
Abstract

On 4 June 2022, the US Supreme Court overruled both Roe v. Wade and Planned Parenthood of Southeastern Pennsylvania v. Casey and returned the legality of abortion to the States. 1 A significant number of States subsequently banned abortion, with 13 States having even prepared so-called trigger laws in advance, ready to be enacted if the challenge was successful. This ruling is a direct assault upon the rights and bodily autonomy of women, as well as gender and health equity more broadly. In some States, this ruling does not even include exemptions for rape or incest. However, even where laws might make abortions permissible, actually finding a health provider still offering such services can be problematic. 2 Given the severe penalties involved, this ruling means that in many States life-threatening pregnancy complications will now inevitably result in unnecessary deaths of pregnant women. It is also important to note that as the American Medical Association have noted ‘States that end legal abortion will not end abortion—they will end safe abortion’. 3 An overview of negative outcomes of the Supreme Court Judgement is given in Table 1.
Wider impacts of the US abortion ban. 4
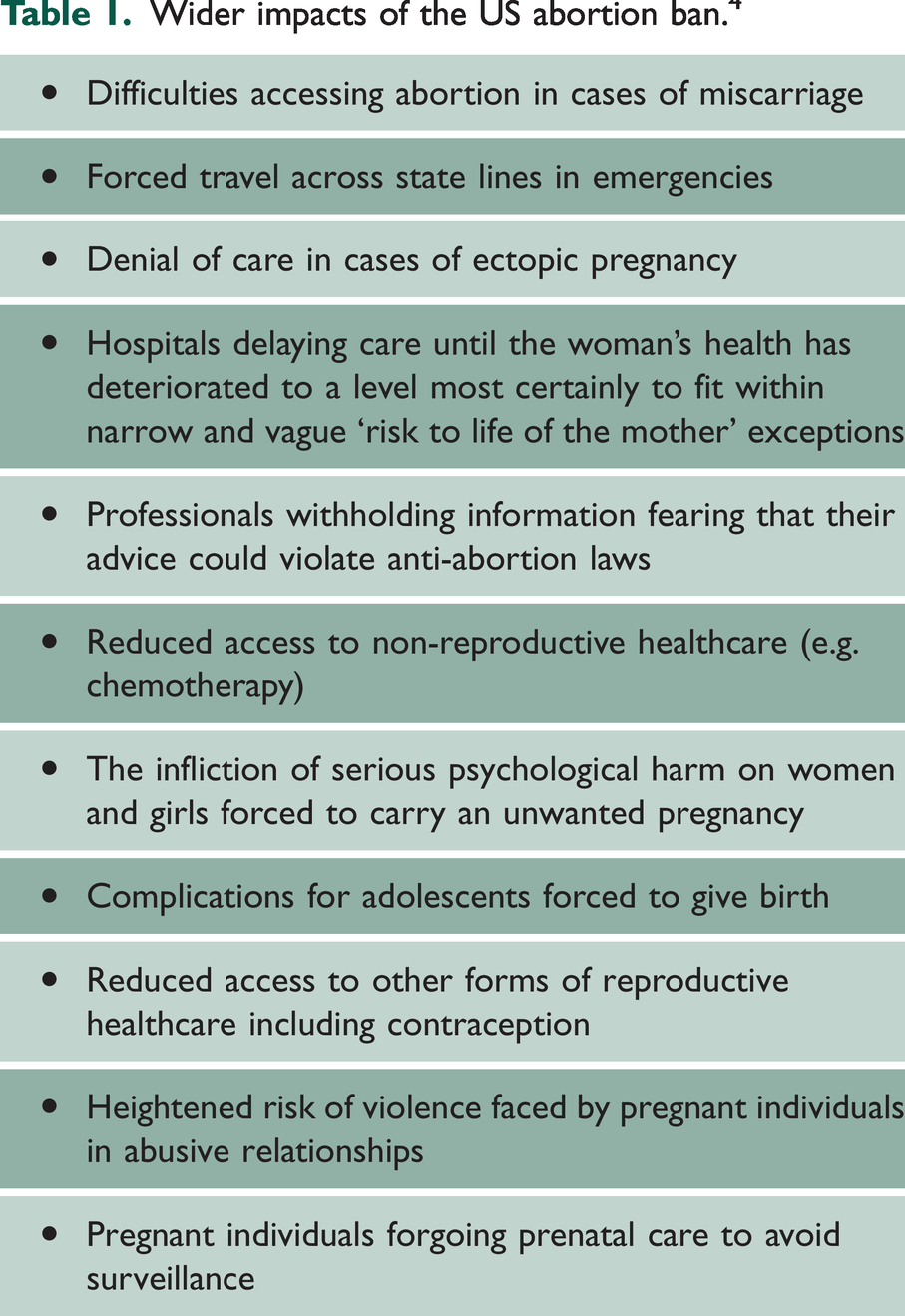
The wider implications of the Supreme Court decision may yet have implications for access to contraception, end-of-life care, care for LGBTQ patients and in-vitro fertilisation. 1
It must be acknowledged that US healthcare was broken long before these latest assaults. Maternal mortality rates in the US have been an outlier among industrialised nations for decades. US maternal and infant mortality rates are far nearer to those of significantly poorer nations than industrialised countries. In 2018, New Zealand’s maternal mortality rate, for example, was 1.7 per 100,000 live births. In the US, in contrast, it was 17.4. 5 CDC data have shown a continued rise in maternal mortality from a rate of 7.2 per 100,000 live births in 1987. 6 The National Center for Health Statistics identified the maternal mortality rate for 2021 as 32.9 deaths per 100,000 live births, compared with a rate of 23.8 in 2020 and 20.1 in 2019. In 2021, the maternal mortality rate for Black women was 69.9 deaths per 100,000 live births. 7 Given the ongoing development of abortion restrictions, this figure has probably since risen further.
