Abstract

Patient-centred care has become a key concept in modern medicine. Most clinicians recognise its core principles: treat the person, not just the disease; listen carefully; explain clearly; involve the patient in decisions. Yet many patients still experience care as something done to them, with their role limited to occupying the centre of a system whose rules are already fixed. The gap is not primarily about empathy; it is about power: who defines the problem, who designs the clinical pathway, who determines the outcomes and who has the authority to change the rules when they fail.
The limits of ‘patient-centred’ become visible whenever the consultation collides with the system around it. A patient with multimorbidity may need time, continuity and coordination, but the template allocates a fixed time and fragments responsibility across different services and clinicians. Someone with intermittent symptoms may need an agreed safety-net and an easy route back, but the access model treats repeat contact as misuse. A patient who cannot manage online forms may be told the service is still available by phone, yet the phone queue is an hour (or more) and the call-back arrives while they are at work. These are not failures of bedside manner; they are design choices.
Patient-shaped care is a more demanding concept. It preserves the ethical core of patient-centred care but introduces a deeper question of governance: are patients simply invited to choose between options already defined by clinicians and healthcare organisations; or do they share authority over how those options are created and how success is evaluated? Shared decision-making is necessary, but it offers limited real choice when the available options are constrained by service configuration, capacity limits, rigid pathways or organisational risk thresholds rather than by evidence and patient priorities. 1 Patient-shaped care therefore begins earlier and extends further, reaching beyond the moment of decision to the systems that shape the choices themselves.
This matters clinically because much of what we do is not a discrete decision but a longitudinal relationship with uncertainty.2,3 For multimorbidity, there is often no single best option, only trade-offs across areas such as symptoms, physical function, treatment burden and risk. In mental health, chronic pain, frailty and medically unexplained symptoms, the work is frequently about meaning, pacing and the credibility of suffering as much as diagnostic labels. When patients cannot influence the structure of follow-up, continuity and escalation, ‘involvement’ in decisions is inevitably constrained to what can be fitted into a single encounter.
Patient-shaped care therefore has an organisational dimension. Access systems are part of clinical quality, not mere logistics. Digital routes can improve the speed and convenience of access to care, but they can also widen inequity when literacy, language, disability, device access and confidence are unevenly distributed. 4 A patient-shaped approach does not choose between ‘digital first’ and ‘face-to-face’; it designs multiple equivalent routes into care, with the same clinical standards, and it funds the support that makes those routes usable. It also co-designs escalation: what a patient should do when symptoms worsen, when test results are overdue or when anxiety is rising. The practicalities of access are often the difference between early review and late presentation.
Patient-shaped care has to travel across organisational boundaries. Much patient harm and frustration accumulates in clinical handoffs: discharge summaries that arrive late, medication lists that do not match what was prescribed, outpatient letters written for other clinicians rather than for the patient and follow-up plans that assume unlimited time, transport and health literacy. A patient-shaped system would co-design the minimum reliable information set for transitions and build ‘closed-loop’ communication so that referrals and results are processed systematically. It would also treat access to records as part of care, enabling patients to check, correct and carry their clinical story, rather than repeatedly re-tell it, especially when care is fragmented.
If patient-shaped care is to be more than a slogan, it needs governance. Many health systems now undertake patient and public involvement, but tokenism is predictable when roles are unclear, recruitment is narrow and the work is under-resourced.2,3 Co-design and co-production methods offer more robust ways to share power, but they are not quick fixes; they require facilitation, iterative testing, documentation and evaluation.5,6 At the system level, involvement remains patchy, with variable definitions and limited long-term evidence on costs and impact, which makes it easy for organisations to declare commitment while avoiding accountability. 7 Patient-shaped care treats involvement as part of clinical governance: it has standards, resources and consequences.
Representation is the hardest problem. ‘The patient voice’ is not a single thing. A committee populated by confident, retired, English-speaking volunteers will not reliably represent a working mother with asthma, a migrant with limited literacy or a young man avoiding mental health services. Patient-shaped care therefore needs legitimacy safeguards: transparent selection, rotation, remuneration for time and expertise, accessible formats and explicit attention to who is missing. Paying patient partners is not a luxury; it is an equity intervention and a signal that lived expertise is real expertise.
Clinicians often worry that shifting power will produce unlimited demand. In practice, patient-shaped governance can make rationing more legitimate by making trade-offs explicit. When patients help shape the rules of access, continuity and prioritisation, the conversation moves from consumer grievance to shared stewardship. The ethical question becomes: how should finite capacity be used so that care is fair, safe and humane?
Quality improvement is a natural home for patient-shaped care, but only if patients are treated as partners rather than as occasional storytellers. Effective partnerships require shared leadership, co-learning and support for both staff and patient partners, including role clarity and development. 8 This is work: it needs protected time for induction, safeguarding and supervision. Done well, it can also reduce rework, complaints and wasted effort by aligning processes with the realities of living with illness.
Measurement is where patient-centred care often becomes performative. Organisations measure what is easy; for example, throughput, waiting times and satisfaction. Patients however care about being able to reach help when worried, being recognised and remembered, having a coherent plan and avoiding harm at transitions. Patient-shaped care needs a small, co-designed outcomes set that includes not only clinical indicators but also capability and agency: can the patient understand the plan, influence it and act on it? Tools that assess activation can help operationalise agency, but they must be used as mirrors for system design, not as instruments of blame. 9 Low agency should trigger redesign – simpler processes, better continuity, translation and practical support – rather than moralising about ‘engagement’.
