahn, 2006). This work on cultural cues is particularly relevant to this paper since the causal link between social construction, political culture, and the ultimate rate of medical marijuana usage resides precisely in the types of cultural cues that can be manifest in everyday social interactions and yet predicted by highly polarized voting behavior. In addition, this line of theory connects social construction to the larger body of research on “polarization.” Certain scholars argue that the American electorate is deeply polarized, particularly when measured by political and cultural homogeneity at the county level (Bishop & Cushing, 2004). The existence and extent of “polarization” is an ongoing debate in political science. However, it is worth noting for this paper that coming to terms with county-level cultural differences is a crucial policy implementation problem in many, if not most, contexts. This paper proceeds on the assumption that these cultural differences are connected to differences in the social construction of medical marijuana users.
In short, while survey data directly of county-level attitudes toward medical marijuana use would be ideal, these data would be expensive to collect. In the meantime, we have a reliable theoretical basis for using county-level voting data as a cost-effective proxy until such time as the reliability of this choice can be specifically confirmed with public opinion survey data. Proceeding from this framework, national votes provide a clearer picture of ideology than local elections, where personal relationships often trump party association. At the same time, the local orientation of medical marijuana implementation requires, at a minimum, county data. Consequently, the measure is constructed as the percentage of county residents voting for the 2008 Democratic presidential candidate. The reason for this is that the coefficient will be a positive number since we expect medical marijuana use to be higher in “liberal” counties. While some states have data from their medical marijuana referendum votes, the 2008 election data seemed more appropriate for several reasons. First, it was a nationwide case of a deeply ideological, polarized election that drove high turnout. In other words, there were few dispassionate voters in the election, and the results were not skewed based on bias from low turnout. However, this election data also allows us to develop finely attuned county-level data that is difficult, if not impossible, to access in the context of other votes. This advantage is particularly important in a state like Oregon, for example, that went largely for Obama although the majority of (rural) counties were strongly for McCain. This matters little to an election strategist; it matters a great deal to the resident of a conservative county—in an otherwise liberal state that is more likely to have legalized medical marijuana at the state level—who may face general stigma or difficult conversations with friends and family locally when considering the use of medical marijuana. Conversely, it also likely captures preferences for marijuana that would exist regardless of its legality.
While the institutional design aspects of implementation are not the focus of this paper, it is important to control for these variations in this model. The regulation of supply is one of the key components of medical marijuana implementation. Two variables in the model control for supply: dispensaries (disp_reg), which can be measured at the county level, and individual production (indv_prod), which is legal only in Montana. There is a tremendous amount of variation in supply rules across states and even counties. Some states allow personal growing (Montana), other states have a mostly deregulated system with a high number of dispensaries (Colorado, California), and most are now moving toward a limited number of state-sanctioned dispensaries. The claim of almost all marijuana advocates and a growing number of state officials is that marijuana dispensaries are necessary to ensure a safe, legal supply of marijuana for medicinal users. State-controlled dispensaries are becoming the standard approach for medical marijuana laws.
The variation is good in the sense of providing the opportunity to measure the effect of supply. However, a great deal of anecdotal evidence suggests that there is very little connection between the legalization of supply and the legalization of use. Standard market theory suggests that there should be a close relationship between supply and demand. However, the system represents an unusual combination of a quota imposed through regulation, legalized production of a federally illegal good, and incentives for continued reliance on the black market. The distribution of dispensaries between states that allow free competition (an estimated and/or planned 2,306 dispensaries in Colorado and California) and those that provide through the state (20 for all other states) is staggering. The following findings demonstrate the ramifications of this disparity.
The rest of the model is composed of key state-level controls. The first control is for the length of time the state has been a medical marijuana state, in months. One alternative hypothesis is that governments learn (Sabatier, 1998), so implementation may be improved (in terms of the numbers of patients registering more quickly) in states that have had a program longer. This process may create fewer institutional barriers to achieving desired outcomes, and legislators and advocacy coalitions may adopt implementation lessons for future campaigns. A second alternative hypothesis is that states have engaged in learning from previous medical marijuana states. In either case, this is an important control.
