
Abstract
This study examines how healthcare professionals and administrators experience and respond to volatility, uncertainty, complexity, and ambiguity (VUCA) during digital transformation, integrating SWOT analysis to capture systemic strengths, weaknesses, opportunities, and threats. Thirty-five semi-structured interviews with physicians, nurses, and administrators (2021–2024) were analyzed abductively within the combined VUCA-SWOT framework. Volatility reflected technological acceleration; uncertainty arose in decision-making and telemedicine; complexity involved fragmented infrastructures and workforce shortages; ambiguity appeared in inconsistent training, intergenerational digital divides, and reduced human connection. The VUCA-SWOT lens provides strategic insights to enhance resilience and guide sustainable healthcare delivery in evolving environments.
Introduction
In recent decades, healthcare systems have been operating in an increasingly volatile, uncertain, complex, and ambiguous environment (VUCA) that is shaped by rapid technological advancements, economic pressures, demographic shifts, and socio-political changes (Otter, 2019; WHO, 2016, 2019). Three interconnected levels can be used to examine this environment: the macro (policy and system-wide governance), the meso (organizational adaptation and management), and the micro (day-to-day professional practice and patient care) levels.
At the macro level, these wide-ranging technological, economic, demographic, and socio-political dynamics drive structural transformations that require adaptive strategies to ensure sustainability and resilience (Benjamin, 2010; Counte et al., 2019). In the face of complex global challenges such as pandemics, climate change, and technological disruption, healthcare organizations must pursue structural transformation to remain sustainable and resilient (WHO, 2020). Such transformation necessitates the adoption of adaptive strategies that align with systems thinking and dynamic capabilities (Begun & Jiang, 2020). Moreover, economic constraints and digital transformations also necessitate innovative approaches to healthcare management, pushing organizations to develop new adaptation and service delivery frameworks (Ginter et al., 2018; Marzaleh et al., 2022; Naamati-Schneider, 2020, 2023).
At the meso level, healthcare organizations find themselves increasingly relying on digital health technologies – such as telemedicine, electronic health records (EHRs), and home care programs – to optimize resource allocation, improve accessibility, and strengthen system resilience, while also enhancing organizational flexibility (Harjula et al., 2022; Sheaff & Schofield, 2016). Agile governance structures and leadership models that support decentralization and rapid decision-making are also vital (Braithwaite, 2018). Sustainability requires a shift to value-based care, prioritizing outcomes over service volume to improve cost-effectiveness and equity (Porter & Lee, 2013). Environmental sustainability further requires initiatives such as green hospital design and sustainable procurement, as demonstrated in recent European healthcare reforms (Kuhn et al., 2025). For instance, hospitals taking part in the Practice Greenhealth 2025 Environmental Excellence Awards collectively cut over 185,000 metric tons of greenhouse gas emissions and saved over $203 million by implementing sustainability programs. The development of resilience has become increasingly dependent on the enhancement of workforce capacity, the integration of scenario-based planning, and the adoption of climate-resilience frameworks. These practices increased by 140% from 2023 to 2024 (Practice Greenhealth, 2025). Furthermore, cross-sector collaboration with technology firms, logistics providers, public health agencies, and NGOs has expanded the adaptive capacity of healthcare organizations, facilitating innovations such as climate-informed disease surveillance, decentralized public health networks, and integrated delivery and financing models for improved access to care (Alfina et al., 2025; Shafik et al., 2025).
At the micro level, healthcare professionals must navigate shifting workplace dynamics, digitalization of medical services, and evolving patient-provider interactions (Coorevits et al., 2013; Wan et al., 2021). Although digital tools can enhance clinical decision-making and improve access to information, they also introduce new demands that reshape professional roles and responsibilities. Clinicians must learn to balance the efficiency of technology with the human aspects of care while navigating pressures that affect both their daily practice and their relationships with patients (Naamati-Schneider, 2023; Naamati-Schneider et al., 2024a, 2024b).
To address these multilayered challenges, this study examines the VUCA ecosystem in healthcare through a qualitative analysis of the experience of healthcare worker. Using SWOT analysis, the study identifies strengths, weaknesses, opportunities, and threats within the VUCA framework and offers strategic insights to enhance system resilience and sustainability. The findings of this study are intended to inform policymakers, healthcare administrators, and practitioners about effective approaches for navigating an increasingly unpredictable healthcare landscape.
The VUCA Framework and Its Impact on Healthcare
The concept of VUCA originally emerged in military strategy to describe unpredictable global conditions (Otter, 2019). Over time, VUCA has been widely adopted in business, policy, and healthcare to highlight and explain the challenges of an ever-changing environment (Cernega et al., 2024; WHO, 2016, 2019). In healthcare, VUCA conditions find expression in economic pressures, technological advancements, regulatory changes, and shifting patient expectations, all of which require continuous adaptation at multiple levels of governance (Benjamin, 2010; Counte et al., 2019). This section explores the elements of the VUCA framework in the context of healthcare organizations.
Volatility in Healthcare
Volatility refers to rapid and unpredictable fluctuations that disrupt stability (Otter, 2019). Healthcare organizations must increasingly cope with volatile conditions due to shifting funding models, fluctuating resource availability, and sudden and frequently unanticipated public health crises (Ginter et al., 2018; Marzaleh et al., 2022). For example, the COVID-19 pandemic exposed the fragility of healthcare systems, forcing hospitals to reallocate resources and scale services under extreme conditions (Naamati-Schneider & Zaks, 2022; Zangrandi et al., 2020). Additionally, technological innovations in telemedicine, AI-driven diagnostics, and data analytics are evolving at an unprecedented pace, creating both opportunities and challenges in service delivery (Rathee et al., 2020).
Uncertainty in Healthcare Systems
Uncertainty arises when future developments are unpredictable, making decision-making difficult (Otter, 2019). In the healthcare context, regulatory changes, evolving disease patterns, and economic instability create uncertainty for organizations, policymakers, and professionals (Counte et al., 2019). Digital transformation, while essential for enhancing efficiency and accessibility, also introduces new uncertainties related to cybersecurity risks, interoperability, and ethical dilemmas in patient data management (Harjula et al., 2022; Sheaff & Schofield, 2016).
Complexity in Healthcare Structures
Healthcare is inherently complex due to its interdependent systems, multidisciplinary teams, and diverse patient needs (Benjamin, 2010). The growing integration of digital health technologies, AI-driven diagnostics, and remote care models has increased the number of variables in healthcare delivery, requiring new approaches to data management, workforce training, and regulatory compliance (Bhuvana & Vasantha, 2020; Marzaleh et al., 2022). A key challenge lies in aligning healthcare policies, financial models, and technological advancements while ensuring equity and quality of care (Coorevits et al., 2013; Wan et al., 2021).
Ambiguity and Decision-Making in Healthcare
Ambiguity refers to situations in which outcomes are unclear due to a lack of precedents or reliable data (Otter, 2019). In the healthcare context, ambiguity is particularly evident in emerging diseases, innovative treatments, and evolving patient expectations. For instance, while digital platforms have improved access to care, they also create ethical and legal ambiguities regarding patient confidentiality, liability, and informed consent (Whitten et al., 2010). Similarly, the shift in healthcare delivery models from hospital-centric to community-based and digital-first approaches has introduced new challenges in defining roles and responsibilities among healthcare providers (Sheaff & Schofield, 2016).
The Role of Digital Transformation in the Changing VUCA Healthcare System
The rapid technological advances of the Fourth Industrial Revolution (Schwab, 2017, 2024) have generated a global shift across industries, placing increasing pressure on healthcare systems to adapt. Within this context, digital transformation has emerged both as a strategic response to the challenges posed by VUCA conditions and as a factor contributing to their intensification. Even as digital tools such as AI, big data, and telemedicine offer solutions to volatility, uncertainty, complexity, and ambiguity, their implementation introduces new forms of disruption that reshape workflows, roles, and expectations across all levels of the healthcare system (Naamati-Schneider, 2020, 2023). This dual role positions digital transformation not only as a pathway to resilience but also as a dynamic force that redefines the very environment it seeks to stabilize.
