
Abstract
Nondiscrimination rules—statutes, regulations, and soft law protections—are critical for reducing health and health care disparities. Although scholarship has interrogated how nondiscrimination rules affect behavior by discriminators, comparatively little has considered how protections can affect choices made by members of protected groups. A number of states and some interpretations of federal law protect people from discrimination on the basis of sexual orientation. This Article seeks to identify relationships between actual state law, perceived state law, and experiences of discrimination and medical mistrust. This Article reports the results of a national cross-sectional survey of over 3,000 men using Grindr to meet male partners. Participants scored comparable to chance in knowledge about state nondiscrimination protections, with “optimistic errors” (erroneous beliefs that one was protected) significantly more common than pessimistic errors. Perceptions of protection were significantly correlated with lower medical mistrust and greater uptake of care, as well as lower perceived barriers to disclosure and care-seeking. Actual state law protections, however, were significant predictors of having had discussions with providers that depended on disclosure of sexual behavior or orientation. Building on these results, this Article considers pathways by which nondiscrimination law may exert welcome mat (and “unwelcome mat”) effects.
INTRODUCTION
These are tumultuous times for nondiscrimination law. The Department of Health and Human Services (“HHS”) has proposed new regulations that strip LGBT populations of nondiscrimination protections in health care, and these rules have also narrowed protections for people with limited English proficiency. 1 Along with other changes, these revisions have undermined the reach of § 1557 of the Affordable Care Act (“ACA”), which extends civil rights protections to health care entities receiving federal funds. The Office of Civil Rights within HHS has redirected its emphasis away from protecting patients alleging discrimination, and has enacted new regulations protecting providers who refuse patients services due to religious or conscience-based objections. 2 Despite a favorable circuit court interpretation of Title VII of the Civil Rights Act as protecting against employment discrimination on the basis of sexual orientation, the issue is now pending determination by a majority-conservative Supreme Court. 3 Protections “on the basis of sex” under Title IX of the Education Amendments are also in flux, with the Obama and Trump administrations taking contrary views on whether protections “on the basis of sex” extend to sexual orientation and gender identity. 4 States are widely diverging in their protections, or lack thereof, for sexual and gender minorities. 5
In health care settings, advocates fear that lax or absent protections will allow continued discrimination against patients, and that discriminatory experiences will discourage care-seeking. 6 This is an important pathway by which law may influence patient choices, but there is another pathway: separate from experiences of discrimination, the presence or absence of nondiscrimination laws may exert expressive effects that shape patient decision-making. In order for law to either encourage or chill engagement, however, individuals in protected groups need to be aware of what the law has provided. This Article uses state variation in health care nondiscrimination protections for LGB individuals to understand how people's perceptions of protection are related to choices about entering (un)protected spaces.
Statutory nondiscrimination protections such as ACA § 1557 and its state law equivalents have given rise to analyses testing whether such laws are indeed effective in producing equal treatment and reducing marginalization. 7 These analyses, however, typically consider the extent to which such laws deter discriminatory actions by gatekeepers in health care, education, the workplace, and housing. Theories by which nondiscrimination laws may affect discriminators' behavior include two principal mechanisms. First, the laws have an incentive impact, in that they make discrimination costlier. Second, the laws have an expressive impact: 8 namely, they convey that there is a social norm against discrimination, and discriminators who wish to conform with social expectations are more likely to refrain from unequal treatment.
This Article shifts the focus to considering the effects of nondiscrimination rules for the attitudes and behaviors of protected beneficiaries, who hold a new legal entitlement to participate in a domain on equal terms. The expressive impacts of law may change not only the decisions of gatekeepers, but also the decisions made by beneficiaries themselves. This is a new theoretical focus for research on expressive law, which has typically considered how laws communicate information to people who must act, 9 rather than to people who have a new legal entitlement. This Article also adds to ongoing work on how people develop expectations about legal rules—such as through motivated reasoning about what the law should be, or deductive reasoning that infers law from social experiences.
In the health care context, patient care-seeking behaviors and doctor-patient communication are important drivers of disparities in quality of care. Discrimination in care settings is independently harmful for quality of care, but also indirectly harmful through discouraging health-promoting patient behaviors such as uptake of preventive care services and adherence to medication. 10 Care-seeking and disclosure of personal information in care settings are complicated for patients experiencing discrimination, which can amplify medical mistrust and associated communication barriers, as well as exacerbate internalized stigma and the effects of discrimination-related stress. 11
As part of a project on access to health care and HIV prevention services, I have previously studied how discrimination may affect patients' care-seeking behaviors. 12 In a set of qualitative interviews and focus groups with gay men, bisexual men, male sex workers, and other men who have sex with men, I explored experiences with health care discrimination, care-seeking, and disclosure. Evidence from these findings suggested that past and anticipated health care discrimination on the basis of sexual orientation can affect patient decisions and access to care. Specifically, past and anticipated discrimination can deter care-seeking, reduce or complicate disclosure, and exacerbate medical mistrust.
This Article moves from qualitative to quantitative evidence, by way of an original nationwide survey addressing perceptions of state laws intended to bar discrimination on the basis of sexual orientation. I gathered quantitative data from a large cross-sectional survey study of over 3,000 men using the dating application Grindr to meet male partners, with the goal of assessing how perceived and actual legal rules are correlated with medical mistrust, past discrimination, barriers to accessing care, and care-seeking. This survey collected data nationwide, and regression analyses identified relationships among perceived law, actual law, and a range of patient care-seeking behaviors and attitudes.
The survey has several key findings. First, people are often wrong about the law. Many participants in the national survey were uncertain or inaccurate about legal protections, and they erred in a systematic way: far more participants erroneously believed themselves to be protected in the absence of a rule, compared to the erroneous belief that no law existed. I consider possible explanations for this, including confusion between state and federal law, the possibility that people deduce the law from their social experience, 13 or the possibility that people reason about law on the basis of their normative preferences. 14
Next, I identify associations that are consistent with the view that perceived legal protections are related to patient engagement and care-seeking, although the data in this study were correlational rather than causal. Perceived legal protections were associated with lower medical mistrust and greater likelihood of having a primary care provider and a recent HIV test; actual law had fewer significant associations with variables of interest. Although law in the mind does not always fit law on the books, it may exert greater influence in shaping patient behaviors, which opens new directions for thinking about models of expressive law and the development of legal consciousness. These findings also raise difficult normative questions, such as whether misperceptions about the law should be corrected (or induced), and whether it is problematic if some rules reshape private vigilance about discrimination.
This Article proceeds in three Parts. In Part I, I outline the state of nondiscrimination protections in health care settings, focusing specifically on sexual orientation discrimination. Part I also highlights several theoretical pathways by which legal rules may exert expressive effects on beneficiaries' engagement in protected domains, all mediated through beneficiaries' perceptions of legal protection. Part II presents the findings of the national survey. Part III considers explanations for the associations observed here, including alternative views of law as conveying information (expressive theories), as a marker for contemporaneous social norms (legal consciousness theory), as the embodiment of normative aspirations (motivated reasoning), or as a direct incentive for compliance (the traditional deterrence view).
I. NONDISCRIMINATION PROTECTIONS IN HEALTH CARE
Research across multiple bases of discrimination—including sexual orientation discrimination, but also discrimination on the basis of race, sex including gender identity, language, disability including HIV status, weight, mental illness, history of drug use, national origin, and poverty—has found that experienced and anticipated discrimination can amplify medical mistrust, intensify internalized stigma, discourage or delay care-seeking, undermine adherence to long-term courses of treatment, and inhibit disclosure of relevant information in care settings. Each of these mechanisms contributes to disparities in the quality of care and patient outcomes. 15 Patients vulnerable to discrimination in health care are simultaneously likely to experience stigma and discrimination in other life domains as well (e.g., employment, housing), 16 which can increase social marginalization and deplete the socioeconomic resources that patients may need to advocate for improved quality of care.
Discriminatory experiences and lack of cultural competence in care can be common for patients in sexual minority communities. A national survey in 2014 found that 56% of gay, lesbian, and bisexual patients and 70% of transgender patients reported care refusals, rough treatment, blaming, or harsh language, 17 and a 2017 survey found that 8% of lesbian, gay, and bisexual patients and 29% of trans patients had been refused care in the prior year. 18 For patients who are members of sexual minority groups, discrimination in health care compounds other sources of marginalization. These dynamics culminate in poorer health outcomes for sexual minority groups, who have elevated incidence of hypertension, ulcers, pneumonia, tuberculosis, liver disease, asthma, headaches, allergies, arthritis, gastrointestinal difficulties, greater incidence and severity of cancer, higher cardiovascular disease, increased substance use, and experiences of violence. 19
Although nondiscrimination laws in health care settings cannot alleviate the structural sources of these disparities, they represent significant efforts to improve the quality and sensitivity of care. The understanding of how such laws may affect the frequency and severity of discrimination has been the focus of prior scholarship, which tends to show reduced engagement in discrimination. But comparatively less attention has focused on how these protections may shape patients' behaviors. This Part will consider federal statutes, state statutes, local ordinances and soft law protection against discrimination in health care settings, followed by a brief summary of prior work evaluating the impacts of such laws.
A. Nondiscrimination Rules for Health Care Providers
In the absence of a federal constitutional right to health or health care, access to care in the United States depends on statutory rights, the boundaries of insurance policy contracts, and patients' ability to pay. Even where physicians are contractually or statutorily bound to treat an individual patient, federal and state conscience protections may safeguard the refusal of particular treatments on moral or religious grounds. 20 Nondiscrimination laws in health care are a recent innovation against this backdrop. Although nondiscrimination laws impose no independent, binding obligations to treat individual patients, they do prohibit the refusal of individual patients or treatments for discriminatory reasons. 21
1. Statutory Protections
Historically, the reach of federal nondiscrimination statutes—such as the Americans with Disabilities Act, the Federal Rehabilitation Act, the Civil Rights Act, the Age Discrimination Act of 1975, and Title IX of the Education Amendments Act—has been limited in health care settings. Prior to 2010, the applicability of these statutes to clinical care depended on statutory definitions of “public accommodation” (some of which—such as the definition in Title II of the Civil Rights Act—do not include hospitals or physicians' offices), receipt of federal funding for the purposes of applying Title VI of the Civil Rights Act, or the delivery of care within an “education program or activity” in the case of Title IX. 22
The ACA, however, vastly expanded the reach of these protections, and for the first time prohibited sex discrimination by health care providers outside educational settings. Section 1557 of the ACA applied each of the above-mentioned statutes (with the exception of the ADA) to “any health program or activity, a part of which is receiving Federal financial assistance,” defined broadly to include “credits, subsidies, or contracts of insurance.” 23 Moreover, the structure of ACA tax credits and cost-sharing reduction payments expanded the reach of federal funding, enabling these nondiscrimination rules to cast a far wider net than prior protections. The HHS Office of Civil Rights has construed § 1557 broadly to reach all institutional health care providers receiving federal funds, as well as individual providers who receive federal funds from sources other than Medicare Part B. 24 As of 2016, HHS had interpreted the law's substantive protections broadly when implementing regulations, finding private rights of action for disparate impact claims arising under every statute; 25 expanding sex discrimination to include discrimination on the basis of gender identity and history of pregnancy termination; 26 and announcing an intent to prohibit sexual orientation discrimination as a Title IX violation where it is founded on sex stereotyping. 27
Like many provisions of the ACA, however, these laws have been truncated or reversed in the current administration. Regulations extending ACA § 1557 protections on the basis of gender identity and pregnancy termination history were enjoined nationwide in the 2016 Franciscan Alliance case as likely violations of the Religious Freedom Restoration Act (“RFRA”) and the Administrative Procedures Act. 28 The rules were remanded to HHS for reconsideration. Observers who were attentive to the new administration's positions on gender identity, 29 sexual orientation, 30 and religious exceptions to legal mandates 31 had little reason for optimism.