In addition, the issue of reciprocity is a unique institutional feature of Montana’s medical marijuana regime. Because of the present state of the law, this control variable is essentially a Montana control. Montana is demonstrably the highest medical marijuana usage state per capita—despite the fact that it does not allow dispensaries. As a result, the reciprocity control did not disappoint.
The question of what diseases and conditions should qualify for medical marijuana is one of the most controversial issues in medical marijuana implementation and one of the sharpest splits between public health and law enforcement advocates. Patients with certain “hard” medical conditions are allowed to use under nearly every state law (cancer, HIV/AIDS). However, states have varied widely in the number and type of conditions allowed. Of the 15 states (including DC) with rules presently in place, judgment varies widely in regard to Crohn’s disease (9), cachexia (14), migraines (1), muscle spasms relating to permanent muscle or spinal injury (14), severe nausea (14), neuropathy (2), and “severe” and/or “intractable” pain (15). This issue is a double-case of discretion; on one hand, there is discretion in allowing or disallowing conditions, but on the other is the expression of a secondary tolerance for an increased potential for unlawful use, if conditions become more vague and susceptible to gaming.
On the medical issue, one limitation of this model is the inability to control for the underlying health of the counties measured here. While many county public health data do exist, these data do not generally capture directly the types of palliative conditions covered by medical marijuana laws. In other words, the conditions listed earlier have a second-order connection to public health issues since many medical marijuana patients are HIV or cancer patients who are using marijuana for palliative purposes. However, none of the said conditions are catalogued in a systemic, multi-state manner in such a way that allows for efficient statistical control in this paper.
Results
I used OLS to test the model. The dependent variable is an interval-level variable conditioned upon a predictive variable (political culture) that measures culture on a linear basis rather than the forced dichotomous measure of other models. As predicted, political culture and the rate of registered medical marijuana users had a strong and statistically significant effect. Political culture has the largest coefficient (.0657) and a reasonably sized standard error (.02; see Table 1). This appears to be a solid and reliable result that validates the hypothesis that variation in political culture acts as either a barrier or conduit for achieving policy outcomes. A measure of only the management or institutional design features of implementation would have produced a very different result.
Operational and Institutional Variables and Medical Marijuana Utilization.
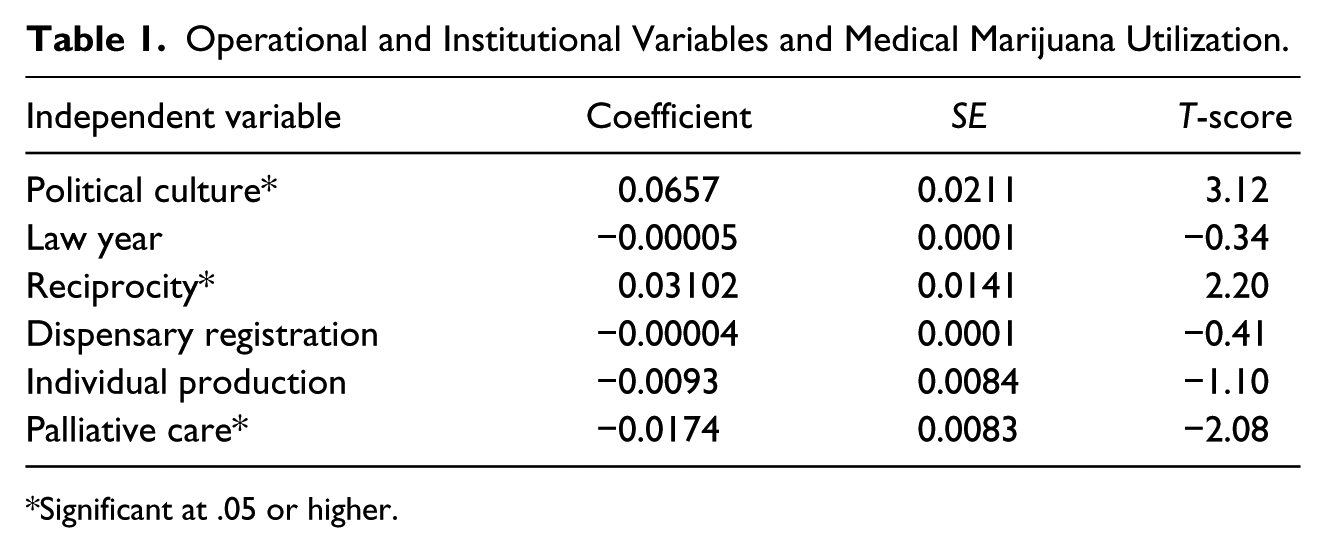
Significant at .05 or higher.
