
Abstract
Trauma exposure and structural inequities contribute to mental health disparities among Black men and create barriers to care. Black men face elevated risk from opioid and stimulant co-use, including overdose from unintentional opioid exposure, yet heterogeneity in trauma exposure among men who co-use substances is understudied. Using latent class analysis, this study identified unobserved trauma subgroups and examined associations with cocaine use in a sample of Black men co-using opioids and stimulants; most were formerly incarcerated (88%). Three profiles emerged: Low Trauma (36%), High Non-Sexual Trauma (42%), and High Trauma Across All Categories (21%). In regression models, men in the High Trauma Across All Categories class had higher odds of lifetime powder cocaine use (OR = 4.13, p < .01) and crack cocaine use (OR = 2.08, p < .05) versus the Low Trauma class. Older age was associated with stimulant use, while incarceration history predicted powder cocaine use only. Findings underscore within-group heterogeneity and support trauma-informed interventions to reduce overdose risk among Black men who co-use opioids and stimulants. Targeted screening and tailored services may strengthen engagement in care and harm reduction.
Black men face profound mental health disparities shaped by systemic racism, economic marginalization, and exposure to trauma (Scott-Jones & Kamara, 2020). Scholars estimate that 56–74% of Black males who experience traumatic events do not receive necessary mental health care (Motley & Banks, 2018). Yet, little research has explored how the specific trauma experiences of Black men who use opioids and stimulants intersect to influence substance use and mental health vulnerabilities. The rapid infiltration of fentanyl into the unregulated drug supply has created an urgent public health crisis, placing stimulant users at heightened risk of opioid overdose (Syvertsen et al., 2025). Black men who use stimulants are particularly vulnerable due to systemic inequities, including limited access to harm reduction services, unstable housing, unemployment, and disproportionate policing (Friedman & Hansen, 2022). Recent incarceration further increases overdose risk, as formerly incarcerated individuals often have reduced opioid tolerance and limited awareness of evolving drug market risks, disproportionately affecting racial and ethnic minorities (Brinkley-Rubinstein et al., 2018).
Black men’s mental health must be understood within the context of cumulative trauma exposure, racialized stress, and structurally constrained coping environments, as research consistently demonstrates strong associations between experiences of discrimination, violence, and incarceration and elevated risk for depression, posttraumatic stress symptoms, and substance use among Black men (Amaro et al., 2021; Hurd et al., 2014; Motley et al., 2022). However, conceptualizing Black men’s mental health solely through shared structural exposures risks obscuring important within-group differences, as studies documenting variation in trauma exposure, coping responses, mental health outcomes, and treatment barriers underscore the need for heterogeneity-focused approaches (Coleman-Kirumba et al., 2022; Gran-Ruaz et al., 2022)
Scholars have further noted that culturally grounded norms surrounding masculinity, medical mistrust, and differential access to resources shape how Black men respond to trauma and engage in help-seeking or substance use as coping strategies (Hammond, 2010; Motley & Banks, 2018; Seidler et al., 2016). Despite these advances, much of the existing research relies on variable-centered approaches that aggregate trauma exposure, limiting understanding of how distinct patterns of trauma may differentially relate to substance use behaviors and related risks.
Trauma
To contextualize these vulnerabilities, it is important first to define trauma and its manifestations among Black men. Trauma is defined as distressing events that occur to a person and have a sustained negative influence on that person’s well-being and daily functioning (American Psychological Association, n.d.). Trauma has devastating physiological and psychological impacts that have the potential to affect an individual for a lifetime. Psychologically, trauma manifests itself as chronic stress, depression, anxiety, and other mental illnesses (Maeng & Milad, 2017) that make daily life functioning a challenge. Further, stress works as an impetus, synergistically aggravating the effects of trauma (Duric et al., 2016).
The types of trauma individuals may experience vary according to the overarching descriptive classification, age during exposure, and whether it was personally experienced or witnessed (Kira, 2001). Traumatic life events can consist of but are not limited to a vehicular accident, physical assault with or without a weapon, involving or not involving sexual assault, war, or terroristic attack (Weathers et al., 2013). Notably, Jones and colleagues (2022) found that 5-6% of Black men met criteria for a PTSD diagnosis; Black men are disproportionately exposed to multiple forms of violence across the life course, including but not limited to gun violence, which contributes to elevated risk for PTSD and related mental health conditions such as anxiety, depression, and substance use disorders (Motley & Banks, 2018; Smith & Patton, 2016; Ugwuede, 2023).
Contextually, incarceration warrants particular attention as a potent and often overlooked source of trauma among Black men, especially given that the study’s sample is composed largely of formerly incarcerated individuals. This focus is further underscored by the disproportionate representation of Black men within the U.S. prison system, who constitute approximately 35% of individuals who are incarcerated despite representing only 13% of the general population (Johnson & Manyweather, 2023). Incarceration can be viewed as a three-fold cord of trauma: exposure to adverse events prior to incarceration, the state of being incarcerated, and reentry challenges. Jäggi and colleagues (2016) found that repeated exposure to trauma, witnessed or perpetrated, is associated with increased justice involvement. Witnessing brutalities toward inmates, experiences of racism, the pressure to perpetuate violence, hypervigilance and paranoia, and forced loneliness have been cited as points of trauma for incarcerated Black men (Addison et al., 2025). The reentry phase is a critical period marked by diminished access to essential resources and a sharp decline in social support within the first 6 months post-release, a trend that continues over time (Pettus-Davis et al., 2020). Nearly half of individuals experience at least one traumatic event within the first 8 months of release (e.g., violent assault, witnessing serious injury or death, or losing a loved one) (Pettus-Davis et al., 2020). The compounded effects of such trauma on Black men first became evident during the War on Drugs, when the criminalization of drug use fueled community violence and contributed to the disproportionate incarceration of Black men nationwide (Fornili, 2018). Thus, further highlighting the relationship between trauma and substances among Black men.