The new proposed federal regulations interpreting § 1557 were issued in May 2019. 32 These regulations aim for a broad construction that would eviscerate even some nondiscrimination protections that existed before the ACA. 33 Protections on the basis of gender identity, sex stereotyping, and sexual orientation have been eliminated, and providers no longer need post signs to alert the public to their § 1557 rights. 34 Moreover, the regulations also remove nondiscrimination protections for LGBT individuals from ten other regulations reaching HHS programs beyond Medicaid, including programs that were not originally covered by § 1557. 35 The rules also note that covered entities may not be required to protect individuals on the basis of sexual orientation and gender identity, suggesting that state laws that conflict with this (presumably by establishing state law nondiscrimination protections for LGBT patients) are preempted. 36 All enforcement authority for § 1557 is delegated to Office of Civil Rights under these new rules, and the regulations eliminate protections for claimants against retaliation or intimidation. 37 Finally, although the 2016 guidance supported a private right of action (and even as providing a private right of action to sue for disparate impact claims) the new regulations are silent on this interpretation. 38
Litigation is ongoing to determine whether other federal statutes can provide protection on the basis of sexual orientation. In the Civil Rights Act, Titles VI and VII apply respectively to federally funded programs and employment. Title VI does not prohibit sex discrimination, 39 which limits its utility for sexual orientation discrimination in federally funded health care programs. But Title VII does bar sex discrimination in employment settings, and these protections extend broadly to prohibit “sex stereotyping,” whereby individuals experience discrimination because they do not fit the stereotypes for their biological sex. 40 The pending Supreme Court decision in Altitude Express v. Zarda will determine whether Title VII's prohibition of sex stereotyping extends to employment discrimination against LGB people, due to nonconformity with straight sex stereotypes. 41 This matters for health care employees, but it can also influence protections for patients. Interpretations of “sex” in Title VII often influence the reading of analogous language in Title IX of the Education Amendments Act of 1972, which bars discrimination on the basis of sex in educational settings. 42 Section 1557 of the ACA explicitly incorporates Title IX and makes it applicable to federally funded health care programs. 43 If Title VII is interpreted as barring discrimination due to sexual orientation (i.e., because discrimination against LGB people is based on nonconformity with straight sex stereotypes), this will be instructive for interpretations of Title IX and § 1557. As with interpretations of Title VII, courts have also interpreted Title IX independently as extending to sexual orientation discrimination on the theory of sex stereotyping. 44 If judicial decisions accord with this interpretation, sexual orientation discrimination would be unlawful in education settings under Title IX, and in health care settings under § 1557.
Where current federal law does not extend protection, state statutes and local ordinances (where permitted by state law) can fill the gap in protections against discrimination in health care settings. States have long regulated medical practice, and indeed “health laws of every description” are included in Chief Justice Marshall's archetypical description of state legislative authority in 1824. 45 At the time of this study, twenty-two states barred discrimination on the basis of sexual orientation in public accommodations, and all but three states allowed local nondiscrimination ordinances on this basis. 46 State definitions of public accommodations typically extend to hospitals and clinics, and may reach individual providers' offices as well. 47 Local ordinances in jurisdictions such as New York City provide similar protections, where these laws apply to public accommodations. 48 States can also address complaints of discriminatory behavior through medical licensing boards, which have authority to discipline providers for substandard care, actionable misconduct, and breaches of state regulations. 49
2. Soft Law
Soft law provides additional protections. The Joint Commission, which accredits U.S. hospitals, has since 2011 required that hospital policies prohibit discrimination on the basis of sexual orientation, gender identity, and gender expression. 50 The Joint Commission is the primary accrediting body for hospitals to participate in Medicare and Medicaid, which gives these requirements more bite. Professional self-regulation is another source of nondiscrimination rules: the American Medical Association has enacted several nondiscrimination policies to guide conduct by member physicians, 51 and professional associations such as the American Psychological Association have similar codes. 52 Hospitals, clinics, provider group practices, and individual providers may also establish and publicize their own nondiscrimination policies. As one example, the LGBT provider organization GLMA has established a directory of providers designated as “LGBT friendly,” 53 and physicians can create listings to signal their nondiscriminatory policies.
3. Exceptions and Non-Actionable Sources of Discriminatory Treatment
Notwithstanding these layers of nondiscrimination rules, individual and institutional providers may also claim exemptions, particularly when they withhold treatments for reasons unrelated to medical need. Federal conscience protections originated in protections for doctors with religious objections to providing abortions. 54 A separate protection extends to employers and insurers that raise moral or religious objections to birth control. 55 But conscience clauses underwent a massive expansion in May 2019, when HHS issued new regulations for institutions receiving federal funding. 56 These rules are designed to protect individual providers and staff with conscience objections, including certifying compliance with twenty-five conscience protection statutes as a condition of federal funding, maintaining records of any actions taken against providers who refuse to provide care to patients on conscience, moral, or religious grounds, cooperating with investigations, and posting notices to those who may wish to invoke conscience objections. 57 Objecting providers must not be required to “refer” patients to others who may provide the care that they have refused. 58 These conscience protections would be enforceable against programs that reassigned or refused to hire physicians or staff members who refused services to LGBT patients. 59 Dozens of states and municipalities sued to enjoin the regulations, and they have been vacated in multiple districts as arbitrary and capricious. 60
The HHS Office of Civil Rights 61 has also established a new Conscience and Religious Freedom Division to investigate federally funded health care institutions where there has been an allegation of discrimination against providers on the basis of conscience or religious objections to care. 62 Although these complaints had been rare in prior administrations (averaging one per year), the number skyrocketed to 343 in 2019. 63
State statutes have granted broader exemptions for the exercise of conscience refusals, 64 including a few states that specifically protect providers who refuse care on the basis of sexual orientation. 65 State RFRA equivalents may reach more broadly still, 66 along with challenges to state protections on the basis of the free exercise clause of the Constitution. 67 Consolidations and merger activities by Catholic hospitals that follow Ethical and Religious Directives for Catholic Health Care Services have also expanded the reach of hospitals that opt out of care on religious grounds. 68 A Request for Information by HHS sought comments on ways to lift regulatory requirements for faith-based providers and hospitals, which may lead to a broader scope for religion-based refusals. 69
Providers' refusals to provide particular treatments can also be difficult for patients to detect. A nationwide survey of physicians has estimated that approximately forty million patients receive care from physicians who do not feel obligated to disclose information about treatments they find morally objectionable, and 100 million patients receive care from physicians who do not believe they are obligated to refer patients to providers who are willing to provide such treatments. 70
An additional shortcoming of nondiscrimination rules is that they do not reach some sources of experienced discrimination, including implicit bias 71 and lack of cultural competency in care. 72 Discrimination may take many forms beyond refusal to treat or differential treatment, including disrespectful comments, abusive language, excessive precautions, blaming patients for their health status, rough examinations, comments on gender expression, lack of awareness of health needs, and allowing explicit or implicit biases to affect clinical judgments. 73 These sources of discrimination may not be legally actionable, even in jurisdictions that have nondiscrimination statutes.
B. Impacts of Nondiscrimination Rules for Providers
Despite the proliferation of nondiscrimination rules and exceptions in health care, little to no research has examined how these provisions affect the expectations and behavior of health care providers and patients. But analyses in other contexts have considered the effectiveness of legal rules for shaping the behavior of those who are in a position to discriminate, as well as effectiveness for securing greater representation of protected classes in domains of interest.
In the area of employment discrimination, for example, Laura Barron and Michelle Hebl conducted a set of studies that were responsive to ongoing debates about the Employment Non-Discrimination Act—an unsuccessful proposal to bar discrimination on the basis of sexual orientation in employment as a matter of federal law. 74 These studies found that randomly selected households were more likely to be aware of sexual orientation laws when they lived in communities with legislation, that gay and lesbian job applicants face less discrimination in fact in cities with nondiscrimination ordinances, and that manipulating nondiscrimination rules in a laboratory setting led to less discrimination in lab tasks. 75 Other studies have documented the efficacy of nondiscrimination rules in employment settings. 76 Findings suggest that some nondiscrimination rules may backfire; for example, a study of the Age Discrimination in Employment Act found that rules making claims easier to enforce may have discouraged companies from hiring older workers (for fear of being sued later). 77
C. Impacts for Members of the Protected Class
Comparatively less research has focused on how nondiscrimination law affects protected beneficiaries. A series of cross-sectional studies has considered state statutes barring sexual orientation discrimination in other domains—particularly employment discrimination—as indicators of state-level social support for LGB communities, along with other supportive laws such as same-sex marriage protections, protection against hate crimes, and laws on joint adoption for same-sex couples. 78 These studies have found that social support, as indicated by supportive laws, may improve mental health (including anxiety disorder and PTSD), decrease medical visits and expenditures (particularly mental health visits and costs), increase access to post-exposure prophylaxis medication, and increase comfort disclosing sexual behavior to providers. 79 Research on employment discrimination laws has suggested that supportive laws can reduce minority stress and encourage disclosure of sexual orientation, but these studies have said little on how protected individuals form their perceptions about law. 80 Soft law protections in workplaces may improve job satisfaction, although they were not related significantly to job stress; 81 one study also found that job seekers with strong heterosexist views are deterred from positions when they encounter gay-friendly statements during recruitment. 82 Time spent in social environments with unsupportive laws and policies can have an enduring effect on health and health risk behaviors, as indicated by an international survey of men migrating from countries with laws that allow or reinforce unequal treatment on the basis of sexual orientation. 83
Prior work has also examined the frequency with which intended beneficiaries of nondiscrimination protections file claims to enforce their rights. 84 One such study considered the experience of claiming under the Massachusetts Fair Labor Act, which was revised in 1989 to bar sexual orientation discrimination in hiring; a survey of employees who had filed claims ten years later found that many had success in claiming, but that the process of rights enforcement could be separately traumatic and stigmatizing. 85
Interestingly, most of this prior research has considered law as evidence of social support, casting an inclusive social environment as the independent variable driving other outcomes. These studies treat law as an indicator of social environment. Given this emphasis, few of these studies interrogated community perceptions and beliefs about state-law legal protections. 86 Prior studies linking law to attitudes and health behaviors have not examined nondiscrimination protections specific to health care settings. The present study sets an agenda for filling these gaps.
D. Pathways between Nondiscrimination Law and Patients ' Decisions
Nondiscrimination rules allocate an entitlement to be free of discriminatory treatment, and they extinguish discriminators' previous entitlement to treat people unequally. The processes by which nondiscrimination laws may influence choices made by protected people are incompletely theorized. I offer several such pathways here, drawing in part on expressive legal theory: the idea that people perceive laws as communicating information. 87 Prior work divides these signals into several categories, including signals about social norms, signals about the risks and benefits of behavior, signals about how others behave, and “expressive-politics” signals that shows which interest groups are valued by lawmakers (and which cultural values control). 88 Nondiscrimination laws can send all of these signals. Someone who observes a state law barring discrimination may draw the inference that it is against social norms to discriminate, that discrimination causes some kind of harm in the world, that many people discriminate, and that the protected group is a priority for the state. Someone observing a lack of state law protection may draw the opposite inferences.
