
Abstract
Risk of self-harm among clinic referred children aged 6- to 12-years-old was investigated using the recently developed Self-Harm Risk Assessment for Children (SHRAC) instrument which comprises six factors: Affect traits; verbalizing of self-harm; socialization; dissociation; self-directing; and self-appraisal. The SHRAC was completed by the mothers of 125 primary school aged children referred to a University based clinic for psychological assessment. These children were subsequently assigned to one of four groups (non clinical, externalizers, internalizers, and combined internalizers/externalizers). Multivariate analysis of variance with univariate F and Scheffé follow-ups revealed differences in risk of self-harm between the four groups. Overall, individuals with both internalizing (anxiety/withdrawn, anxiety/depressed and somatic complaints) and externalizing (rule-breaking behavior and aggressive behavior) characteristics were more at risk of self-harm. These individuals scored highest across each of the six domains. The findings demonstrate the SHRAC to be a reliable instrument for educational psychologists to use with children they suspect of being at risk of self-harm.
Deliberate self-harm (DSH) among young people and adults is a major public health issue (Borschmann, Hogg, & Phillips, 2011; Pryjmachuk & Trainor, 2010), blighting the lives of young people, seriously affecting their relationships with families and friends, and presenting a major challenge to services and organizations from schools through to hospital accident and emergency departments (see Tuisku et al., 2009). According to Warm, Murray, and Fox (2003) DSH has been used interchangeably with terms such as self-mutilation and self-injurious behavior to describe a form of actively managed self-destructive behavior that is not intended to be lethal. DSH has also been defined as the intentional and direct destruction or alteration of body tissue, resulting in tissue damage (see Fliege et al., 2006) and as the intentional injuring of one’s own body without apparent suicidal intent or intention to die (Klonsky, Oltmanns, & Turkheimer, 2003; Tuisku et al., 2009). Many definitions of DSH deliberately exclude behaviors with conscious suicidal intent but as argued by some researchers, intent cannot always be reliably measured (Cooper et al., 2005; Pryjmachuk & Trainor, 2010). Thus, it may be important to assess for the presence of suicidal behaviors in studies of DSH given the high rates of comorbidity between the two and that risk of suicide increases with a history of DSH (Borschmann et al., 2011; Cooper et al., 2005; Greydanus & Shek, 2009; Ougrin et al., 2011; Zahl & Hawton, 2004).
Although DSH has become increasingly prevalent among adolescents (Fortune & Hawton, 2005; Hawton & Harriss, 2008; Laukkanen et al., 2009) establishing the precise prevalence is difficult, primarily because of a reliance on hospital-derived data and the relative lack of community studies (Storey, Hurry, Jowitt, Owens, & House, 2005), and definitional issues (Best, 2006; Gratz, 2001) irrespective of the country reporting the evidence (Chitsabesan, Harrington, Harrington, & Tomenson, 2003). According to Hawton, Rodham, Evans, and Weatherall (2002), 6.9% of UK 15- to 16-year-olds (11.2% of girls and 3.2% of boys) report an act of self-harm and of these, only 12.6% result in presentation to hospital. Similar hospital presentation rates of 12.2% and 11.3% have been reported for 14- to 17-year-olds from Australia, Belgium, England, Hungary, Ireland, The Netherlands, and Norway (Ystgaard et al., 2008) and Ireland (Morey, Corcoran, Arensman, & Perry, 2008), respectively. Further data from the UK suggests that 5.8% of 5 to 15 year olds have attempted to hurt, harm or kill themselves at some point (Meltzer, Harrington, Goodman, & Jenkins, 2001).
In Ireland, a cross-sectional survey of 3,881 adolescents by Morey et al. (2008) found a lifetime DSH prevalence rate of 9.1%, with 45.9% of these young people’s reporting more than one episode of DSH. Females (13.9%) reporting DSH outnumbered males (4.3%) and self-cutting (66%) was more common than drug overdose (35%). Higher life time prevalence of self-cutting (11.4%) and other self-harm (10%) has been found among Finnish adolescents aged 13-18 years (see Laukkanen et al., 2009).
