
Abstract
Prior research highlights the detrimental effects of loneliness and social isolation on health, yet Black men’s mental health in this context remains underexplored. This study examines how loneliness-related stress relates to anxiety and depression symptoms, and whether social support moderates these effects among Black men. Using cross-sectional data from 690 participants in The Association of Black Psychologists’ COVID-19 and Black Mental Health Needs Assessment, we compared men who identified “fear of being alone” as a major stressor (n = 83) to those who did not (n = 607). Those reporting being alone as a stressor showed higher anxiety and depressive symptoms. Moderation analyses revealed that informal support was unrelated to mental health outcomes for this group, but formal support significantly reduced depressive symptoms. Among men who did not fear being alone, formal support was associated with substantially lower depressive symptoms; among men who did fear being alone, depressive symptoms remained elevated regardless of support. These findings underscore the protective role of formal social support in mitigating loneliness-related distress among Black men, offering key implications for mental health interventions and future research.
Loneliness is a pervasive and debilitating condition associated with numerous adverse mental and physical health outcomes, including depression, anxiety, cardiovascular disease, and premature mortality (Fried et al., 2020; Hawkley & Cacioppo, 2010; Holt-Lunstad et al., 2015; Lee et al., 2020; Lim et al., 2023). The isolating conditions created by the COVID-19 pandemic further intensified these risks, as shelter-in-place mandates, remote work, and reduced community contact fundamentally changed how individuals connected with others (Einav & Margalit, 2023; Gruber et al., 2021; Holt-Lunstad et al., 2015; Ibrahimi et al., 2020). By 2023, loneliness had become so widespread that the United States Surgeon General’s Office officially declared it an epidemic in the United States (Office of the Surgeon General, 2023). Yet, even before the COVID-19 pandemic, public health agencies had already recognized loneliness and social isolation as pressing global concerns (Loneliness as a Public Health Threat, 2023).
Although loneliness is often conflated with being alone, the two concepts are distinct. Being alone refers to the physical state of solitude, while loneliness reflects the emotional perception that one’s social needs are unmet (Hawkley & Cacioppo, 2010; Hwang et al., 2020). Previous research suggests the psychological impact of solitude ultimately depends on an individual’s perception of that experience–whether it is felt as restorative or distressing. Rodriguez et al. (2025) found that individuals who hold unfavorable views about being alone tend to feel significantly lonelier after spending time alone, while those with more positive attitudes toward being alone experience reduced loneliness after solitary periods.
This distinction between objective isolation and the perception of being alone is central to understanding mental health during the COVID-19 pandemic. While being alone may be a neutral or even restorative state for some, when it is interpreted as rejection or disruption of belonging, it can amplify depressive, anxiety, and suicidal ideation symptoms as a byproduct of loneliness (Allen et al., 2022; Bu et al., 2020; Cacioppo et al., 2006; Danilovich et al., 2021; Ernst et al., 2021; Groarke et al., 2020; Killgore et al., 2020; Özdemir & Çelen, 2024). Most concerningly, previous research has found men most susceptible to increases in suicidal ideation as a result of loneliness (Ernst et al., 2021). For Black men—who already face unique cultural and structural stressors—the experience of being alone may lead to additional impacts (Brewer et al., 2022; Chang, 2018; Watkins et al., 2009).
Research among Black adults shows that both objective isolation (infrequent contact with family or friends) and subjective isolation (lack of emotional closeness) are associated with higher depressive symptoms and psychological distress (Taylor & Taylor, 2020). Moreover, national polling indicates that young Black adults report higher rates of frequent loneliness than many other demographic groups (Mansour et al., 2021; Schumacher et al., 2023). In this study, we operationalize this cognitive-emotional pattern as isolation-related stress, measured by the “fear of being alone.” This framing captures the subjective strain of solitary states, distinct from loneliness itself, and reflects a culturally and contextually situated vulnerability intensified by the pandemic’s forced solitude.
Additionally, these challenges intersect with broader sociocultural and structural inequities faced by Black men. Black men face disproportionate exposure to racial discrimination, economic instability, and systemic exclusion, all of which contribute to elevated risks for depression and anxiety (Banks & Kohn-Wood, 2007; Charles & Witherspoon, 2019; Hammond, 2012; Hankerson et al., 2015; Johnson et al., 2024). Although recent surveys estimate that nearly one in four Black men experience depressive symptoms (Cenat et al., 2025), these figures likely underrepresent true prevalence due to cultural mistrust of healthcare systems and masculine norms that discourage vulnerability (Lateef et al., 2023; Sanders et al., 2024; Watkins et al., 2009). The COVID-19 pandemic further disrupted key protective networks—such as churches, barbershops, fraternities, and extended family systems—that traditionally provide informal emotional support (Blumberg et al., 2015; Brother, You’re On My Mind, 2023; DeSouza et al., 2020; Sneed et al., 2020; Ward & Mengesha, 2013). In the absence of informal support, Black men may turn to self-reliance or maladaptive coping to handle stressors (Cox et al., 2023; Watkins et al., 2020). However, Greer and Cavalhieri (2019) found that coping strategies rooted in self-reliance were significantly associated with greater severity in mental health symptoms among African American men.