More specifically, the adoption of telemedicine, EHRs, AI, big data analytics, and remote patient monitoring has become central to enhancing decision-making, patient care, and organizational management (Harjula et al., 2022; Sheaff & Schofield, 2016). These advancements reflect a shift from traditional hospital-based models to more decentralized, technology-driven healthcare solutions (Whitten et al., 2010). This shift was accelerated by the COVID-19 pandemic, which exposed structural vulnerabilities and increased demand for rapid, technology-enabled decision-making (Argenziano et al., 2020; Marzaleh et al., 2022; Naamati-Schneider & Zaks, 2022). Yet the successful implementation of digital transformation is not solely dependent on technological infrastructure. It requires systemic, organizational, governmental, and professional adaptation across the healthcare system. Aligning policies, workflows, and professional practices demands flexibility, continuous learning, and a supportive environment capable of navigating technological, structural, and cultural changes (Figueroa et al., 2019; Ginter et al., 2018).
Despite its potential benefits, digital transformation also introduces significant challenges, among them organizational resistance, ethical dilemmas, and workforce-related issues (Karni & Reches, 2018; Naamati-Schneider et al., 2024a, 2024b). Strategic guidance and ethical frameworks are essential to ensure that digital innovations are integrated in ways that align with system needs, uphold professional standards, and support long-term sustainability (Naamati-Schneider, 2023).
The VUCA Healthcare Ecosystem: A Multi-Level Perspective
The concept of a VUCA environment has gained increasing relevance in the healthcare literature, as scholars and policymakers seek to understand how systemic instability, rapid technological advancement, and shifting population needs shape health service delivery (Morgan-Gorman et al., 2025; Otter, 2019) To address these multifaceted challenges, recent studies advocate a multi-level analytical framework that considers the macro, meso, and micro dimensions of healthcare systems (Coorevits et al., 2013; Ginter et al., 2018; Marzaleh et al., 2022; Naamati-Schneider & Alt, 2024).
At the macro level, VUCA conditions are driven by broader socioeconomic forces, including demographic change, global pandemics, political instability, and technological disruption. National health systems are subject to evolving policy frameworks, funding models, and regulatory expectations that demand strategic foresight and systemic adaptability (Marzaleh et al., 2022; WHO, 2016, 2019). Scholars emphasize the critical role of healthcare governance in creating resilient organizations capable of withstanding future shocks, particularly through investments in digital interoperability, ethical standards, and equitable access (Figueroa et al., 2019; Harjula et al., 2022). Indeed, the literature indicates that contemporary healthcare governance must evolve beyond compliance frameworks to integrate strategic business models that reinforce institutional resilience, particularly through digital interoperability and equitable access (Mshelia et al., 2025). From an economic-administration standpoint, this involves mobilizing investments in interoperable health platforms that yield productivity gains. Studies predict that integrating EHRs, e-prescribing, and management systems will yield up to 15% improvements in system-wide efficiency by 2030 (McKinsey Health Institute, 2025). Such infrastructure investments not only reduce administrative costs, but also strengthen the organization’s bargaining power with customers and suppliers by streamlining care delivery (Cardoso et al., 2018; McKinsey Health Institute, 2025). Moreover, economic administration strategies have increasingly incorporated equitable financing models, such as blended public-private funding, performance-based contracts, and investment, to ensure that digital expansion yields both fiscal sustainability and social inclusion (Oso et al., 2025). Governance is therefore reimagined as an integrative business function that includes setting ethical protocols, evaluating economic returns, and aligning capital flows to advance infrastructure resilience, equitable access, and long-term institutional adaptability.
At the meso level, healthcare organizations function as the operational bridge between national policy directives and everyday clinical practice. Here, volatility and complexity often are manifested through fragmented digital infrastructures, overlapping managerial roles, and insufficient institutional support mechanisms (Ginter et al., 2018; Sheaff & Schofield, 2016). Organizational responses to digital transformation typically involve restructuring workflows, reallocating resources, and revising staff training programs. These processes are influenced by internal cultural dynamics and the organization’s managerial capacity. In the absence of coherent strategies and internal alignment, digital innovation may unintentionally intensify inefficiencies and exacerbate workforce pressures rather than improving service delivery and resilience (Coorevits et al., 2013; Marino & Diaz Paz, 2025; Naamati-Schneider, 2023).
At the micro level, healthcare professionals experience the effects of VUCA most directly. Studies have documented the growing emotional and cognitive burdens on clinicians as they navigate role ambiguity, shifting patient expectations, and new digital tools (Kuhlmann & Knorring, 2014; Naamati-Schneider et al., 2024a, 2024b; Wan et al., 2021). Although technologies such as electronic health records and telemedicine can support decision-making and improve access to care, they may also compromise the interpersonal aspects of healthcare, particularly among aging professionals or those with limited digital training (Whitten et al., 2010). Scholarship on digital competence and professional adaptation suggests that successful implementation depends not only on technological infrastructure but also on sustained investment in communication, training, and interprofessional collaboration (Khan et al., 2025).
When viewed through this multi-level lens, the VUCA framework offers a powerful tool for understanding the evolving complexity of healthcare. To remain effective and sustainable, healthcare systems must coordinate policy, business governance, organizational strategy, and professional capacity. This layered model creates a foundation for using strategic frameworks such as SWOT analysis to help identify internal capabilities, anticipate external threats, and build system-wide resilience (Fiet, 2025; Ngwenya et al., 2025).
Strategic Management Approaches: The Application of SWOT Analysis in Healthcare
In the context of a volatile and rapidly evolving healthcare environment, strategic planning tools are essential for navigating systemic uncertainty and ensuring organizational resilience. One widely used approach is SWOT analysis, a diagnostic framework that categorizes internal factors (strengths and weaknesses) and external influences (opportunities and threats) to support evidence-based decision-making and strategic adaptation (Fiet, 2025). Although initially developed in the business sector (Learned et al., 1965), SWOT analysis has been increasingly applied in healthcare to assess business performance, identify governance flaws, and guide innovation across varying service domains and structural levels (Salvatore et al., 2024).
Recent studies have demonstrated the applicability and flexibility of SWOT analysis in healthcare organizations. Harel and Magnezi (2024), for example, used SWOT analysis to assess managerial attitudes toward Acute Hospital at Home (AHaH) models. Their findings pointed to a consensus about the clinical advantages of AhaH, while revealing institutional concerns about caregiver burden, financial incentives, and insufficient standardization. Similarly, Mansuroğlu and Davut (2025) employed a qualitative SWOT case study to explore community-based mental health services, incorporating both provider and patient perspectives. Their analysis highlighted the importance of aligning organizational strengths with service users’ needs while addressing infrastructural and training-related weaknesses. In a related study, Ngwenya et al. (2025) conducted a scoping review of digital triage tools in obstetrics. The analysis identified diagnostic accuracy and resource limitations as key weaknesses, while underscoring the transformative potential of digital interventions to improve emergency care access and system efficiency. Furthermore, Ozughalu et al. (2024) conducted a methodologically robust strategic assessment of a local teaching hospital using a SWOT analysis framework integrated with the Modified Delphi Technique. The study examined hospital executives and administrative staff as they attempted to reach consensus on strategic priorities across 12 organizational domains. This approach allowed for both a quantitative aggregation of expert insights and a qualitative reflection on institutional dynamics, making it particularly well-suited for analyzing business-administrative performance in complex healthcare settings.