In one of the largest studies conducted to date, Madge et al. (2008) examined data from over 30,000 14- to 17-year-olds from Australia, Belgium, England, Hungary, Ireland, Netherlands, and Norway. Overall, 8.9% of females and 2.6% of males reported an episode of DSH in the 12 months prior to the study, while 13.5% and 4.3%, respectively, reported an episode during their lifetime. Of seven countries, Australia recorded the highest rate for females DSH (11.8%). The data also revealed that one in five females and one in ten males had thought about DSH. With reference to method of DSH, 55.9% involved self-cutting only, 22.3% overdose only, 11.7% another single method, and 10.7% multiple methods. Among the specific methods cited was hanging or strangulation, electrocution, shooting, drowning, burning and self-battery. Participants commonly cited multiple reasons to explain their DSH, with the most frequent being “I wanted to get relief from a horrible state of mind” (70.9%), “I wanted to die” (59%), and “I wanted to punish myself” (43.6%). Madge et al. (2008) concluded that ‘much more attention needs to be paid to identifying young people who are suffering from emotional and mental health difficulties in order to prevent self-harm’ (p. 676).
In a USA based study involving 3,332 12- to 15-year-olds, Patton et al. (2007) reported a prevalence of DSH of 3.7%, with a more than two-fold higher rate in females. In Canada, Nixon, Cloutier, and Jansson (2008) analysed data from the Victoria Healthy Youth Survey, a population based longitudinal survey of 14- to 21-year-olds in Victoria British Columbia. Of 568 participants, 16.9% reported they had deliberately harmed themselves, with 37.6% reporting DSH on more than three occasions. Cutting, scratching, and self-hitting were most frequent (83.2%). More females (77%) than males reported DSH, with 40% of these reporting repeated (i.e. >3) DSH. Similar lifetime prevalence rates for DSH have been found in two other Canadian studies: 13.9% (Laye-Gindhu & Schonert-Reich, 2005) and 15% (Heath, 2003).
In Australia the focus of DSH research has primarily been on late adolescence through to middle adulthood (i.e., 16-years-old and above; Chitsabesan et al., 2003). Furthermore, most of this research has focused on individuals in institutional settings such as inpatient psychiatric units. In one of the few school-based studies of self-harm in Australia, DeLeo and Heller (2004) administered several instruments to 3,757 Year 10 and Year 11 (16- to 17-year-olds) students from 14 Gold Coast, Queensland high schools. Findings revealed that 233 students (6.2%) met the criteria for having deliberately self-harmed over the previous 12 months, with the prevalence being considerably higher in females than males. In New Zealand, Coggan, Bennett, Hooper, and Dickinson (2003) found that of 3,265 adolescents surveyed 32% had thought about DSH and 19% had attempted DSH. Somewhat similar rates of DSH among New Zealand high school students were also reported by Garisch and Wilson (2010). That is, approximately 15% had self-harmed at least once, with females (19%) reporting greater rates than males (8%).
The incidence of DSH among adolescent inpatients is much higher than in non referred populations, ranging from 40% to 61% (see Suymoto, 1998). Indeed, associations between DSH and psychopathologies is extensive: borderline personality traits (Herpertz, Sass, & Favazza, 1997; Paris, Zweig-Frank, & Guzder, 1994), dissociation (Briere & Gil, 1998; Nijman et al., 1999), eating disorders (Favaro & Santonastaso, 1998), anxiety (Briere & Gil, 1998; Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006) and depression (Fliege et al., 2006; Harrington et al., 2006; Klonsky et al., 2003). Prevalence of DSH among 5- to 16-year-olds with emotional disorder (28%), conduct disorder (21%), and hyperkinetic disorder (18%) has also been found to be considerably higher than general prevalence rates (Green, McGinnity, Meltzer, Ford, & Goodman, 2005).