Medical Mistrust, Masculinity, and Coping
Lifetime experiences of traumatic events can be exacerbated by perceived discriminatory interactions with clinicians, which contributes to the medical mistrust among Black men (Hammond, 2010). Their mistrust of the healthcare system may become heightened when considering stigmatized conditions, like mental health and drug use treatment. Cultural messages surrounding masculinity and reliance on willpower may also widen the gap between Black men and receiving adequate care (Klingemann & Klingemann, 2023).
Research suggests that rigid masculine norms can constrain emotional expression and psychological help-seeking among Black men, particularly in response to trauma-related distress (Coleman-Kirumba et al., 2022; Dennis & Zolnikov, 2023). In the context of cumulative trauma and structural stressors, these constraints may increase reliance on alternative coping strategies, including substance use, as a means of regulating distress while preserving masculine identity when professional support is perceived as inaccessible or stigmatizing.
These culturally and structurally rooted challenges influence how Black men cope with stress and trauma, often leading to emotion-based strategies such as distancing and finding meaning through spirituality or religiosity, which are used more frequently by Black adults than by their white counterparts (Brantley et al., 2002). Moreover, spirituality and religiosity are protective factors for Black men; however, distancing as a coping strategy can be detrimental as it may lead to destructive behaviors and discourage individuals from seeking treatment (Seidler et al., 2016).
Polysubstance Use and Coping
When systemic trauma and discrimination are minimized or unacknowledged, Black men may attribute psychological distress to individual-level stressors rather than structural oppression, increasing the likelihood of coping through substance use as a form of self-medication (Oh et al., 2025). Studies have shown that although Black men and women report similar frequency of PTSD symptoms, Black men are more likely to have substance use as a comorbidity (Cross et al., 2015). Stimulant and opioid co-use is rapidly rising among Black individuals, as is the fatal opioid-related overdose (Tanz, 2025). Individuals report using stimulants like cocaine and methamphetamine with opioids to mitigate the effects of opioid withdrawal and the anxiety of using opioids, leaving individuals feeling alert and productive (Leri et al., 2003; Rigg et al., 2025), characteristics often praised by the patriarchy.
Opioid-Stimulant Co-Use and Overdose Risk
Opioid and stimulant co-use poses a unique heightened overdose risk for Black men. Unintentional opioid exposure from fentanyl-adulterated stimulants further amplifies this danger (National Institute on Drug Abuse [NIDA], 2025). In 2022, the age-adjusted overdose death rate among Black men (69 per 100,000) exceeded that of white men (45 per 100,000) and persisted longer across the life course, declining around age 45 for white men but not until age 65 for Black men (Windsor & Reeves, 2025). In the same year, fentanyl was the leading contributor to opioid-related deaths among Black men, and cocaine-related fatalities also rose sharply (Windsor & Reeves, 2025). The complexity of polysubstance use patterns, particularly when unintentional opioid exposure occurs among individuals seeking only stimulants, underscores an urgent need to better understand overlapping risk pathways and intervention opportunities, especially as overdose deaths among Black men in their 30s and 40s are projected to rise substantially (Harris, 2023).
Current Study
This study responds to recent calls within Black psychology for research on Black men’s mental health that moves beyond homogeneous models to examine heterogeneity in trauma exposure and coping processes, including substance use (Gran-Ruaz et al., 2022; Hurd et al., 2014). Specifically, we examine patterns of trauma exposure and their associations with substance use among Black men. Using latent class analysis of 14 trauma indicators, we identified distinct trauma profiles among Black men who use stimulants and reported opioid use within the past 6 months, an understudied yet highly impacted population. We then assessed how latent class membership was associated with stimulant use, specifically crack and powder cocaine, to better understand within-group variation and its implications for polysubstance use outcomes and prevention strategies.
Theoretical Framework
Guided by the self-medication hypothesis, which posits that individuals may engage in substance use as a means of alleviating psychological distress, regulating mood, or coping with unresolved trauma (Khantzian, 1997), this study conceptualizes substance use as a coping response to traumatic stress within a polysubstance use context. This perspective is further informed by the stress and coping theory, which emphasizes that individuals respond to stressors using coping strategies shaped by available resources, prior experiences, and social context (Lazarus & Folkman, 1984). Within this combined framework, cocaine and crack use among Black men may reflect attempts to manage the lingering psychological effects of traumatic experiences, particularly in the contexts where adaptive coping resources (e.g., social support and spirituality) are constrained. These coping responses may be further shaped by structural inequities, racism, and stigma surrounding both substance use and victimization, which may limit access to social support and mental health resources (Hammond, 2010). Over time, reliance on substance use as a form of self-medication can reinforce substance dependence and increase the risk of overdose and accidental opioid exposure. Together, self-medication and stress and coping theory provide an integrated framework linking trauma exposure, coping responses, including substance use behaviors within structurally constrained contexts.
Method
Participants
The present study is a secondary analysis of data drawn from Aim 2 of the larger NIDA-funded Research Examining Factors Associated with Opioid Use Disorders Among Underserved African Americans Study (REFOCUS). The parent study examines factors influencing nonmedical prescription opioid use (NMPOU) among Black adults, with attention to differences across gender and generational lines. Aim 2 of the parent study focuses on structural, social, and cultural dynamics shaping opioid misuse, illicit drug use, and engagement with treatment services.
Eligible participants were English-proficient Black Americans, who reported nonmedical prescription or illicit opioid use in the past 6 months. Participants were stratified by age (1955–1965, 1970–1979, 1980–1994, 1995–2001) and gender. Of the 799 (n = 395 men; n = 404 women) participants who completed the survey, only complete cases of men were included in the analyses, yielding a final sample size of 389.
