
Abstract
A group of 124 children orphaned by AIDS (COA), who resided in two orphanages funded by the Chinese government, participated in a study investigating the efficacy of a grief-processing-based psychological group intervention. This psychological intervention program was designed to specifically help COA process their grief and reduce their psychological distress. Six sessions of group intervention focused on processing grief, reducing traumatic symptoms and psychological distress, and fostering hope about the future. At the three-month post-test, children in both groups (intervention group and control group) reported significant reduction in trauma symptoms and demonstrated similar levels of hope. However, the intervention group reported significantly increased levels of grief processing and decreased levels of trauma symptoms, depression, and threat appraisal. The intervention group also reported subjective improvements in mood, relationships, individual growth, self-confidence, and perceived social support. These outcomes supported the potential efficacy of grief-processing-based psychological intervention to reduce the psychological distress among COA.
Keywords
In 2005, more than 15 million children less than 18 years of age worldwide were orphaned by parent deaths due to Acquired Immune Deficiency Syndrome (AIDS). In 2010, this number increased to 25 million, with projected totals reaching 40 million by 2020 (UNICEF, 2009). In China, an estimated 100,000 children were orphaned by AIDS, with the majority of these children living in rural and central China (Hong et al., 2011).
Children’s grief
Recently a growing international body of literature has focused specifically on the reaction of children following traumatic events, including natural disasters (Evans & Oehler-Stinnett, 2006; Zeng & Silverstein, 2011), the horrors of war and ethnic cleansing (Layne et al., 2008), and death and disruption in the wake of disease epidemics such as AIDS (Cluver, Gardner, & Operario, 2007, 2008, 2009). Among all traumatic events, losing one or both parents during childhood was one of the most traumatic events and might lead to disrupted attachment, emotional insecurity, and even loss of food, shelter, and protection (Bowlby, 1980; Haine, Ayers, Sandler, & Wolchik, 2008).
Grief is a common reaction of children following the death of a parent. Children’s grief reactions range on a continuum in terms of severity, including a set of emotional, cognitive, behavioral, and physical reactions (Bruce & Perry, 2001; Worden, 1996). The primary emotional reaction of children after losing a beloved parent was fear, and children suffered more emotional pain than adults because of children’s limited ability to verbalize their grief and the tendency to avoid facing grief by resorting to denial (LeVieux, 1993). Children who have experienced the death of a parent have more internalizing and externalizing problems on the Child Behavior Checklist and have elevated scores on the Grief Checklist (Spuij, Londen-huiberts, & Boelen, 2013). Over time, children’s thoughts may be dominated by feelings of loss and sadness, however, some children avoid talking about losing their loved one (Bruce, 2001).
Grief in children orphaned by AIDS (COA)
The death of a parent is particularly painful for children. Kinai (2008) reported that approximately 80% of children orphaned by AIDS (COA) continued to grieve their parent’s death across time, even years later. Grief of COA might accumulate by experiencing multiple losses such as the loss of both parents, siblings, and other relatives (Family Health International [FHI], 2003; Nyamukapa et al., 2008). In comparison with children orphaned in other ways, the grief of COA might be especially complicated due to the stigma associated with AIDS (Wood, Chase, & Aggleton, 2006). AIDS-related death was often stigmatized as a ‘bad’ death and linked with shameful-sex and moral depravity (Posel, 2004). Grief that was complicated by such social stigma was often referred to as ‘disenfranchised grief’ (Balk, Zaengle, & Corr, 2011; Kinai, 2008).
COA might also need to take on multiple caregiving roles, including self-care, taking care of family members, which might disrupt household routines, shift traditional family roles, and negatively influence children’s schooling (Zhang et al., 2009). Furthermore, many COA were also confronted with increasing economic hardship, depriving them of even basic survival necessities such as food and shelter (He & Ji, 2007; Zhao et al., 2007). Consequently, such COA had no chance or ability to process their grief (Lin, 2007).
