
Abstract
Historically, African American women have experienced racial disparities in miscarriage, stillbirth, and infant mortality rates. Yet, little attention has been given to stressors that African American women may experience prior to, during, and after experiencing fetal/infant loss. This study provided an opportunity for African American women to describe their lived experiences of stressors prior to, during, and after experiencing each type of fetal/infant loss. Semi-structured interviews were conducted with seven African American women. Each participant experienced miscarriage, stillbirth, and infant mortality and were 18 years of age or older. Recruitment occurred in 2019 in a county in Northeast Ohio and data were analyzed using descriptive coding and thematic analysis. Four themes identified how these African American women navigated stressors prior to, during, and after experiencing each type of fetal/infant loss: (a) social support, (b) grief, (c) internal conflict, and (d) pregnancy, delivery, and death of child. Our findings expand the literature by being an innovative study may bring awareness and influence programs that assist African American women during their experience with fetal/infant loss.
According to guidelines for perinatal care published by the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists (Kilpatrick et al., 2017, p. 618), fetal loss is defined as “death before the complete expulsion or extraction from the mother of a product of conception, irrespective of the duration of pregnancy that is not an induced termination of pregnancy.” When examining different types of fetal loss, the death of a fetus before 20 weeks of gestation is considered a miscarriage, while fetal loss at or after 20 weeks of gestation is referred to as stillbirth (Kilpatrick et al., 2017). Whereas, the death of an infant that occurs within the first year of birth (i.e., less than 365 days) is defined as infant mortality (Kilpatrick et al., 2017). Therefore, we adopted these definitions and categorized fetal/infant loss into three types: (a) miscarriages, (b) stillbirth, and (c) infant mortality.
Recent studies suggested that racial disparities persist in miscarriages, stillbirths, and infant mortality rates across races and ethnicities in the United States, particularly when comparing African Americans and Whites (Brown Speights et al., 2017; MacDorman & Gregory, 2015; Page et al., 2018; Silver et al., 2007). Compared to White women, African American women experienced an increased risk of miscarriage, especially in gestational weeks 10–20 (Mukherjee et al., 2013). Similarly, African American women were twice as likely to experience stillbirths in comparison to White women (MacDorman & Gregory, 2015; Page et al., 2018; Silver et al., 2007). When examining disparities in infant mortality rates, data revealed that infant mortality rates for African Americans were 10.75 per 1000 live births compared to 4.63 per 1000 live births for Whites in 2018 (Ely & Driscoll, 2020).
The loss of an infant, whether occurring prior to, during, or after birth, can be considered a traumatic event to parents (Christiansen, 2017). No matter the type of fetal/infant loss (i.e., stillbirth, miscarriage, and infant loss) experienced, such history may potentially impact health status and has been shown to have substantial psychological implications (Davoudian et al., 2021; Kersting & Wagner, 2012). African American women who have experienced miscarriage, stillbirth, or infant mortality may encounter stressors related to self-blame, shock, suicidal thoughts, grief, and sleep disturbance (Boyden et al., 2014; Côté-Arsenault et al., 2019; Kavanaugh & Hershberger, 2005). These stressors were further complicated with abnormally high levels of anxiety during the loss (Côté-Arsenault et al., 2019).
In addition to the impacts of such indelible events, scholars examined the risk factors of fetal/infant loss among African American women (Alio et al., 2010; Dominguez, 2011; Kiely et al., 2011). Research demonstrated racism embedded in the lives of African American women was as an underlying factor of African American women’s persistent reproductive disadvantage (Alio et al., 2010; Dominguez, 2011). African American women were often exposed to oppression and disadvantage throughout their lifetime (Crenshaw, 1990). Moreover, researchers have asserted repeatedly that more studies are needed to apply more complex approaches for investigating the complexity of persisting racial disparities in fetal/infant loss (Alio et al., 2010; Boyden et al., 2014; Dominguez, 2011; Reno & Hyder, 2018). Specifically, studies examining the associations between race, racism, and fetal/infant loss and considering the social contexts of racism across all levels in African American women’s life are needed. However, qualitative research using a theory focused on racism to examine race, racism, and racial disparities in fetal/infant loss is sparse. Therefore, the current study used Critical Race Theory (Crenshaw et al., 1995) to better understand the experiences of African American women prior to, during, and after each type of fetal/infant loss, and the perceived stressors associated with their fetal/infant loss experiences.
Critical Race Theory
A lens of the Critical Race Theory has been beneficial to examine the stressors African American women have been confronted with throughout fetal/infant loss experiences and thus have provided directions to diminish the racial disparities in fetal/infant mortality. Critical Race Theory emerged in response to the critical legal studies and racial feminism movements during the mid-1970s (Delgado & Stefancic, 2001). The theory was originally proposed in the field of legal studies, and has been adopted in various disciplines, such as anthropology, history, sociology, philosophy, and politics (Delgado & Stefancic, 2001; Mitchell & Stewart, 2013). The aim of Critical Race Theory is not merely to elucidate the structure of racial power, but also to transform social power hierarchies and social situations for social justice advancement (Crenshaw, 2010; Delgado & Stefancic, 2001). Additionally, Crenshaw (2010) stated that Critical Race Theory in the current time undertakes the task of generating an inventory of critical tools that have been fashioned by generations of Race Crits effectively replicates across disciplines the construction of Critical Race Theory within one discipline. There are four assumptions of Critical Race Theory: (a) racism is endemic to be a part of American society, encompassing all people and experiences, (b) it is crucial to understand racism through the experiential knowledge of Black, Indigenous, and People of Color, (c) narratives (e.g., allegories, parables, pungent tales) are a central way to present experiential knowledge in detail, and (d) there is a need for interdisciplinary collaborations to challenge, assert, and continuously develop Critical Race Theory framework (Delgado & Stefancic, 2001; Martinez, 2014).