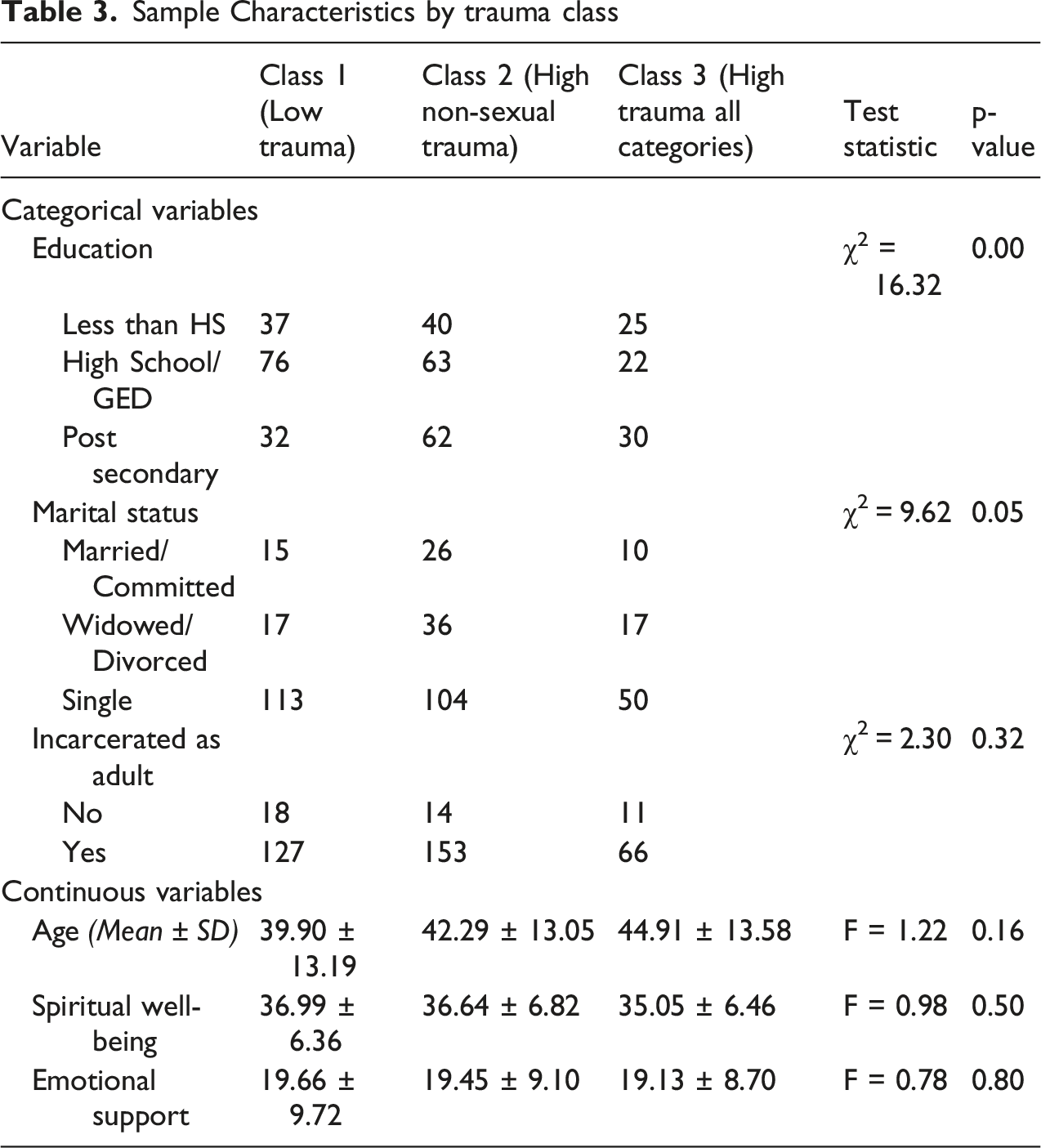
Participants ranged in age from 18 to 69 years (M = 41.92, SD = 13.30). Most participants had a high school diploma or GED (41.48%) and were single (68.27%), with an additional 18.53% reporting being divorced or widowed. The majority of participants reported a history of incarceration during adulthood (88.83%). The mean emotional support score was 19.43 (SD = 9.25, range = 0–32), and the mean spiritual well-being score was 36.49 (SD = 6.59, range = 7–42). Demographic characteristics by latent class membership are presented in Table 3.
Measures
Sociodemographic Characteristics
Standard demographic variables included age, gender, and educational attainment (e.g., less than high school, high school/GED, and postsecondary). Incarceration history as an adult was also measured with a yes/no item.
Substance Use
Lifetime substance use was assessed using two dichotomous items indicating whether participants had ever used crack cocaine or powder cocaine.
Emotional Support
Perceived emotional support was measured using the subscale from the NIH Toolbox Adult Relationship Scale (Cyranowski et al., 2013). The emotional support subscale consists of eight items (e.g., “I have someone who will listen to me when I need to talk”), rated on a 5-point Likert scale ranging from 0 (never) to 4 (always). Items were summed, with higher scores indicating greater perceived emotional support.
The emotional support subscale has demonstrated excellent internal consistency in prior research (i.e., α = .96) (Cyranowski et al., 2013). Subsequent work has confirmed strong reliability and stable performance of the NIH Toolbox social relationship measures across diverse adult samples (Salsman et al., 2013). Evidence for convergent validity is supported by strong positive correlations with other established measures of social support and interpersonal functioning, whereas discriminant validity has been demonstrated through weak or nonsignificant associations with unrelated physical health constructs (Cyranowski et al., 2013). The subscale has been previously used in adult Black samples, including a study examining emotional support and opioid misuse among Black adults (Smith et al., 2025). Internal consistency in the current sample was excellent (α = .96).