Conceptual Integration of VUCA and SWOT
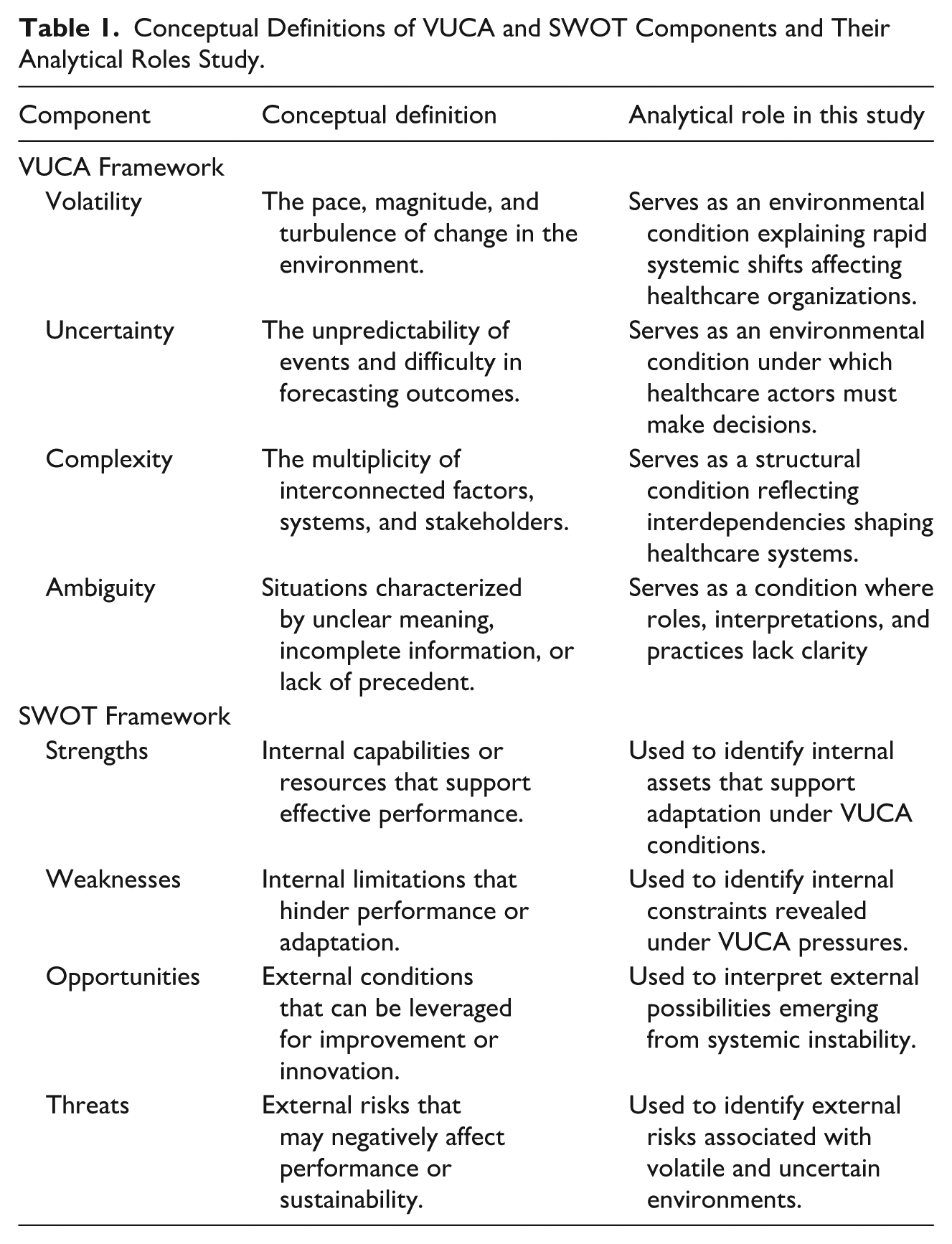
To clarify the analytical logic guiding this study, this section presents the conceptual integration of the VUCA framework with SWOT analysis. While VUCA describes the environmental conditions shaping healthcare systems, SWOT provides a strategic interpretive lens through which these conditions can be translated into actionable organizational insights. The integration of these frameworks enables a structured understanding of how systemic instability is experienced across healthcare system levels and interpreted as internal strengths and weaknesses alongside external opportunities and threats, ultimately informing strategic responses.
Table 1 details the conceptual definitions of the VUCA and SWOT components and clarifies their analytical role in the study. Figure 1 illustrates the analytical pathway linking environmental conditions, professional and organizational experience, SWOT interpretation, and strategic healthcare responses.
Conceptual Definitions of VUCA and SWOT Components and Their Analytical Roles Study.
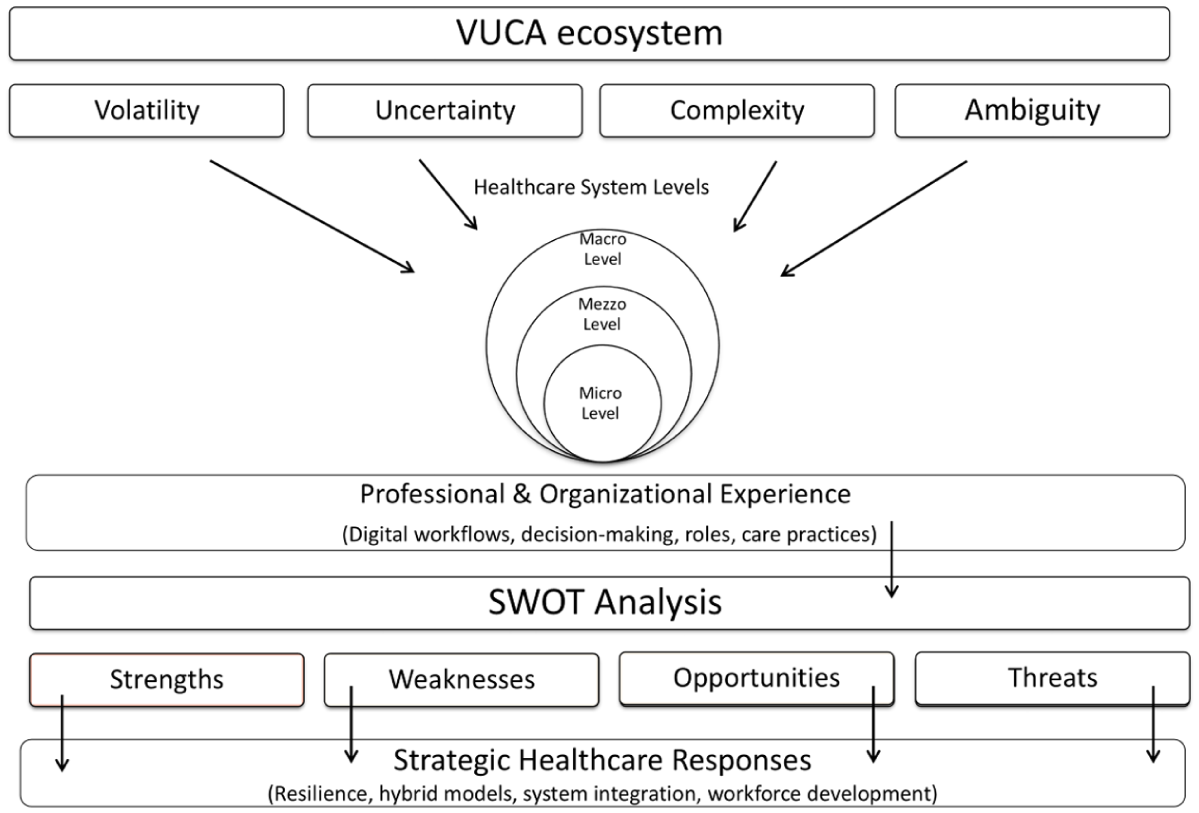
Conceptual integration of the VUCA framework and SWOT analysis in healthcare systems.
This conceptual model underpins the approach the following section describes.
Research Design
Study Design and Scope
This qualitative study explored how healthcare professionals and administrators perceive, interpret, and respond to the challenges posed by a VUCA environment in the context of ongoing digital transformation. Adopting a system-level perspective, the study investigated the effects of VUCA dynamics across macro (policy), meso (organizational), and micro (professional) levels of the healthcare system. The aim was to illuminate how digital disruption intersects with institutional structures, managerial practices, and clinical roles, and how professionals adapt strategically under conditions of instability. By integrating the VUCA framework with SWOT analysis, the analysis provides a multi-dimensional understanding of how digital change is navigated in practice, offering insights into system resilience, professional agency, and sustainable transformation in healthcare delivery.
Participants and Sampling
The study was conducted between 2021 and 2024 among 35 healthcare professionals, including physicians, nurses, and administrators serving as key decision-makers in large public hospitals. Participants were drawn from five major hospitals representing different regions of the country and varying organizational scales. The hospitals were selected based on their size, patient volume, and operational complexity. To preserve institutional confidentiality, hospitals are described in aggregate rather than by name, in accordance with ethical research guidelines. By including both clinical and managerial perspectives, the study offers a comprehensive understanding of how professionals at different levels of the system navigate and leverage VUCA dynamics.
A snowball sampling approach was employed, starting with an initial group of participants who were invited via email. These individuals were encouraged to refer colleagues who met the study criteria, ensuring a diverse representation of experiences across various medical specialties and professional backgrounds. The sample size was determined based on data saturation. That is, recruitment continued until no new themes emerged, ensuring a robust and in-depth analysis of adaptive strategies in a VUCA healthcare system (King, 2004).