Applying Critical Race Theory principle to explore the perceived stressors surrounding fetal/infant loss events adds historical and socioeconomic contexts. When stressors are noted, these contexts widen and deepen the understanding of stressors prior to, during, and after the occurrence of fetal/infant loss events, as well as the intensity of stressors. For example, interview questions were constructed to center on African American women’s lived experiences to examine stressors associated with fetal/infant loss. Additionally, the tenet of “voice of color” (Delgado & Stefancic, 2001, p. 9) provides an opportunity for those with minority status to voice their unique stories with oppression and helps transform the oppressed situation (Crenshaw et al., 1995; Delgado & Stefancic, 2001). In this study, African American women voiced their experiences of fetal/infant loss and the perceived stressors through semi-structured interviews and thematic analysis.
Researchers have indicated that racial identity and socioeconomic status were two of the important predictors in psychological distress among African Americans (Mouzon et al., 2016; Willis & Neblett, 2019). Adverse impacts of racism were found embedded within multiple aspects of society, such as health status, economic status, and access to desirable resources like housing and healthcare. (Williams & Mohammed, 2013). The stressors that were relevant to African American women were categorized into three areas: race-related stressors, socioeconomic related stressors, and familial-related stressors (Alio et al., 2010; Brown et al., 2017), which are reviewed in the subsequent sections.
Race-Related Stressors
African American women were more likely to experience acute and chronic stress compared to White women due to race-related stressors (Hogue & Bremner, 2005; Kavanaugh & Hershberger, 2005). Alio et al. (2010) used the ecological model to examine stressors associated with fetal/infant loss disparities between African American and White women. Findings revealed that racism and discrimination impacted African American women’s health outcomes and contributed to adverse birth outcomes, specifically miscarriage, stillbirth, and infant mortality (Alio et al., 2010). Further, Hogue and Bremner (2005) suggested early in life or ongoing racism-related stressors (e.g., interpersonal racism experiences, race-associated income differentials and living environment) were a potential cause of fetal/infant loss for African American women.
Race-related stressors carried over into the medical care that African American women received, often in the form of discrimination, implicit bias, and color blindness. Mushonga et al. (2020) stated that race-related stressors kept African American women from seeking formal services such as mental health providers or medical providers. Instead, African American women sought support through informal services such as family, friends and clergy. While informal support services can be helpful, they can potentially keep African American women from vital medical services. Daoud et al. (2022) found discrimination towards ethno-racial minorities in maternity wards rampant. The authors cited that poorer health outcomes for women and newborn babies were linked to implicit and explicit discrimination due to medical providers’ clinical decision-making being hindered and minority patients not receiving high quality medical care. Several authors expanded on implicit bias by discussing the impacts of the medical field being “colorblind.” Color blindness and lack of empathy led White medical providers to shift the narrative from racism as the source of health disparities to the “mother blame” narrative, which suggests that the poor birth outcomes are due to the mother’s poor choices such as smoking or not seeking prenatal care (Cunningham & Scarlato, 2018; Hardman and Kozhimannil, 2019; Janevic et al., 2020).
Socioeconomic Related Stressors
Socioeconomic factors have been another major stress contributor to African American women experiencing miscarriages, stillbirths, or infant mortality (Brown et al., 2017). These factors include living in lower socioeconomic neighborhoods, receiving public assistance, and experiencing financial hardship (Alio et al., 2010; Boyden et al., 2014; Brown et al., 2017; Fiscella, 2004; Kavanaugh & Hershberger, 2005). There was a positive association found between high poverty and infant mortality rates (Sims et al., 2007). Financial challenges are often a non-stop, continuous issue from the beginning of a pregnancy until long after the loss of the fetus/infant (Brown et al., 2017). When parents were unemployed, the odds of miscarriage significantly increased (Maconochie et al., 2007), the risk of stillbirth increased (Hogue et al., 2013), and infants were at greater risk of experiencing infant mortality (Boyden et al., 2014).
Furthermore, those living in poverty and the working poor continued to have low rates of health insurance (Entress & Anderson, 2020). This issue was not by choice, but due to policy decisions rooted in racism (Entress & Anderson, 2020;; Snowden & Graaf, 2019). The Affordable Care Act sought to expand Medicaid fully; however, multiple states with disproportionately high populations of African Americans declined to expand Medicaid due to biases towards the “Undeserving Poor.” This act prevented millions of African Americans from accessing needed health care and health disparities such as miscarriages, stillbirths and infant mortality continued to widen (Entress & Anderson, 2020;; Snowden & Graaf, 2019).
Familial-Related Stressors
In addition to race and socioeconomic related stressors, familial-related stressors have been associated with fetal/infant loss (Boyden et al., 2014; Brown et al., 2017). These include familial-related life events and the quality of the relationships among family and partner (Boyden et al., 2014). Research has determined that negative familial-related life events (e.g., illness or death of other close family members) and deficient familial and partner relationship quality (e.g., unstable partnerships, violence, death of other close family members) increased miscarriage, stillbirth, and infant mortality rates among African American women (Brown et al., 2017; Fiscella, 2004; Kavanaugh & Hershberger, 2005). Moreover, marital status has been found to be a risk factor for stillbirth (Hogue et al., 2013). Unmarried women or women residing with a partner were at an increased risk for miscarriage compared to married women (Maconochie et al., 2007). Additionally, stressful familial-related life events (e.g., death in the family) and poor family relationship quality (e.g., lack of support) increased African American parents’ burdens following a fetal/infant loss (Boyden et al., 2014).