Data pertaining to young persons under 15 years of age who present to general hospitals because of DSH, are limited however. One of the few studies conducted analysed data covering a 25-year period, during which time young people aged 15 years and under presented at one general hospital in Central England following acts of DSH. Findings revealed that 710 individuals (the youngest being 8-years-old) presented with a total of 831 episodes (118 males and 713 females) (see Hawton & Harriss, 2008). Some 92% of episodes involved self-poisoning alone (primarily using analgesics), with the remainder being a combination of self-poisoning and cutting. Of those who received a psychosocial assessment, 27% had a history of previous DSH and 26% repeated DSH later during the study period.
In summary, it is recognized that rates of DSH are higher than those actually recorded due to the under-reporting of the phenomenon (Sawyer et al., 2001). One reason for this may be the focus on older adolescents, with few studies being conducted with younger children and young adolescents. Furthermore, small sample sizes and/or specially selected cases such as psychiatric inpatients appear to have been the main methodological characteristics of the studies conducted (Hawton & Harriss, 2008).
Given that treatments have not been particularly successful in reducing repetition of DSH (Low, Jones, Duggan, Power, & MacLeod, 2001), Best (2006) emphasized the importance of the primary school years in the development of young people and advocated a “prevention is better than cure” (p. 173) approach. Little is known about DSH in this population and to improve educational and clinical practice it is important to increase our knowledge of DSH (Klonsky et al., 2003) in various contexts.
The research presented here addresses the relative absence of information about risk of DSH in young children by examining data obtained from the mothers of children referred to a university based clinic for child and adolescent disorders. To date, studies of DSH have tended to rely on interviews or self-report of participants to measure psychological variables. According to Klonsky et al. (2003) verbal reports about one’s own mental processes can be inaccurate and misleading. Thus, assessing the psychopathology of self-harmers through instruments that do not rely on self-reports may improve the validity of any findings. Furthermore, given that we were collecting information about young children we decided that those who know the young school aged child well (i.e., parents) would be more reliable informants on his/her behavior, than the child him/herself. Although some concern has also been expressed that parents are often unaware their children are self-harming (Meltzer et al., 2001), this has primarily been where family dysfunction occurs (Pfeffer, 2000). Parent reports are often solicited by educational psychologists as part of the diagnostic process and studies point to the value of parents as reliable sources of information on the behavior of young people (see Mitsis, McKay, Schulz, Newcorn, & Halperin, 2000; Rogers, Wiener, Marton, & Tannock, 2009).
Method
Participants and settings
The Self-Harm Risk Assessment for Children (SHRAC; Angelkovska, 2008) instrument and the Achenbach Child Behavior Checklist (CBCL; Achenbach, 1991) were administered to 125 mothers of clinic referred children who provided data on their children. The ages of the children ranged from 6- to 12-years-old (Mean = 9.06 years, SD = 2 years); 83 were male (66.4%) and 42 were female (33.6%). To be included in this group the children had to be (i) aged between 6- and 12-years-old and experiencing problems at school that were either behavioral, learning, or both; (ii) currently not receiving clinical intervention from either a Child and Adolescent Mental Health Service (CAMHS) or psychiatrist, and (iii) the problem behaviors did not meet criteria specific to any psychiatric disorder classified under the DSM-IV-TR (American Psychiatric Association, 2000). The mothers of the children, who were recruited from the database of the University based referral clinic, completed the instruments while at the clinic with their child(ren).
The children were subsequently categorized into one of four groups (Non clinical, Externalizers, Internalizers, and Combined internalizers/externalizers) based on the scores for the internalizing and externalizing composites of the CBCL as derived by Achenbach (1991).
Instrumentation
The 33-item SHRAC, which is available from the first author on request, was initially developed from a review of the literature relating to self-harm and a number of established instruments that measure self-harm, risk of suicide attempt, and variables associated with self-harming behavior (e.g., depression, anxiety, impulsivity, externalizing/internalizing behaviors). New items for the SHRAC were also generated from semi-structured interviews conducted with experienced developmental pediatricians (pediatric experience range = 15 to 40 years) and 24 mothers (age range 35- to 45-years-old) whose children had been referred to a university based clinic for assessment as a result of verbalized self-harming ideation, and/or engagement in self-harming behaviors.