Under such conditions, formal support systems—mental health professionals, medical services, and structured interventions—become critical. Yet, their effectiveness depends heavily on perceived safety, trust, and cultural congruence (Earl et al., 2011; Hudson et al., 2016; Watkins et al., 2020). Many Black men seek formal support only after reaching a “tipping point,” such as a major life crisis, which may diminish its preventative potential (Lindsey & Marcell, 2012). Studies suggest that while social support is protective against depression and anxiety (Dour et al., 2013; Hankerson et al., 2015; Hoffmire et al., 2024; Qin et al., 2020), its benefits are reduced when support is mismatched to cultural values or delivered within environments that evoke mistrust (Alvarez et al., 2022; Hudson et al., 2016; Khan et al., 2020). Conversely, when support fosters belonging and respect, it can buffer against the psychological burden of isolation and loneliness (Goodwill et al., 2018).
The Current Study
The present study extends existing research by examining how perceptions of being alone moderate the relationship between formal support and mental health outcomes among Black men during the COVID-19 pandemic. “Fear of being alone” is conceptualized as a proxy for isolation-related stress—reflecting distress about solitude rather than the experience of solitude itself. By analyzing how this perception interacts with formal support, the study clarifies when and for whom formal interventions are most effective, informing culturally responsive systems that strengthen community and belonging central to Black men’s resilience.
Guided by African American Male Theory (AAMT), which emphasizes contextual and strengths-based understandings of Black men (Bush & Bush, 2013), we test whether receiving formal support is associated with fewer depressive and anxiety symptoms and whether this association varies by perceptions of isolation-related stress during the COVID-19 pandemic. This framework acknowledges structural and relational influences without assuming all mechanisms can be captured within the present dataset. Isolation-related stress was indexed by endorsement of “fear of being alone”; formal support was assessed as receipt of professional assistance in the past month (items adapted from the National Survey of American Life [NSAL] program of research; Jackson et al., 2004); and mental health outcomes were measured using the depressive and anxiety symptoms subscales of the Patient Health Questionnaire-4 (PHQ-4; Kroenke et al., 2009).
Method
Design
This study was a secondary analysis of the national survey component of The Association of Black Psychologists’ (ABPsi) COVID-19 and Black Mental Health Needs Assessment Project (Randolph Cunningham et al., 2021). The cross-sectional data in the study were from Black adults in six states in the U.S. that comprised the primary study sites (California, Washington, DC/Maryland, Louisiana, Michigan, Mississippi, and Texas) and three convenience states (Florida, Georgia, and Ohio).
Participants
Participant Characteristics. (N = 690)
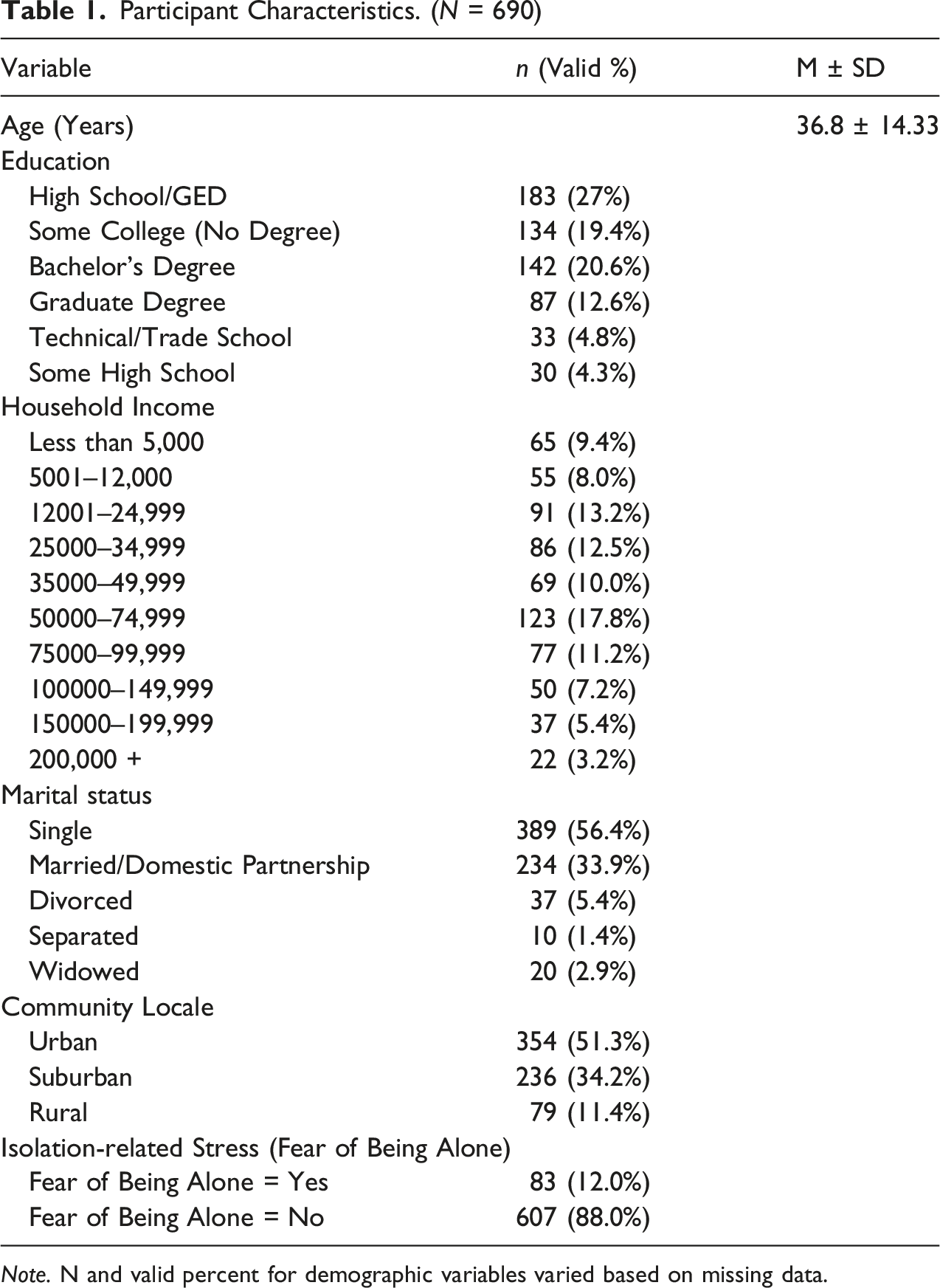
Note. N and valid percent for demographic variables varied based on missing data.