A taxonomy of the effects of nondiscrimination law on patient behavior may be as follows:
1. Direct Effects
Nondiscrimination laws may communicate social norms and expressive-politics signals that are supportive of LGB populations, such as the message that society disapproves of sexual orientation discrimination, or the message that sexual minority populations are recognized and valued by the state. The latter message may be particularly valuable for individuals who identify as part of a community that has advocated for recognition and equality; for this group, laws are part of an arc of successful advocacy and progress. Messages that communicate inclusive social norms, as well as the fact of direct sanctions for discriminatory behavior, may reduce anticipated discrimination and internalized stigma. These dynamics may promote care-seeking and disclosure in care settings.
Signals about how others behave may be mixed. If people view a prohibition as evidence that many people are acting badly, this signal may increase anticipated discrimination. But for people who believe that health care providers will obey the new law, they may trust that the prohibition will be effective in future health care interactions.
For protected individuals who have the resources and a private right of action to enforce nondiscrimination law, these statutes can increase confidence that there will be a remedy for anticipated wrongs. This reduces the possible losses that may result from a discriminatory experience in care, and may thus encourage care-seeking and disclosure. Although many may not sue, some protected individuals affirmatively enforce their rights privately, 89 or they may seek enforcement or report violations to state or federal enforcement agencies.
Discrimination rules also supply vocabulary and a conceptual framework for recognizing and labeling treatment as illegitimate. Nondiscrimination laws provide a shared way to understand mistreatment as linked to sources of inequality, and they can encourage beneficiaries to identify and name the wrongs they experience. Alternatively, if people believe that others obey the law, protective laws may also prompt people who experience mistreatment to consider alternative explanations beyond discrimination. Prior studies suggest that where possible, people resist classifying others' choices as legally discriminatory, perhaps out of the belief that others are likely to be in compliance with the law. 90
2. Indirect Effects
Nondiscrimination protections may also affect patients' choices indirectly, through pathways such as changing providers' behavior. If patients have fewer discriminatory experiences with providers, they may anticipate less discrimination and lower mistrust in future encounters, which can reduce barriers to care-seeking. Nondiscrimination law might also signal to third parties that social norms disapprove of discrimination, that discrimination causes harm, and that LGB individuals are valued and respected by the state. All of these signals, if internalized by society generally, can encourage socially inclusive attitudes and alleviate discrimination in contexts outside health care.
3. Other Functions of Law
Another way to view law is as a marker for existing social conditions, in keeping with prior public health research using law as an indicator of social support for LGB populations. In this view, law provides evidence of existing norms, but this function is separate from law's consequences. The extent to which law reflects existing social norms depends on whether legislators mirror the preferences and priorities of the public; law may be a less reliable marker of social experiences in cities and neighborhoods with preferences that differ from state legislators.
Finally, a skeptical beneficiary may also view nondiscrimination rules as disingenuous marketing intended to attract paying business or to impress third parties who sympathize with nondiscrimination goals, or as a hollow, cosmetic gesture made without more substantial efforts to address socioeconomic marginalization. This may particularly affect soft law protections, which are enacted by service providers who also have profit motives. This message may prompt disillusionment or disengagement, and some may be offended if they perceive a mismatch between ostensible and actual commitments to nondiscrimination.
The present study does not prove (or falsify) any one of these hypotheses, but instead answers the baseline question of whether perceptions of nondiscrimination protections in health care are correlated with care-seeking attitudes and behaviors. If perceptions of the law are associated with outcomes such as medical mistrust, perceived barriers to care, and care-seeking, the pathways suggested above provide hypotheses that may explain the relationship.
II. A SURVEY OF LEGAL KNOWLEDGE, BELIEFS, AND CARE-SEEKING
This national survey investigated associations between perceived nondiscrimination protections and predictors of patient decision-making. The central findings of this survey show that perceptions of protection are associated with less medical mistrust and anticipated discrimination, greater care uptake, and lower barriers to disclosure. Approximately half of participants were mistaken in their beliefs about state law, and these mistakes tended to be optimistic: participants were more likely to mistakenly believe that they were protected, when in fact they were not, than vice versa. Part III will consider possible interpretations of these findings.
A. Method and Sample
This study used a national survey of men who use the smartphone application Grindr to meet male partners. As this survey was part of a larger project on willingness to use PrEP, an HIV prevention medication, the survey embedded a set of three randomized trials of strategies for informing HIV-negative men about PrEP; trial results are not reported here. The survey included n=3078 men, who are the focus of this analysis.
The study recruited respondents using nationwide banner advertisements on the Grindr application, which showed in the United States and Canada in August 2016. Men were eligible for the study if, according to screening questions, they were older than 18, able to read and understand English, male gender at birth, HIV-negative by self-report, and had sex in the past six months with a male partner. Canadians were excluded from all analyses of state law, as were men who did not report their state of residence. This narrowed the sample to n=1870 men. Participants who clicked on the banner ad were redirected to the survey instrument on Qualtrics. They completed an informed consent process online and then proceeded to the survey. All data collection was anonymous, but used Qualtrics controls to prevent ballot box stuffing (i.e., multiple surveys taken by the same person). Afterwards, men who were interested in being compensated for their survey were redirected to a separate survey, unlinkable to the first, where they entered their email address for a lottery drawing to receive a $100 Amazon gift card. Although the study design for evaluating the effectiveness of PrEP education messages was a randomized trial, all data on perceptions of state law were cross-sectional; this portion of the study did not use an experimental manipulation.
I also classified states as having or lacking state nondiscrimination protections on the basis of sexual orientation in employment, housing, and public accommodations (including health care settings). I focused on state law protections for several reasons. State law provides the strongest and most unambiguous protection against sexual orientation discrimination, and it provides a source of variation in a national sample that allows testing of associations between actual law, perceived law, and patient care-seeking. I used the classifications provided by the Movement Advancement Project (“MAP”) in August 2016. MAP keeps an up-to-date database of nondiscrimination statutes on the basis of sexual orientation and gender identity in employment, housing, and public accommodations. 91 I consulted statutory definitions of public accommodations to ensure that health care settings were included in all states with these laws. Because people may not understand public accommodations to include health care, I asked participants separately about public accommodations and health care settings.
Like any study, this sample and approach have limitations. Men who use Grindr differ from the general population of men who have male partners, and from the general population of men who would identify their sexual orientation as gay or bisexual. This was an HIV-negative population; people living with HIV may have health care experiences that differ from this group. The results reported here may not extend to discrimination on other bases, such as race, age, or gender. Fraudulent survey completions were possible, but given the anonymity protections in this survey, I was unable to track them; Grindr uses moderators to ban bots and spam profiles from the site. 92 But despite these limitations, this work can help to illuminate some of the pathways by which nondiscrimination law may shape the attitudes and choices of protected individuals.
1. Measures
In addition to the PrEP education messages, the survey also included a full set of demographic questions, items about health care utilization, disclosure to providers, HIV testing, stigma and experiences with discrimination in health care, discrimination in other settings, a validated measure of medical mistrust based on sexual orientation discrimination, and items on willingness and barriers to using PrEP. The items on nondiscrimination law perceptions included four separate questions: men were asked to select “Yes,” “No,” or “I don't know” in response to the following items:
Does your state have any laws that protect gay, lesbian, and bisexual (LGB) people from discrimination on the basis of sexual orientation? Please answer for each type of law: My state protects gay and lesbian people against discrimination in the workplace My state protects gay and lesbian people against discrimination in housing My state protects gay and lesbian people against discrimination in public accommodations My state protects gay and lesbian people against discrimination in hospitals and doctor's offices.
Medical mistrust was measured using a series of items from the Group-Based Medical Mistrust scale, which asked men to report agreement on a 1-5 scale (with 1 being “strongly agree” and 5 being “strongly disagree”) with items such as “Gay and bisexual men receive the same medical care from doctors and health care workers as everyone else” and “Doctors and health care workers sometimes hide information from gay and bisexual men” (reverse-scored). 93
All cross-sectional analyses in this section controlled for a set of demographic correlates, including age, race, income, education, health insurance, and Latino ethnicity. To isolate the effect of perceived law from social support, I controlled for the frequency of experiencing discrimination in daily life apart from health care settings. Correlates also included actual legal protections in the state.
2. Analysis
Stata 14 was used for analyses. I used a chi squared analysis to test the extent to which participants in the study were correct about the law (and if they made errors, how were those errors distributed). I then sought to identify correlates of the belief that one is protected by nondiscrimination law, and I conducted a logistic regression with demographic variables, actual state law, and the covariates of daily discrimination experiences and shame about sexual orientation. I used these two covariates throughout the analyses to try to exclude the possibility that perceived law reflects either a supportive social environment or internalized social stigma. By controlling for these variables, I hoped to better isolate associations with perceived and actual law. The other analyses sought to test whether perceived law and actual law are significantly associated with medical mistrust, care uptake, and perceived barriers to care.
3. Sample Characteristics
Among the 1,870 men in this study, 68% were younger than age forty; distribution by race was 66% White, 9% Black, 7% Asian, and the rest of other races. Twenty-four percent of men identified as Latino. Fifty-five percent had completed college. Approximately 13% were below the federal poverty line for an individual; another 39% made above this line, but less than $40,000 per year. Health insurance varied: 19% had no insurance, 54% had private insurance, 17% had insurance through public sources (generally equally distributed between Medicaid and Medicare, with some TRICARE and VA), and 10% had insurance through other sources. Sixty percent reported having a primary care provider, and 47% of this subgroup had disclosed to that provider that they have sex with male partners. Approximately 17% of men reported having experienced discrimination in a hospital or doctor's office on the basis of their sexual orientation. In general settings of daily life, 14% reported feeling discriminated against “often” or “all the time” on the basis of sexual orientation.
B. Results
1. Optimistic Errors about State Laws
As noted above, n=1870 men in this study reported their U.S. state of residence; All states and the District of Columbia were represented in the data; the most populous states were California (10.8%), New York (9.3%), Texas (9%), and Florida (8.6%). A robust and consistent finding across all types of law was that perceptions of the law sharply diverged from reality. Accuracy was highest for nondiscrimination protections at work, with 54.7% of men correct about the law; accuracy was only 48.3% for discrimination in housing, 47.8% for discrimination in public accommodations, and 44.7% for discrimination in health care.