Continuity is a concrete test case because it links experience to outcomes and efficiency. Higher relational continuity in primary care is associated with lower mortality, and the erosion of continuity has been framed as a policy and practice problem rather than an inevitable trend. 10 Empirical work has documented declining continuity in England over time. 11 Continuity can be measured using routine data and correlated with what patients report, allowing organisations to treat it as a quality metric rather than. 12 Patient-reported continuity measures also show associations with outcomes across settings. 13 Patient-shaped care would therefore design continuity deliberately: target it to those with complex needs, monitor it transparently and align access models so that ‘rapid access’ does not quietly dismantle relationship-based care.
Safety provides another sharp contrast between centring and shaping. Person-centred interventions are often assumed to improve safety, but the evidence is mixed and context-dependent. 14 Patient-shaped care responds by treating patients as partners in safety design: co-creating clear safety-netting language, reliable test-result communication, medication reconciliation processes and escalation routes that work in real life. It also brings patient partners into learning from harm, not as witnesses but as contributors to redesign. Learning health systems, in particular, risk optimising what is easily counted unless patients help interpret data, define value and set improvement priorities. 15
Health policy can either enable or undermine this shift. When funding and regulation prioritise speed and volume, patient-shaped care is easily displaced. By contrast, commissioners and regulators can promote it by requiring evidence of co-designed access standards, co-produced outcome measures and transparent reporting of continuity, safety-net reliability and equity impacts. They can also ensure that patient partnership is properly resourced through paid roles and training, rather than relying on voluntary labour. Data policy matters as well: patients cannot shape care if they cannot see how the system performs. Transparency underpins shared accountability.
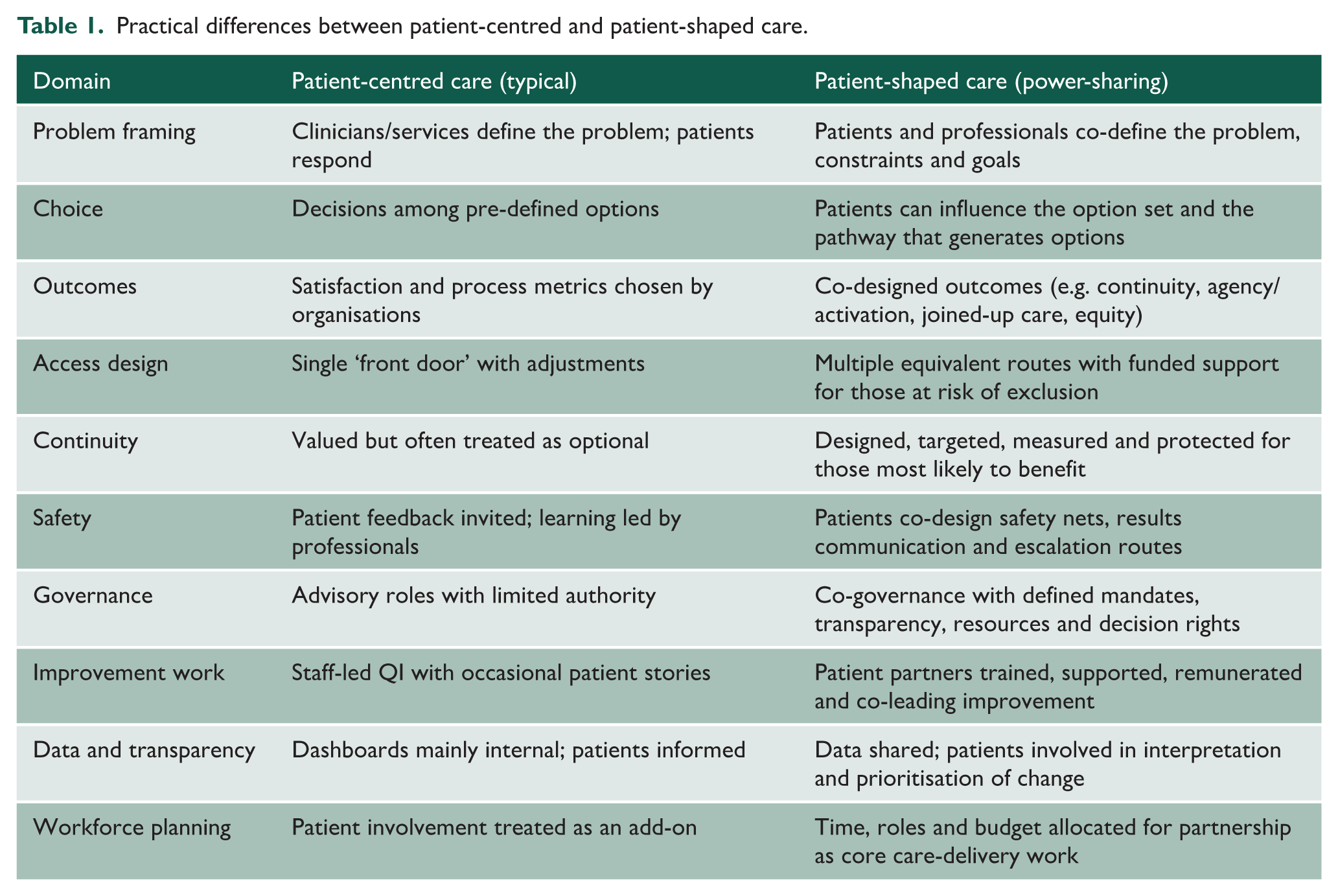
Patient-shaped care is not an optional add-on for already overstretched health services. It is a strategy for making care more clinically effective, safer and more legitimate in the face of growing complexity and resource constraints. It asks clinicians to broaden their understanding of professionalism: not only to make good decisions in the consultation room but also to question and redesign the systems in which those decisions are made. The practical differences, and the tests of whether power is genuinely shared, are summarised in Table 1. If patient-centred care concerns posture, patient-shaped care concerns structure. It is about sharing power, not merely decisions.
Practical differences between patient-centred and patient-shaped care.