To meet eligibility requirements, participants had to report that they had been living in the United States since at least the last quarter of 2019, which was the quarter before COVID-19 was officially designated a pandemic in the U.S. Participants were primarily sampled from the following states/regions: Louisiana, California, the District of Columbia, Maryland, the Mississippi Delta, Texas, and Michigan. At the time of collection, these states/regions were COVID-19 hotspots. These states/regions were also selected for their high concentration of Blacks/Africana folx as well as their geographic and population diversity (mid-sized cities/areas [Detroit and Washington, D.C. and its Maryland suburbs]; metropolitan/urban areas [Houston, New Orleans, and Los Angeles]; and rural areas in Maryland, Louisiana, Texas, and the Mississippi Delta). Additionally, convenience sampling was utilized to collect data from respondents living in Florida, Georgia, and Ohio.
Measures
Mental Health Outcome Variables
Depressive and anxiety symptoms were assessed using the Patient Health Questionnaire–4 (PHQ-4; Kroenke et al., 2009). Two items each measured depressive and anxiety symptoms on a 0–3 scale (0 = “Not at all,” 3 = “Nearly every day”; 4 = “Prefer not to answer,” missing). Subscale scores were computed as the sum of each item pair (range = 0–6). Scores ≥3 indicate probable clinical relevance (Kroenke et al., 2009). Prior studies report strong reliability (α ≈ .81–.85); in the current sample, α = .89 for the total scale, with strong inter-item correlations (r = .67 for depressive symptoms, r = .66 for anxiety symptoms).
Prior psychometric work supports the PHQ-4’s convergent and discriminant validity. Convergent validity is evidenced by moderate-to-strong positive associations with established anxiety and depression measures and with mental health-related quality of life (e.g., significant correlations with DASS total and subscales, and with the SF-12 Mental Health/Mental Component Summary), as well as by the expected pattern in which the PHQ-2 and GAD-2 relate most strongly to depression- and anxiety-specific comparators, respectively (Kroenke et al., 2009, 2019; Löwe et al., 2010; Obeid et al., 2024). Discriminant validity is supported by negative associations with positive well-being indicators (e.g., inverse associations with the WHO-5 well-being index) and comparatively weaker relations with physical-health functioning than with mental-health functioning (Havnen et al., 2023; Kroenke et al., 2019; Lara-Cabrera et al., 2022). U.S. population-based research further documents good internal consistency, factorial validity, and measurement invariance of the PHQ-4, reinforcing its construct validity in racially and ethnically diverse national samples (Adzrago et al., 2024).
Predictor Variables
The formal support measure was adapted from the National Survey of American Life (NSAL) (Jackson et al., 2004). Participants indicated whether, in the past month, they had received formal or professional help to assist with COVID-related needs (e.g., professional advice, medical or mental health care, food bank access, employment assistance). Responses of “yes” or “no” were dichotomized (Yes = 1, No = 0). “Prefer not to answer” was recoded to missing). “Fear of being alone” was conceptualized as a proxy for the moderator variable—isolation-related stress. Participants were asked, “What have been your greatest sources of stress from the COVID-19 outbreak? Please check all that apply.” One option was, “Fear of being alone.” “Yes”/“No” responses were dichotomized (1 = Yes, 0 = No; and “Prefer not to answer” was coded to missing). Although “fear of being alone” does not fully capture the subjective emotional experience of loneliness, it reflects a salient loneliness-related stressor and has been linked in prior work to perceived social isolation (Hawkley & Cacioppo, 2010).
Procedure
The Institutional Review Board of the MayaTech Corporation evaluated and approved this study (Protocol No. 2020-001). The data were collected cross-sectionally, from January 1, 2021 through April 30, 2021, via an online survey administered by Qualtrics, LLC, a fee-based recruitment platform. The parent study surveyed 2,480 Black Americans regarding the impact of COVID-19 across physical, mental, financial, and social domains (Randolph Cunningham et al., 2021). All participants provided informed consent and confirmed that they met all eligibility requirements before beginning the survey. Qualtrics applied industry standards to ensure only eligible respondents were included. The present subsample included men who met the eligibility criteria and had complete data on study variables. Although the survey requested much more information from respondents, this particular study only included the data collected on mental health outcomes, the formal support variable, and the potential “perception of being alone” moderator of the relation between formal support and mental health. Most participants completed the survey within 30 minutes. No order effects were expected, so all items were presented to every respondent in the same order. Qualtrics provided a financial incentive based on pre-arrangements with their survey panels.