Current Study
In the past, Critical Race Theory has been used to examine and illustrate current racial phenomena including healthcare, housing, social justice, and education disparities (Freeman et al., 2017). In respect to gaining a better understanding of African American women’s stressors prior to, during, and after experiencing each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality, Critical Race Theory helps explain how racial identity might intersect and link lived stressors with fetal/infant loss experiences. Further, only holistic lenses, such as the one provided through Critical Race Theory, can address the impact of oppression (Lens, 2021). Therefore, Critical Race Theory fits with the study’s purpose because its central idea is to understand and eliminate disparities with experiential knowledge of Black, Indigenous, and People of Color. Critical Race Theory was applied to the interview guide and findings to focus the study on examining how stressors in societal, economic, and familial aspects shaped fetal/infant loss experiences among the African American women and inform future interventions and policy development.
While previous research has examined possible factors for miscarriage, stillbirth, and infant mortality and their impacts (Brown et al., 2017; Hogue & Bremner, 2005; Kavanaugh & Hershberger, 2005; Murphy & Cacciatore, 2017) most had other foci. Some research explored the loss experiences broadly with general terms (e.g., fetal or infant mortality, pregnancy loss) and others addressed losses with a single term (i.e., miscarriage, stillbirth, or infant mortality; Brown et al., 2017; Hogue & Bremner, 2005; Murphy & Cacciatore, 2017; Van & Meleis, 2003). No identified qualitative research has examined the impacts of the stress African American women experienced who have suffered all three types of fetal/infant loss (i.e., miscarriage, stillbirth, and infant mortality). Therefore, this study aims to gain a better understanding of African American women’s stressors prior to, during, and after experiencing each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality using Critical Racial Theory.
Two research questions guided this study: (a) How do African American women describe their stressors in relation to their lived experiences with all three types of fetal/infant loss and (b) How have their perceptions of these stressors changed over time? The purpose of this study is to explore the perceived stressors experienced by African American women who have suffered all three types of infant loss, a significant phenomenon not previously explored in the literature. The goal of this study, therefore, is to gain a deeper understanding of African American women’s stressors prior to, during, and after suffering each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality. As such, the significance of this study is that it will extend and provide context to the current data on fetal, infant, and maternal health.
Method
Overview of Study
This research study is part of a larger study consisting of 150 African American men and women who experienced miscarriage, stillbirth, and/or infant mortality. However, present study consisted of seven African American women who specifically experienced all three types of fetal/infant loss (miscarriage, stillbirth, and infant mortality). Based on guidance from Malterud et al. (2016) the sample size was considered adequate to obtain sufficient information power. Eligibility criteria required participants to (a) be African American, (b) be 18 years of age or over, (c) reside in a county in Northeast Ohio, and (d) to have experienced each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality. These criteria were based on prior research (a) demonstrating a higher rate of infant mortality in Ohio than most other states (Centers for Disease Control & Prevention, 2021; Kids Count Data Center, 2020), (b) revealing that disparities in infant mortality rates in Ohio among African Americans to be almost three times greater compared to White women (14.3 versus 5.1 deaths per 1000 births in 2019, respectively; Health Policy Institute of Ohio, 2021), and (c) highlighting a significantly higher infant mortality rate among African American women compared to White women within a Northeast Ohio county, where the study was conducted (First Year Cleveland, n.d.).
Research Design
The authors used interpretive and descriptive qualitative research methodology, where the researchers are foremost interested in understanding how participants make meaning of a situation or phenomenon, use inductive data analysis, and develop a descriptive outcome (Merriam & Grenier, 2019; Sandelowski, 2000). To explore the phenomenon of African American women’s experiences with all three types of fetal/infant loss (miscarriage, stillbirth, and infant mortality), the research team used semi-structured interviews because they allowed researchers the opportunity to ask participants open-ended and follow-up questions based on responses (Fylan, 2005; Saldana, 2016; Weiss, 1994) by providing researchers the ability to deviate from the interview guide when necessary to contextualize participants’ narratives (Fylan, 2005; Weiss, 1994). The interview guide was prepared in advance from literature to gather in-depth data and provided the research team with greater insight into African American women who have experienced all three types of fetal/infant loss (miscarriage, stillbirth, and infant mortality). Narratives are an essential way to present the experiential knowledge of Black, Indigenous, and People of Color, which is one of the Critical Race Theory assumptions (Delgado & Stefancic, 2001; Martinez, 2014). Thus, Critical Race Theory was compatible with the semi-structured interviews by ensuring participants could tell their stories/experiences.
Procedure
Institutional Review Board approval was obtained by the authors’ institution prior to participant recruitment. All participants were recruited via snowball sampling through social media recruitment, and from various community agencies, churches, hair salons, and auto shops located in a county in Northeast Ohio. Recruitment strategies included flyers posted at the various recruitment sites, social media, and community agencies’ webpages.