With the unprocessed grief, COA suffered various psychological problems. Previous studies consistently reported that AIDS orphans had higher rates of post-traumatic stress disorder (PTSD) and other psychological problems such as anxiety, anger, and depression (Atwine, Cantor-Graae, & Bajunirwe, 2005; Nyamukapa et al., 2008). Research documented that AIDS orphans suffered from feelings of sadness, depression, fear, loneliness, low self-esteem, social withdrawal, and feelings of hatred. They also were more likely to have sleep problems, lowered future expectations, decreased hope for the future, and limited sense of control over their future (Fang et al., 2009; He et al., 2007; Zhao et al., 2009). In comparison with children orphaned by other causes and non-orphaned children, COA in South Africa were more likely to report symptoms of depression, peer relationship problems, post-traumatic stress, delinquency, and conduct problems (Cluver, Gardner, & Operario, 2007). Moreover, COA reported a heightened sense of desperation, evidenced by increased reports of suicidal ideation and plans to attempt suicide (Atwine et al., 2005; Cluver et al., 2007; Zhao et al., 2007).
The grief process of children could be further hindered by the cultural taboos of death in certain cultures. In some societies, children were not usually permitted to get close to a dead body or to attend funerals (Wood et al., 2006). In Chinese culture, individuals were taught to control emotions such as grief from childhood (Tseng & Wu, 1985). A study documented that although all COA felt depressed and repressed grief after their parents died, 37% said that what they could do was to ‘keep it inside,’ 35% said they did not want to tell anybody, and 16% said they did not know whom to tell; only 4% of these orphans talked about their feelings with others (Xu, Wang, Ji, & He, 2006). Moreover, children were criticized as ‘good-for-nothing’ when they cried and expressed comments such as missing their parents. Children were asked to focus more on learning how to hide and ignore their feelings. Consequently, many children avoided processing their grief. However, after going to bed at night, many children found it difficult to fall asleep. Instead, they cried silently or covered their head with a quilt to muffle their whimpering (Zhao et al., 2009).
Previous studies noted that children who suffered from grief need to talk about their feelings, to have someone to listen to them, and to learn adaptive strategies to mourn, accept, and cope with their losses (Kinai, 2008; Webb, 2011). Previous studies also suggest that psychological intervention could effectively decrease the psychological distress among COA (Kumakech, Cantor-Graae, Maling, & Bajunirwe, 2009; Lee, Deteis, Rotheram-Borus, & Duan, 2007). In particular, psychological intervention with COA utilizing peer group support has the potential to significantly decrease the children’s depression, anger, and anxiety (Kumakech et al., 2009). Building social support systems for these children could also effectively prevent mental health problems and behavior problems in COA (Lee et al., 2007). Lastly, family economic intervention might also be effective in decreasing high-risk behaviors in COA (Ssewamala, Alicea, Bannon, & Ismayilova, 2008).
Although COA experienced great grief and other psychological distress, very limited psychological intervention driven by grief theory has been provided to this group, and there were even fewer studies evaluating the efficacy of grief-processing-based psychological intervention among this population (Siegel & Gorey, 1994; Zhao et al., 2007). A report assessing the need for support and intervention for bereaved children noted that children should be involved in each of the five stages, including pre-death, death occurrence, immediate aftermath, short-term stage, and long-term stage. Children should be taught the meaning of death prior to the death of their loved one, should be present at the funeral, informed and supported when the death occurs should be understood and supported in expressing their grief immediately after the parent’s death, and should be provided opportunities to express grief in the five stages (Dowdney, 2008). According to the studies mentioned above, the current study designed a grief-processing-based psychological intervention program and examined whether it could effectively facilitate the grief processing of COA and decrease their psychological distress.
Method
Study site
The current study was conducted in 2007–2008 in two AIDS orphanages in central China. These two orphanages were established by the Chinese government for children whose father and mother were both deceased due to AIDS-related illness. Many adults in this specific area of China were infected with HIV through unsanitary blood collection, resulting in numerous deaths caused by AIDS.