This finding provides direct evidence of, at the least, an association between the self- and other-perception of target populations and the achievement of a policy’s intended outcomes. In this particular case, we can motivate the finding of substantially higher utilization in “liberal” areas with the theory that the political “liberality” is connected to an underlying and intertwined social network that opens or closes the space for some within the community to take on the role of a “medical marijuana patient.”
There is, of course, some relationship between the fact that urban areas, with more patients, are more likely to be concentrated areas of Democratic voters and have more access to medical marijuana resources. However, the “liberal” vote and the percentage of the county’s population who are medical marijuana users are standardized measures. Consequently, a higher percentage of users can be achieved in a rural county with very few actual users. In addition, a review of user data shows that there are very few counties in states where medical marijuana is legal that there are not at least some users (4 out of 312 counties have 0 registered users), which includes a significant percentage of rural, conservative counties.
As further evidence of the underlying mechanism of social construction in these findings, not one state, as of the time of the 2008 voting data used here, showed poll numbers where a majority of voters favored outright marijuana legalization or decriminalization. The medical dimension of marijuana use, in other words, has an effect even among traditionally Democratic constituents who may not be “liberal” enough to be interested in achieving full legalization, but who are willing to support use if it is for patients under the care of a medical doctor for purposes of alleviating suffering. California’s 2010 (failed) vote on marijuana legalization is the case in point.
We should also highlight that the finding is embedded within a particular institutional context. In other words, political culture represents the informal rules of social and political association in a community, whereas institutional design represents the core formal rules of a given implementation effort. The model controlled for two important areas of institutional design. Reciprocity, recognizing the permits granted in other states, increases medical marijuana usage in Montana, as one would expect. In addition, the palliative care index is related to implementation; also, the interpretation of the negative coefficient requires more attention. Both of these variables are direct measures of important institutional design choices made in state programs.
The focus on formal rules and informal norms should not be construed as diminishing the role of public managers and other public actors. On the contrary, because medical marijuana implementation has been accomplished through rulemaking and negotiation, public health officials, law enforcement, and patient advocates have all played a strong role in constructing the institutions within which they will engage in future management activities. Because most state medical marijuana programs delegate some scope of authority to counties in regard to the administration of ID card programs (California), the zoning of dispensaries (Colorado, Maine), and even, informally, the discretion of police officers in regard to enforcing the law, political culture has a direct causal influence on the implementation of medical marijuana laws.
From the perspective of administering state medical marijuana programs, we may reasonably assume that there is variation in the perceived legitimacy of policy goals on the basis of the political values and culture of the organization that has been delegated responsibility for administering medical marijuana programs. Future research may reveal a substantially different approach to institutional design when the task is delegated to law enforcement agencies as opposed to public health agencies. This paper argues, however, that models which control only for the behavior of formal actors are limited because they focus only on the actors within the system rather than on the full network of informal social relationships that are responsible for resisting, stigmatizing, or facilitating the policy within the political community. Political culture as a concept extends beyond this limitation by acknowledging the very thin line between politics and administration at the local and, to some extent, state level.