The psychometrics of the SHRAC are well established with item affectivity values ranging between 0.35 and 0.75 and item discrimination values ranging between 0.34 and 0.85 (see Kline, 2000). Exploratory factor analysis has revealed six factors comprising 33 items: Seven-item Affect traits (internal distress); six-item Verbalizing of self-harm (overt verbal threats of self-harm); five-item Socialization (social withdrawal or preference to be on own); four-item Dissociation (the child’s difficulty separating reality from fantasy); six-item Self-directing (the degree to which the child is motivated to succeed, the motivation is essentially self-driven); and five-item Self-appraisal (a negativistic attitude directed towards the self). With an overall Chronbach’s alpha of 0.92 and alphas for the subscales: Affect traits (α = 0.79), Verbalizing of self-harm (α = 0.86), Socializing (α = 0.76), Dissociative (α = 0.59), Self-directing (α = 0.81) and Self-appraisal (α = 0.83) the 33-item SHRAC has a satisfactory degree of internal consistency. An independent samples t-test has also demonstrated the SHRAC differentiates risk of self-harm between clinic referred and a community comparison group of age matched children t(196) = 11.388, p < 0.001 (Angelkovska, 2008).
SHRAC items are preceded by the statement ‘My child … ’, and participants respond to each item by circling a number that denotes one of four response options, ranging from ‘Always’ (score 4) to ‘Rarely’ (1). For each of the items parents are also required to indicate with either a ‘Yes’ or ‘No’ to the statement ‘Have these behaviors been present for six months or longer?’.
The Achenbach Child Behavior Checklist was also administered to the mothers to determine the range and severity of problem behaviors in the referred group. It was also administered so that participants could subsequently be assigned to one of four different groupings used as the independent variables in the multivariate analysis conducted.
The CBCL is one of the most widely used checklists in clinical settings and assesses behavior problems in individuals aged between 4- and 18-years-of-age. The checklist allows individual behavior problems (e.g., anxiety, depression, somatic complaints, social problems, attention problems, thought disorder, conduct problems, and aggressive problems) to be assessed in addition to providing an assessment of broader band problems (e.g., externalizing behavior problems and internalizing behavior problems) and an assessment of the totality of the problem behaviors. It uses a three-point scale ranging from 0 (Not true), 1 (Sometimes true) to 2 (Very often true). Test–retest reliabilities are reportedly in the high 0.80s with good inter-parent agreement correlations ranging from 0.65 to 0.75. Additionally, the CBCL has been shown to possess sound content, construct and criterion related validity with supporting evidence that the items of the CBCL are able to discriminate between demographically matched referred and non-referred children (Achenbach, 1991).
Procedure
Approval was obtained from the administering institution’s Human Research Ethics Committee. The database at the university based referral clinic was searched for children who met the inclusion criteria. Each of the mothers whose children met the study inclusion criteria were then sent an information sheet explaining the purpose of the research along with a consent form and a reply paid envelope. A follow up telephone call was made to individual mothers three days after receiving returned consent forms to confirm appointment times at the clinic. The instruments were administered by the first author who is a state registered psychologist.
To determine whether SHRAC scores differentiated between children who presented with externalizing behaviors or internalizing behaviors, (two problem behaviors known to be associated with DSH), participants were assigned to one of four groups (Non clinical, Externalizers, Internalizers, and Combined internalizers/externalizers) based on the scores for the internalizing and externalizing composites of the CBCL as derived by Achenbach (1991). The internalizing composite of the CBCL includes items relating to Anxiety/Withdrawn, Anxiety/Depressed and Somatic complaints, while the externalizing composite of the CBCL includes items relating to Rule-breaking behavior and Aggressive behavior. Participants who received a T-score greater than or equal to 65 for the internalizing composite were assigned to the ‘Internalizing’ group, while participants with a T-score greater than or equal to 65 for the externalizing composite were assigned to the ‘Externalizing’ group. Participants with a T-score greater than or equal to 65 on both the internalizing and externalizing composite scales were assigned to a ‘Combined’ group. Some participants within the referred group had scaled scores on each of the composites below a T-score of 65. That is, their scores did not meet the criteria for inclusion in either the Internalizing group or Externalizing group. In such instances individuals were assigned to a ‘Non clinical’ group.