When participants were incorrect about the law, they systematically erred on the side of believing that legal protections existed, when in fact they did not. As shown by the four charts in Figure 1, almost all errors were in the direction of erroneously believing that a legal rule existed. This was significant across all types of law, with chi squared analyses significant at p < 0.001. 94
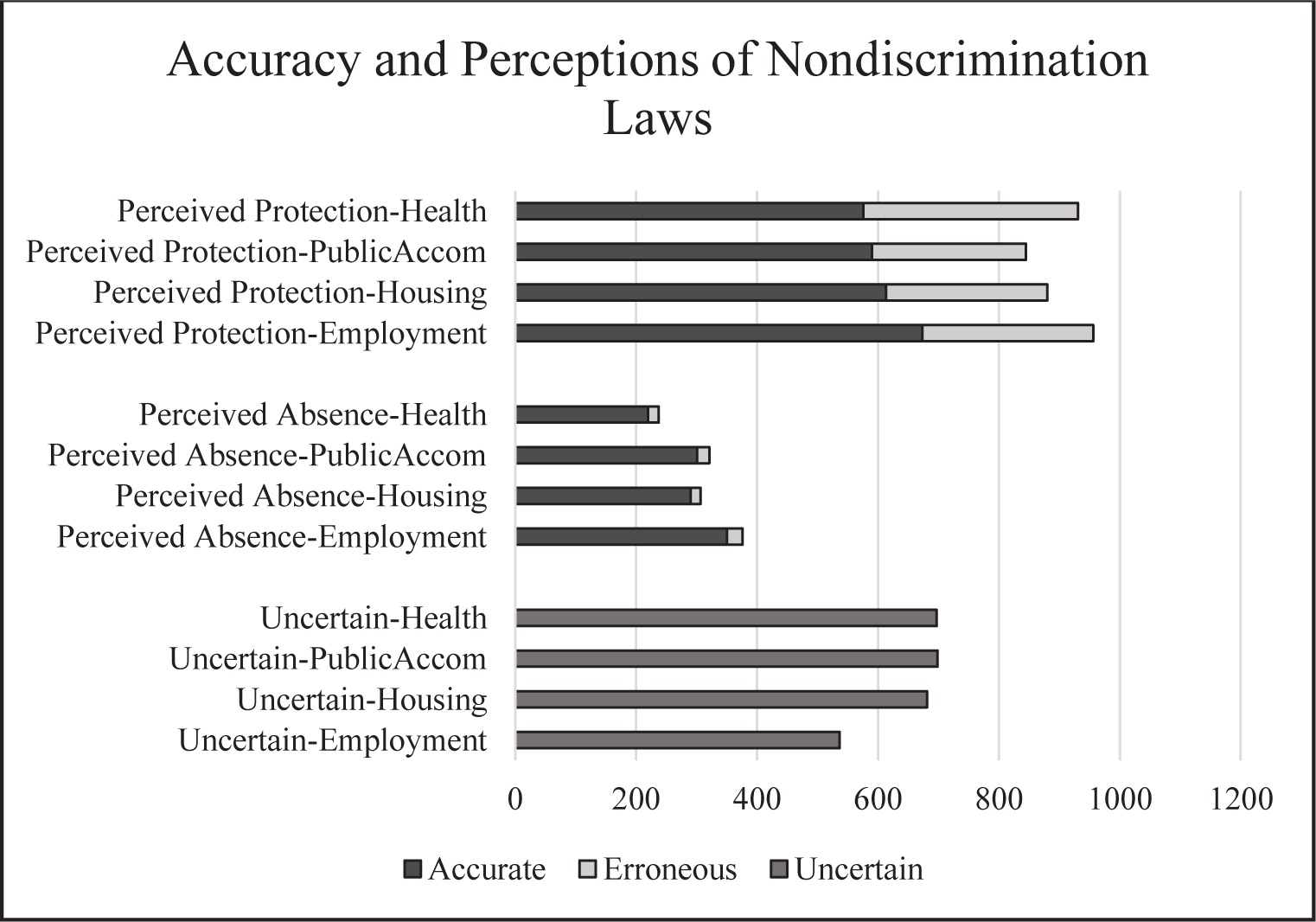
Systematic Errors about the Presence of Nondiscrimination Laws
Uncertainty was also more likely when laws were absent. This may be due to migration, if people consciously move to states where there are greater protections on the basis of sexual orientation, either because of the laws themselves, because of the more progressive social environment that supported the passage of such laws, or both. 95 These results also align with prior findings that people tend to believe that the applicable law embodies their normative aspirations. 96 In tandem with the theory that people reasonably believe that law fits their normative priors, I also suggest that negative beliefs about the law can reflect internalized stigma—the extent to which people may tacitly adopt negative beliefs about themselves based on community attitudes.
Another possible explanation for optimistic errors is that men deduce the law from their experiences in the world. Scholarship focusing on gay and bisexual men has documented concentrated populations in urban areas, and theories of “syndemic” risks among urban gay men have considered urban migration as a reaction to social marginalization in more conservative rural areas. 97 Men who live in comparatively progressive urban areas of conservative states may experience less discrimination, which could inform the expectation of nondiscriminatory treatment, and the belief that it must be unlawful to discriminate. The overall political makeup of state legislatures, however, may be more conservative than the population of areas where gay and bisexual men choose to live.
These findings may also have skewed toward optimistic errors because of confusion between federal, state, and municipal law, and the timing of this survey some months after the initial § 1557 regulations were released in 2016. In the closing months of the Obama administration, HHS had issued regulations suggesting that they would read § 1557 to prohibit sex stereotyping and to protect against discrimination on the basis of sexual orientation. 98 Individuals who knew about these new protections may well have answered affirmatively to the question of whether their state has nondiscrimination laws, because federal law would apply simultaneously. Many municipalities have their own nondiscrimination ordinances, and it is easy to confuse city for state law as well. To ensure anonymity, I did not query participants about zip code or city of residence, but this would have been useful in disaggregating state and city provisions.
Notably, errors in the direction of perceived sexual orientation protections are not limited to the protected group; the general population makes the same mistakes with respect to LGB rights. In a national poll in 2019, 45% of Americans reported believing that federal law protects lesbian, gay, and bisexual people against discrimination, when no such statute exists; only 23% believed that federal law lacked these protections. 99
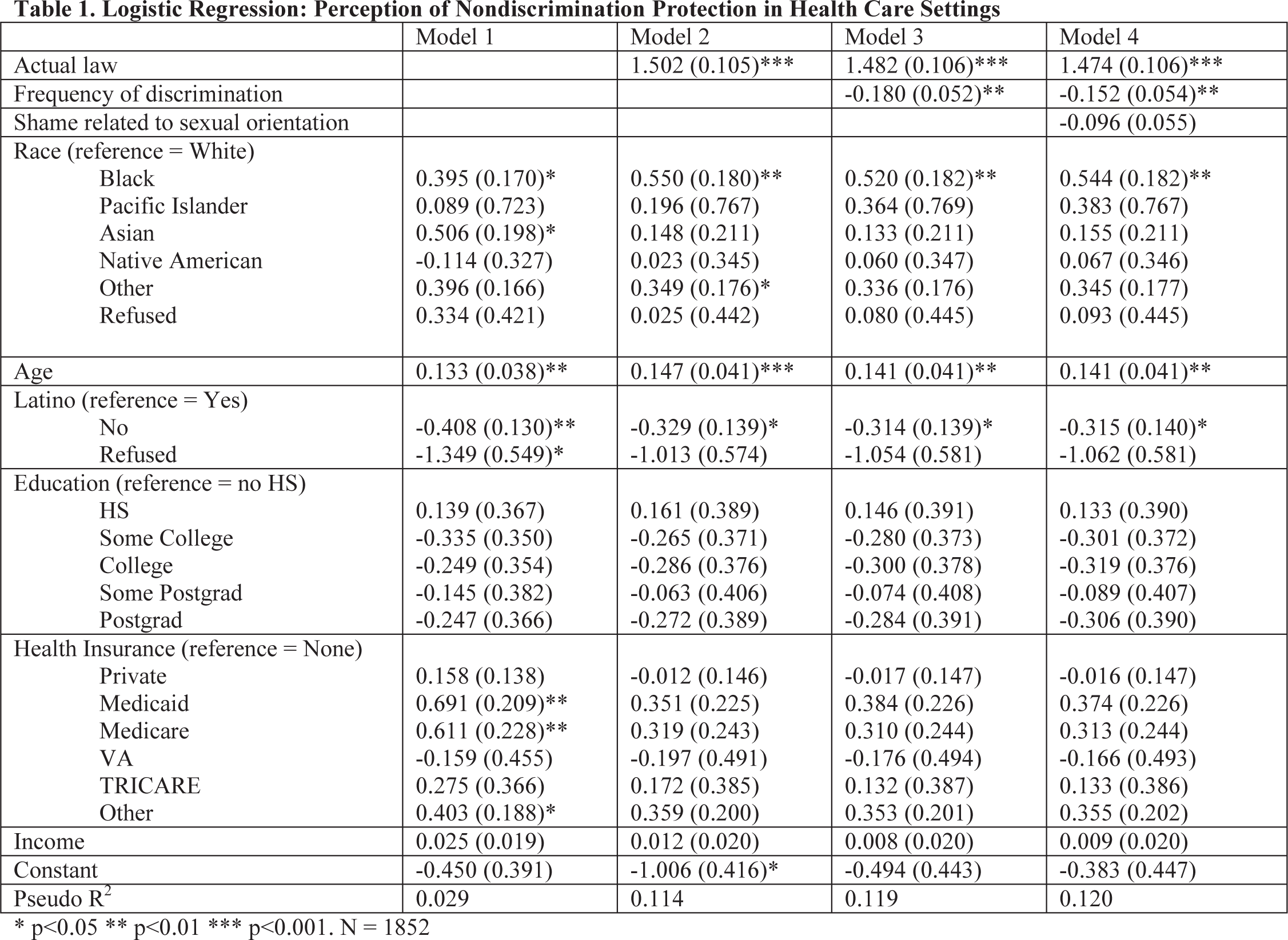
Although cross-sectional methods cannot test how people develop their beliefs about law, an exploratory analysis may help; I note that these are post hoc tests and should be considered hypothesis-generating rather than hypothesis-testing. To identify demographic predictors of perceiving a protective state law, I ran a logistic regression, where the outcome was whether participants believed that they were protected by law. I began with demographic predictors alone (Table 1), finding that race and age were related to the perception of being protected. I then added three more independent variables: actual state law, frequency of experiencing discrimination in everyday life, and internalized shame about sexual orientation. I included actual state law to account for people who in fact know the law. I included daily discrimination to test the possibility that men deduce law from daily experiences; I reasoned that if this is true, more frequent experiences of discrimination should be associated with a reduced belief in legal protection. I included shame about sexual orientation to test whether internalized stigma can influence perceptions of law: if people agree with negative attitudes about LGB populations, they may find nondiscrimination laws less of an aspirational priority, and may be less likely to think that LGB populations are protected.
Logistic Regression: Perception of Nondiscrimination Protection in Health Care Settings
p<0.05
p<0.01
p<0.001.
N = 1852
These regressions suggest that beliefs that one is protected are correlated with actual law (i.e., many people may know the law), but that the perception of protection is also strongly correlated with actual experiences of discrimination. That is, participants who experienced more discrimination were less likely to believe that there was a law protecting them. Shame was also correlated with beliefs about the law, but statistical significance was marginal (p=0.083); men who experienced more shame associated with sexual orientation were less likely to believe that there were laws protecting them.