Data Collection and Ethical Considerations
Ethical approval for this study was obtained from the ethics committee at the first author’s institution. After the study was approved, participants were contacted via email and invited to participate in virtual interviews conducted via Zoom. Prior to each interview, participants were given an informed consent document detailing the study’s ethical approval, voluntary participation, confidentiality measures, and the option to withdraw at any time. To ensure anonymity, all personal identifiers, including names and workplaces, were removed from transcripts. Participants explicitly agreed to audio recording, transcription, and use of the research findings, with assurances that their identities would remain confidential (Morse, 2021).
Interview Process and Thematic Focus
Between 2021 and 2024, a team of researchers trained in healthcare management conducted interviews, each lasting approximately 45 min. Standard verbatim transcription protocols were followed to maintain data accuracy. To ensure consistency and reliability, all interviewers underwent pre- and post-interview briefings to coordinate data collection methods and reflect on their interactions with participants.
To balance thematic consistency with the necessary flexibility for capturing individual perspectives in depth, a semi-structured interview format was employed. The interview guide served as a framework for exploring how healthcare professionals perceive and respond to systemic pressures, operational constraints, and the evolving landscape of digital transformation. Participants were invited to reflect on their experiences with resource limitations, organizational restructuring, and policy shifts, as well as the impact of technological change on their roles, responsibilities, and decision-making. The study further examined how professionals leverage organizational strengths, mitigate external threats, and identify opportunities for sustainability within a volatile healthcare environment. This approach facilitated a nuanced understanding of adaptive strategies and generated insights into how healthcare institutions and professionals can reinforce system resilience under conditions of persistent uncertainty.
Data Analysis
The study employed an abductive analytical approach (Timmermans & Tavory, 2012) to examine how healthcare professionals navigate and respond to challenges within a VUCA-driven healthcare system and organizations. By integrating predefined theoretical constructs from the VUCA framework with emergent themes from participant narratives, this methodology provides a comprehensive understanding of systemic adaptation, workforce resilience, and strategic sustainability. The approach ensures that the analysis remains both structured and open to unexpected insights while capturing the multilayered impacts of VUCA components in healthcare organizations. Given the dynamic and unpredictable nature of healthcare environments, the analysis systematically examines how macro, meso, and micro factors interact under VUCA conditions. Additionally, a SWOT-based perspective is applied to identify strengths, weaknesses, opportunities, and threats within this evolving healthcare landscape.
The analysis was conducted using multiple steps designed to support both theoretical alignment and grounded exploration.
Data Familiarization and Initial Thematic Mapping: The researchers read all the transcripts multiple times to allow for immersion in the data. This step supported the identification of initial themes, including those related to the four VUCA dimensions and those that arose inductively from participant narratives. Early observations were kept open and exploratory to avoid imposing fixed categories too soon.
Inductive Coding and Theme Development: Emergent codes were identified directly from the data using open coding. This method enabled researchers to discover themes not initially covered by the VUCA framework, including perceptions of digital overload, organizational fatigue, and intergenerational tensions. These inductive insights enriched the theoretical lens by highlighting novel dimensions of healthcare transformation.
Iterative Refinement and Thematic Consensus: Themes were refined through repeated comparisons across transcripts. The researchers iteratively reviewed and discussed patterns, yielding a coherent coding structure. Emerging themes were grouped into categories that captured systemic adaptation, professional coping, and organizational resilience.
Structuring Themes within the VUCA Framework: Once inductive coding was completed, the themes were systematically organized according to the four VUCA dimensions: volatility, uncertainty, complexity, and ambiguity. This alignment ensured that the analysis remained anchored in the study’s core conceptual framework while allowing for analytical flexibility.
Mapping across Healthcare System Levels: To enhance contextual understanding, the researchers positioned the themes within a three-tiered model of the healthcare system: macro (policy/systemic), meso (organizational), and micro (individual/professional). This step clarified how VUCA conditions and adaptive strategies manifest themselves differently across structural levels.
In the final stage, all the themes were translated into a comprehensive SWOT matrix that facilitated identifying internal strengths and weaknesses alongside external opportunities and threats across the healthcare system. This stage yielded a multidimensional analysis of how healthcare professionals and organizations not only confront systemic vulnerabilities and resource limitations but also leverage digital capabilities, policy shifts, and emergent practices to adapt and innovate. The SWOT lens provided a strategic scaffold for interpreting the findings, revealing both risks and untapped potential for enhancing resilience, sustainability, and forward-looking healthcare leadership.
Findings
The analysis is organized into four main themes: organizational disruption and acceleration through digital transformation; decision-making challenges and the role of technology in reducing diagnostic ambiguity; navigating multisystem demands and interdisciplinary burdens; and role confusion, inconsistent practices, and the human cost of digital transformation.
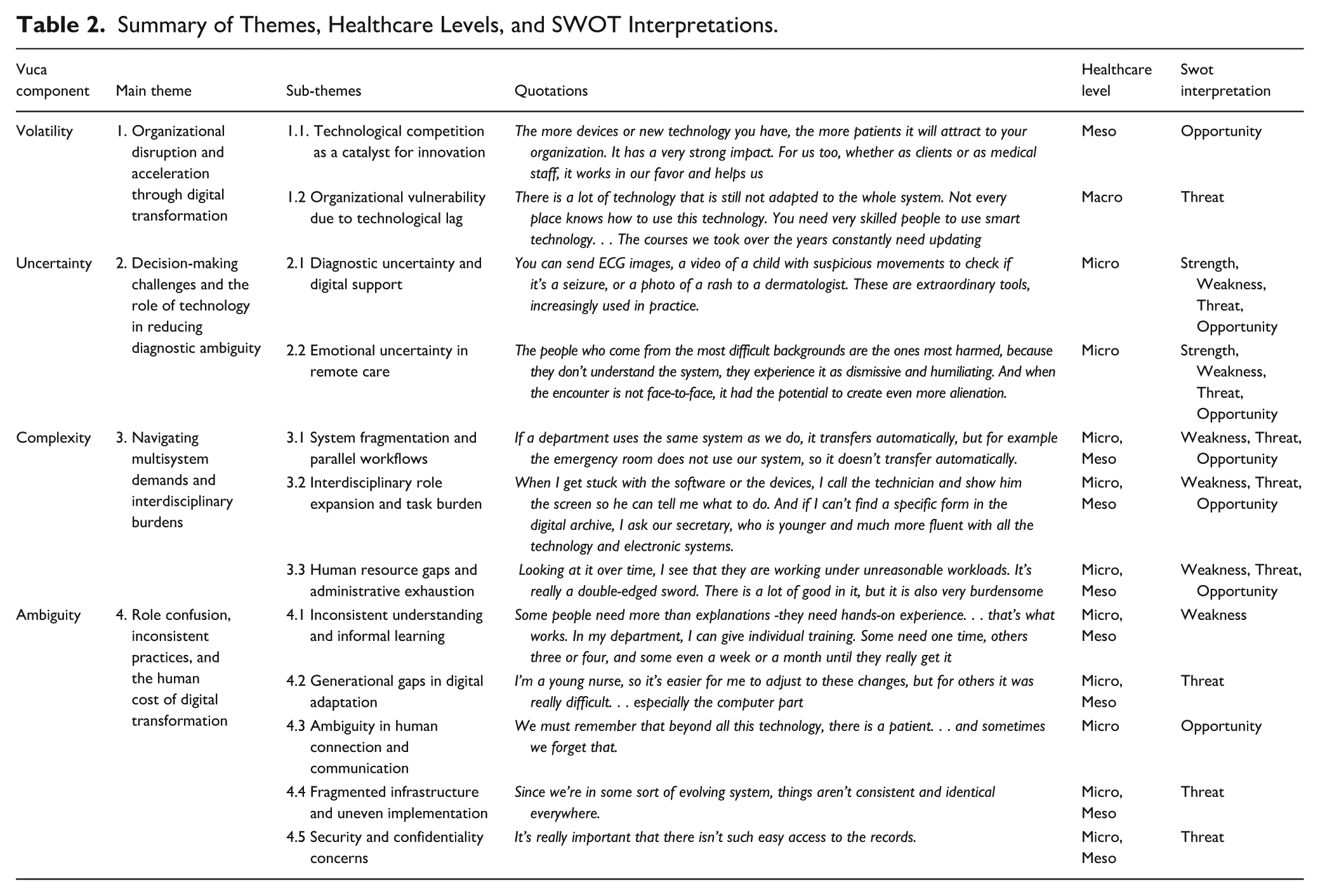
Each theme is further divided into sub-themes that reflect the nuanced ways in which participants described their day-to-day realities, challenges, and adaptive strategies. Illustrative quotes are used to ground the analysis in lived experience. The findings are interpreted through two analytical lenses: healthcare system level (macro, meso, micro) and SWOT dimensions; this offers a layered view of both systemic and professional responses to ongoing digital change. Table 2 summarizes the themes and sub-themes, each aligned with its relevant healthcare system level and analyzed using the SWOT framework.