Interested participants were directed to contact the community research coordinator to determine eligibility. Eligible participants who agreed to participate were instructed to complete an electronic informed consent and online demographic questionnaire prior to their scheduled interview. The community research coordinator scheduled all interviews.
All interviews were conducted via telephone for convenience and availability of the interviewees. Two members of the research team conducted the interviews. The interviewers were African American women allowing for a “sister-to-sister talk” to occur, which is where the interviewer has similar characteristics to the participant to increase trust during interviewing (Few et al., 2003). On the predetermined date and time, an interviewer called the participant and conducted the interview. Each interview began with an explanation of the study procedures, answered any participant questions, and reminded the participant that the interview would be audio-recorded. All participants were assigned an interview number at the beginning of the interview allowing the researchers to match demographic questionnaires to participant interviews while protecting participants’ identities and confidentiality. Interviews lasted approximately 30–45 minutes in length. At the end of each interview, the participant was thanked and provided a $100 gift card.
Participants
Demographic Characteristics of Participants (N = 7).
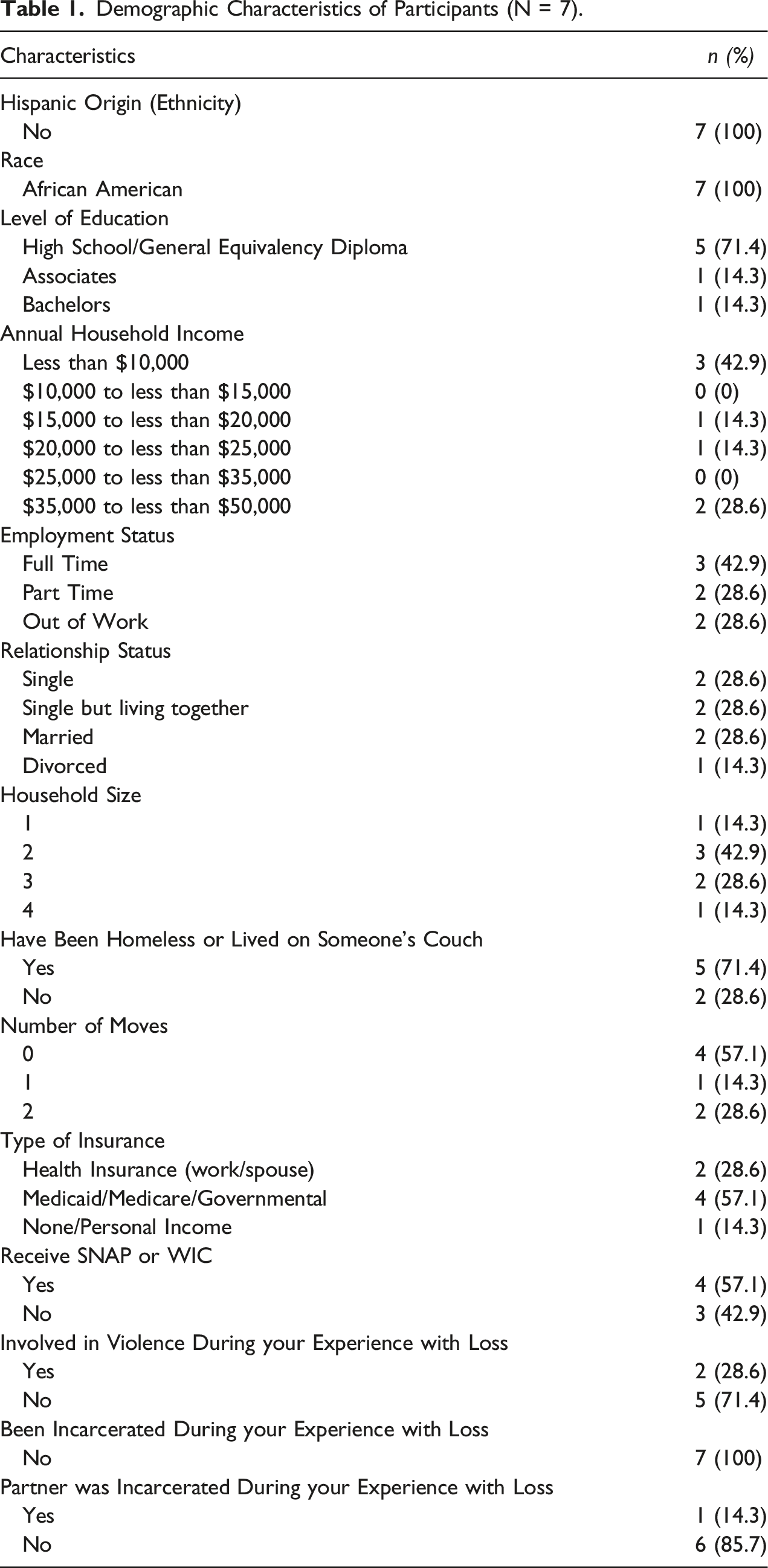
As for type health insurance type, the majority of women (n = 4) had Medicaid, Medicare, or governmental insurance, two had health insurance through work or spouse, and one had no health insurance. The majority of women (n = 4) had or were receiving Supplemental Nutrition Assistance Program or Women Infant and Children benefits. During their experience with loss, most (n = 5) did not report being involved with violence.
Measures
A 36-item electronic questionnaire was created that assessed participant demographic characteristics at both the time of the loss and the time the study was conducted. These demographic questions included age, gender, race and ethnicity, educational attainment, annual household income, employment status, relationship status, housing situation and stability, zip code, health insurance and supportive services, violence, incarceration, and fetal and infant mortality.