Results
A multivariate analysis of variance was conducted to explore the effect of the independent variable of group on the six variables of the SHRAC. Wilks’ criterion was used to evaluate multivariate significance, and univariate F-tests were conducted when significant multivariate results were obtained. Univariate F-values were determined to be significant using a Bonferroni-adjusted α level of 0.008 to control for Type 1 errors. Effect sizes and power estimates are reported. Scheffé post hoc comparisons were also conducted to explore mean differences, and these are reported where there were significant differences between the means.
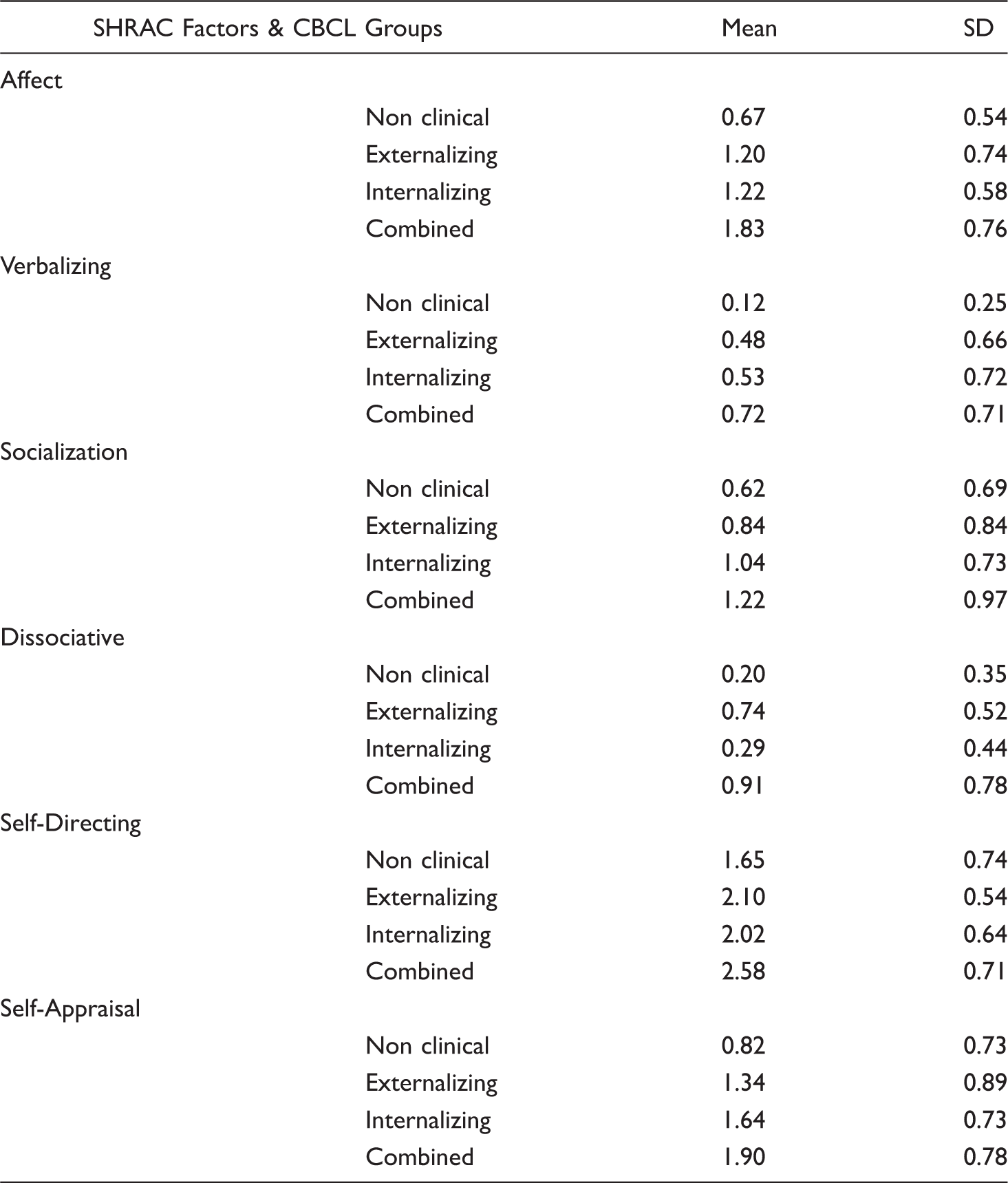
There was a multivariate main effect of group F(3, 121) 4.57, p < 0.001, partial η2 = 0.22. The follow-up Univariate F-tests revealed significant differences for five of the six dependent variables: Affect F(3, 1,410.83) 18.78, p < 0.001, η2 = 0.31; verbalizing F(3, 534.17) 8.01, p < 0.001, η2 = 0.16; Dissociative F(3, 1,003.27) 19.48, p < 0.001, η2 = 0.32; Self-directing F(3, 674.10) 8.33, p < 0.001, η2 = 0.17; and Self-appraisal F(3, 748.54) 10.57, p < 0.001, η2 = 0.20. There was no main effect for Socializing F(3, 286.11) 2.92, p > 0.05, η2 = 0.06.