Summary of Themes, Healthcare Levels, and SWOT Interpretations.
1. Volatility: Organizational Disruption and Acceleration Through Digital Transformation
Participants described how volatility, driven primarily by rapid digital evolution and inter-organizational competition, has shaped the trajectory of healthcare organizations by simultaneously stimulating innovation and posing risks to operational stability. Two main sub-themes emerged from the interviews:
1.1 Technological Competition as a Catalyst for Innovation
Several interviewees identified digital transformation as a key driver of competition between healthcare organizations, stimulating improvements in service quality and accessibility. One participant noted: The more devices or new technology you have, the more patients it will attract to your organization. It has a very strong impact. For us too, whether as clients or as medical staff, it works in our favor and helps us. Another participant reinforced this perspective, stressing the benefits for patient care: In certain ways, yes. . . technology helps us provide better and higher-quality care.
In general, participants perceived this drive for technological leadership as beneficial, fostering a culture of continual advancement and responsiveness to patient needs. Another participant, however, emphasized that technology alone does not guarantee competitive advantage: In my field, I think we already understand that technologies themselves do not lead the competition. What can actually win in competition is service, because technology can always be bought. In fact, technologies alone are not such a strong competitive tool, since everyone can buy them.
These pressures were not perceived as negative but rather as catalysts that pushed institutions to explore novel solutions and expand their capabilities. One participant emphasized the broader impact: Then came Zoom, and from a departmental management perspective it created a whole new world. We now hold structured meetings with multidisciplinary teams, significantly raising the level of our work. For me, this has placed us at the forefront of operating at the highest level.
1.2 Organizational Vulnerability Due to Technological Lag
While digital transformation fostered innovation and institutional advancement, participants also highlighted the risks faced by organizations that adapted slowly or struggled with uneven adoption. Limited access to advanced technologies, insufficient training, and outdated infrastructures were seen as critical vulnerabilities. As one participant explained: There is a lot of technology that is still not adapted to the whole system. Not every place knows how to use this technology. You need very skilled people to use smart technology. . .. The courses we’ve taken over the years constantly need updating.
Another participant pointed to inequities in access and efficiency: The technology is very smart, but it requires skilled people. First of all, it is not available to everyone, only to a limited number of people. And again, some technologies take more time and ease our work, others take less time. . . but mainly, not everyone gets to use them.
These accounts illustrate how technological lag found expression in practical inefficiencies, unequal access, and skill gaps, ultimately undermining organizational capabilities. Institutions that failed to ensure widespread access and systematic training risked falling behind in both service quality and operational effectiveness.
Healthcare Level and SWOT Interpretation
These findings reflect the dynamics at the meso level of the healthcare system, where institutions confront and respond to external technological pressures.
From a SWOT perspective:
Opportunity: The competitive momentum created by digital innovation encourages service development, strategic modernization, and institutional agility.
Threat: Uneven adaptation to digital change threatens organizational sustainability, contributing to financial instability and workforce strain.
2. Uncertainty: Decision-Making Challenges and the Role of Technology in Reducing Diagnostic Ambiguity
Uncertainty emerged as a significant theme in the healthcare professionals’ narratives, encompassing both clinical decision-making and emotional engagement with patients. Participants described how digital transformation simultaneously alleviated some forms of uncertainty, particularly in diagnostics, while reinforcing others, especially in remote care contexts. Two key sub-themes were identified: diagnostic uncertainty and emotional uncertainty.
2.1 Diagnostic Uncertainty and Digital Support
Many participants emphasized how access to digital tools has substantially improved their ability to make timely and informed decisions in ambiguous clinical situations. Technologies such as digital imaging, laboratory test integration, and electronic health records were seen as reducing reliance on intuition and enabling more evidence-based practice. As one participant explained: We do everything on the computer, making it possible to access patient information from anywhere, whether from the HMO or another hospital. . . including imaging, actually viewing the different layers of CT scans, X-rays, ultrasound. . . this greatly improves the way medicine is practiced.
Another participant highlighted how these tools enable real-time collaboration and rapid consultation: You can send ECG images, a video of a child with suspicious movements to check whether the child is having a seizure, or a photo of a rash to a dermatologist. These extraordinary tools are being increasingly used in practice.
This technological ability was particularly valued in urgent settings, where swift access to accurate data is critical. As another participant remarked: For example, if I am doing follow-up today, I want to see the patient’s vital signs, blood tests from this morning and so on, and I would like the hospital system to display this without me having to go back and search for it.
The immediacy of this access was described not only as improving clinical outcomes but also as enhancing the confidence and decisiveness of care providers. This real-time information availability enhances clinical autonomy and supports faster, more informed decision-making under pressure.
2.2 Emotional Uncertainty in Remote Care
Whereas digital tools have improved the technical clarity of clinical practice, participants expressed concerns about the emotional disconnection that often accompanies remote or technologically mediated care. The transition to telemedicine, though deemed necessary at certain times, was seen as compromising the interpersonal dimension of caregiving. As one participant explained: There’s no substitute for face-to-face meetings. You can’t always take responsibility for what you don’t see. It’s a screen, it’s filtered, it’s not the same as seeing with your own eyes.
Another participant reflected on the disproportionate negative impact of technology on vulnerable groups: The people who come from the most difficult backgrounds are the ones most harmed because they don’t understand the system; they experience it as dismissive and humiliating. And when the encounter is not face-to-face, it has the potential to create even more alienation.
Others pointed to the therapeutic value of simple gestures such as physical touch that are lost in remote care: Placing a hand on the patient’s shoulder, seeing how they are - that’s part of the human need. Half of the treatment is just that.
This form of uncertainty is not about medical data, but about presence, empathy, and trust, all elements that are difficult to replicate in virtual settings. Professionals described the tension between achieving efficiency through digital platforms and preserving human contact, particularly with patients in distress or facing chronic conditions.
Healthcare System Level and SWOT Interpretation
These findings are rooted at the micro level of the healthcare system, reflecting the individual experiences of frontline clinicians as they navigate both diagnostic clarity and interpersonal ambiguity.
From a SWOT perspective:
Strength: The use of digital diagnostic tools improves accuracy and responsiveness, supporting confident clinical decision-making.
Weakness: Emotional disconnection in telemedicine settings hinders patient engagement and satisfaction.
Threat: Uncertainty in both medical and emotional domains can compromise care if not proactively managed.
Opportunity: Continued investment in hybrid care models that balances technological precision with human interaction may offer sustainable solutions to the challenges raised.
In summary, the uncertainty faced by healthcare professionals extends beyond clinical data and decision-making. It also includes emotional and interpersonal aspects of care that are disrupted by remote and digital communication. Although digital tools reduce diagnostic uncertainty, they can simultaneously limit the human connection essential to therapeutic relationships. Addressing this issue requires models of care that integrate technological efficiency with genuine human presence.
3. Complexity: Navigating Multisystem Demands and Interdisciplinary Burdens
The theme of complexity emerged strongly from the interviews, with healthcare professionals describing the challenges of operating in an increasingly fragmented digital environment. The complexity was not only technological but also organizational, as manifested in overlapping systems, evolving roles, and increased administrative load. Participants conveyed a sense of constant multitasking and adaptation, often without sufficient structural support. According to one professional: Alongside all the good, we constantly add more and more demands on the nursing staff. . . in the end, what is supposed to support us often becomes very burdensome.
The overlapping of digital tools placed significant strain on day-to-day operations. This cumulative pressure reflected the compounded effects of overlapping systems, blurred professional boundaries, and resource limitations. The following sub-themes illustrate the dimensions of complexity professionals experience in their daily practice.
3.1 System Fragmentation and Parallel Workflows
One of the most frequently mentioned challenges involved working with multiple non-integrated digital platforms. Participants described the strain of having to navigate several systems simultaneously, often repeating the same information across different interfaces. As one clinician observe: Everything is through the computer; software is used for everything. I worked at several places, and each place has its own system.
Another participant highlighted the lack of interoperability between departments: If a department uses the same system as we do, the information transfers automatically, but for example the emergency room does not use our system, so the data is not transferred automatically.