Interview Protocol
The research team developed a semi-structured interview guide to use during interviews based on the following research questions: “thinking back, what were your biggest stressors during your experience with loss,” and “currently, what are your biggest stressors regarding your loss?” The interview protocol was developed using a modified interview protocol refinement framework suggested by Yeong et al. (2018). The research team applied the following three steps when finalizing the interview guide: (a) examined the research question and the interview questions to ensuring alignment, (b) conversed with individuals from a community-based agency of a similar background as the participants for question recommendations, and (c) sought feedback from a community-based agency focused on reducing African American fetal/infant loss rates (Yeong et al., 2018).
Critical Race Theory provided additional guidance as the research team developed the interview guide. An important construct of Critical Race Theory is understanding the experiential knowledge of Black, Indigenous, and People of Color through narratives. Semi-structured interviews allowed the research team to explore deeply personal and sensitive subject matter about experiencing fetal/infant loss. Critical Race Theory has been used to explain the intersections and impacts of structural forces (e.g., race, economics, and social policy) on various public health issues among African Americans (e.g., HIV testing, family formation and fatherhood, and breastfeeding experiences; Ford & Airhihenbuwa, 2010; Knox-Kazimierczuk et al., 2021; Lemmons & Johnson, 2019). Therefore, questions in the interview guide were created to explore the stressors (i.e., social, economic factors) that interweave a racial group’s (i.e., African American women) experiences in miscarriage, stillbirth, and infant mortality.
Data Analysis
Audio files were transcribed verbatim using QSR International’s NVivo 12 transcription software and checked for accuracy by listening to the recording and editing the transcript. While assessing the accuracy of the transcripts, one interview file was found to have poor audio quality and was, therefore, not used in the qualitative analysis. Quantitative questionnaires were inputted into IBM’s SPSS Statistics for Windows, Version 25. Participants who indicated they had experienced each type of fetal/infant loss (miscarriage, stillbirth, and infant mortality) were analyzed separately for this study. Each of these selected transcripts was de-identified and inputted into QSR International’s NVivo 12 qualitative data analysis software for analysis. All authors immersed themselves within the transcripts by reading each transcript several times.
After reading the transcripts, descriptive coding followed by thematic analysis was completed (Saldana, 2016). Descriptive coding assigns labels (such as a word or short phrase) to summarize the basic topic of the data passage (Saldana, 2016). After descriptive coding, thematic analysis, an extended phrase or sentence identifying what the unit of data is about or means, was used to develop overarching themes from the data corpus (Saldana, 2016). Both analysis types were deemed appropriate for this research study due to the purpose being exploration of participant experiences. To verify findings, authors independently coded and then discussed each code until consensus was reached. Each theme and subtheme were reviewed by the entire research team who then developed final overarching themes through consensus.
Results
Definitions and Examples of Themes (N = 7).
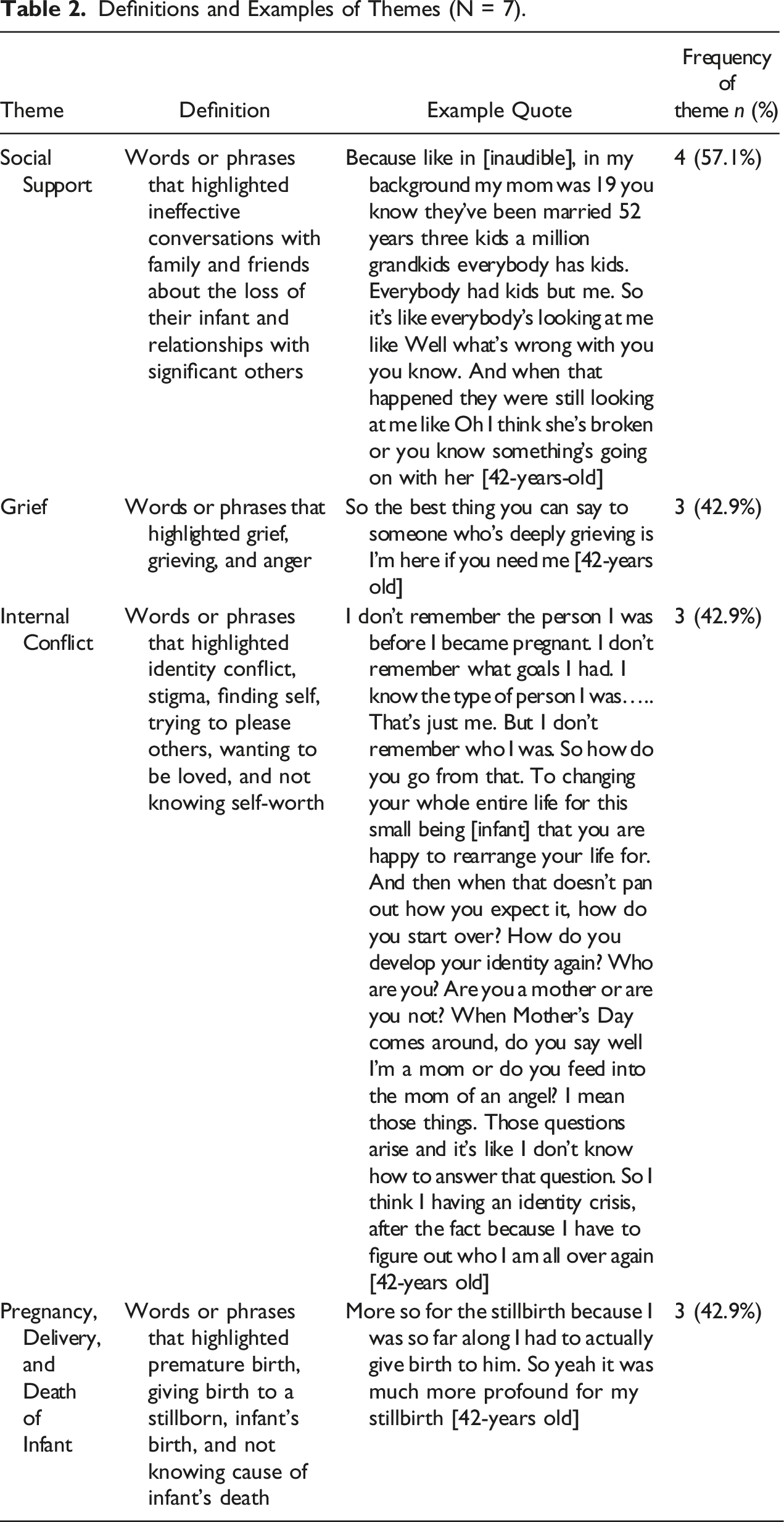
Theme 1: Social Support
Sixty-six percent (n = 4) of participants indicated that social support was a common stressor they experienced after their losses. Interview data coded in this category included participants’ words or phrases that highlighted ineffective conversations with family and friends about the loss of their infant and relationships with significant others.