Participants
In total, 124 COA from two orphanages were initially considered potential participants. Of the 91 children in the first orphanage, 64 were recruited into the intervention group. Of those who did not participate, eight children left to attend a boarding school, 15 returned to their home, and four remained ill. This intervention group consisted of 38 boys and 26 girls, with an age range of 11- to 17-years-old and a mean age of 13.69 ± 1.22 years. Among these orphans, their fathers had died 4.95 ± 4.17 years ago and their mothers had died 4.7 ± 4.17 years ago. The number of siblings was 1.08 ± 1.17 in the intervention group.
Of the 73 children in the second orphanage, 60 were recruited to the control group. Of those who did not participate, ten children returned to their home and three were ill. This control group consisted of 38 boys and 22 girls, with an age range of 9- to 16-years-old and a mean age of 13.46 ± 1.57 years. Among these orphans, their fathers had died 5.68 ± 2.84 years ago and their mothers had died 5.20 ± 2.24 years ago. The number of siblings was 1.36 ± 1.35 in the control group.
Demographics of COA in the intervention and control groups.
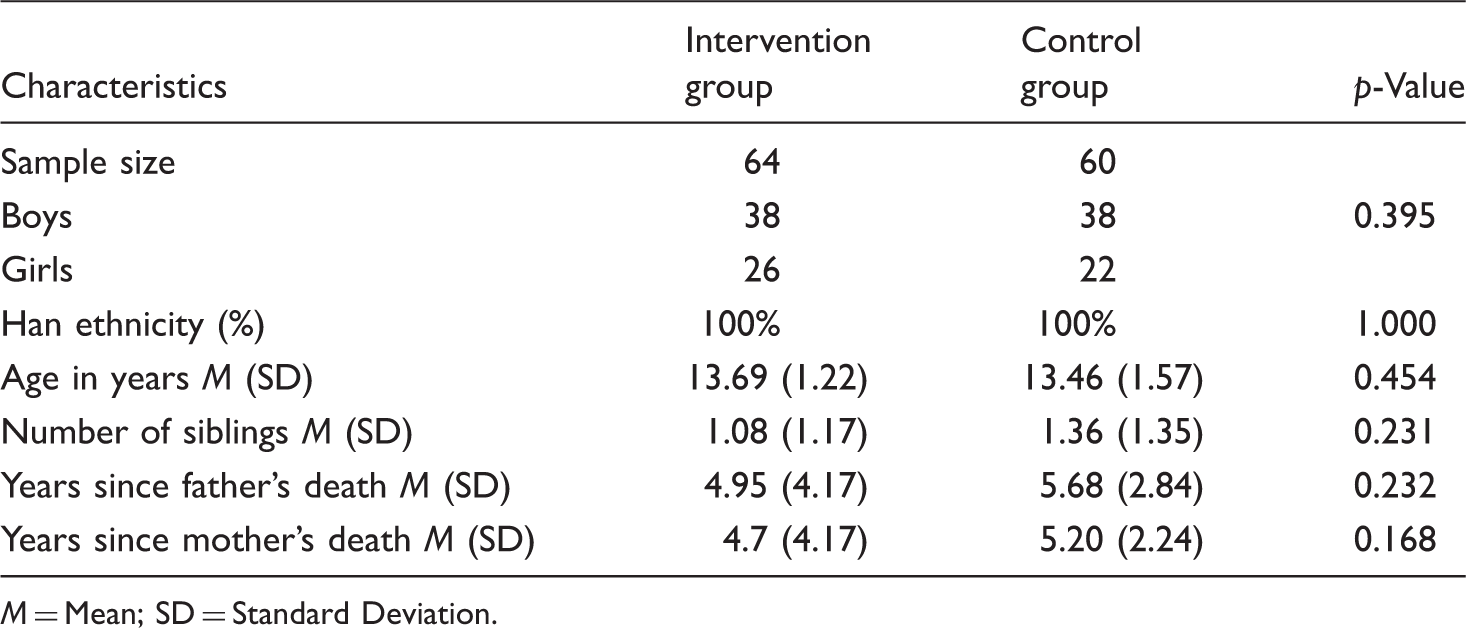
M = Mean; SD = Standard Deviation.
At the three-month post-test, the attrition rate was 5.6 %. This attrition occurred because seven children (all from the control group) left the orphanage and returned to live with family members.