Yet another participant reflected on the burden of duplicating documentation: With patients we use manual documentation, even though everything is also entered into the computer. This allows us to be present with the patient, but it complicates the process because we end up documenting things twice.
This duplication of tasks driven by fragmented digital infrastructure not only consumed valuable time but also introduced risks of data omission and reduced attention to patient care. Additional frustrations stemmed from incompatible systems across organizational boundaries. These misalignments reflected a systemic weakness that undermined the potential benefits of digital documentation.
3.2 Interdisciplinary Role Expansion and Task Burden
Beyond technological complexity, participants noted expanded professional expectations that blurred the lines between clinical, administrative, and technical roles. The digital transformation increased the number of tasks clinicians were expected to perform, often without sufficient support. As one participant commented: When I get stuck with the software or the devices, I call a technician and show him the screen so he can tell me what to do. And if I can’t find a specific form in the digital archive, I ask our secretary, who is younger and much more adept with all the technology and electronic systems.
This reliance on technical and administrative support reflects the growing overlap between clinical care, IT troubleshooting, and bureaucratic demands. A nurse working in an emergency unit added: Every woman who comes to triage - I have to indicate that I gave her guidance. . . it’s just another form to fill out. It wastes time. To me, it’s pure bureaucracy.
Rather than streamlining the work, in some instances digital tools added additional bureaucratic demands to already stretched workflows, reducing opportunities for meaningful clinical interaction. Such accounts highlight the tension between digital documentation requirements and the desire to provide meaningful, patient-centered care.
3.3 Human Resource Gaps and Administrative Exhaustion
The complexity introduced by digital systems was further exacerbated by staff shortages. Participants emphasized the cumulative toll of filling multiple roles while managing fragmented workflows. As one nurse described: Examining the situation over time, I see that nurses are working under unreasonable workloads. It’s really a double-edged sword. There is a lot of good in it, but it is also very burdensome.
This exhaustion was not limited to physical fatigue, but also reflected the cognitive load of juggling incompatible systems, administrative duties, and patient care under increasing pressure. The experience of complexity, therefore, is not simply a matter of organizational design. It is experienced and felt by professionals in the field, shaping their ability to perform effectively, remain engaged, and avoid burnout.
Healthcare System Level and SWOT Interpretation
These findings operate across the micro and meso levels of the healthcare system. While system integration and workflow design are organizational responsibilities, the consequences are felt most acutely by individual staff members.
From a SWOT perspective:
The lack of system interoperability, growing task complexity, and unclear role boundaries constitutes a clear weakness, compromising care quality and efficiency.
The resulting fatigue and disengagement among staff represent a threat to organizational resilience and service continuity.
Nonetheless, identification of these issues reveals an opportunity to restructure workflows, invest in interoperable technologies, and clarify professional roles to better align digital transformation with clinical realities.
In sum, complexity in the digital era is not an incidental feature of modern healthcare, but a defining condition. Addressing it requires more than technological upgrades; it demands deliberate attention to system integration, staff capacity, and the human dimensions of clinical work.
4. Ambiguity: Role Confusion, Inconsistent Practices, and the Human Cost of Digital Transformation
Ambiguity emerged as a central theme in the interviews, capturing the uncertainty, inconsistency, and disorientation that often accompanied the rapid implementation of digital tools. While digital transformation was recognized as inevitable, the lack of clarity around its rollout, expectations, and impact on professional roles generated persistent tension.
One participant reflected on the generational challenges and the stress of adapting to unfamiliar technologies: Every new technology comes with difficulties. We are not a generation born into technology, so we had to learn many of these systems from scratch. . . .. every new tool feels stressful.
Another participant described the lack of sufficient support once new machines were introduced: At first, when the new machines were introduced, I didn’t know how to operate them. After the training ended, I realized I was on my own and had to solve the problems myself. You need to find a solution on your own. . .to figure out what can be done.
This sense of navigating change without adequate preparation demonstrates how ambiguity permeates both operational routines and the broader emotional experience of adapting to digital healthcare. The sub-themes below show how this ambiguity found expression in everyday healthcare practice.
4.1 Inconsistent Understanding and Informal Learning
Many professionals reported being introduced to new digital systems without structured instruction or shared protocols. This lack of standardized onboarding led to divergent interpretations of how systems should be used. One participant observed: I actually define myself as a technophobe, but at work I somehow manage. . . Still, it’s true that there needs to be proper training and implementation before introducing a new system or device to ensure that everyone knows what it’s about, rather than just throwing us into the water.
In the absence of formal guidance, staff often relied on informal peer-to-peer learning. Another participant commented: What’s important is how the technology is explained. Some people need more than explanations; they need hands-on experience. Touching and trying—that’s what works. In my department, because the team is small, I can give individual training. Some need only one training session, others three or four, and some even a week or a month until they really get it.
Even though this approach allowed work to continue, it also resulted in inconsistent practices across individuals and teams. The variability in digital literacy and interpretation reduced workflow efficiency and introduced potential safety risks. Professionals described this inconsistency as frustrating, especially when expected to comply with protocols that were never clearly communicated.
4.2 Generational Gaps in Digital Adaptation
Ambiguity also emerged in how staff members from different generations responded to digital change. Participants highlighted that though younger employees adapted relatively quickly to new systems, many senior professionals struggled to keep pace. As one nurse noted: I’m a young nurse, so it’s easier for me to adjust to these changes, but for others it was really difficult. . . especially the computer part. This generational divide in digital fluency generated operational friction within teams.
Another participant reflected on the toll this change took on older colleagues: I see that the midwives with more seniority get stuck using the technology. It takes them time, it causes frustration and stress, it just makes things harder for them and takes them longer in practice. These challenges often led to uneven task distribution, with younger staff informally absorbing more digital responsibilities.
For some more veteran staff members, the shift to digital tools disrupted long-standing routines and professional confidence. One participant explained: It took much, much longer for the older staff. It was really hard for them, and for us it was a bit easier. It’s really a mindset change. . . especially since their generation wasn’t born with computers. We were trained to treat patients, not machines.
These accounts underscore the human implications of digital transformation when adaptation is assumed but not structurally supported, particularly for experienced professionals who face steep learning curves late in their careers.
4.3 Ambiguity in Human Connection and Communication
Several participants expressed concern about how digital tools have disrupted the human element in healthcare. One interviewee reflected: We must remember that beyond all this technology, there is a patient. . . and sometimes with all this technology, we forget there’s a patient. . . we have less face-to-face time with the patient and we need to dedicate time to them. And this is something I really, really regret.
Others emphasized the emotional disconnect caused by digital mediation. Another participant stated: There’s no substitute for face-to-face meetings. And this needs to be said. Sometimes you can’t take responsibility for what you don’t see. It’s a screen, it’s filtered, it’s not the same as what you see with your own eyes.
These sentiments highlight a growing ambiguity in healthcare, as digital systems prioritize efficiency at the expense of interpersonal depth. For some professionals, this shift increased the burden of emotional labor, as they struggled to maintain patient-centered communication within a system dominated by screens and protocols.
4.4 Fragmented Infrastructure and Uneven Implementation
Ambiguity was further reinforced by inconsistencies in infrastructure and technological availability across departments and institutions. Professionals described how digital tools were introduced unevenly, with some units equipped with updated systems and others still relying on manual methods. One participant commented: Some departments are fully computerized, while others still rely on paper files. In places where computers are not used at all, patients are transferred with their paper charts, and sometimes essential details are forgotten or missing, creating further problems
Another interviewee elaborated: Since we’re in some sort of evolving system, things aren’t consistent and identical everywhere. Yet another participant noted: You experience this more in certain departments in which they’re testing things. . .. Hospitals differ greatly, with government hospitals using one system and hospitals affiliated with the Clalit HMO using another. This fragmentation was illustrated most clearly in the transition between departments. As one participant recounted: After surgery patients go to recovery—another department that does not use computers at all. It’s a problem—patients are sent with paper files, sometimes with the wrong file or missing important notes, and we have to call the department.
These inconsistencies not only slowed down processes but also created uncertainty around preferred practices. The lack of standardization made it difficult to establish clear expectations, leading to fragmented routines and hesitation in using available tools.
4.5 Security and Confidentiality Concerns
Ambiguity extended to digital security and confidentiality practices. Professionals expressed concern about the accessibility of sensitive patient information and the ethical dilemmas arising from insufficient safeguards. One participant reflected: Confidentiality. . . I often meet patients who share very personal things. . . I’m constantly trying to figure out what I can enter into the patient file and what I shouldn’t, to make sure that children and adolescents won’t feel that what they tell me will immediately be read by their parents. I think all these issues of confidentiality are extremely important.