When examining ineffective conversations with family and friends, participants mentioned the ways in which others would speak and their fear of having conversations with family and friends. For instance, a 42-year-old participant named Erica stated: It’s people not knowing what to say. That would be one of my greatest stressors…People would say things like, ‘You don’t want no kids, they’re a headache’ or ‘You don’t want this headache’ or you know different n things like that. His mom passed, I went over with a bottle to comfort him and that’s how I got pregnant. So, 4 months later I’m like oh we’re having a child and we were already struggling because he had an estranged wife. They had been living apart for two years. So technically, he was still married. So that caused a lot of stress on me.
Furthermore, 33 percent (n=2) of participants indicated that relationships caused stress during and after experiencing each type of infant loss: miscarriage, stillbirth, and infant mortality. A 42-year-old woman named Angela had a particularly powerful statement that illustrated how ineffective and stressful conversations could be. She stated: But I think that that's probably one of my biggest stressors like people trying to comfort me but not really knowing how, that the way they're trying to comfort me is counterproductive. Like … they'll say something like ‘well God wanted an angel.’ And you want to take them in a room with their, and I actually did this, my friend to her world in her room where all the kids were and I’d say ‘pick one.’ And she was like ‘what do you mean?’ I'm like ‘pick one. If God wanted an angel, pick one of your kids to go back to God.’ And she she kind of saw how that how that could come across. And I'm like ‘you have five. I only have one, so imagine the grief that I feel.
Theme 2: Grief
Fifty percent (n=3) of the participants’ responses were to stressors related to grief, which was predominately present after experiencing each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality. Interview data coded in this category included participants’ words or phrases that highlighted grief, grieving, and anger. A 39-year-old participant named Michelle said, “I needed to deal with the grief.” Likewise, a 42-year-old participant named Angela added, “I didn’t understand why did God take my baby from me.”
Another participant (aged 59) named Mary expressed dealing with her grief “annually, especially on his date of birth.” A 42-year-old woman named Erica simply said, “I miss him.” Erica elaborated and expressed frustration with people not understanding why she was still grieving the loss of her child. She said, “People who have the mentality of you just got to get over it. I’ve had someone tell me like, man that happened five months ago or it happened a year ago, are you still on that?”
Theme 3: Internal Conflict
Fifty percent (n = 3) of the participants’ responses were to stressors related to internal conflict in general and 33 percent (n=2) discussed internal conflict as being a stressor specifically before and after experiencing each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality. Interview data coded in this category included participants’ words or phrases that highlighted identity conflict, stigma, finding self, trying to please others, wanting to be loved, and not knowing self-worth. A 49-year-old participant named Abigail said, “I wanted to be on my own. I was trying to find myself.” Similarly, another 39-year-old participant named Michelle added, and performing self-care on myself. That was a big big factor. I was trying to be superwoman. Trying to do everything trying to run a household take care of a baby. You know you know keep my hair up and going to work. That was one of the biggest stressors.
A 42-year-old woman named Erica internalized how her young age created stress for her before she experienced her miscarriage, stillbirth, and death of her child. She explained the following: well I was young, I wanted to be on my own. I was trying to find myself. Didn’t have it didn’t get the proper education. I just wanted to be loved. Just wanted to be trying to seek the not settle in for anything. Not knowing my worth. Not knowing my worth. Just trying to please everybody.
Michelle, aged 39, further described the internal conflict she experienced before and after experiencing her miscarriage, stillbirth, and death of her child. Prior to her loss, she discussed that “I had poor time management. I was trying to be superwoman.” After her loss, she expresses guilt for not having better time management skills, and the impact that it had on her, “But now sitting here looking back, I wish I would have done what I’m doing now back then because I would have dealt with the loss instead of letting it linger.”