Life Events
Exposure to potentially traumatic events was assessed using a modified version of the Life Events Checklist for DSM–5 (LEC-5; Weathers et al., 2013), a self-report measure of lifetime exposure to a range of traumatic experiences (e.g., physical assault, serious accidents, witnessing violence). In the current study, 14 items were included, with responses coded as 0 (never happened to me/never witnessed) or 1 (happened to me/witnessed).
Prior research supports the construct validity of the LEC-5, with evidence of adequate temporal stability, good convergent validity with other validated trauma exposure measures, and expected associations with PTSD symptoms and psychological distress (Gray et al., 2004). Consistent with this work, studies of the LEC-5 demonstrate associations with clinician-assessed trauma exposure and posttraumatic stress symptom severity, alongside weaker associations with unrelated psychopathology, supporting both convergent and discriminant validity (Weathers et al., 2013). The LEC-5 has also been widely used to assess trauma exposure in racially and ethnically diverse populations (Crouch et al., 2024). Internal consistency in the current sample was acceptable (α = .81).
Spiritual Well-Being
Spiritual well-being was assessed using a 7-item abbreviated version of the Spiritual Well-Being Scale (SWBS), which measures religious well-being (relationship with God or personal spirituality) and existential well-being (sense of meaning and purpose in life). Items (e.g., “I have a personally meaningful relationship with God”) were rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree) and summed, with higher scores indicating greater spiritual well-being.
The Spiritual Well-Being Scale (SWBS) has demonstrated good to excellent internal consistency across multiple studies, with original validation work reporting Cronbach’s α values in the high .80s (Ellison, 1983) and subsequent reviews documenting reliability estimates ranging from the .80s to .90s across diverse populations (Paloutzian & Ellison, 2009). Evidence also supports a stable two-factor structure and construct validity, with SWBS scores correlating positively with indicators of general well-being and psychological adjustment while remaining conceptually distinct from measures of mental and physical health (K. Bufford et al., 2023). In the current study, internal consistency was good (α = .87).
Procedures
Data were collected between November 2021 and October 2025. Recruitment occurred through flyers, community events, neighborhood canvassing, and targeted social media ads. Interested individuals contacted the team via email, phone, or QR code and completed eligibility screening before providing consent and participating in an interview. Surveys were administered using audio computer-assisted self-interviewing (ACASI) and computer-assisted personal interviewing (CAPI) methods. To ensure cultural sensitivity, all data were collected by race-matched study staff (Januszka et al., 2007).
Data Analytic Plan
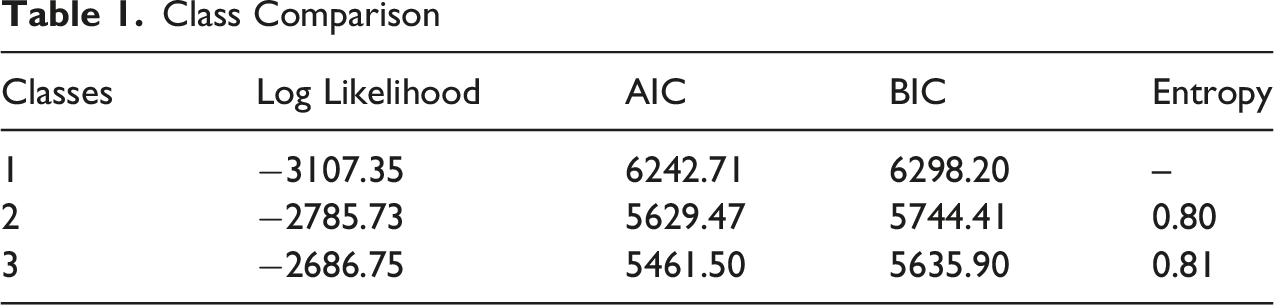
Latent class analysis (LCA) was used to identify subgroups of Black adult men who use opioids and stimulants based on trauma histories (Weller et al., 2020). Fourteen dichotomous indicators from a modified LEC-5 (Weathers et al., 2013) captured exposure to potentially traumatic events among the participants. Analyses were conducted in Stata/BE 17.0 using an unconditional model to allow trauma indicators to define class structure independent of covariates. Models were estimated via maximum likelihood using the default expectation–maximization (EM) algorithm in Stata, under the assumption of local (conditional) independence of indicators within classes (Lanza et al., 2018). Model selection relied on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and entropy. Participants’ most likely class membership was then used as a predictor in logistic regressions examining associations with lifetime crack and powder cocaine use, adjusting for sociodemographics, emotional support, and spiritual well-being. Robust standard errors accounted for heteroskedasticity.