Concerns were not limited to documentation but also included the conditions under which information was recorded and stored. One participant explained: Even if it looks like only you and I are in the meeting, there’s still the issue of medical confidentiality. Some people are unsure; maybe someone is listening or watching behind the screen. They’re not entirely used to this, and it causes discomfort. Another participant added: People are very afraid the information will leak, even though we’re all bound by medical confidentiality. It creates certain trust issues. The information is there, but it still needs to be protected.
These reflections illustrate how the lack of standardized privacy protections and inconsistent system implementation generate uncertainty for clinicians, who must constantly navigate between maintaining ethical standards and operating within unclear digital frameworks.
Healthcare System Level and SWOT Interpretation
The experiences described in this theme span both the micro and meso levels of the healthcare system. At the micro level, ambiguity disrupts clinicians’ daily routines, erodes confidence, and weakens trust in communication structures. At the meso level, uneven implementation of technologies and lack of coordinated training strategies expose institutional shortcomings.
From a SWOT perspective:
The fragmentation in knowledge, workflow, and infrastructure reflects a systemic weakness that diminishes efficiency and increases cognitive and emotional burden.
The risk of disengagement among senior professionals as well as inconsistent practices pose a threat to workforce continuity and patient safety.
Yet these challenges also point to opportunities, particularly in improving training models, standardizing infrastructure, and reinforcing human-centered care within digital environments.
In summary, ambiguity is not a residual effect of digital transformation but rather a central tension that influences how technology is used, interpreted, and experienced. Addressing this ambiguity requires more than technical fixes. It calls for clear communication, inclusive training, and a reaffirmation of the interpersonal core of healthcare.
Discussion
This study explored how healthcare professionals experience and respond to the challenges posed by a VUCA healthcare environment, particularly in the context of ongoing digital transformation. The findings reveal that although digital tools have introduced significant opportunities, such as improved diagnostic capabilities, enhanced workflow efficiency, and greater strategic adaptability, they have also generated new vulnerabilities at both the professional and organizational levels.
These insights are consistent with prior research emphasizing the transformative potential of digital healthcare technologies in enhancing organizational responsiveness and clinical decision-making (Ginter et al., 2018; Harjula et al., 2022). Indeed, from a business administration perspective, a 2025 BCG report outlines how integrating AI-powered tools can significantly upgrade care delivery and operational agility across an entire healthcare organization (Afkhami et al., 2025). These capabilities foster a more responsive organizational structure, reducing latency in diagnosis and treatment and improving overall service delivery. Eastburn et al. (2024) further emphasize that healthcare organizations investing in digital platforms, including interoperable EHRs and analytics frameworks, can realize $200 to 360 billion in net savings globally, driven by improved throughput, reduced duplication, and optimized staff utilization.
From an administrative viewpoint, these investments necessitate new governance mechanisms, such as digital business units and dedicated Return on Investment (ROI) oversight, to ensure capital is efficiently allocated and results are tracked against key economic indicators. Moreover, Deloitte (2024) highlights that when organizations implement robust change-management protocols supported by executive sponsorship and workforce upskilling, they experience higher uptake of digital tools and more sustainable performance improvements. Collectively, these academic and industry insights highlight that digital healthcare technologies, when aligned with business administration principles such as cost–benefit analysis, performance metrics, and governance structures, can significantly heighten organizational responsiveness and improve decision-making quality and efficiency.
At the same time, the findings underscore a recurring tension: Although digital systems contribute to operational improvements, they often introduce unintended interpersonal gaps that complicate the delivery of empathic care. Similarly, the coexistence of fragmented infrastructure and expanding professional roles reflects a deeper challenge: Poor system integration tends to produce role confusion and administrative overload, a pattern observed in earlier literature on digital health implementation (Karni & Reches, 2018; Sheaff & Schofield, 2016).
Volatility, as expressed through uneven adoption of digital tools, aligns with broader patterns of systemic instability driven by technological competition, policy shifts, and economic restructuring (Otter, 2019; Zangrandi et al., 2020). In this context, rapid digital acceleration can serve both as a catalyst for innovation and as a threat to organizational sustainability, especially when institutions lack the infrastructure to support ongoing transformation (Naamati-Schneider & Zaks, 2022).
Uncertainty emerged in two distinct but interconnected forms: clinical uncertainty, which digital systems helped reduce, and emotional uncertainty, which often was intensified by the shift to remote and digitally mediated care. Participants emphasized that technologies such as EHRs, imaging tools, and integrated laboratory data improved diagnostic accuracy and supported faster, more confident decision-making. These experiences are consistent with findings that digital systems can help mitigate ambiguity in high-pressure clinical settings (Harjula et al., 2022).
Conversely, the interpersonal aspects of care were frequently disrupted by the absence of physical presence and reduced interpersonal interaction. Participants described how digital interfaces limited their ability to offer affective presence, read non-verbal cues, and establish therapeutic trust. This emotional disconnection created uncertainty around patient engagement and professional responsibility. These accounts echo broader critiques in the literature concerning the interpersonal limitations of technologically mediated care (Subramanya et al., 2023; Whitten et al., 2010).
The coexistence of increased diagnostic certainty and diminished interpersonal clarity illustrates a central paradox in digital healthcare. Even as systems have evolved to support precision and speed, they have introduced new forms of ambiguity in interpersonal responsibility, therapeutic presence, and patient engagement. Managing this duality requires a shift toward hybrid models of care that integrate the strengths of digital efficiency with the enduring need for human connection.
Complexity was most evident in the participants’ descriptions of fragmented workflows, duplicated documentation processes, and blurred boundaries among clinical, administrative, and technical roles. These findings support Benjamin’s (2010) conceptualization of healthcare as a multidimensional, interdependent system, where digital transformation, if implemented without coordination, can exacerbate rather than resolve inefficiencies. As echoed in Marzaleh et al. (2022), when digital tools are layered atop legacy systems or siloed infrastructures, they may introduce parallel processes that heighten administrative burden. This was particularly salient in resource-constrained environments, in which clinicians reported performing multiple roles simultaneously without adequate support, leading to fatigue, disengagement, and diminished care quality.
Ambiguity emerged in the interviews in multiple and interconnected forms. Participants described inconsistencies in training, unclear expectations around new technologies, and divergent interpretations of digital protocols. These challenges were especially pronounced among senior professionals who had not received adequate preparation for the rapid shifts in digital practice. In line with earlier criticisms by Kuhlmann and Knorring (2014) and Ouschan et al. (2000), these findings underscore the ethical and operational blind spots that can emerge when digital systems are implemented without coordinated professional development or transparent communication.
This finding highlights the need for ongoing workforce development, particularly among senior healthcare staff and administrators, and the creation of supportive digital ecosystems that are secure, interoperable, and equitably distributed (Figueroa et al., 2019; Khan et al., 2025).
From VUCA to Strategic Action: Leveraging SWOT in Healthcare Management
Integrating SWOT analysis into each VUCA dimension offers healthcare organizations a practical framework for managing digital disruption. Building on the findings, which revealed both vulnerabilities and adaptive strategies, SWOT analysis helps reframe the VUCA component not solely in terms of threats but rather as conditions under which internal strengths and external opportunities can be strategically mobilized to mitigate risk and guide innovation.
In the context of volatility, strategically aligned digital transformation enhances institutional agility and competitive advantage. As shown, digital innovation fostered both service improvements and institutional collaboration. Shao (2025) similarly found that organizations that effectively implemented digital initiatives responded more swiftly to external changes and demonstrated innovation in service delivery. These insights affirm that volatility, when met with robust infrastructure and visionary leadership, can drive institutional renewal. Digital platforms, in particular, support cross-institutional collaboration through open innovation ecosystems, enabling real-time data exchange among business stakeholders, joint problem-solving, and value co-creation, as confirmed by studies on telemedicine implementation in Europe in response to COVID-19. Yet the literature also cautions that to unlock these outcomes, healthcare organizations should invest in governance structures and transformational leadership to overcome operational barriers, manage regulatory complexities, and embed digital tools into standard clinical workflows (Naamati-Schneider & Salvatore, 2023; 2024).