Data Management
Responses coded as “Prefer not to answer” were treated as system missing across all variables. Available-case (pairwise) deletion was applied for the primary analyses, with analytic Ns of 732 and 734 for the depression and anxiety models, respectively. Outliers for depression and anxiety symptoms were assessed using the 1.5 × IQR rule; no extreme cases were identified beyond expected variance on the 0–6 scales. Distributional assumptions were verified using skew and kurtosis (values < ±1); Levene’s tests confirmed homogeneity of variances. Because the independent variables were dichotomous, normality assumptions applied only to the dependent variables.
Analytic Strategy
Analyses were conducted using the Statistical Package for the Social Sciences (SPSS) Version 29. Two ordinary least squares (OLS) moderation models were estimated, with depressive symptoms and anxiety symptoms as dependent variables. Predictors were (a) isolation-related stress (Fear of being alone; 0 = No, 1 = Yes), (b) formal support (0 = No, 1 = Yes), and (c) their interaction term (Fear × Formal Support).
Familywise α across the two models was controlled at .025 using Holm correction. For each predictor, we report unstandardized B, SE, 95% CI, p, and semi-partial R2 (sr 2 = Part2); model R2 and analytic n are also reported. Descriptive statistics (means, standard deviations, skew, kurtosis), reliability indices, and zero-order correlations among key variables were examined prior to primary analyses.
Results
Preliminary Screening and Assumptions
After recoding “Prefer not to answer” as system missing and applying listwise deletion, 690 participants had complete data for the focal variables. Because predictors were dichotomous, distributional checks were conducted only on the continuous outcomes. For depressive symptoms and anxiety symptoms (PHQ-4 subscales), distributions were approximately normal (depressive symptoms: M = 2.01, SD = 1.92, skew = 0.56, kurtosis = –0.87; anxiety symptoms: M = 1.84, SD = 1.90, skew = 0.69, kurtosis = –0.65). Outliers were evaluated using the 1.5 × IQR rule; mild outliers were retained; and conclusions were unchanged in sensitivity checks. Levene’s tests were nonsignificant for both outcomes, supporting homogeneity of variances. All tests were two-tailed with Holm-adjusted /u03b1 = .025 across the two primary models.
Descriptives, Reliability, and Correlations
Descriptives, Reliability, and Correlations
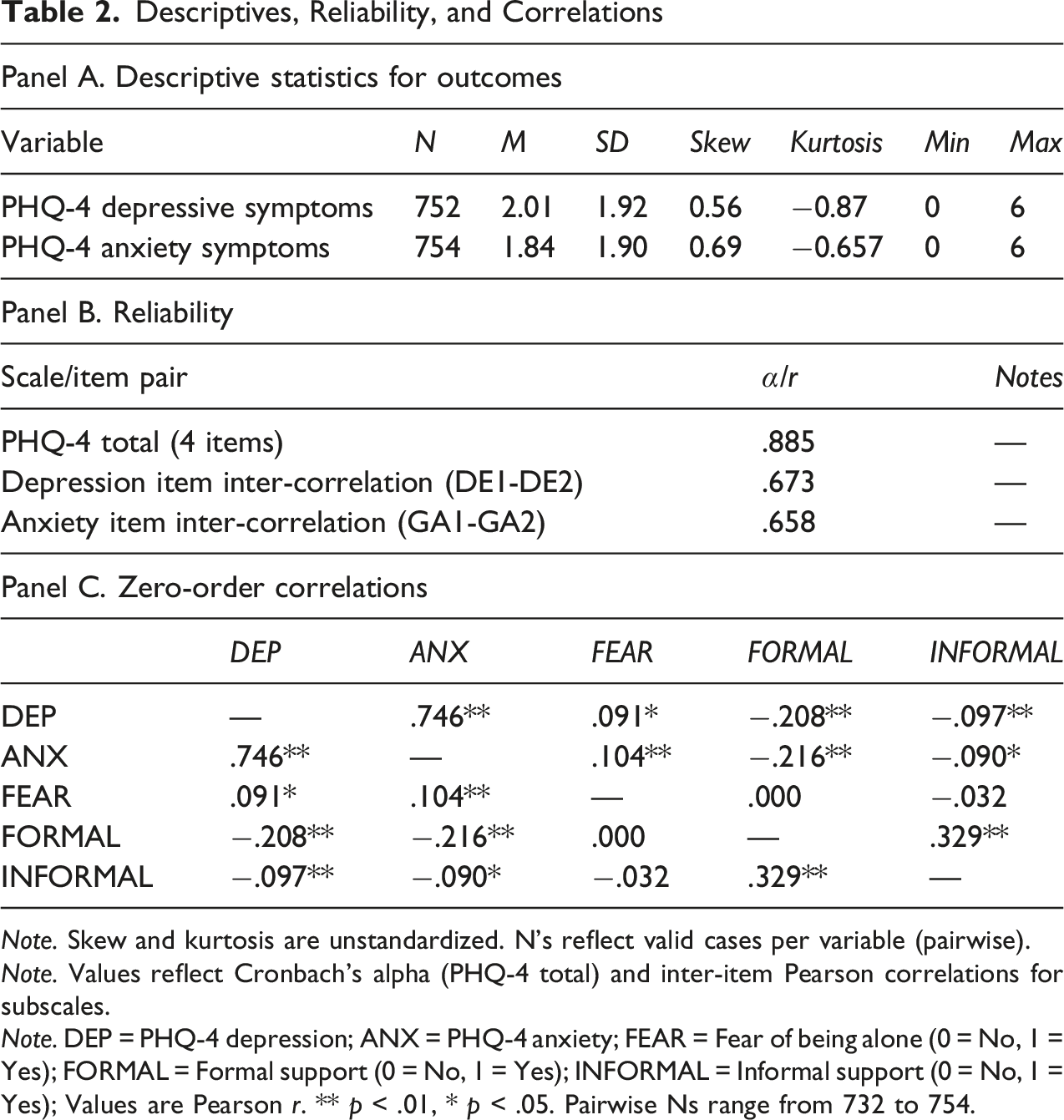
Note. Skew and kurtosis are unstandardized. N’s reflect valid cases per variable (pairwise).