Theme 4: Pregnancy, Delivery, and Death of Child
Fifty percent (n = 3) of participants’ responses were to stressors related to pregnancy, delivery, and death of a child. Interview data coded in this category included participants’ words or phrases that highlighted premature birth, giving birth to a stillborn, infant’s birth, and not knowing the cause of infant’s death. This theme was the only theme that all was discussed at all three timepoints: before, during, and after a miscarriage, stillbirth, and loss of an infant. The oldest participant, 59 years old named Mary, described how long she and her partner had tried to have children. “We had tried for a couple of years to get pregnant and having to deal with endometriosis and having treatment before” was stressful. She further described the uncertainty that she experienced during her loss. “Part of my stress at that time was will I’m able to have a family you know. The natural way. I should say. So that was a major stress.” The same participant also shared the stress that came with the uncertainty surrounding her loss. “The biggest stress was not knowing. Having a definitive reason that they have to do is cause of death. And just being fearful stressing over.” Finally, the youngest participant, a 22-year-old woman named Brittany, described how the stress concerning future pregnancies remains years after experiencing each type of infant loss. She pondered “am I ever going to be able to get pregnant again?”
Discussion
The purpose of this study was to gain a better understanding of African American women’s stressors prior to, during, and after suffering each type of fetal/infant loss: miscarriage, stillbirth, and infant mortality using Critical Race Theory. Two research questions guided this study: (a) How do African American women describe their stressors in relation to their lived experiences with all three types of infant loss and (b) How have their perceptions of these stressors changed over time?
Our findings expand the literature by being one of the first studies to examine African American women who have experienced all three types of fetal/infant loss and provide a better understanding of stressors prior to, during, and after experiencing each type of loss. Four themes emerged: (a) social support, (b) grief, (c) internal conflict, and (d) pregnancy, delivery, and death of a child. Ultimately, these themes reveal how the stressors impacted women before, during, and after their loss, while also bringing to light an intimate narrative of these women’s experiences with multiple fetal/infant loss.
Study participants stated that social support was the largest stressor and was predominantly experienced during and after their fetal/infant loss, which is consistent and expands previous findings for women who only experience one type of loss (Cacciatore et al., 2009). When miscarriage, stillbirth, or infant mortality is discussed with family and friends, conversations are often ineffective due to women feeling social pressure to move on, forget their unborn child, or have another child (Cacciatore, 2013). Further, pregnant women who experienced low levels of partner support during early pregnancy had higher levels of pregnancy-related anxiety and depression (Cheng et al., 2016). High level of social support was also found to reduce psychological distress and improve wellbeing of pregnant women, especially among pregnant African American women who reported having experienced racial discrimination, including in the healthcare system (Giurgescu et al., 2017). These findings suggest that African American women who experienced each type of fetal/infant loss need increased, yet effective and appropriate social support to reduce stressors associated with fetal/infant loss, including assistance from prenatal care providers.
Participants experienced grief after all three of their fetal/infant losses and is consistent while also expanding literature on women who experienced only one type of fetal/infant loss (Farren et al., 2020). Although not having built up a relationship with their infant, grief after pregnancy loss does not differ significantly in intensity from other loss scenarios (Kersting & Wagner, 2012). Despite experiencing similar levels of grief, women who experience a miscarriage, stillbirth, or infant mortality often feel disenfranchised from the grieving process because healthcare professionals and society minimize their loss by not considering it to be as painful as losing an older child (Lang et al., 2011). These findings suggest that it is even more critical to validate grief women experience after losing multiple children to miscarriage, stillbirth and infant mortality. Additionally, care institutions and providers should increase their counseling services and initiatives to help African American women who experience multiple types of fetal/infant loss.
When examining internal conflict, participants stated that they experienced this stressor in general as well as specifically before and after all three fetal/infant loss types. Stigma was noted as a major source of internal conflict. Prior research confirms that stigma and the culture of silence surrounding miscarriages prevented women from seeking needed support to address grief and stress (Bellhouse et al., 2018; Pollock et al., 2021). For women experiencing infant mortality, lack of validation by health or social service professionals, family members, or community networks was a major source of stress (Watson et al., 2019). This minimization, even if unintentional, had dire consequences when committed by healthcare professionals as it reduced their ability to recognize and support women following fetal/infant loss (Watson et al., 2019). These findings suggest that healthcare providers and those who assist African American women after experiencing each type of fetal/infant loss should undergo additional sensitivity training to better understand women’s needs, wants, values, and desires to better assist them with internal conflict as it may be magnified due to multiple losses.
Finally, participants stated that pregnancy, delivery, and death of a child influenced their stressors prior to, during, and after experiencing each type of fetal/infant loss. Consistent with research, women with high levels of stress prior to and during pregnancy had an increased risk of miscarriage (Li et al., 2012) and stillbirth (Staneva et al., 2015); however, only preconception stress, and not prenatal stress, was associated with infant mortality (Class et al., 2013). These findings suggest that African American women who have a history of each type of fetal/infant loss should receive additional support to address stressors they encounter prior to, during and after pregnancy.
In this study, we used Critical Race Theory to provide additional insight into the understanding of African American women’s stressors prior to, during, and after experiencing each type of fetal/infant loss. Currently, there is minimal research using Critical Race Theory as a framework that analyzes stressors specifically focusing on African American women that experienced each type of fetal/infant loss. We expanded the use of the theory by demonstrating the interactions of intersectionality between race, gender, and health outcomes, specifically when examining miscarriages, stillbirths, and infant mortality. Although our data did not explicitly demonstrate participants’ experiences of racism or discrimination, this does not mean race-related stressors did not exist. One possible explanation is that race-related stressors were already part of participants’ lives and they did not see it as a source of stress surrounding their fetal/infant loss. Using Critical Race Theory was helpful for the research team to ensure participants’ voices were expressed without oppression and fragmentation (Ford & Airhihenbuwa, 2010). It also helps to understand this critical but hidden issue by highlighting African American women’s perspectives.