In the case of uncertainty, the SWOT lens reveals a dual narrative. Access to real-time data, such as lab results and imaging, reduces diagnostic ambiguity and supports more confident, evidence-based decisions (Brommeyer et al., 2024). Yet as this study underscores, the expansion of telemedicine has intensified emotional uncertainty by limiting clinicians’ ability to offer interpersonal interaction, read non-verbal cues, and build therapeutic trust. These findings highlight an opportunity to develop hybrid care models that integrate technological precision with human-centered engagement (Subramanya et al., 2023).
With respect to complexity, internal weaknesses such as fragmented digital systems, overlapping responsibilities, and limited human resources must be acknowledged. Participants described duplicated documentation, multitasking, and exhaustion resulting from under-integrated technologies. This complexity is echoed by Marino and Diaz Paz (2025), who emphasize the importance of interoperability for patient-centered care, as well as by Borges do Nascimento et al. (2023), who found that workflow fragmentation can lead to clinician burnout. Addressing these challenges requires streamlined processes, system integration, and better alignment between digital tools and staff capacity. Recent applications of SWOT in healthcare, such as in community-based mental health services (Mansuroğlu & Davut, 2025) and digital triage in obstetrics (Ngwenya et al., 2025), illustrate the framework’s utility in linking user needs with organizational capacity. As in the present study, these studies show that strategic responsiveness depends both on environmental awareness and on internal alignment.
Finally, ambiguity, as reflected in inconsistent training, unclear roles, intergenerational digital gaps, and concerns over data security, can be proactively addressed using SWOT. This study found that ambiguity disrupted communication, reduced confidence, and led to uneven adoption of digital systems, particularly among senior staff. Khan et al. (2025) stress the importance of ongoing digital competency development, especially for experienced professionals. At the same time, the creation of secure, standardized, and interoperable infrastructures is essential to reduce ambiguity and build trust in digital healthcare systems. These strategic reflections underscore the complex interplay of technological, structural, and human factors within digital transformation. Analyzing these dynamics using VUCA and SWOT reveals key areas of fragility as well as of resilience in healthcare systems adapting to continuous change.
Lastly, embedding SWOT analysis within the VUCA framework provides healthcare leaders with a multidimensional strategy toolkit that facilitates not only diagnostic reflection but also targeted planning and resource allocation. This integrative approach supports a transition from reactive responses to proactive, value-driven strategies that can enable healthcare systems to remain resilient, equitable, and ethically grounded amid ongoing digital transformation.
Implications for Policy and Practice
Integration of the VUCA-SWOT framework offers a practical foundation for strengthening healthcare systems at the macro, meso, and micro levels as they undergo digital transformation. By linking systemic observations with strategic insights, this study provides actionable guidance for policymakers, institutional leaders, and clinical teams navigating the evolving healthcare landscape.
Macro Level (Policy and System-Wide Governance)
At the national level, health authorities should address the structural inequities that hinder cohesive digital transformation. As the findings show, fragmented infrastructures and inconsistent system adoption create volatility and ambiguity that compromise continuity of care and institutional responsiveness. Standardizing digital platforms and ensuring interoperability across hospitals, HMOs, and governmental sectors are of critical importance. Equally important is fostering equitable access to technology along geographic and socioeconomic lines. Investment in national frameworks for digital literacy and cybersecurity, particularly for aging workforces and under-resourced regions, can mitigate systemic threats and promote sustainable innovation (Figueroa et al., 2019; Marzaleh et al., 2022). Applying the VUCA-SWOT lens at this level facilitates strategic regulation that is both resilient and future-oriented.
Meso Level (Organizational Strategy and Management)
At the institutional level, digital transformation should be treated as a long-term strategic process requiring continuous adaptation. The study identified complexity in the form of duplicated documentation, parallel workflows, and blurred role boundaries—challenges that reflect underlying organizational weaknesses. Addressing such challenges demands a shift toward integrated systems, clear role delineation, and streamlined workflows. From a business administration perspective, workforce development in the healthcare context should prioritize tailored digital competency training for both professionals and administrators to serve as a critical enabler of responsive, resilient organizations. Empirical data from an EU-wide needs-assessment study reveals that while over half of healthcare workers report basic digital skills, only one in five effectively uses advanced tools such as telemedicine and smart data systems in clinical contexts. Learning uptake is uneven despite technology awareness (Lapão et al., 2024).
A broader systematic review published early in 2025 highlights that interventions such as short-term targeted training, skills assessments, and structured managerial curricula effectively enhance digital readiness and adoption among healthcare administrators and professionals (Smith et al., 2025). Complementing this, studies focusing on healthcare administrators affirm the value of a multi-tiered workforce development model with formal curricula, workplace-embedded learning, and credentialing to cultivate digital leadership competencies aligned with organizational transformation (Chen et al., 2024). This implies that capital invested in digital tools should be matched by investments in human capital, setting clear ROI metrics and integrating performance-driven training governance. Organizations that employ such policies can bridge skill gaps (evident in OCED data tracking demands for AI, telehealth, and data analytics competencies) and thereby enhance institutional agility, reduce adoption resistance, and bolster long-term efficiency (Manca & Eslava, 2025). Therefore, institutions should embed SWOT analysis into routine strategic planning to proactively identify risks, optimize resource allocation, and align technological capabilities with operational needs (Marino & Diaz Paz, 2025).
Micro Level (Clinical Practice and Professional Experience)
At the level of day-to-day clinical work, the focus must remain on preserving the human dimension of care within increasingly digital environments. As reflected in the findings here, professionals struggle to maintain empathy, interpersonal presence, and therapeutic trust when care is mediated by screens. Hybrid care models that combine digital efficiency with in-person connection offer a viable path forward. Supporting this transition requires more than technical training; it also entails fostering communication skills, emotional intelligence, and interpersonal awareness within virtual care settings (Subramanya et al., 2023). Role clarity, emotional support, and collaborative team culture are essential for reducing burnout and ensuring that care remains ethically grounded and patient-centered.
Limitations
Even though this study was conducted in a specific healthcare context, the challenges and responses it identified reflect broader patterns seen in digital health transformation across the globe. The qualitative design and purposive sampling enabled in-depth exploration of professional experiences, though it did not aim for statistical generalizability. Nevertheless, the recurring themes, such as fragmented infrastructures, transformative governance, organizational change, evolving professional roles, and the emotional dimensions of care are not unique to one system and may resonate across diverse healthcare settings undergoing digital transition. The sample included a variety of clinical roles, although perspectives from non-clinical actors such as IT personnel or policy implementers were limited, potentially constraining analysis of system-wide coordination. Additionally, although the abductive analytical approach supported theoretical integration, it also involved interpretive processes shaped by the researchers’ engagement with the VUCA and SWOT frameworks. Nonetheless, the findings offer transferable insights that may inform strategic responses to digital transformation in similarly complex healthcare environments.
Conclusions and Future Directions
This study advances understanding of how healthcare professionals and administrators experience and respond to the challenges of digital transformation within a VUCA environment. By integrating the VUCA framework with SWOT analysis, it offers a multidimensional lens through which to assess not only the opportunities afforded by digital tools, such as enhanced diagnostic precision, improved workflow efficiency, and strategic adaptability, but also the systemic and human vulnerabilities they introduce, including role confusion, emotional disconnection, fragmented infrastructures, and ethical uncertainty. The findings demonstrate that the effects of digital transformation are unevenly distributed across all healthcare levels. This layered impact demands differentiated strategies tailored to institutional capacity, professional readiness, and patient needs. Applying SWOT as an interpretive tool helped uncover strengths to be leveraged, weaknesses to be addressed, and opportunities for improvement within a rapidly evolving healthcare landscape.
Future research should extend this integrative model to diverse healthcare systems and organizations, including under-resourced settings, private institutions, and international comparisons. Longitudinal and interdisciplinary studies can further illuminate how organizations build resilience, preserve interpersonal care, and adapt ethically to ongoing digital disruption.
Ultimately, ensuring that digital transformation supports rather than fragments the mission of care will require not only technological innovation but also continuous investment in professional development, system integration, and human-centered design. From a business administration viewpoint, this demands strategic alignment between digital initiatives and organizational goals, supported by robust governance, performance metrics, and sustainable resource allocation to maximize value creation and institutional resilience.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee of the first author’s College as meeting the requirements of ethical research.
Author Contributions
LNS: Conceptualization, data curation, methodology, writing—original draft preparation writing—reviewing and editing. FPS: Conceptualization, writing- original draft preparation writing—reviewing and editing. The authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon request.