
Abstract

Health services now organise and evaluate performance around metrics such as speed, access routes and activity: how quickly a request is processed, how many contacts are delivered and how many patients are seen. Continuity of care in contrast has been steadily downgraded in favour of these alternative measures. 1 This shift is understandable in health systems facing high demand for care, but it has had both clinical and system consequences. By treating continuity as optional, health systems have stopped routinely monitoring whether care remains coherent over time, whether responsibility is held across healthcare encounters and whether complex problems are resolved rather than being repeatedly revisited.
Why continuity matters
The critical point is that continuity is not merely about familiarity or patient satisfaction. It functions as both a safety and an efficiency mechanism in clinical contexts where uncertainty is high and consequences are asymmetric such as multimorbidity, frailty, serious mental illness and safeguarding. 2 In these settings, fragmentation does not simply create inconvenience. It increases the likelihood of delayed diagnosis, duplicated testing, medication drift, avoidable escalation and an erosion of trust that makes future care less effective.
Continuity is commonly described across three overlapping domains: relational, informational and management.1 –3 Informational continuity concerns whether meaningful knowledge is available, interpretable and trusted across settings. Management continuity concerns whether care plans remain coherent over time and across transitions. Relational continuity concerns whether an ongoing therapeutic relationship exists with a clinician, or a small stable team, who accumulates knowledge about the patient’s baseline, preferences, risks and thresholds. All three are necessary, but relational continuity plays a distinctive role in complex care because it is the only domain that reliably produces clinical synthesis. A record can hold facts; a relationship holds meaning. When patients repeatedly present with the same unresolved problem, relational continuity increases the likelihood that someone will detect the clinical trajectory rather than simply document events.
This commentary advances a specific argument: the central failure is not simply the erosion of relational continuity but the absence of metrics that capture whether care episodes reach resolution rather than being repeatedly managed. What is currently measured is access; what matters clinically is resolution.
Continuity as a promotor of safety and efficiency of care
Resolution refers to whether a clinical problem is actively owned across encounters until it reaches a defined endpoint – such as diagnostic clarification, stabilisation or agreed management – rather than being repeatedly addressed as a series of isolated decisions. This distinction is largely absent from contemporary performance frameworks.
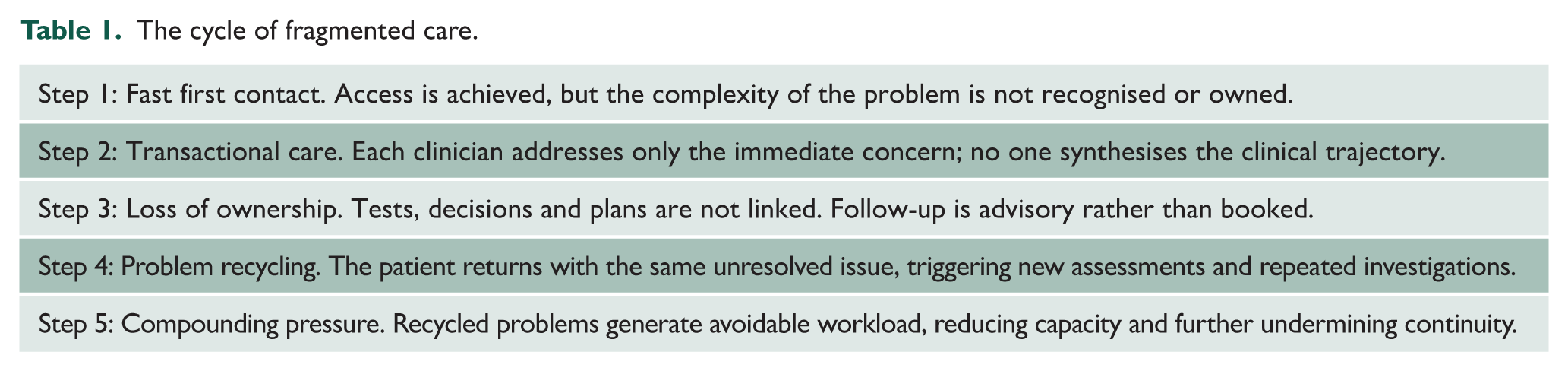
The contemporary evidence base should have moved continuity towards the centre of quality assessment rather than away from it. A systematic review focusing on personal continuity between patients and general practitioners found that higher continuity is associated with improved outcomes, including reductions in premature mortality and hospital utilisation, with moderate certainty for these outcomes. 1 The review also suggested that relatively small improvements in continuity could lead to meaningful reductions in unplanned hospital admissions and emergency department attendances. This matters for policy because it reframes continuity from a perceived trade-off against access into a potential lever for access: if continuity reduces repeat contacts and avoidable escalation, it may create capacity rather than consume it (Table 1).
The cycle of fragmented care.
Why continuity has declined
Despite this, continuity in English general practice has declined. A longitudinal analysis demonstrated a substantial fall in relationship continuity over recent years, accompanied by widening variation between practices. 2 The associations identified are instructive. Practices with greater clinical capacity and higher proportions of same-day contacts experienced slower declines, indicating that continuity is shaped by service configuration. If continuity is eroding, it is in part because systems have been designed to prioritise throughput and flexibility over longitudinal ownership.
The relationship between access and continuity is often framed as a zero-sum equation. Yet emerging evidence challenges this assumption. A large analysis of English primary care consultations reported that continuity was associated with increased physician productivity by reducing demand for additional consultations. 3 The implication is not that continuity is easy to deliver under workforce constraints, but that systems which systematically undermine continuity may be self-defeating. Fragmented care increases re-attendance, duplication and escalation, allowing services to appear fast at first contact while becoming slow in resolution, with rising workload as a downstream effect.