Results
Latent Class Enumeration and Model Fit
Class Comparison
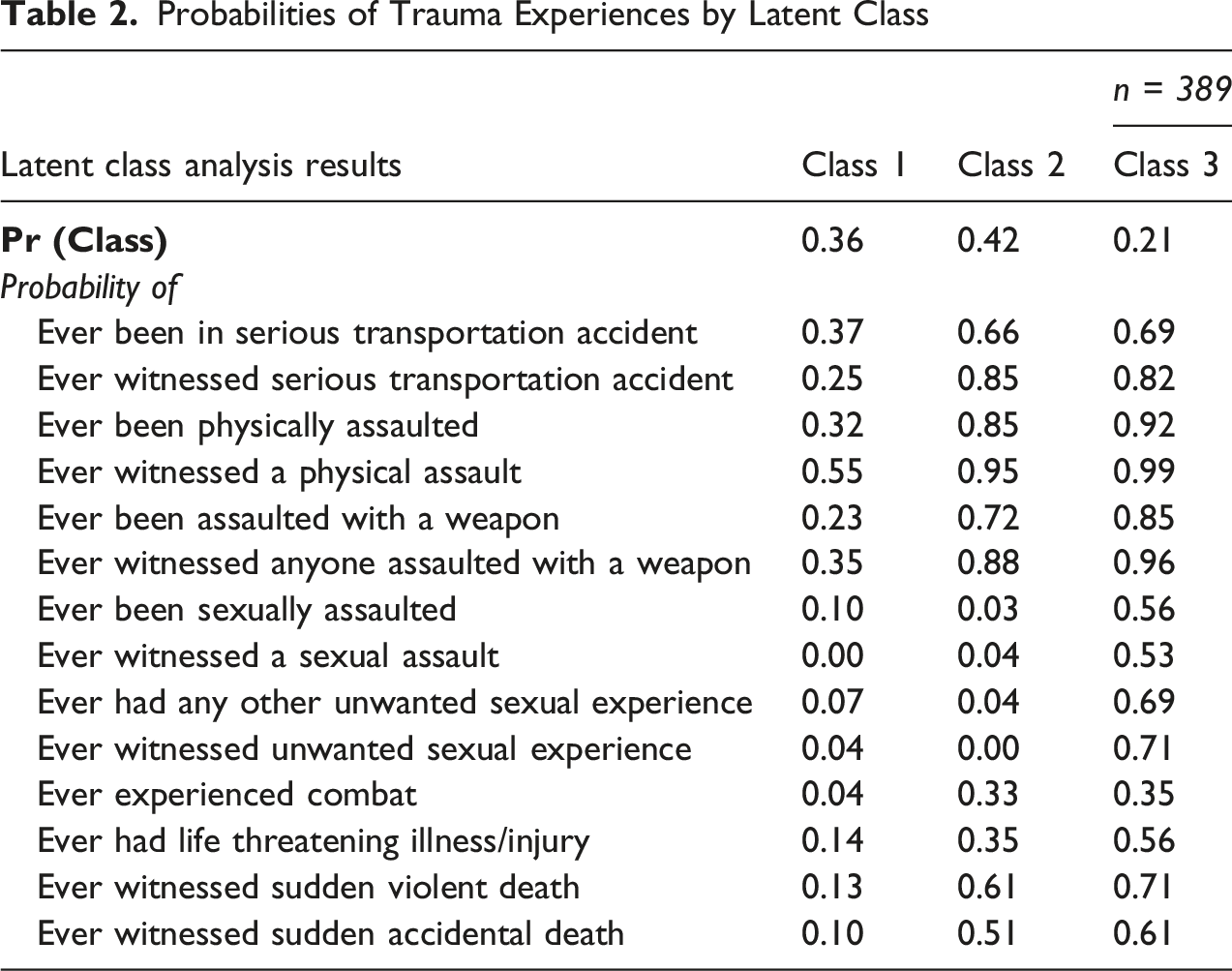
Trauma Class Characteristics
Probabilities of Trauma Experiences by Latent Class
Bivariate Differences by Trauma Class
Sample Characteristics by trauma class
Trauma Class and Substance Use
Binary Logistic Regression Predicting Stimulant Use by Most Likely Class
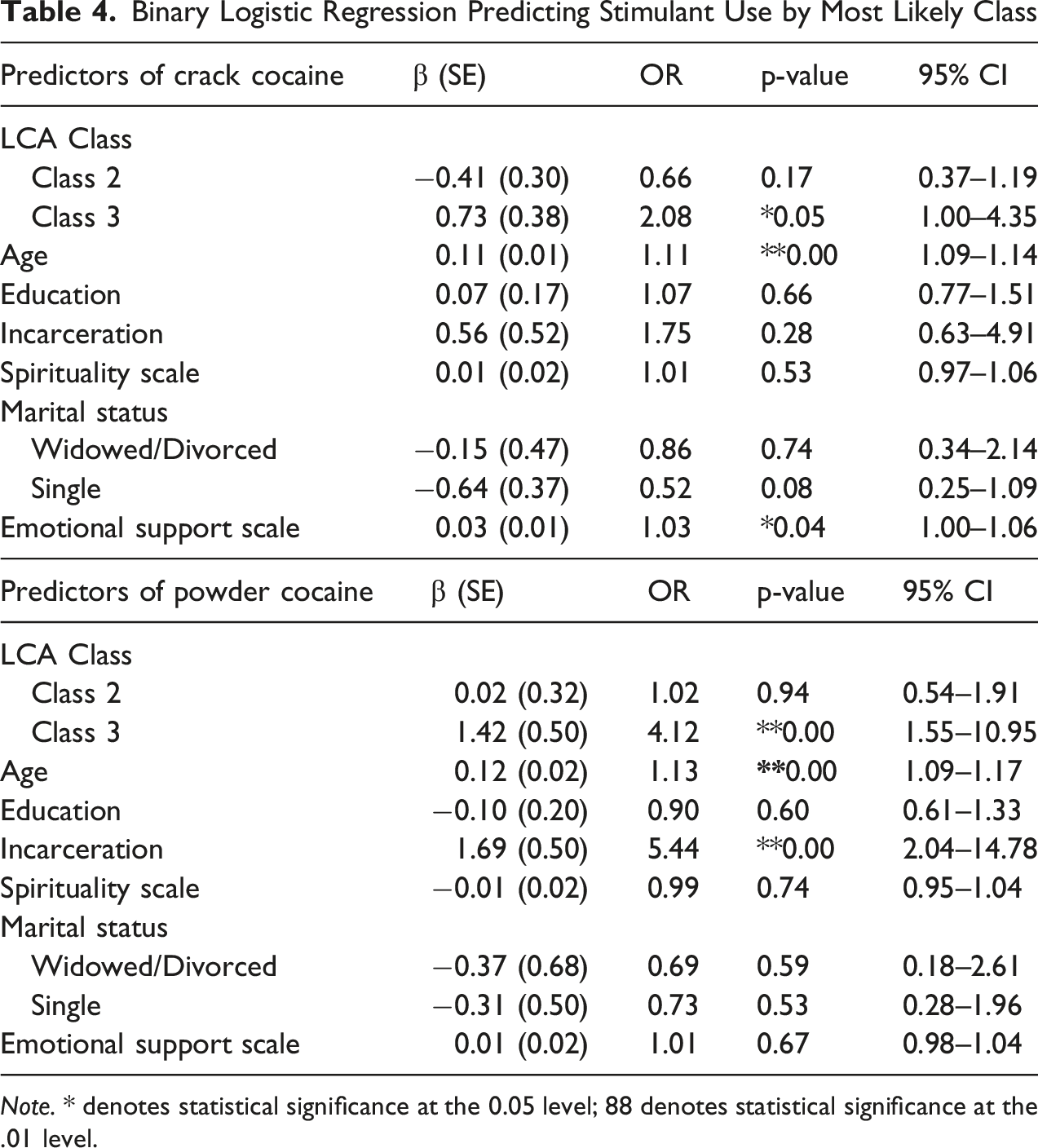
Note. * denotes statistical significance at the 0.05 level; 88 denotes statistical significance at the .01 level.