Study design
This study employed a comparison design between an intervention group and a control group. One orphanage (64 participants) served as the intervention group and the other (60 participants) as the control group. This type of arrangement avoided contamination between the intervention and control groups and increased the feasibility of conducting psychological intervention. These two orphanages were located at the end of the town in one county about five kilometers apart. Each of the orphanages was built by the local government for AIDS orphans who lost both parents, and the government provided approximately equal education and life level support to them. Thus the two orphanages have similar economic level, culture, and care for children. More over, all the orphans in these two orphanages are from the same local county.
Children in the intervention group were randomly divided into four groups with each group size ranging from 15 to 18 children (mixed gender and age). Pre-test and the three-month post-test were implemented for both the intervention and control groups. The pre-test was completed in October 2007, the psychological intervention was delivered in November and December 2007, and a three-month post-test conducted in February 2008.
The psychological intervention
The psychological intervention curriculum, based on grief theory and grief of COA, was designed by three family therapists. All three family therapists had doctoral degrees and had conducted interviews, data collection, and counseling of COA in a project regarding bereavement of children orphaned by AIDS for more than three years prior to developing this intervention curriculum. Considering COA’s internalizing and externalizing problems, the six-session psychological intervention was designed from the perspective of how to process grief (including expressing grief, drawing a family picture, writing a letter to parents, commemorating parents in their own way, saying farewell to parents, etc.), cope with stress and discrimination, manage emotions, perceive support, love oneself, and increase hope for the future.
Six weekly sessions (1.5–2.0 hours per session) were delivered by the first author and a trained postgraduate student with a degree in family therapy. The psychological intervention consisted of several group activities, and each session was started with a warm-up activity and ended with a hug to each participant. During each session, children were encouraged to share and discuss topics of grief through well-designed games or activities. They were encouraged to discuss individual doubts about death or bereavement and support each other during the intervention.
Evaluation and survey procedure
Demographic information, grief, trauma symptoms, depression, cognitive appraisal, and future orientation were included in the pre-test. All scales were self-administered by the children who could read and write in Mandarin. For children who were in the third grade and younger, and for those children with limited reading abilities (nine out of 124 children), researchers read each question aloud and recorded the child’s responses. During the survey, necessary clarification or instruction was provided promptly when needed.
Each participating child was administered an assessment inventory, including demographic information and several scales. As a token of appreciation, each child received a gift worth 20 RMB (equal to 3 USD) after completing the assessment.
Ethical consideration
COA and their caregivers or guardians signed informed consent forms before participation. Each of them received an information sheet with a detailed description of the study design and potential benefits and risks (including confidentiality issues) to facilitate an informed decision concerning whether to participate. The research protocol, including the consent procedure, was approved by the Institutional Review Board of Beijing Normal University, China.
Measures
Demographic characteristics
COA were asked to report on individual and family characteristics including age, gender, ethnicity, number of siblings in the family, and number of years since their father and mother had died.
Grief Processing and Deliberate Grief Avoidance (GPDGA)
A total of 20 items were divided into two dimensions: Grief processing (13 items) and deliberate grief avoidance (seven items). The grief processing dimension included five behaviors: Thinking about the deceased, searching for meaning, having positive memories of the deceased, talking about the deceased, and expressing feelings about the deceased. The deliberate grief avoidance dimension included three behaviors: Avoiding thinking about the deceased, avoiding talking about the deceased, and avoiding expressing feelings about the deceased. The frequency of these behaviors was assessed on a five-point Likert scale (1 = almost never to 5 = almost always). A higher score in grief processing indicated more processing, and a higher score in deliberate grief avoidance indicated more avoidance. Each behavior was considered in two different scenarios: With family members and with friends. Additionally, four behaviors (three grief processing behaviors and one deliberate grief avoidance behavior) were considered when individuals were alone (Bonanno, Papa, & Zhang, 2005).
Based on preliminary results (Zhang et al., 2009), another scenario was added to this study; that was, grief processing and deliberate grief avoidance of COA in the company of other important people such as a school principal, caregivers, roommates, and other supporters. These individuals were especially important to COA due to the extensive time and contact spent in orphanages and schools. By adding this scenario, five grief processing items and three deliberate grief avoidance items were added to the scale. The Cronbach’s alpha of these two dimensions for the current sample was 0.92 and 0.87, respectively.