Note. Values reflect Cronbach’s alpha (PHQ-4 total) and inter-item Pearson correlations for subscales.
Note. DEP = PHQ-4 depression; ANX = PHQ-4 anxiety; FEAR = Fear of being alone (0 = No, 1 = Yes); FORMAL = Formal support (0 = No, 1 = Yes); INFORMAL = Informal support (0 = No, 1 = Yes); Values are Pearson r. ** p < .01, * p < .05. Pairwise Ns range from 732 to 754.
Primary Analyses
OLS Regression Predicting Depressive Symptoms (PHQ-4)
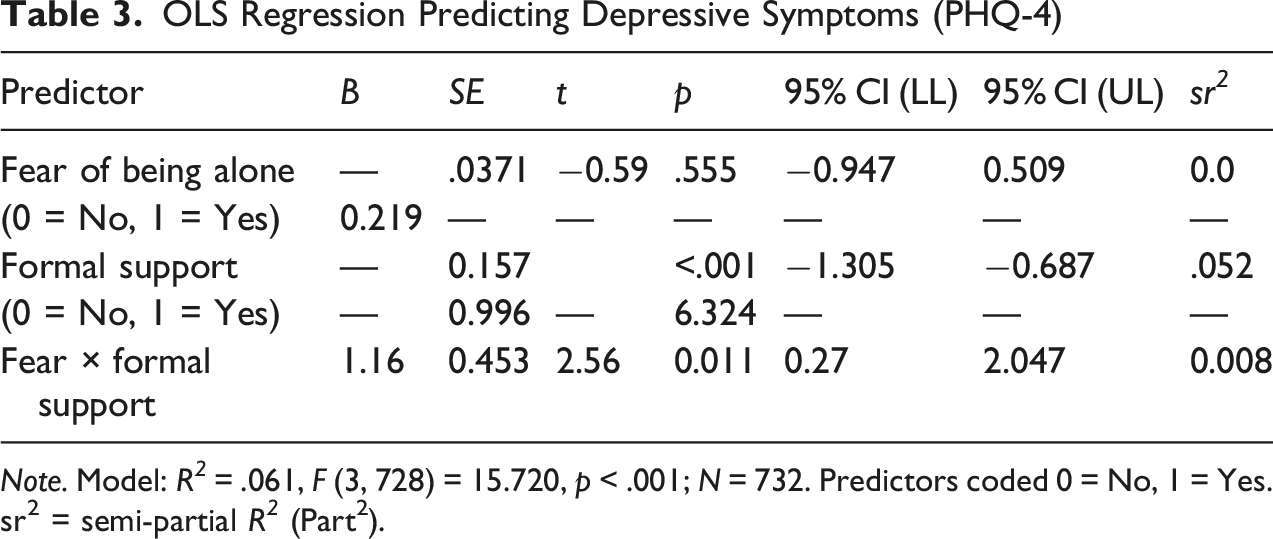
Note. Model: R 2 = .061, F (3, 728) = 15.720, p < .001; N = 732. Predictors coded 0 = No, 1 = Yes. sr2 = semi-partial R 2 (Part2).
OLS Regression Predicting Anxiety Symptoms (PHQ-4)
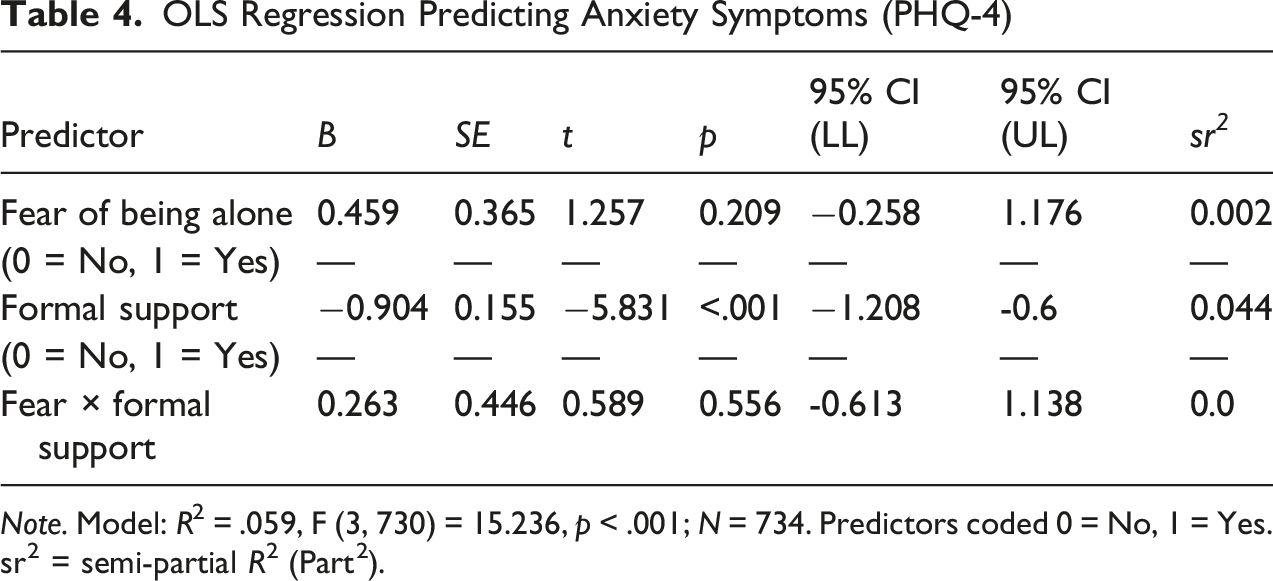
Note. Model: R2 = .059, F (3, 730) = 15.236, p < .001; N = 734. Predictors coded 0 = No, 1 = Yes. sr2 = semi-partial R2 (Part2).