2. Associations between Perceived Law, Actual Law, and Medical Mistrust
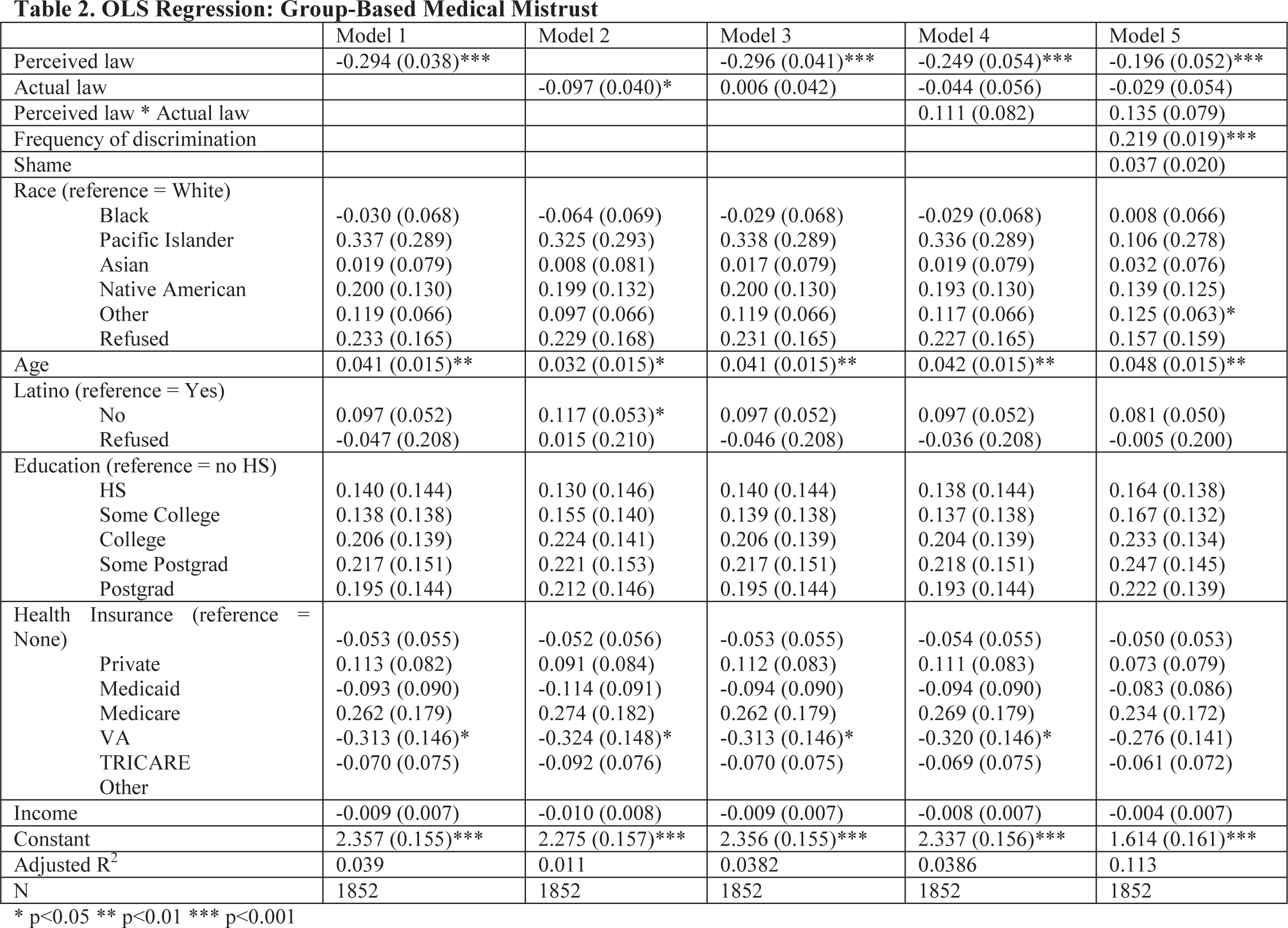
Having identified factors that may give rise to the perception of protection, I sought to understand whether beliefs about the law are associated with medical mistrust. Nondiscrimination laws may encourage patient care-seeking and disclosure if they reduce medical mistrust linked to protected characteristics. The cross-sectional design used here cannot determine the direction of causation: perceptions of the law could affect mistrust, or mistrust could affect beliefs about whether the law is protective. But this study design can show the direction and strength of associations between perceived law, actual law, and medical mistrust. Table 2 shows these regression analyses, using OLS regression with medical mistrust as an outcome, and perceived and actual law as independent variables. I first modeled each separately, then both, then both with an interaction term, and then I added covariates for frequency of daily discrimination and shame. I included the frequency of daily discrimination as an effort to disaggregate law from ambient social support; I included shame as an effort to disaggregate perceived law from internalized negative beliefs about sexual orientation.
OLS Regression: Group-Based Medical Mistrust
p<0.05
p<0.01
p<0.001
Perceptions of the law and actual law were each associated with lower levels of medical mistrust. But when both variables were included in the model, only perceived law remained significantly associated with mistrust; this significant relationship remained even after controlling for all demographic variables, frequency of daily discrimination, and shame.
To clarify the association between mistrust and perceived law, I used an ANOVA to compare mean medical mistrust scores for three groups: men who believed they were protected by the law, men who were uncertain about the law, and men who believed that their state permitted sexual orientation discrimination in health care. The overall association of mistrust with beliefs about the law was significant (F(2, 1862)=43.67, p=0.001). Mean levels of medical mistrust were significantly different in each pairwise comparison, in the expected direction: men who believed they were protected reported least mistrust (mean=2.413), men who were uncertain were in a significantly different middle range (mean=2.620), and men who believed they were unprotected reported significantly more mistrust than either of the other groups (mean=2.940).
One interpretation of these results is that expectations of legal protection foster greater trust in health care providers. The fact that actual laws were not associated with discrimination or mistrust suggests that the laws may have little effect on practice, or at least on care relationships as perceived by patients. It is possible that perceived law simply reflects men's views of social support, which predicts mistrust. But the fact that these associations hold even while controlling for daily discrimination and shame suggests that views about the law are independent of its function as a marker of social support. That is, if perceived law simply reflected perceived social support, then controlling for men's experiences of discrimination in daily life would likely eliminate perceived law as a significant predictor of discrimination and mistrust in care settings.
3. Associations between Perceived Law, Actual Law, and Care
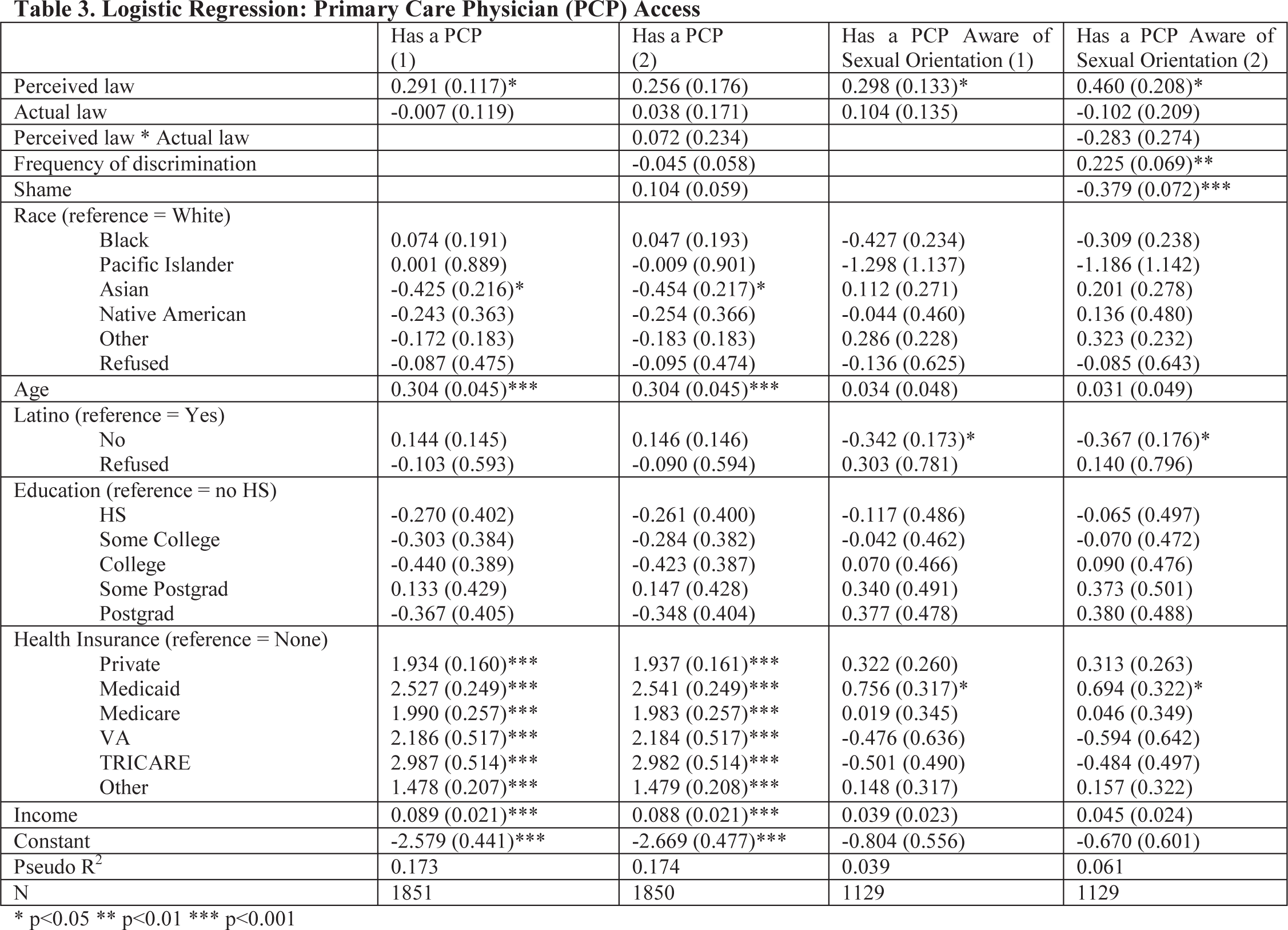
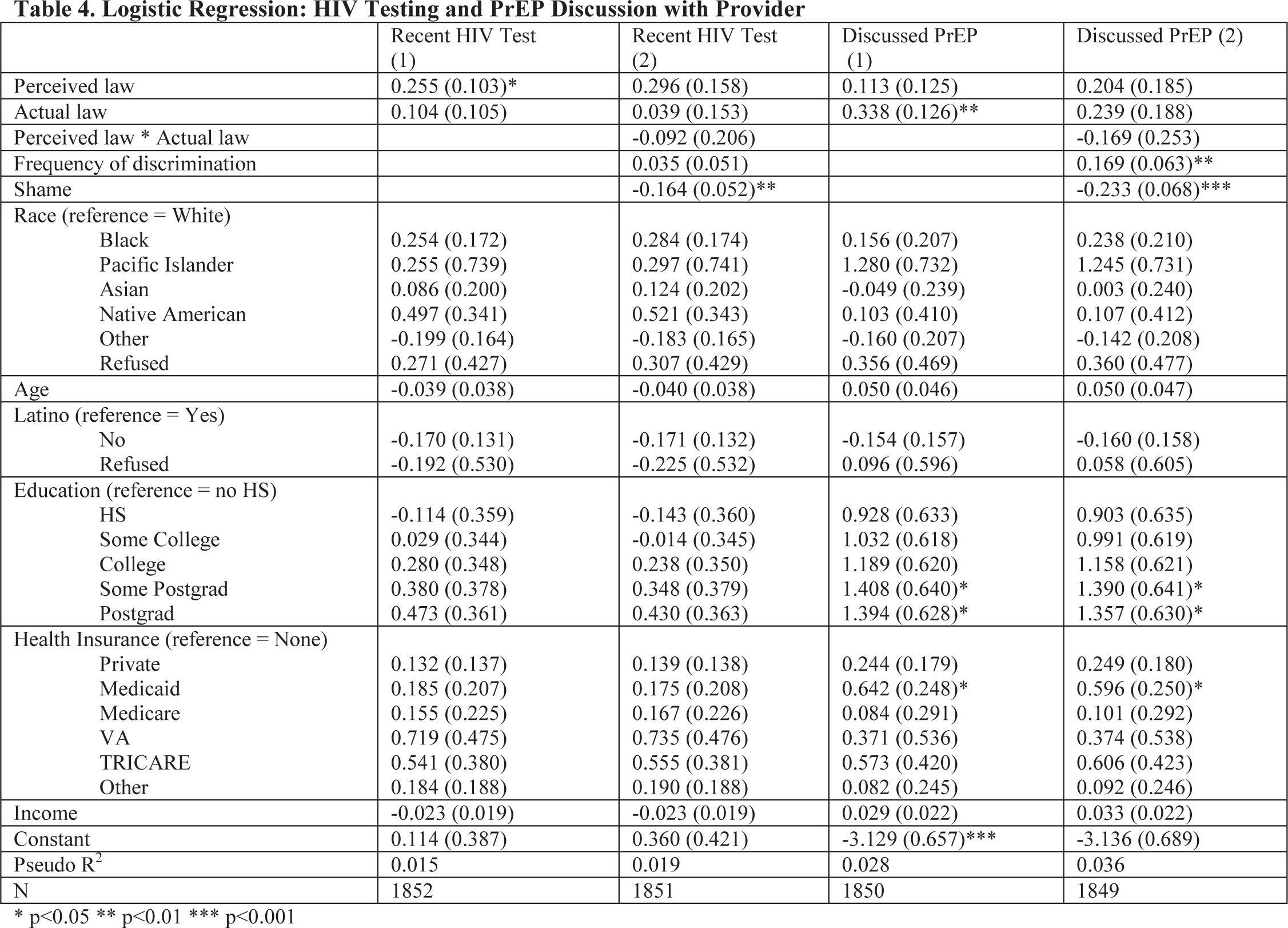
I tested the relationships between perceived law, actual law, and several outcomes related to care uptake. These included having a primary care provider, having a primary care provider to whom the participant has disclosed his sexual orientation or behavior, having had an HIV test in the past six months (which is the CDC-recommended frequency for many sexually active gay and bisexual men, who are at elevated risk of infection 100 ), and having spoken with a provider about the HIV prevention medication PrEP (which typically entails the disclosure of sexual orientation). Table 4 reports these results; for each outcome, I report a model with perceived law and actual law, followed by a model with an interaction term and the covariates of daily discrimination and shame.