In the powder cocaine use model, membership in Class 3 was significantly associated with higher odds of use (OR = 4.13, p = .00, 95% CI = 1.55–10.95), while Class 2 was not significantly different from Class 1.
Among the covariates, older age was positively associated with both crack (OR = 1.11, p < .001, 95% CI = 1.09–1.14) and powder cocaine use (OR = 1.13, p < .001, 95% CI = 1.10–1.17). Incarceration history was significantly associated with higher odds of powder cocaine use (OR = 5.44, p = .00, 95% CI = 2.04–14.48) but not crack cocaine use. Greater emotional support was significantly associated with increased odds of crack cocaine use (OR = 1.03, p = .04), though it was not associated with powder cocaine use. Additionally, single marital status approached significance and was associated with lower odds of crack cocaine use (OR = 0.52, p = .08). No other covariates were significantly associated with either outcome.
Discussion
The current study aimed to identify latent subtypes of trauma experiences among Black men who co-use substances, and to determine the extent to which these subtypes predict powder and crack cocaine use. Three trauma subtypes were identified. Low trauma (class 1), High Non-Sexual Trauma (class 2), and High Trauma Across All Categories (class 3). Class 3 was significantly associated with greater odds of lifetime powder cocaine and lifetime crack use compared to Class 1. No differences between Class 2 and Class 1 in odds of lifetime cocaine use were detected. The present findings advance the limited literature on trauma experiences among Black men, a group often underrepresented in substance use research.
Sexual trauma, including sexual assault and childhood sexual abuse, is robustly linked to substance use in general populations (Khoury et al., 2010; Kihas et al., 2024; Levin et al., 2021). However, far less is known about how sexual trauma operates within the broader patterns of trauma among Black men who may underreport such experiences due to stigma and cultural norms. The current study found that cocaine and crack use were more likely among men classified in the High Trauma Across All Categories profile, a class characterized by co-occurring sexual, physical, and violent trauma exposures. These findings should be interpreted as reflecting associations with trauma profiles, rather than the independent effect of any single trauma type.
The elevated risk observed among the High Trauma Across All Categories class may reflect the cumulative psychological burden associated with exposure to multiple forms of trauma. Sexual trauma, as one component of the broader trauma profile, has been linked to lower self-esteem, greater self-criticism, less secure attachment style, and heightened internalized shame (Dorahy & Clearwater, 2012; Schnittker, 2022). The impact of trauma on a sense of personal power and control may be particularly salient for Black men due to chronic experiences of racial discrimination and systematic disadvantage that impede a sense of personal agency (Khazvand et al., 2022). In addition, culturally grounded masculine norms emphasizing emotional restraint, self-reliance, and resilience, as well as a desire to avoid appearing vulnerable, may further deter help-seeking for traumatic experiences among Black men. Prior research suggests that these norms are linked to greater frequency of substance use as means of coping with sexual trauma for Black men relative to men of other races (Myrie & Schwab, 2023; Payne et al., 2014). The multiplicative effect of these experiences may explain why Black individuals with sexual trauma have more severe PTSD symptoms than other races (Ceroni et al., 2023).
Despite these potential implications, sexual trauma remains understudied among Black men, likely due to lower reported prevalence relative to White individuals and Black women (Clark et al., 2012) and prior evidence suggesting stronger associations between sexual abuse and substance use among women (Hyman et al., 2008). The current findings suggest that even when sexual trauma is underreported (Thomas & Kopel, 2023), its presence within the broader pattern of cumulative trauma exposure may be particularly relevant for understanding cocaine use risk among Black men. Importantly, sexual trauma is also associated with various other comorbid mental health concerns (Chen et al., 2010), suggesting that men in the High Trauma Across All Categories class may have high symptom acuity in other domains that may require additional services and resources. Given the growing risk of fatal overdose associated with cocaine use among Black men (Volkow, 2024), these findings underscore the urgency of trauma-informed, culturally responsive interventions for this population.