Depressive Symptoms
The model was significant (R2 = .06, p < .001). Formal support predicted lower depressive symptoms (B = −0.996, SE = 0.157, 95% CI [–1.31, −0.69], p < .001). The Fear × Formal Support interaction was significant (B = 1.159, SE = 0.453, 95% CI [0.27, 2.05], p = .011), meeting the Holm-adjusted criterion. Estimated marginal means (EMMs) clarified the pattern: among men without fear of being alone, those with formal support reported lower depressive symptoms (EMM ≈1.57, SE = 0.09) than those without formal support (EMM ≈2.56, SE = 0.26); among men who did fear being alone, depressive symptoms did not differ by support status (EMMs ≈2.38 vs. 2.60). The 2 × 2 profile is shown in Figure 1. EMMs/plot were obtained via GLM for visualization; and inference derives from the OLS model (see Table 3). Depressive Symptoms by Fear of Being Alone x Formal Support (EMMs)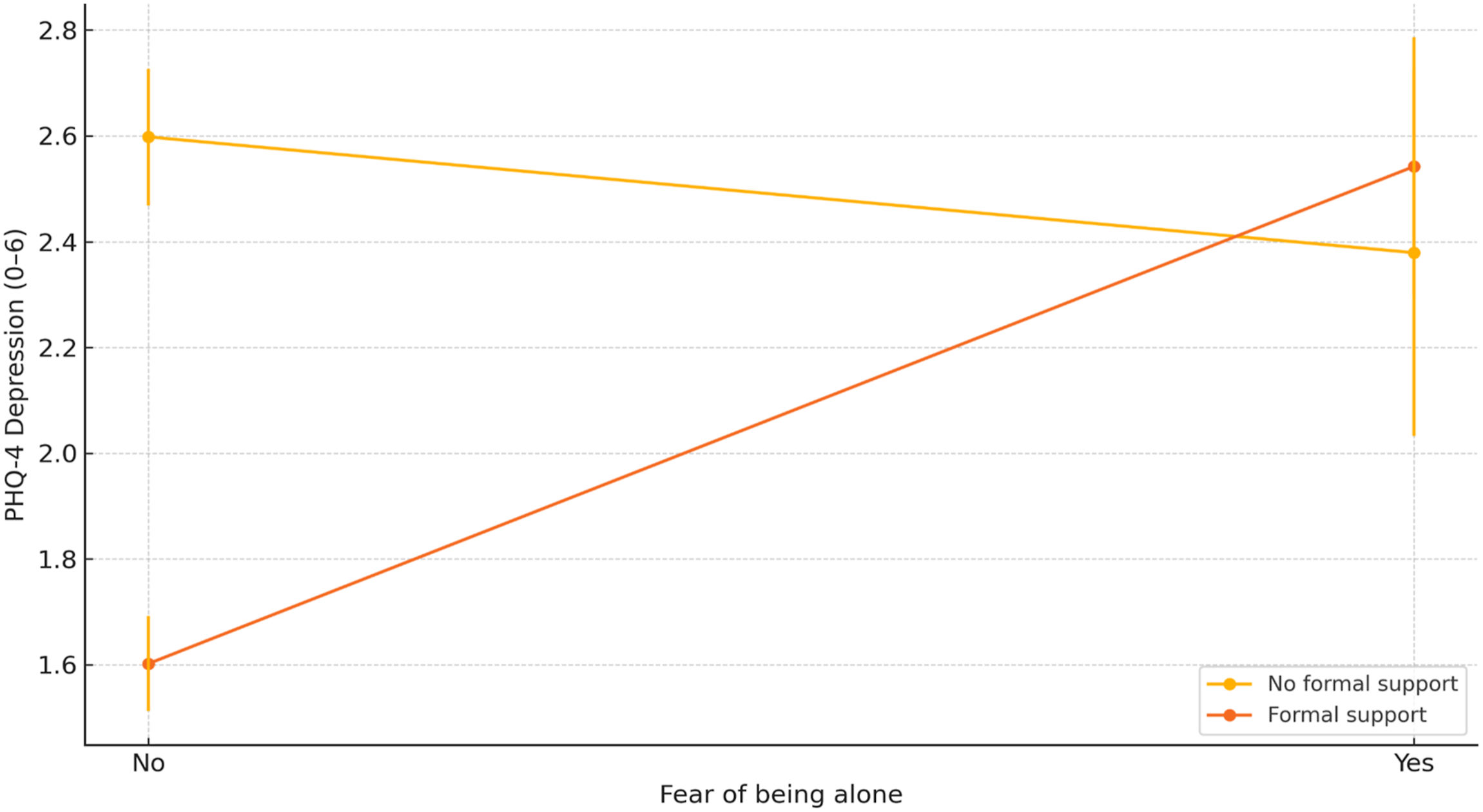
Anxiety Symptoms
The anxiety symptoms model was also significant (R2 = .06, p < .001). Formal support predicted lower anxiety symptoms (B = −0.904, SE = 0.155, 95% CI [–1.21, −0.60], p < .001). The main effect of fear of being alone and the Fear × Formal Support interaction were not significant at the Holm-adjusted threshold (ps > .025; see Table 3B).