Limitations of contact-based metrics
This exposes a central weakness in current measurement methods. Dominant primary care metrics are contact-based: such as time to first response, appointment numbers, waiting times and system throughput. These measures describe how efficiently demand is converted into an interaction. They do not capture whether the interaction resolves the clinical episode, whether responsibility for follow-up is explicit, whether results are owned and communicated or whether a reliable route back exists if symptoms persist or change. In short, they measure access to contact rather than continuity of resolution.
Clinically, this distinction is critical because fragmentation rarely manifests as a single identifiable error but rather as incomplete closure. Unresolved problems are managed through serial low-risk decisions that are individually defensible but cumulatively inadequate. Results are reviewed without synthesis across time. Care plans are generated without a clearly accountable relationship. Safety-netting becomes passive, relying on the patient’s capacity to re-access care rather than the system’s ability to track and review. In patients with multimorbidity, this pattern amplifies guideline conflict and polypharmacy risk. 4 In the absence of continuity, additive prescribing, cautious investigation and deferred trade-offs become the path of least resistance – particularly when follow-up access is uncertain.
Frailty intensifies these risks. In frail patients, small clinical decisions carry disproportionate consequences. Early deterioration often presents as a subtle deviation from baseline rather than a discrete abnormality. 5 Management continuity is therefore inseparable from relational continuity: clinicians must understand not only what was done, but how this individual usually responds to illness and what outcomes matter most to them. Fragmented care pushes frail patients towards reactive pathways, increasing emergency admissions and iatrogenic harm.
An investigation into delayed diagnosis in general practice identified lack of continuity systems as a contributory safety risk. 6 The mechanism described was not incompetence, but diffusion of responsibility and loss of synthesis. When multiple clinicians see a patient over time without a continuity framework, no one is positioned to recognise patterns of repeated presentation or escalating risk. In such systems, individually ‘safe’ decisions can accumulate into unsafe trajectories. This is a systems failure driven by allocation of work and follow-up design, not individual clinician performance.
There is now growing recognition that continuity is a safety issue rather than a preference. NHS England’s primary care patient safety strategy explicitly links continuity of care to safety and workload. 7 The challenge is operationalisation. Strategies frequently endorse continuity in principle while leaving services without mechanisms to protect it when access pressures intensify. Without measurement, continuity remains invisible and therefore expendable within commissioning and performance frameworks.
Designing systems for continuity and resolution
A modern framing is therefore required. Continuity should be understood not only as relational familiarity but also as continuity of responsibility and continuity of resolution. The practical question for systems is not whether every encounter must involve the same clinician, but whether accountability is maintained across time until problems reach closure. Relational continuity can be supported through micro-teams, defined clinical ownership for high-risk groups and appointment rules that prioritise continuity for follow-up. Management continuity can be strengthened through explicit care plans that specify responsibility for results, timing of review and escalation triggers. Informational continuity can be improved through record design that privileges trajectory and meaning rather than isolated events.
Measurement must mature accordingly. Reducing continuity to the proportion of contacts with the same clinician risks flattening a complex function into a crude ratio. A more informative approach would complement relational measures with indicators of resolution: whether repeated contacts for the same problem are recognised as a longitudinal episode; whether follow-up recommendations result in booked review rather than aspirational advice; whether test ordering includes a named reviewer and review-by time and whether safety-netting includes a reliable re-entry route that does not depend on persistence, literacy or luck. None of these indicators conflict with access ambitions. They acknowledge that access without resolution is a fragile success.
Equity considerations are central. When continuity is framed as a preference to be requested, it is distributed by confidence and capacity rather than clinical need. Patients most likely to benefit – those with multimorbidity, frailty, mental illness, safeguarding risk, learning disability, neurodivergence or language barriers – are also those most disadvantaged by transactional systems. A model that delivers equal speed while fragmenting care for those with greatest complexity is not equitable; it is predictably harmful. Restoring continuity, particularly for high-risk groups, is therefore both a clinical and fairness imperative.
There is also a workforce dimension that remains under-acknowledged. Continuity reduces cognitive load and duplication by allowing clinicians to start from a richer, more reliable model of the patient. It reduces defensive practice, supports safer prescribing and deprescribing through longitudinal monitoring and shared decision-making that is not reset at each contact. It also restores professional meaning by re-embedding clinical decisions within a narrative rather than a series of transactions. In a context where retention is as critical as recruitment, these conditions should be recognised as part of the safety infrastructure.
The way forward
Continuity cannot be restored by rhetoric alone. Workforce constraints, part-time working and rising demand are all real challenges. The argument here is that continuity should no longer be treated as an unmeasured casualty of modern service design. If continuity is clinically protective and system-efficient, failure to measure it represents a governance error. Health systems optimise what they count. When continuity disappears from dashboards, it becomes structurally unsupported.
A clinically coherent performance framework would therefore treat continuity as an outcome alongside access and safety. It would recognise continuity of resolution as a measurable property of care, particularly for those at highest risk. It would support service models that preserve relational continuity through defined ownership while maintaining timely access. Above all, it would align policy intent, commissioning incentives and operational design around a simple principle: fast contact is not the endpoint. Coherent care over time is.
Conclusion
Continuity is not an argument against innovation. Integrated care, multidisciplinary practice and digital access can all improve outcomes, but only if they preserve longitudinal synthesis rather than replacing it with transactions. The outcome we stopped measuring remains among the most clinically consequential. Restoring continuity as a core metric will not resolve every pressure facing primary care, but it would correct a fundamental distortion in what we currently treat as success. Continuity of resolution therefore functions as a core safety mechanism and an efficiency mechanism; precisely the qualities health systems attempt to optimise but currently fail to measure.