Logistic Regression: Primary Care Physician (PCP) Access
p<0.05
p<0.01
p<0.001
Logistic Regression: HIV Testing and PrEP Discussion with Provider
p<0.05
p<0.01
p<0.001
The perceived presence of a nondiscrimination law was positively correlated with having a primary care provider, having a primary care provider who was aware of the patient's sexual orientation, and having had a recent HIV test. Actual nondiscrimination law was not significantly associated with any of these three outcomes. But this pattern reversed for the outcome of whether participants had discussed PrEP with a health care provider; this outcome was positively correlated with the presence of an actual law in the state, but was not correlated with perceptions of the law.
Notably, shame was highly negatively correlated with all care closely associated with sexual behavior disclosure, including having a primary care provider aware of sexual orientation, having had an HIV test, and having discussed PrEP with a provider. Surprisingly, increases in self-reported daily discrimination were positively associated with several of these outcomes, including having disclosed sexual orientation to a primary care provider and having discussed PrEP. This may be because individuals who are more public about their sexual orientation are more likely to disclose, including making disclosures in health care settings, but disclosing sexual orientation also makes these individuals more likely to experience discrimination.
In two analyses not shown here, I sought to understand how perceived and actual law might be related to perceived ease of getting care. I used the same regression models as above, and the dependent variables were a set of perceived barriers to accessing PrEP. Using the simpler model with demographic covariates, perceived law, and actual law, I found that perceived nondiscrimination law was significantly associated with predicting more ease finding a doctor, disclosing sexual orientation to a doctor, and keeping appointments (all p< 0.05). Perceived law had no significant association with predicted ease of obtaining a prescription. Actual law was significantly, positively associated with perceived ease in finding a doctor and disclosing sexual orientation to a doctor (both p < 0.05). In the full model with the interaction between perceived and actual law, as well as daily discrimination and shame, actual law was positively associated with ease of finding a doctor and ease of obtaining a prescription (all p < 0.05); perceived law had no significant associations.
C. Summary
Overall, this survey shows that beliefs about state nondiscrimination laws are associated with a range of attitudes and behaviors with relevance to patient care. The perception of protection was correlated with reduced medical mistrust, greater likelihood of having a primary care provider and self-disclosing to that person, and having had a recent HIV test. Actual protective laws were correlated with some outcomes of interest, including having discussed PrEP with a health care provider. But for medical mistrust, the perception of protection was a more important predictor. Law may have indirect effects on patient choices, such as by deterring discrimination and thereby improving care relationships over time, but the perception of law may also have a more direct relationship with medical mistrust, care-seeking, and ease of communicating information to care providers. But notably, perceptions of the law were often mistaken—and mistaken in a systematically optimistic way. Law matters, but the idea of law may be powerful even when it is erroneous. Finally, actual law and perceptions of the law each yielded findings that persisted despite controlling for experiences of daily discrimination and internalized stigma. These findings suggest that law and beliefs about the law may have independent associations with care-seeking, rather than simply reflecting a supportive (or unsupportive) social environment.
Again, this study has a number of limitations with respect to generalizability; the population of HIV-negative men who use Grindr is a specific subgroup of men who have male partners, and results may be limited to this group. But this is also a population of men with particular health care needs, such as more regular HIV testing and access to HIV prevention medication. It is useful to understand that perceptions of nondiscrimination law were associated with variables that matter for patient care-seeking, and this can generate ideas for testing in other samples. The focus on HIV in these analyses is a product of the broader research project, and of course gay and bisexual men have many other health care needs of equal or greater priority. This complex picture should not be reduced to HIV prevention alone. But HIV prevention was the focus of the large research project, and receipt of testing and discussion of PrEP are both CDC priorities for this population.
Finally, I note that the R-squared values were low for many of these regressions. But the goal of these analyses was not to provide a perfect predictive model for medical mistrust, having a primary care provider, or receiving a recent HIV test. Rather, the goal was to illuminate significant relationships between law, perceptions of law, and variables that matter for care-seeking. The strength of these associations would have the same interpretation regardless of R-squared; the findings of this study do not depend on whether the regression models are precise predictors of the outcomes.
III. EXPLAINING ASSOCIATIONS BETWEEN LAW AND PATIENT CARE-SEEKING
Part II reported several central findings, which admittedly allow for competing interpretations. First, perceptions of nondiscrimination protections were often wrong, but these errors were almost entirely attributable to people who erroneously believed that they were protected, when in fact they were not. Second, perceived laws were generally more important predictors of care-seeking attitudes and behaviors, such as medical mistrust, past discrimination in care, having a primary care provider, and perceived barriers to seeking and using a preventive care option like PrEP for HIV prevention. Third, actual law was more indicative of whether participants had in fact spoken with a health care provider about an HIV prevention option, but actual law was generally not associated with perceptions of discrimination and medical mistrust beliefs.
The results in this study are consistent with several legal theories, with different implications for nondiscrimination rules. The design of this study does not permit causal inferences linking actual laws, perceptions of the law, and care-seeking attitudes and behaviors. But the associations observed here are consistent with several causal explanations that are useful in framing ongoing work. This Part will consider three explanations that need not be mutually exclusive: (1) laws exert expressive effects, such that perceptions of the law (whether erroneous or accurate) encode information that shapes expectations; (2) people deduce law from their general experiences; (3) people reason about law in motivated ways that reflect their prior commitments; and (4) laws in fact deter discrimination, and people deduce laws from their specific experiences in the setting of interest.
A. Law as Information
The results of this study are consistent with a number of the expressive pathways suggested in Part I. First, participants who believe that they are protected by a discrimination law may infer positive information about the breadth and depth of social support for sexual minority populations among the general community that votes for state legislators. Perceptions of social support are protective for mental and physical health, and reduced barriers to care-seeking may be one benefit of this pathway—people who believe they are socially supported may devote more attention to self-care, and they may perceive lower barriers (including less fear of discrimination) in seeking care and disclosing in care settings.
This is separate, conceptually, from the theory that people deduce the law based on their perceptions of social support. Both explanations may be simultaneously true; people may experience a supportive community, deduce that they are protected from discrimination by law, and then have their belief in social support strengthened or reinforced by their perception of legal protection. There was a correlation between perceived law and reduced perceptions of discrimination in health care settings, as well as reduced perceptions of discrimination in daily life. Correlation cannot show causation in a setting with this design, but the effects are consistent with the idea that laws can communicate social support to their beneficiaries.
This study tends to contradict the possibility that expressive messages are bad news—they do not alienate potential beneficiaries of nondiscrimination laws, such as by communicating that many people discriminate, or by offending people who view such rules as hollow marketing efforts. If these explanations were accurate, this study may have shown greater mistrust among people who believed that there is a nondiscrimination law in place; this was absent.
B. Law as Indicator
The findings of these studies also support causal arrows in the reverse direction: instead of gleaning information from the presence or absence of law (despite the accuracy of those beliefs), people may form beliefs about the law based on the way they experience daily life. Specifically, people may interpret their daily experiences as evidence of what is legally or socially supported in their society, and they assume that these values are already encoded in the law.
Longitudinal methods and qualitative work are needed to understand how people develop their beliefs about nondiscrimination law. One possibility is that people deduce the law based on their social experiences generally. This might be suggested by the quantitative finding that people who believed that they were protected from discrimination reported fewer experiences of discrimination in their daily lives, as well as less shame related to sexual orientation. These participants may have viewed the people around them as representative of the democratic majority in the state legislature, and reasoned further that those nondiscriminatory views would have taken effect in law.
This pathway between perceived law and social experience may also underpin the disparities between perceived law and actual law in states lacking nondiscrimination protections. Daily experiences in progressive areas within conservative states may be comparatively less indicative of state discrimination law. But perceptions of social norms may not generalize to the democratic majority in state legislatures of such states, which would be necessary to secure the legal protections of interest here. Because the questions in this study asked about state statutory protections, rather than local ordinances or “soft” protections arising from social norms, men who deduced state-level laws based on their local experiences made predictable errors in the optimistic direction of erroneously believing they were protected. And as noted above, it is also possible that participants confused federal and state law and were reflecting the protections extended (and now withdrawn) under § 1557 of the ACA.
C. Law as Aspiration
A recent analysis of ten types of state laws suggests that although people tend to be correct about the law, they tend even more strongly to believe that the law is what they would optimistically prefer it to be. 101 This “phantom representation” of normative beliefs in the law is far more likely than “phantom misrepresentation”—the belief that one's normative priors are rejected by actual law. 102 This phenomenon may be evidence of motivated reasoning: 103 “motivation may cause people to make self-serving attributions and permit them to believe what they want to believe because they want to believe it,” and because they rely on “a biased set of cognitive processes.” 104
Throughout all four categories of nondiscrimination law, participants were far more likely to err on the side of believing that they were protected. I assumed that this aligns with their normative priors; that is, men in this group likely wish to be protected against discrimination. But it is separately useful to note that a higher frequency of shame—which suggests internalized stigma, including the genuine belief that one is undeserving of protection—predicted the belief that one is not protected by law. This study was a preliminary effort, and it does not disaggregate motivated reasoning, legal consciousness, or expressive impacts of law. Future work will make more headway in this direction. But the findings of this study are indeed consistent with motivated reasoning.