Summary
Across outcomes, formal support was associated with lower symptoms. For depressive symptoms, the association was conditional: men who did not fear being alone showed the clearest benefit of formal support, whereas men who did fear being alone reported elevated depressive symptoms regardless of support. For anxiety symptoms, formal support related to lower symptoms independent of fear of being alone (see Tables 2 and 3; and Figure 1).
Discussion
This study examined how formal support moderates the relationship between isolation-related stress—operationalized as “fear of being alone”—and depressive and anxiety symptoms among Black men during the COVID-19 pandemic. Drawing on the African American Male Theory framework (Bush & Bush, 2013), we sought to understand how cultural, ecological, and identity-based factors shape the interplay of perceived solitude, mental health, and support among a population often under-studied in this domain.
Our results show “fear of being alone” functions as a disruptive cognitive-emotional stressor in this sample. Traditional research treats loneliness or social isolation as risk factors, but our findings point to the added nuance that the perception of being alone can alter how formal support is received and its effectiveness. The fact that men who feared being alone had elevated depressive symptoms regardless of support suggests that simply providing formal resources is not enough when the underlying stress involves disrupted belonging, emotional vulnerability, or relational mistrust.
For men who did not endorse fear of being alone, formal support was strongly protective against depressive symptoms, and the buffering effect of formal support held across groups for anxiety symptoms as well. This aligns with prior work showing that structured, professional help can reduce symptoms when accessed (Hankerson et al., 2015; Qin et al., 2020). However, the attenuation of support’s benefit among men who feared being alone points to an important caveat: support must not only be present but might also need to be perceived as safe, culturally responsive, and relationally trustworthy (Alvarez et al., 2022; Ellison et al., 2021; Khan et al., 2020). For these men, formal support without relational alignment may not overcome the emotional barrier imposed by fear of solitude.
The differing pattern for anxiety symptoms versus depressive symptoms is noteworthy. Anxiety symptoms were lower among those with formal support regardless of fear of being alone, suggesting that formal support may meet instrumental needs—structure, guidance, coping tools—that mitigate anxiety. In contrast, depressive symptoms appear to require more than utility; they require relational belonging and safety. When fear of being alone is high, formal support appears insufficiently relational to buffer depressive symptoms. This aligns with the hypothesis that depressive pathways may be more deeply linked to perceived disconnection or unmet relational needs, while anxiety may respond to more immediate or pragmatic support (Dour et al., 2013).
Several contextual factors may help to explain these patterns. Black men face compounded stressors, including racial discrimination, economic precarity, and masculine norms discouraging emotional disclosure (Charles & Witherspoon, 2019; Hammond, 2012; Johnson et al., 2024). In this context, fear of being alone likely reflects not only anxiety about solitude, but the loss of culturally grounded networks (church, fraternity, barbershop) that serve as informal support. During the COVID-19 pandemic those networks were disrupted; for men already primed to manage stress through self-reliance, the combination of forced isolation and weakened informal supports may have amplified the impact of being alone as a stressor.
This pattern underscores a central tenet of Black psychology—that communalism and connectedness serve as protective factors against distress. When the pandemic restricted access to collective spaces of affirmation, the resulting isolation disrupted not only social contact but also cultural identity expression. Formal support, if not culturally aligned, might fail to offset the emotional cost of perceived disconnection.
Limitations
There are several important limitations for this study. First, our operationalization of isolation-related stress as “fear of being alone” offers a focused lens, but it does not capture the full richness of loneliness, social isolation, and their emotional consequences as defined in prior literature (Hawkley & Cacioppo, 2010; Leary & Asbury, 2022). Second, while we measured receipt of formal support, we did not assess perceived quality, cultural congruence, or relational trust in that support–factors likely critical to effectiveness (Earl et al., 2011; Ward & Mengesha, 2013). Additionally, this study measured received rather than perceived support. Distinguishing these constructs is critical, as perceived quality and trust often predict outcomes more strongly than mere receipt (Rodriguez et al., 2025). This study also did not examine men’s satisfaction with the formal support they received, a factor explored (although not found significant) in a predominantly female sample using the same parent dataset (Burlew et al., 2025). Nor were other sociocultural factors explored such as the now well-studied intersection of racism and mental health (Cokley et al., 2022) due to the George Floyd murder and Black Lives Matter Movement, and the increase in Blacks’ cultural mistrust of the healthcare system that resulted in race-related COVID worries (Castelin et al., 2023) and vaccine hesitancy (Hall et al., 2025). Lastly, this is a cross-sectional design; causality cannot be inferred. Future longitudinal or mixed-methods work could examine how fear of being alone and support interactions evolve over time. Despite these limitations, our results highlight that formal support must be relationally sensitive and culturally resonant to buffer the mental health impacts of perceived solitude among Black men.