Limitations
The research team acknowledges study limitations, specifically limited generalizability due to a small sample size and limited geographic region. However, using semi-structured interviews allowed the research team to gather in-depth discussions that would not have been obtained otherwise. Although the participants were only from a county in Northeast Ohio, other parts of the United States can use the study takeaways and learn from them. In particular, miscarriage, stillbirth, and infant mortality among African American women are higher in other states (Kids Count Data Center, 2020). Though political and healthcare systems may vary slightly, the stressors of social support, grief, internal conflict, and pregnancy, delivery, and death of a child are likely similar. Future research should explore these and other stressors within other geographic areas (with higher and lower miscarriage, stillbirth, and infant mortality rates) to determine if and/or how stressors change.
Further, participants were drawn from a larger study and, therefore, the findings may not be representative of all African American women who experienced all three types of losses. The research team also did not account for demographic differences in participants. In addition to experiencing all three types of losses, some participants may have experienced multiple miscarriage, stillbirth, and infant mortality events. While all participants indicated they experienced all three loss types on the demographic questionnaire, when interviewed, most participants focused on only one loss.
Implications for Future Research and Practice
The study’s findings have several implications. These results highlight the need for healthcare institutions and providers to continue efforts working on culturally specific ways to decrease miscarriage, stillbirth, and infant mortality and improve interventions and policies. Providing culturally specific healthcare may be a key strategy to reduce racial disparities in miscarriage, stillbirth, and infant mortality rates.
The first culturally specific suggestion is to increase mental health screenings to African American women across healthcare systems. Specifically related to prenatal and postpartum depression, Sidebottom et al. (2021) found that although the majority of prenatal and returning postpartum patients in their study were screened for depression, African American women were least likely to be screened. Prenatal and Postpartum depression left untreated can lead to many factors including an increased risk of infant mortality (Sidebottom et al., 2021). Increasing depression screenings for African American women can lead to increased diagnosis, referral, and treatment (Dolbier et al., 2013), helping them cope with and handle their stressors through different methods.
Another culturally specific recommendation is for nurses (and other healthcare providers) to adopt Watson’s Theory of Human Caring, which explains that nursing is a person-to-person process of caregiving centered on helping the patient achieve a higher degree of harmony in the mind, body, and soul (Tektas & Cam, 2017). Adopting this model can provide holistic bereavement support to African American women who have experienced fetal/infant loss. African American women who experience more than one fetal/infant loss are inclined to feelings of depression, anxiety, guilt, and anger, with incidence of depression being approximately five times higher amongst those women as well (Ruderman et al., 2020). Poor treatment from healthcare providers can add to the stressors of African American women, exacerbating their mental health concerns. Fenstermacher and Hupcey (2020) explain that nurses play a major role in planning and providing culturally sensitive and developmentally appropriate bereavement support for women who have experienced loss (especially for young African American women), and support should extend beyond the hospital. Providing emotional support, bereavement support, and intentional outreach even after being discharged can help reduce prevalence of mental health concerns amongst African American women after experiencing fetal/infant loss.
The last culturally specific recommendation, considering mental health screenings and increased support from healthcare providers, is to increase African American women’s mental health resources and referrals for treatment after their fetal/infant loss experience. Bodnar-Deren et al. (2017) found that African American women are more likely to accept spiritual counseling than mental health counseling and were not able to associate stigma to lack of treatment for postpartum depression. This could suggest a lack of access and support, particularly from healthcare providers.
To address fetal/infant loss and reduce the health disparity injustices experienced by African American women, removing structural racism from the healthcare system should be a priority. Structural racism is described as interconnected institutions that foster and reinforce racial discrimination to leverage one racial group over others (Owens-Young & Bell, 2020). For racially marginalized groups, racism in healthcare restricts access to many health-promoting determinants (e.g., healthcare, safe housing) that can lead to pregnant women having high risk pregnancies resulting in infant morbidity and mortality (Wallace et al., 2017). For those who have experienced each type of fetal/infant loss (miscarriage, stillbirth, and infant mortality), interventions should focus on: (a) promoting positive social support, (b) addressing grief, (c) working through internal conflict, and (d) addressing concerns regarding pregnancy, delivery, and after birth. Further, we suggest increasing societal awareness to reduce stigma associated with miscarriage, stillbirth, and infant mortality.
This study showed that African American women need a holistic network of care and support to improve pregnancy outcomes. The research is significant in providing context to current data on fetal, infant, and maternal health. Existing literature has explored African American infant mortality and the myriad factors contributing to rates higher than other racial groups. However, this study was the first to explore and give significance to a subset of African American women who have experienced each type of fetal/infant loss (miscarriage, stillbirth, and infant mortality). Priority needs to be placed on removing structural racism from healthcare systems to reduce health disparity injustices experienced by African American women who experience miscarriage, stillbirth, and infant mortality. Future additional research is needed to further explore African American women’s experiences of multiple losses, as well as to gain a better understanding how length of time between each loss may influence their stressors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We say thank you to the YWCA of Greater Cleveland and First Year Cleveland for funding this research.