This dynamic between management and institutional design demonstrates the usefulness of the IAD framework’s multi-level approach. At the same time, it reinforces the importance of the main findings, that the social construction of medical marijuana patients has a strong causative relationship to the likelihood of achieving outcomes. In addition to the direct influence on users’ willingness to participate in the system, I have speculated on a secondary influence between political culture and the social constructions of local and state officials. Future research can map the specific parameters of this influence.
Institutions, similarly, have structured the boundaries of this implementation situation. The diffused, localized nature of implementation has, in this paper, enhanced the influence of local cultural factors on implementation. The importance of this finding for political actors and policy analysts is that those who study, design and implement institutions must adopt a more nuanced understanding of the way in which target populations as socially constructed groups and institutions influence one another. In other words, this dimension of medical marijuana bears resemblance to other socially divisive policies with diffused implementation strategies, particularly social welfare programs.
On the other hand, it is disappointing that the palliative care index is statistically significant with a negative coefficient. The theory I have used and just described would seem to indicate that palliative care would be both positive and have a large coefficient. However, there are several mitigating circumstances. First, the variation between states is, for the most part, fairly small; there is more agreement on palliative care issues than expected. This can be corrected in the future by dropping the conditions (chronic pain, cachexia) in which there is near-unanimous agreement. Second, it is possible that this is a true result. One possible outcome is that states that have allowed for more ambiguous conditions have triggered a backlash of discretion on the part of law enforcement. It is also possible that there are interaction effects between variables that require more study in the future.
Finally, there appears to be no connection between the levels of regulated, legal supply and patient use outcomes. This aspect of the study, while treated as a control in this model, is crucial to building a bridge between culture, social construction, and policy implementation. As discussed before, anecdotal evidence (and common sense) suggests that the majority of medical marijuana users still obtain marijuana, plants, seeds, and technical assistance from the black market (e.g., Medical Marijuana of Hawaii, 2011). Patients in nondispensary states have advocated for dispensaries on the ground that it is unsafe to continue seeking their medical supplies from illegal suppliers (e.g., Bonenfant, 2010). It is possible that we have discovered a case but the black market is an essential player in the successful implementation of state policy. There is a robust literature, primarily in international development, on the role that black markets play in economic development. However, there is very little literature on black markets in the official policy process. This aspect of the study sheds a whole new dimension on political culture and the interaction between policy, society, and the market. A more conclusive test of this hypothesis will be to run this test again once regulated dispensaries are open in the new medical marijuana states. These states may end up requiring patients to acquire their supplies at dispensaries, disincentivizing black market activity.
Conclusion
This paper has suggested that political culture, as a proxy for social construction, intervenes in the implementation of state medical marijuana policy. I have also demonstrated statistically that informal norms in a given community can help or hinder the achievement of formal policy goals.
At the state level, the political preferences of the state’s legal organs is correlated to the choice of implementation strategy and the level of discretion built into the state’s system. At the county level, the political culture manifest in voting behavior has a strong influence on end users’ medical marijuana use and the distribution of dispensaries in states where that distribution is driven by voluntary rather than political choice. At the individual level, we have discovered a striking theory that the culture of the black market continues to play a shaping role in what has become a quasi-legal activity.
All of these findings lay the groundwork for future studies that more closely assess the relationship between implementation strategy, political culture, and the criminal justice and public health impacts of medical marijuana. It is possible that these programs have demonstrated that drug policy can be responsibly managed; indeed, each new state appears anecdotally to depend more heavily on the practices of the last, although the amount of policy learning cannot be quantified as constructed in this paper. At the same time, it is possible that the attempt to “end around” the ironclad drug war orthodoxy has led to a hybrid, dead-end form of public policy that will inevitably continue to be entangled in a net of federalist, black market, and cultural confusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.