While trauma class membership was significantly associated with both lifetime use of powder cocaine and crack cocaine, the difference in magnitude of these associations suggests need for further study. Our findings are consistent with previous research examining associations between crack and cocaine use and trauma among predominately Black samples (Jester et al., 2024; Zapolski et al., 2016). Crack cocaine use is typically more strongly associated with structural disadvantage that predisposes individuals to encountering and witnessing traumatic events, such as neighborhood disorder and disinvestment, whereas cocaine use is associated with higher socioeconomic status (Palamar et al., 2015; Sterk et al., 2014). Thus, it might be expected that the strength of the association between membership in the High Trauma Across All Categories class would have been more pronounced in the crack cocaine model compared to the powder cocaine model. Contrarily, our models showed that belonging to the most severe trauma class was associated with four-fold greater odds of powder cocaine use, whereas it was associated with two-fold greater odds of crack cocaine use. One other study found a similar difference in robustness of association between crack/cocaine and sexual trauma in all Black sample (Zapolski et al., 2016). This previous study noted potential methodological limitations that may have contributed to this finding that may also be reflected in the current sample (i.e., lower proportion of the sample used crack compared to powder cocaine). It may be that crack cocaine use is more robustly predicted by socioeconomic indicators, whereas powder cocaine has stronger direct associations with cumulative psychological burden reflected in the severe trauma profiles.
Other Predictors
Age
Older men were more likely to report lifetime crack and powder cocaine use, regardless of trauma class, consistent with previous literature that finds that older Black men are more likely than younger Black men to experience fatal overdose from unintentional opioid exposure during stimulant use (e.g., fentanyl in cocaine; Volkow, 2024), indicating potential greater use among older men. Alternatively, this pattern may be elucidated by the Subcultural Evolution and Illicit Drug Use theory (Golub et al., 2005), which highlights that there are different drug eras and norms that shape drug patterns among subcultures. The current findings appear to indicate a subculture and norm of cocaine use among older Black men, compared to younger generations.
Further, if Black men (regardless of trauma) utilize stimulants to manage mental health due to trauma as previously established in literature (Dangerfield et al., 2020), then clinicians working with this population should explore coping strategies for reported trauma-related symptoms among Black men using stimulants. Additionally, clinicians should prioritize exploring motivations to use with this sample as this population may not be forthcoming about difficult mental health and trauma symptoms given their diminished likelihood to seek help for such experiences (Motley & Banks, 2018).
Incarceration
Black men with an incarceration history were more likely to report lifetime powder cocaine use, but not lifetime crack cocaine use. Notably, the relationship between incarceration and substance use is cyclical as 85% of the prison population has an active substance use disorder or was incarcerated for a crime involving drugs (NIDA, 2020). Given the cross-sectional nature of the current data, this study is unable to delineate the specific complex patterns between incarceration and substance use, but results are consistent in that there is a relationship between these variables.
The finding that incarceration history was associated with powder cocaine use but not crack cocaine use may also be explained by the sampling in the current study. Specifically, the Black men in this study also misuse opioids, and powder cocaine is more likely to be mixed with opioids, like fentanyl, than crack cocaine (Wagner et al., 2023). Therefore, this study may have inherently recruited participants more likely to use powder cocaine, regardless of incarceration history. Importantly, the current study did not examine specific co-use patterns of stimulants and opioids, and future research should examine these patterns of use more distinctly to see if results replicate. Nonetheless, implications suggest a focal need for successful reentry skills for Black men who use stimulants, particularly powder cocaine.
Emotional Support
Surprisingly, as emotional support increased, participants were more likely to report lifetime crack cocaine use, but not powder cocaine, even though increased support has been shown to be associated with decreased substance use among Black adults (Miller-Roenigk & Stevens-Watkins, 2025). This result may indicate that among Black men, other types of support (i.e., instrumental support) may be more relevant than emotional support. Further, opioid use can lead to deficits in emotion recognition and social bonding (Nummenmaa & Tuominen, 2018). Given that our study sample consisted of men who used opioids within the past six months, it is possible that participants may perceive high levels of emotional support even when such support is limited. This perceived support could be associated with increased stimulant use, as stimulant use can produce emotionally reinforcing effects (Substance Abuse and Mental Health Services Administration [SAMHSA], 1999). Providers should therefore assess the types and quality of social support, particularly emotional support, among Black men who use both stimulants and opioids.
Relationship Status, Spiritual Well-Being, and Education
The remaining predictors, including relationship status, spiritual well-being, and education, were not significantly associated with stimulant use. However, relationship status did approach significance, with single men less likely to report lifetime crack use than married men. This may reflect the influence of relationship quality or partner substance use, as supportive partnerships can protect against substance use, while partner use may increase risk (Fleming et al., 2010). In this sample, relationship quality may not have been positive, or participants may have used substances with their partners, which could explain why single men reported less use. Future studies should assess relationship quality and partner substance use to better understand their role in stimulant use among Black men.
Spiritual well-being and education were also unrelated to stimulant use. Although spirituality is often protective against substance use among Black adults (Kane et al., 2024), it may be less relevant for Black men, who might seek support from other sources (Staton-Tindall et al., 2013). Education similarly showed no association with stimulant use, contrary to prior research linking higher education to reduced substance misuse (Ford et al., 2020). Informal education, such as programs in justice settings, may be more protective than formal education, particularly given the high rate of incarceration in this sample. Future research should explore how informal education influences stimulant use among this population.
Implications
The findings of this study have implications for both clinical and community settings. Interventions addressing the intersection of stimulant use and trauma among Black men should consider intragroup differences, including the distinct trauma profiles identified. Men exposed to personal or vicarious sexual trauma are at increased risk for stimulant use; thus, integrated trauma-focused treatments such as Concurrent Treatment of PTSD and SUDs Using Prolonged Exposure (COPE), a manualized cognitive behavioral therapy (CBT)-based approach addressing both PTSD and relapse prevention (Persson et al., 2017), may be beneficial. COPE has shown efficacy among Black women with alcohol use disorder (Jaconis et al., 2017), suggesting promise for adaptation among Black men with SUD. Its successful telehealth delivery also highlights potential to reduce treatment barriers and address health disparities affecting Black Americans.