Observed means with Standard Deviations for the SHRAC factors according to non clinical (n = 55), externalizing (n = 29), internalizing (n = 18), and combined (n = 23) grouping
Discussion and implications
This research has used an empirically derived instrument (the SHRAC) to assess risk of self-harm among young school aged children. Given the absence of such instruments and the call for the comprehensive and thorough assessment of individuals who self-harm, including risk for suicide (Isacsson & Rich, 2001) the development of the SHRAC is timely. Moreover, given that DSH among adolescents is an international problem of a considerable scale (Madge et al., 2008), that rates of self-harm among young people are increasing (Fortune & Hawton, 2005) and that treatments have met with only partial success (Low et al., 2001), focusing on prevention rather than cure (Best, 2006) through assessing risk of self-harm may offer more favorable treatment outcomes.
When participants in the present study were assigned to one of four groups (Non clinical, Externalizers, Internalizers, and Combined internalizers/externalizers), the SHRAC differentiated risk of self-harm between them on five of the six risk factors. These findings are in line with those found in previous studies of adolescent DSH and with the limited previous findings with young children. For example, Affect (e.g., depressive like symptoms) appears to be among the strongest predictors of future self-harming behaviors in children (Pfeffer, 1997) and has been linked to self-harm in both adolescents (Gratz, 2001) and young children (Rosenthal & Rosenthal, 1984). In addition, research has demonstrated that depressive symptoms invariably precede or coexist with self-harming behaviors in young children (Harrington, Fudge, Rutter, Pickles, & Hill 1990; Kovacs, Goldstone, & Gatsonis, 1993; Rao, Weissman, Martin, & Hammond, 1993) and/or predicts its repetitive nature (Chitsabesan et al., 2003). Kirkcaldy, Eysenck, and Siefen (2004) found that the most general predictor of suicidal ideation and self-injurious behavior among a sample of 998 German adolescents aged 14- to 18-years-old was anxiety/depression. In the present study children who were Combined internalizers/externalizers recorded the highest scores on Affect, followed by Internalizers, Externalizers and children in the Non clinical group. In addition, the SHRAC was able to differentiate between children in the Externalizing group compared to those in the Combined group.
With reference to Verbalization of self-harm Pfeffer (1986) argued that for young children it does not matter whether or not a child is cognizant about the irrevocability of death, rather what is more pertinent is the fact that a child who verbalizes an intent to die is more likely to attempt this through repetitive self-harming behaviors. Although the SHRAC clearly differentiated verbalization of self-harm between children from the Non clinical group and the Combined internalizers/externalizers (the latter group recording the highest scores), there were no differences between the clinical groups.