One normative question arising from this work is whether it is ethical or normatively desirable to correct misperceptions about nondiscrimination law. Many of the men in this study erroneously believed that they were protected; separately, the perception of protection was associated with greater care-seeking behaviors and attitudes. It would not be ethical to deceive people about the existence of legal protections, even if those beliefs were somehow health-promoting. But where nondiscrimination laws exist, publicizing these protections may be essential for realizing their full value; enactment alone is not enough. Where protective laws do not exist, enacting and publicizing soft law protections may fill the gap.
But where neither enforceable nor soft laws are present, inducing beliefs in a protective law is fraught. Misrepresenting the law violates autonomy and is unethical. Inducing a false perception of protection may impose risk, such as encouraging people to disclose sexual orientation in a care setting that could then result in discrimination (which is separately harmful and may have long-lasting detriments on health and care-seeking). At a societal level, inducing more disclosures in care settings may lead to a greater frequency of disclosures; ultimately, this may cause providers to reevaluate discriminatory beliefs, and it would likely challenge discriminatory providers' negative perceptions of sexual minority communities. But encouraging individuals to take those risks is unethical. At a societal level, the false belief that protective laws already exist may undermine political mobilization to get such laws on the books, either at a state or local level.
D. Law as Incentive
The findings in this study also invoke a fourth potential pathway; nondiscrimination laws may work to deter actual discrimination, which then could have downstream consequences for beneficiaries' choices. Men who live in states with nondiscrimination laws may experience less discrimination in daily life, and men in states with nondiscrimination laws for specific settings may experience less discrimination in those settings. These comparatively better experiences, over time, may alleviate mistrust and encourage more care-seeking and disclosure, creating a virtuous cycle of improved care relationships.
This study was mixed on these points. Throughout the study, actual laws were sometimes useful predictors of experience, such as speaking with a provider about PrEP. Furthermore, actual laws and perceived laws were correlated when actual laws were on the books. But more frequently, actual laws were not independent predictors of care-seeking attitudes and behaviors when perceived laws were included in the regression. One possible explanation for these findings is that law is more likely to be a reflection of existing social practice, rather than directly incentivizing news types of (nondiscriminatory) practice. In areas where there is a law protecting against discrimination on the basis of sexual orientation in health care, the culture of medical practice may be more attuned to the health care needs of this population, thereby increasing the salience of information about HIV prevention strategies such as PrEP for men who have sex with men. Further work is needed to disaggregate these explanations.
CONCLUSIONS
Legislatures, administrators, and practitioners considering the adoption (or retraction, as in the recent HHS regulations) of a nondiscrimination rule typically consider the direct incentive effects of such rules: the effects on the frequency and magnitude of discriminatory behavior. Regulators may also consider the expressive effects of nondiscrimination rules—the message that they will send to would-be discriminators and the public, including people who are the intended beneficiaries of nondiscrimination protections. But little research to date has focused on the ways in which beneficiaries deduce the fact of discrimination, identify legal protections (or the lack thereof), adjust their expectations in light of perceived rules, and ultimately make decisions about entry into domains where they may experience discrimination.
This study contributes several insights to the understanding of how nondiscrimination rules may affect the behaviors of beneficiaries, apart from their impacts on discriminatory behavior. I used sexual orientation discrimination as a case study, for which affirmative disclosure is a matter of both patient discretion (in disclosing) and provider discretion (in asking). This study also used willingness and ability to seek PrEP as an example of care with heightened disclosure burdens, given that people who seek to use PrEP must meet clinical indications, and those indications are easier to meet if people are willing to disclose that they engage in same-sex sexual behavior. For PrEP, willingness and ability to disclose same-sex sex (despite possible discrimination) is an important dividing line for prescribing purposes, and disclosure is a heightened access barrier for individuals who do not disclose, regardless of their reason for not doing so. Where discrimination leads to nondisclosure, it is a de facto bar to accessing this potentially life-saving care.
My findings from a nationwide survey of men seeking male partners were consistent with these explanations, and these results supported additional theoretical linkages between nondiscrimination rules and patient care-seeking behavior. Namely, perceptions of nondiscrimination rules may shape beneficiaries' interpretation of care experiences as discriminatory or not, and people who believe that they are protected are less likely to report experiencing discrimination in care. Alternatively, people may reason deductively about the law from their experiences, and that people who experience less discrimination in their daily life (as well as in health care specifically) are more likely to believe that the law entitles them to equal treatment in care settings. They do not, however, seem to interpret the perceived presence of a nondiscrimination rule as bad news about animus, nor do people seem to increase vigilance to detect discriminatory behavior.
To round out this set of potential explanations, my survey results also suggest the idea that people who wish to be protected from discrimination may infer that the law already realizes these aspirations. Each of these previous pathways—deducing the law from experiences, or from normative priors—is fully operational even if law has no effect on practice, perception, or behavior. But as a final explanation, if the law operates as a direct incentive to deter discriminatory behavior, protected beneficiaries may experience less unfair treatment and may build up expectations of equal treatment that encourage their engagement in the protected domain. The findings of this study are also consistent with this explanation, and further work is needed to disaggregate the moving pieces of this pathway.
Nondiscrimination laws in health care settings are incomplete and in some ways newly weakened, particularly for deterring discrimination on the basis of sexual orientation. This class is not yet fully protected under federal law, which provides an opportunity to identify how attitudes and practices may change according to state law, local law, and soft law protections. Prior scholarship tends to show that discriminatory experiences can cultivate medical mistrust and deter care-seeking on the patient side, but that nondiscrimination laws seek to (and may in fact) deter discriminatory behavior on the provider side. 105 This Article has both theorized and investigated several means of connecting these two domains: if patients are deterred by experiences with discrimination, do nondiscrimination laws “on the books” and/or “in the mind” encourage beneficial attitudes and engagement in the protected domain? How do actual and perceived legal rules exert these effects? And when people hold beliefs about their entitlement to nondiscriminatory treatment, what gives rise to these perceptions? This Article raises a raft of possible answers to these questions.
Nondiscrimination rules alone cannot solve the problems of discrimination in health care, and even if they could, they do not reach the structural societal issues that underlie many health disparities. Many scholars have highlighted the deficiencies of nondiscrimination rules. But as such laws progress in health care and elsewhere, studying how these rules may shape beneficial attitudes and behaviors by beneficiaries can offer a separate rationale for supporting nondiscrimination laws, even if they insufficiently deter discriminatory behavior.
Footnotes
1
See Nondiscrimination in Health and Health Education Programs or Activities, 84 Fed. Reg. 27,846 (proposed June 14, 2019). This was an about-face from HHS's 2016 final rules, which interpreted a provision of the Affordable Care Act—§ 1557, a wide-ranging nondiscrimination law—to protect people who experienced discrimination in health care due to gender identity, sex stereotyping, and limited English proficiency. Nondiscrimination in Health Programs and Activities, 81 Fed. Reg. 31,376 (May 18, 2016) (codified at 45 C.F.R. pt. 92).
2
Protecting Statutory Conscience Rights in Health Care, Delegations of Authority, 84 Fed. Reg. 23,170 (May 21, 2019) (codified in 45 C.F.R. pt. 88).
3
Zarda v. Altitude Express, 883 F.3d 100 (2d Cir. 2017), cert. granted, 203 L. Ed. 2d 754 (U.S. Apr. 22, 2019) (No. 17-1623).
4
5
6
Ryan Thoreson, “You Don't Want Second Best”: Anti-LGBT Discrimination in US Health Care, H![]() .
.
7
See infra Part II.B.
8
See generally R
9
See, e.g., Elizabeth S. Anderson & Richard L. Pildes, Expressive Theories of Law: A General Restatement, 148 U. P
10
See Thoreson, supra note 6.
11
Kristen Underhill, Raising the Stakes for Nondiscrimination Protections in the ACA, 48 H
12
Kristen Underhill et al., A Qualitative Study of Medical Mistrust, Perceived Discrimination, and Risk Behavior Disclosure to Clinicians by U.S. Male Sex Workers and Other Men Who Have Sex with Men: Implications for Biomedical HIV Prevention, 92 J. U
13
For instance, there is some evidence that gay and bisexual men choose live in progressive urban areas within more conservative states—where their daily experiences may be supportive, but the state legislation is not. See, e.g., James E. Egan et al., Migration, Neighborhoods, and Networks: Approaches to Understanding How Urban Environmental Conditions Affect Syndemic Adverse Health Outcomes Among Gay, Bisexual and Other Men Who Have Sex with Men, 15 AIDS & B
14
See, e.g., Arden Rowell, Legal Knowledge, Belief, and Aspiration, 51 A
15
See, e.g., Sarit A. Golub & Kristi E. Gamarel, The Impact of Anticipated HIV Stigma on Delays in HIV Testing Behaviors: Finding rom a Community-Based Sample of Men Who Have Sex with Men and Transgender Women in New York City, 27 AIDS P
16
For an elegant description of stigma across six stigmatized statuses and seven domains of social participation, see Mark L. Hatzenbuehler et al., Stigma as a Fundamental Cause of Population Health Inequalities, 103 A
18
19
See Jennifer Kates et al., Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the U.S., K![]() ; James A. Swartz, The Relative Odds of Lifetime Health Conditions and Infectious Diseases Among Men Who Have Sex with Men Compared with a Matched General Population Sample, 9 A
; James A. Swartz, The Relative Odds of Lifetime Health Conditions and Infectious Diseases Among Men Who Have Sex with Men Compared with a Matched General Population Sample, 9 A
20
See Lois Shepherd, HIV, the ADA, and the Duty to Treat, 37 H
21
See discussion infra Parts I.A.1, I.A.3.
22
Title II of the Civil Rights Act of 1964 notably does not include hospitals or physicians' practices, making Title VI the principal source of federal protections in the health care context. 42 U.S.C. § 2000a (2018).
23
42 U.S.C. § 18116 (2018).
24
This imports a restriction previously in place under Title VI of the Civil Rights Act; HHS applied these protections to hospitals receiving Medicare Part A, but not to individual physicians participating in Part B. Although most physicians receive multiple sources of federal funding (and will thus be subject to the ACA nondiscrimination rules), some have argued that the exclusion of Medicare Part B-only physicians is contrary to § 1557 language including “contrac[s] of insurance” as qualifying federal funds. See Sandra H. Johnson, The ACA's Provision on Nondiscrimination Takes Shape, 46 H
25
Nondiscrimination in Health Programs and Activities, 81 Fed. Reg. 31,376, 31,440 (May 18, 2016) (to be codified at 45 C.F.R. pt. 92). This would be a change to permissible claims under the Title VI of the Civil Rights Act, for which private rights of action are unavailable for disparate impact claims. See Alexander v. Sandoval, 532 U.S. 275, 293 (2001). HHS reasoned in the regulations that the Age Discrimination Act authorizes a private right of action for disparate impact, and that Congress's intent in the ACA §1557 was to treat all the underlying nondiscrimination laws equally. Rather than withdrawing protections under the Age Act, HHS's implementing regulations extended a private right of action to claimants bringing disparate impact claims on any of the protected characteristics.
26
45 C.F.R. §§ 92.101, 92.4 (2019).
27
Nondiscrimination in Health Programs and Activities, 81 Fed. Reg. at 31,389-90.