Seeking Safety is another evidence-based intervention designed to treat co-occurring substance use and trauma-related stress (Najavits, 2002). It is a cost-effective and flexible program that can be delivered in both community and correctional settings through group or individual psychotherapy by peers or professionals (Najavits, 2002; Washington State Institute for Public Policy, 2024). The modality is not substance- or gender-specific and does not require a formal PTSD diagnosis. A meta-analysis by Sherman and colleagues (2023) found that Seeking Safety significantly reduced trauma symptoms and substance use at six and three months post-intervention, respectively, showing medium to large effects for trauma and small to medium effects for substance use across seven randomized clinical trials. However, most trials have focused on female and community-based samples (Sherman et al., 2023). Given the present findings that sexual trauma may be central to dual-diagnosis presentations, further research is needed to examine treatment outcomes among Black men, as existing studies have primarily focused on women (Karlsson et al., 2024). Clinicians should adapt manualized treatments like Seeking Safety to align with patient values and cultural context, consistent with evidence-based practice principles.
Given that 88% of the sample had prior incarceration, integrating evidence-based interventions into correctional settings is also critical. Research shows that completion of residential substance use programs within prisons predicts lower rates of arrest and substance use 6 months post-release (Pelissier et al., n.d.). One promising approach is contingency management (CM), a CBT-based intervention shown to be effective for stimulant use disorders (Bentzley et al., 2021; Rash, 2023). CM uses a token economy model that provides tangible rewards for abstinence (Rash, 2023). In a meta-analysis of 157 clinical trials, CM was the only psychotherapy significantly associated with urinalysis-confirmed stimulant abstinence (Bentzley et al., 2021). Notably, CM is already a core component of the Federal Bureau of Prisons’ Drug Abuse Programs, underscoring its feasibility and potential impact for justice-involved populations.
A final key implication of these findings is the critical role of naloxone in reducing opioid overdose mortality. Naloxone rapidly reverses opioid overdose, restoring breathing and consciousness. Since individuals experiencing an overdose often cannot self-administer naloxone, identifying a trusted support person is essential (Green et al., 2014). Clinicians should emphasize carrying naloxone and ensure both clients and their support networks are trained in its use. Barriers include stigma and fear of criminalization, low perceived risk, discrimination in healthcare (e.g., prescription access), and limited availability in pharmacies serving low-income neighborhoods (Abbas et al., 2021; Miller et al., 2023; Seo et al., 2023; Tilhou et al., 2024) Education about fentanyl contamination in the drug supply is critical for individuals using stimulants alone or with opioids. Policies should focus on expanding naloxone access and promoting harm reduction. Integrating these strategies can directly reduce overdose risk and enhance safety among Black men who use stimulants and opioids.
Strengths, Limitations, and Future Directions
This study has several strengths. Unlike continuous or count-based trauma measures, latent class analysis captures heterogeneity in trauma exposure patterns, allowing identification of distinct profiles of trauma rather than assuming a linear accumulation of events. This approach is particularly relevant for understanding trauma among Black men, whose experiences may cluster around specific combinations of interpersonal, structural, and sexual violence with distinct implications for substance use behaviors. The results identified covert trauma patterns among Black men and their association with stimulant use, providing insight for interventions targeting a high-overdose-risk population in a southern state (Freeman et al., 2023). Future research should examine broader samples to test replicability.
Limitations include the cross-sectional design and reliance on lifetime variables, which limit causal inference; future research should include longitudinal studies to assess the relationships over time. Further, self-reported substance use may be affected by recall or social desirability bias, though it remains valid among vulnerable populations (Garg et al., 2016). Additionally, trauma classes combined different exposure types; future studies should separately examine witnessing, experiencing, and learning about trauma to assess differential effects on stimulant use. Finally, this study estimated an unconditional latent class model, which prioritized identifying trauma profiles based solely on patterns of trauma exposure. Although this approach preserves interpretability of trauma classes, it does not account for the potential influence of sociodemographic or psychosocial factors on class membership. Future research could examine covariates as predictors of class membership using conditional or three-step modeling approaches.
Conclusion
This study highlights the significance of examining patterns of trauma among Black men who co-use substances. The findings suggest the need for trauma-informed and culturally responsive interventions that address both substance use and overdose risk within this population, while acknowledging differences between the substances used (e.g., powder vs crack cocaine) and incorporate naloxone education and expanded access. Such strategies should be integrated across clinical, community, and reentry settings to support holistic recovery and overall well-being. Future research directions should expand these findings to deepen understanding of the intricacies of how traumatic experiences shape substance use trajectories among Black men, an understudied yet disproportionately effected group.
Footnotes
Ethical Considerations
This study was approved by the University of Kentucky institutional review board.
Consent to Participate
Informed consent was obtained from all participants in the study.
Author Contributions
All authors have made substantial contributions to the development of this manuscript and meet the criteria for authorship. The first author was responsible for conducting data analysis and interpreting the results. Additionally, the first author led the writing, editing, and submission process, with support from the second author. The third, fourth, and fifth author contributed to writing the manuscript. The sixth author conceived the study, obtained funding, and provided critical input and support throughout the writing and editing process. All authors reviewed and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the National Institute on Drug Abuse through Grants R01-DA049333 (Principal Investigator: Danelle Stevens-Watkins), T32-DA035200 (Principal Investigators: William Stoops & Craig Rush), and R25-DA035163 (Principal Investigators: Carmen Masson & Gideon St. Helen). The views expressed herein are solely those of the authors and do not reflect the official stance of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.