Strengths
Several strengths of this study enhance its potential to inform future research, policy and practices to improve mental health outcomes for Black men. For example, recent literature has noted the lack of studies with large racial/ethnic minority samples, including Black people (Grills et al., 2022). The ABPsi COVID-19 and Black Mental Health Needs Assessment dataset provided a large and diverse sample of 690 Black men with complete data to use in this study. The sample’s diversity includes Black men from various geographic regions, socioeconomic statuses, and family compositions, contributing to the generalizability of our findings. Furthermore, by examining the specific determinants of mental health during a global health crisis, this study offers a critical foundation for developing culturally responsive interventions. Such tools are essential for mitigating the psychological toll of social isolation and systemic stressors during public health emergencies.
Implications
Future Directions for Research, Practice, and Policy
Future studies should parse the distinct constructs of objective isolation (physical solitude), perceived “being alone” stress, and subjective loneliness to clarify how each uniquely contributes to mental health outcomes among Black men. Integrating African American Male Theory with cognitive frameworks of loneliness could clarify how internalized beliefs about independence and self-reliance shape emotional responses to solitude. Qualitative work could explore how Black men interpret “being alone,” how formal support is perceived in their cultural context, and how trust and belonging shape engagement. Comparative work (e.g., by region, age, rural vs urban) may reveal subgroup differences. Moreover, experimental or longitudinal research that manipulates relational aspects of both informal and formal support (e.g., cultural matching, trust-building, and engagement in community building activities) could test whether enhancing the relational fit of formal support improves its buffering effect. Including gender-diverse samples would extend understanding of how masculine norms, identity, and support needs differ across intersections.
This study also has implications that might inform mental health practices when working with Black men during pandemics and epidemics that require social isolation techniques as mitigation guidelines. These findings might be useful in designing culturally and gender-responsive tools and interventions that protect against the adverse effects of social isolation for Black men. For Black men who report the availability of formal supports such as professional help, availing oneself of formal support may be an effective coping strategy during a pandemic if aligned with communal identity and relational trust. Thus, training for mental health professionals about the protective value of culturally responsive care for Black men, as well as, formulating policies that provide funding to increase the availability of said care is warranted.
Moreover, the findings suggest that psychological well-being among Black men is shaped not only by support access, but may also be shaped by how that support affirms communal identity and relational trust. Formal interventions that overlook these cultural dimensions risk replicating isolation under the guise of care. These findings expand the theoretical lens in Black psychology by demonstrating that support efficacy is conditional on relational and perceptual factors. As a result, formal support needs to center fit with cultural identity, trust, and experience of belonging to genuinely connect with Black men. Additionally, interventions should not only promote formal support access, but also focus on aligning the relational and cultural environment of that support with men’s lived experience of loneliness, fear of being alone, and belonging. Tailoring support to address the psychological meaning of solitude may make formal support more effective.
Conclusion
This study illuminates how the perception of being alone—fear of being alone—interacts with formal support to influence mental health outcomes among Black men during the COVID-19 pandemic. While formal support is generally protective, its effectiveness is conditional on men’s experience of belonging, trust, and cultural resonance. Depression appears tied to relational and belonging disruptions, whereas anxiety is mitigated by structured support regardless of solitude stress.
These findings extend Black psychology scholarship by underscoring that support interventions must account for relational meaning, cultural identity, and perceived solitude in order to fully buffer mental health distress. For Black men, “being alone” is not simply a state—it signals deeper disconnection from communal identity and support. Grounded in the liberatory principles of Black psychology, these findings call for formal support systems that function not only as interventions for individuals but as collective restorations of belonging, trust, and identity for Black men.
Footnotes
Author's Note
This manuscript was originally prepared in 2022 as part of The Association of Black Psychologists’ (ABPsi) COVID-19 and Black Mental Health Needs Assessment Project. The present manuscript reflects the original work and secondary analyses from that period.
Acknowledgments
This paper is based on data collected as part of a larger multi-racial research study that was supported by the National Urban League (NUL). The Needs Assessment Phase 1 was funded by grants from The W. K. Kellogg Foundation, JPB Foundation, Ford Foundation, The California Endowment, Weingart Foundation, and the California Wellness Foundation. We acknowledge the support of The Association of Black Psychologists’ (ABPsi) National Office, ABPsi’s current and immediate past Board and staff, staffs at the organizations/institutions at which the research team members were based, staff members and organizational partners in The Alliance of National Psychological Associations for Racial and Ethnic Equity, and our community-based organizational partners and residents in their communities who served as survey respondents. For a full list of the community partners, see the executive summary of the ABPsi’s part of the larger study at the NUL website: ![]() .
.
Ethical Considerations
This study utilized secondary, de-identified data collected as part of The Association of Black Psychologists’ COVID-19 and Black Mental Health Needs Assessment Project. The original project received ethical approval from the Association’s Institutional Review Board, and all participants provided informed consent prior to participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Urban League and The Association of Black Psychologists, Inc. Along with those organizations, the primary project was also supported by grants from the W. K. Kellogg Foundation, JPB Foundation, Ford Foundation, The California Endowment., Weingart Foundation, and the California Wellness Foundation.
Declaration of Conflicting Interests
The author (Nolan Krueger) acknowledges their position as a member of the journal’s editorial board. The peer review process for this article was managed by alternative members of the board, and the submitting board member had no involvement in the decision-making process. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are the property of The Association of Black Psychologists and are not publicly available due to privacy and ethical restrictions. Requests for data access may be directed to the Association of Black Psychologists.