Recent studies have clearly and unambiguously demonstrated significant increases in maternal mortality in States that have restricted access to abortion services.8 –10 Much of this research has documented in detail the impact of various restrictions on access to abortion services on adverse maternal outcomes. 8
Vilda et al. also note that the States imposing restrictions on abortion services are those with the worst socioeconomic status, with high rates of poverty, minimal community-oriented primary care and a lack of health and social care safety nets. 8 It is important to note that pregnancy supports in the US are minimal compared with many other developed countries. The US is the only high-income country which fails to guarantee paid leave to mothers after the birth of a child. UK mothers are entitled to 39 weeks’ Statutory Maternity Pay, while in Norway, one year paid leave is available. 4 Removing access to abortion services leaves women at significantly increased risk of economic insecurity. There is a strong concordance between those States restricting abortion services and those where the minimum State pay is the federally mandated minimum ($7.25 per hour). These same States also have a pitiful record of requiring and enforcing child maintenance payments from absent fathers. Another factor seldom mentioned in these debates is the ongoing crisis in US foster care. 11 Although fostering and adoption are routinely suggested as viable alternatives to abortion, these systems are already in disarray.
Convincing evidence has been put forward demonstrating the negative impact of racism and systemic and structural racism on morbidity and mortality rates in the US.6,12 –17 Recent analysis explicitly includes a racial element in examinations of maternal morbidity, amply demonstrating significantly higher death rates among Black mothers.6,13 –15,17
It is important to note that the curtailment of access to abortion and general maternity services will inevitably impact those at the intersection of multiple disadvantage most significantly. Thus, those minority women on low incomes, from rural, remote and disadvantaged backgrounds, with low social and education status will be most impacted. 18 The recent restrictions on abortion access will promote further inequalities, as affluent well-educated middle and higher class women will be better able to travel and access both maternity and abortion services as required.
Maternity healthcare provision in the US was highly compromised long before the recent Supreme Court decision. One obvious aspect of this is the highly inequitable access to healthcare, which negatively impacts the most disadvantaged. Although the Affordable Care Act (‘ObamaCare’) dramatically increased health insurance coverage for many women in some States, distinct problems persisted. 19 Maternity healthcare in the US is further compromised in two crucial ways. Firstly, the US has an under-supply of both midwives and Ob-gyn. The differences are stark. Sweden has, for example, 12 Ob-gyn and 66 midwives per 1000 live births, while the corresponding figures for the UK are 11 Ob-gyn and 43 midwives. The US, in contrast, has just 11 Ob-gyn and 4 midwives per 1000 live births. Thus, for every 15 maternity care providers in the US, Sweden has 78 and the UK 54.
However, it is not only the absolute number of maternity care providers in the US which is a matter of grave concern. Of equal concern is the ratio of Ob-gyn to midwives. The majority of births are low risk and do not require the skills of more expensive and longer-to-train Ob-gyn personnel. Most births can be managed by a combination of midwifery, family practitioner and general practitioner oversight. 5 Whereas Sweden and the UK have a Ob-gyn to Midwife ratios of 1:5.5, and 1:3.9 respectively, the US ratio is 1:0.4. This is unlikely to change. The US Accreditation Commission for Midwifery Education reported no growth in the number of accredited midwifery education programmes nationally between 2008 and 2018, with existing programmes routinely running under-capacity. 20
A recent analysis of the US has identified extensive maternity care deserts. Such deserts are defined as counties without a hospital or birth centre offering obstetric care, and without any obstetric (Ob-gyn/certified nurse midwives/certified midwives) providers. 17 A total of 2.2 million women of childbearing age in the US live in maternity care deserts, with another 4.7 million women living in counties with limited maternity care access. Although robust telehealth provision might be able to remediate this deficit analysis indicates that counties with low access to telehealth were 30% more likely to be maternity care deserts. 17 In American Indian/Alaskan Native populations, for example, high-speed internet access on reservations remains minimal or absent in many areas.21,22 Additional concerns include the potential for service providers in nearby states still providing abortions and maternity care to be overwhelmed. 4
The provision of maternity care is currently deteriorating in many US States as a result of the new prohibitions. Part of the reason for this is the ‘exodus’ of Ob-gyns out of states with newly introduced prohibitions on abortion. 23 However, another significant element that will increasingly feature into the future is the impact that the Supreme Court judgement will have on training in states with abortion bans.24,25 Student numbers in the Ob-gyn field generally have already declined, but notably applicant numbers have declined by twice as much in States with complete abortion bans. 26 Many physicians remain in the State in which they train, suggesting an escalating problem for maternity care in many conservative states into the future. Recent research mapping US residency programmes has predicted that over 40% of Ob-Gyn residency programmes are located in states that have already banned, or are likely to ban, abortions. 27 Given the restrictive nature of the legislation, training in the future in these States will be severely curtailed, and this must threaten both programme viability and the range of training provided.
The Dobbs ruling represents a conservative attack on the rights and bodily autonomy of all women in the US. Maternal death rates have already increased and will probably continue to rise. The ruling risks the lives of women in complicated pregnancies and threatens access to a host of maternal care services, contraceptive access and wider health services. Maternity care deserts look likely to expand dramatically in the impacted States, while bordering States may find their services stretched. Black women are likely to be most disadvantaged by the legislation. The wider impacts on training will lead to a long-term decline in training provision, which will adversely impact women in a progressively negative manner.