28
Franciscan All., Inc. v. Burwell, 227 F. Supp. 3d 660, 670 (N.D. Tex. 2016).
29
Julie Hirschfeld Davis & Helene Cooper, Trump Surprises Military with Transgender Ban, N.Y. T![]() .
.
30
Alan Feuer, Justice Department Claims Gay Workers Aren't Protected by Major Civil Rights Law, N.Y. T
31
Moral Exemptions and Accommodations for Coverage of Certain Preventive Services under the Affordable Care Act, 82 Fed Reg. 47,838 (Oct 13, 2017) (to be codified at 26 C.F.R. pt. 2590).
32
Nondiscrimination in Health and Health Education Programs or Activities, 84 Fed. Reg. 27,846 (June 14, 2019) (to be codified at 45 C.F.R. pts. 438, 440, 460).
33
For overviews of the proposed regulations, highlighting changes from the 2016 rules, see Katie Keith, HHS Proposes to Strip Gender Identity, Language Access Protections from ACA Anti-Discrimination Rule, Health Aff. (May 25, 2019), https://www.healthaffairs.org/do/10.1377/hblog20190525.831858/full; O![]() ; see also Muscemi et al., supra note 6.
; see also Muscemi et al., supra note 6.
34
Nondiscrimination in Health and Health Education Programs or Activities, 84 Fed. Reg. at 27,887. They must, however, post signs advising providers of their rights to refuse care to patients on conscience grounds.
35
Id. at 27, 849.
36
Id. at 27, 870-71.
37
Id. at 27, 864, 27,869.
38
Id. at 27,883-84.
39
42 U.S.C. § 2000d (2018).
40
Price Waterhouse v. Hopkins, 490 U.S. 228 (1989).
41
Altitude Express, Inc. v. Zarda, 139 S. Ct. 1599 (2019) (granting petition for writ of certiorari); consolidated with Bostock v. Clayton County, Georgia, 139 S. Ct. 1599 (2019); see also Hively v. Ivy Tech. Community College of Ind., 853 F.3d 339 (7th Cir. 2017) (finding that Title VII prohibits discrimination on the basis of sexual orientation).
42
20 U.S.C. § 1681 (2018); see also Jared P. Cole & Christine J. Back, C
43
42 U.S.C. § 18116(a) (2018).
44
See e.g., Pratt v. Indian River Cent. Sch. Dist., 803 F. Supp. 2d 135 (N.D.N.Y. 2011); Riccio v. New Haven Bd. of Ed., 467 F. Supp. 2d 219 (D. Conn. 2006); Harrington by Harrington v. City of Attleboro, 2018 WL 475000 (D. Mass., Jan 17, 2018); Videckis v. Pepperdine Univ., 150 F. Supp. 3d 1151 (C.D. Cal. 2015).
45
Gibbons v. Ogden, 22 U.S. 1, 78 (1824).
46
Equality Maps: Non-Discrimination Laws, M![]() (last updated Mar. 16, 2020). The three exceptions are North Carolina (bar on local law left intact through 2020 despite recent revisions to HB2), Tennessee, and Arkansas (whose bar on local ordinances was recently upheld by the Arkansas Supreme Court).
(last updated Mar. 16, 2020). The three exceptions are North Carolina (bar on local law left intact through 2020 despite recent revisions to HB2), Tennessee, and Arkansas (whose bar on local ordinances was recently upheld by the Arkansas Supreme Court).
47
For an example, see N.Y. E
48
See N.Y.C. A
49
See Darren Grant & Kelly C. Alfred, Sanctions and Recidivism: An Evaluation of Physician Discipline by State Medical Boards, 32 J. H
50
J
51
Nondiscrimination Policy H-65.983, A![]() (search “H-65.976”) (last modified 2017).
(search “H-65.976”) (last modified 2017).
52
J.J. Conger, Proceedings of the American Psychological Association, Incorporated, for the Year 1974: Minutes of the Annual Meeting of the Council of Representatives, 30 A
53
54
Church and Weldon Amendments, see 42 U.S.C. § 300a-7 (2018); Weldon Amendment, Consolidated Appropriations Act, 2009, Pub. L. No. 111-117, 123 Stat. 3034 (2009). The executive order governing conscience clause exemptions during the Bush era encompassed far more, protecting institutional and individual providers who “refuse[d] to perform health care services and research activities to which they may object for religious, moral, ethical, or other reasons.” Ensuing that Department of Health and Human Services Funds Do Not Support Coercive or Discriminatory Policies or Practices in Violation of Federal Law, 73 Fed. Reg. 78,072 (Dec. 19, 2008) (codified at 45 C.F.R. § 88). HHS replaced these exemptions under the Obama administration in 2011, which limited federal protection to enforcement of the Church and Weldon Amendments. Regulation for the Enforcement of Federal Health Care Provider Conscience Protection Laws, 76 Fed. Reg. 9968 (Feb. 23, 2011) (codified at 45 C.F.R. § 88).
55
Religious Exemptions and Accommodations for Coverage of Certain Preventive Services Under the Affordable Care Act, 82 Fed. Reg. 47,792 (Oct. 13, 2017); Moral Exemptions and Accommodations for Coverage of Certain Preventive Services Under the Affordable Care Act, 82 Fed. Reg. 47,838 (Oct. 13, 2017).
56
Protecting Statutory Conscience Rights in Health Care; Delegations of Authority, 84 Fed. Reg. 23,170 (May 21, 2019).
57
Id. at 23, 229.
58
Id. at 23, 200-01.
60
61
62
63
Simmons-Duffin, supra note 60.
64
See, e.g., Nadia Sawicki, Mandating Disclosure of Conscience-Based Limitations on Medical Practice, 42 A
65
See, e.g., Mississippi H.B. No. 1523, codified at Miss. Code Ann. § 11-62-3 et seq. (2020) (barring the state from discriminating against an individual who refuses to participate in certain treatments, counseling, or surgeries based on “the belief or conviction that: (a) Marriage is or should be recognized as the union of one man and one woman;(b) Sexual relations are properly reserved to such a marriage; and (c) Male (man) or female (woman) refer to an individual's immutable biological sex as objectively determined by anatomy and genetics at time of birth”).
66
See Jonathan Griffin, Religious Freedom Restoration Acts, N![]() .
.
67
Masterpiece Cakeshop, Ltd. v. Colo. Civil Rights Comm'n, 138 S. Ct. 1719, 1732 (2018).
68
See, e.g., Elizabeth B. Deutsch, Note, Expanding Conscience, Shrinking Care: The Crisis in Access to Reproductive Care and the Affordable Care Act's Nondiscrimination Mandate, 124 Y
69
Request for Information from Faith-Based Organizations about Lifting Regulations, 82 Fed. Reg. 49,300 (Oct. 25, 2017).
70
Farr A. Curlin et al., Religion, Conscience, and Controversial Clinical Practices, 356 N
71
John F. Dovidio & Susan T. Fiske, Under the Radar: How Unexamined Biases in Decision-Making Processes in Clinical Interactions Can Contribute to Health Care Disparities, 102 A
72
Chris Beyrer et al., A Call to Action for Comprehensive HIV Services for Men Who Have Sex with Men, 380 L
73
See Dovidio & Fiske, supra note 71, at 947; Kates et al., supra note 19, at 14; Sabin et al., supra note 71, at 1831-32, 1840.
74
Laura G. Barron & Michelle Hebl, The Force of Law: The Effects of Sexual Orientation Discrimination Legislation on Interpersonal Discrimination in Employment, 19 P
75
Id.
76
See, e.g., William J. Collins, The Labor Market Impact of State-Level Anti-Discrimination Laws, 1940-1960, 56 I
77
See, e.g., Joanna Lahey, State Age Protection Laws and the Age Discrimination in Employment Act, 51 J. L. & E
78
See John R. Blosnich et al., Mental Health of Transgender Veterans in US States With and Without Discrimination and Hate Crime Legal Protection, 106 A
79
Of a piece with this work, a longitudinal study by the same group found that the passage of state constitutional amendments banning same-sex marriage predicted subsequent increases in mood disorders and anxiety, alcohol use disorder, and psychiatric comorbidity among sexual minority populations. See Hatzenbuehler et al., Institutional Discrimination, supra note 78, at 454-55. This comes closer to the question I ask in the present project, but focuses on the signaling impacts of restrictions, and did not interrogate individuals' perceptions of (and explanations for) the law.
80
See, e.g., Riggle et al., supra note 78; Sharon S. Rostosky & Ellen D.B. Riggle, “Out” at Work: The Relation of Actor and Partner Workplace Policy and Internalized Homophobia to Disclosure Status, 49 J. C
81
Nancy E. Day & Patricia Schoenrade, The Relationship Among Reported Disclosure of Sexual Orientation, Anti-Discrimination Policies, Top Management Support and Work Attitudes of Gay and Lesbian Employees, 29 P
82
See Jason R. Lambert, The Impact of Gay-Friendly Recruitment Statements and Due Process Employment on a Firm's Attractiveness as an Employer, 34 E
83
John E. Pachankis et al., Anti-LGBT and Anti-Immigrant Structural Stigma: An Intersectional Analysis of Sexual Minority Men's HIV Risk When Migrating to or Within Europe, 76 J. A
84
85
Toni Lester, Queering the Office: Can Sexual Orientation Employment Discrimination Laws Transform Work Place Norms for LGBT Employees, 73 UMKC L. R
86
Riggle et al., supra note 78 is an example.
87
Anderson & Pildes, supra note 9, at 1565.
88
See M
89
See Rubenstein, supra note 84.
90
Katie R. Eyer, That's Not Discrimination: American Beliefs and the Limits of Anti-Discrimination Law, 96 M
91
Equality Maps: Non-Discrimination Laws, supra note 46.
92
93
The full medical mistrust score comprises three subscales measuring suspicion, discrimination, and lack of support. Qualitative interviews did not invoke suspicion of doctors' quality of care, but did reflect concern about discrimination and lack of support; given limited time for survey administration, I chose to omit the suspicion subscale and administered the other two subscales in their entirety.
94
For accuracy in perceptions of protections in health care, Pearson's chi-squared = 285.14, p = 0.000, n = 1865. Tests for other types of law were similar.
95
Accuracy about the law varied according to demographic characteristics. I developed a composite score of accuracy across all four types of legal protection. In bivariate correlations, accuracy was greater for men who were older (p<0.001), men who identified as white or Asian compared to Black or other (p<0.001), men with higher incomes (p<0.001), men with greater education (p<0.001), and men who had private insurance, Medicaid, or Medicare compared to being uninsured (p<0.001).
96
Rowell, supra note 14, at 230-31.
97
M. Ruel Friedman et al., Effects of Syndemics on HIV Viral Load and Medication Adherence in the Multicenter AIDS Cohort Study, 29 AIDS 1087 (2015); James E. Egan et al., Migration, Neighborhoods and Networks: Approaches to Understanding How Urban Environmental Outcomes Affect Syndemic Adverse Health Outcomes Among Gay, Bisexual, and Other Men Who Have Sex with Men, 15 AIDS & B
98
Nondiscrimination in Health Programs and Activities, 81 Fed. Reg. 31,376 (May 18, 2016) (codified at 45 C.F.R. pt. 92).
99
101
Rowell, supra note 14, at 277-78.
102
Id. at 262-63.
103
See id. at 240 (describing motivated cognition).
104
Ziva Kunda, The Case for Motivated Reasoning, 108 P
105
See discussion supra Parts I.A, I.B.