A strong association between irrational thoughts and self-harming behaviors (i.e., Dissociation—difficulty separating reality from fantasy, hearing voices) was first posited as a risk factor almost three decades ago by Beck, Rush, Shaw, and Emery (1979). According to these authors problems begin to arise when irrational thoughts at one stage of the child’s development (assumed to be developmentally appropriate) do not dissipate but transform into more severe forms of irrationality by middle childhood (such as wanting to kill themselves over a minor incident). According to Go and Cupertino (2001) 21% of American middle school children contemplate suicide at some time. Pfeffer (1997) added to this by suggesting that as a result of a child’s impaired ability to adapt under stressful conditions he/she is more vulnerable to experiencing, among other things, thought problems, and expressions of self-harming ideation. Furthermore, if these early childhood behaviors are permitted to persist into adolescence the effects become pervasive and henceforth increase the likelihood of repeated episodes of self-harm (Hawton, Kingsbury, Steinhardt, James, & Fagg, 1999). In one of the largest studies to date, Madge et al. (2008) found that 20% of adolescent females and 10% of adolescent males had thought about harming themselves while over 70% explained their self-harm as wanting ‘to get relief from a horrible state of mind’ (70.9%). The findings of the present study support the importance of Dissociation, with children in the Combined internalizers/externalizers group recording the highest levels.
The difficulty young people have in motivating themselves (i.e., Self-directing domain) also differentiated between the groupings in the present study. Previous research with individuals who self-harm has shown them to be significantly less dynamic in their problem solving approaches and as tending to either wait for problems to solve themselves or to rely on others for solutions (Linehan, Chiles, Devine, Luffaw, & Egan, 1986; McAuliffe et al., 2006; Orbach, Bar-Joseph, & Dror, 1990). Having a negative attitude directed towards the self (i.e., Self-Appraisal domain) also differentiated between the Non clinical and Internalizers and the Combined groups in the present study.
Although Socialisation (withdrawal or preference to be alone) has been previously identified as a risk factor by several studies focusing on the early school years (e.g., Nagin & Tremblay, 2001; Renken, Egeland, Marvinney, Mangelsdorf, & Sroufe, 1989; Shaw, Lacourse, & Nagin, 2005) this was not the case in the present study. Children who are not accepted by their peers are usually described as being socially inept, emotionally labile, and at risk of having psychological problems in adolescence and adulthood (Wenar, 1994); loneliness is also commonly associated with self-harm among children (Fergusson, Woodward, & Harwood, 2000; Webb, 2002). Mothers in the present study did not observe any differences in terms of their child’s social preferences.
The findings from the present research have important implications for professionals in clinical and educational contexts. For example, although the majority of US school psychologists believe they should play a role in the prevention of all internalizing disorders, they also believe they are ill prepared to deal with major depression, eating disorders and self-injury and that these are best treated by professionals outside the school system (see Miller & Jome, 2010). These same school psychologists reported a significant gap between their training and ‘the skills they need to effectively respond to children and adolescents with internalizing disorders’ (Miller & Jome, 2010, p. 519). The present research has not only provided school psychologists with new information about risk of DSH, but also a reliable (non self-report) measure of risk of self-harm which may assist in closing the current knowledge gap they refer to.
According to Morey et al. (2008) the reported rates of DSH are likely to be the tip of the iceberg, especially given that approximately 45% of adolescents have self-harm thoughts. Moreover, it appears that many who deal with adolescents on a regular basis, such as teachers and pediatricians, underestimate the percentage of adolescents who experience DSH (see Kircaldy et al., 2004). Thus, training teachers as gatekeepers for suicide prevention and DSH, because they have the most frequent contact with young people, should be given serious consideration (Lee, Hong, & Espelage 2010). This training should also examine ways in which the barriers felt by children and adolescents that prevent them from seeking help can be eliminated in a positive medium. With appropriate training school psychologists may be the conduit to achieve this and also increase awareness of DSH and related mental health issues among educators and related professionals. In doing so those at risk of DSH might be identified earlier so that appropriate support can be arranged (Ystgaard et al., 2009).
In conclusion, DSH is an international problem of a significant magnitude. By focusing on risk of DSH this current research has responded to Low et al. (2001) and Best (2006) respectively, who highlighted that as treatments have not been particularly successful in reducing repetition of DSH, a ‘prevention is better than cure’ (p. 173) approach may be warranted. The challenge now is to use the information generated to develop and evaluate preventive treatments so that DSH might be reduced in the adolescent years.