Trauma Symptom Checklist for Children (TSCC)
The TSCC was used to assess the traumatic symptoms of children in this study (Briere, 1996). Fifty-four items were divided into two validity subscales and six clinical subscales. The validity scale was divided into two subscales: Under-response (UND) and hyper-response (HYP). The clinical scale was divided into six subscales: Anxiety, feelings of depression, anger, post-traumatic stress, dissociation, and sexual concerns. All items were presented on a four-point scale (1 = never to 4 = almost all of the time). Considering that sexual knowledge was proportionally limited in this rural area, this study deleted ten items regarding sexual concerns. The Cronbach’s alpha of the six clinical subscales ranged from 0.66 to 0.85 in the current study.
Depression
Children’s depressive symptoms were measured using the Center for Epidemiologic Studies Depression Scale for Children (CES-DC) (Fendrich, Weissman, & Warner, 1990). The scale has 20 items including six major symptoms of depression: Mood, feelings of guilt/worthlessness, feelings of helplessness/hopelessness, psychomotor retardation, loss of appetite, and sleep disturbance. Each item was measured on a four-point scale (1 = no to 4 = always). The Cronbach’s alpha for this scale in the current study was 0.81.
Appraisal Questionnaire (AQ)
A modified version of the AQ was employed to assess the children’s appraisal of threat, challenge, and controllability (Pakenham & Rinaldis, 2001). Five threat appraisal items were rated on a five-point scale (1 = no harm to 5 = extremely harmful) to indicate the extent to which HIV-related problems had the potential to harm areas including important life goals and self-respect. Three challenge appraisal items were rated on a five-point scale (1 = nil potential to 5 = high potential) indicating the extent to which HIV-related problems provided potential for personal growth and challenge. Controllability was measured by two items, and participants rated on a five-point scale the extent to which 1) the problem could be changed, and 2) must be accepted or adjusted to. The Cronbach’s alpha for the threat and challenge subscales were 0.77 and 0.60, respectively.
Future orientation
Future orientation was measured by the children’s future expectation scale (Bryan, Rocheleau, Robbins, & Hutchison, 2005), hopefulness about the future scale (Whitaker, Miller, & Clark, 2000), and perceived control over the future scale (Whitaker et al., 2000). The children’s future expectation scale included six items regarding the children’s assessment of the future. A five-point scale was used to measure the results (1 = completely not sure to 5 = extremely sure). The hopefulness about the future scale consisted of four items to assess the child’s hopefulness toward the future. A four-point scale was used to measure the results (1 = definitely not to 4 = definitely yes). The perceived control over the future scale contained seven items. A four-point scale was used to mark the results (1 = strongly disagree to 4 = strongly agree). The Cronbach’s alpha for these scales were 0.84, 0.78, and 0.64 respectively, in the current study.
Subjective perception of psychological intervention effectiveness
A total of 11 items were designed to assess the effectiveness of the psychological intervention that COA received in the intervention group. Four items examined change in emotion, relationships, self-esteem, and academic performance before and after psychological intervention. Each of these items was measured on a five-point scale (1 = much worse to 5 = much better). Six items assessed the children’s perceived benefits, including individual growth, establishment of self-confidence, hope toward future orientation, overcoming difficulties, grief processing, and perceived support from attending psychological intervention. Each was measured on a four-point scale (1 = not helpful to 4 = very helpful). The last item concerning participants’ willingness to participate in similar activities in the future was assessed on a two-point scale (1 = no or 2 = yes).
The above English scales were first translated into Chinese and then back-translated into English. Chinese language habits were considered, the subsequent adjustments were made, and the age range was extended to be applicable to 6- to 18-year-olds.
Data analysis
First, descriptive statistics were used to compute the Means, Standard Deviations, and ranges for demographic data of both the intervention and control groups. Second, comparison was made through Analysis of Variance (ANOVA) between the intervention and control groups in the pre-test, also between age group and gender. Third, a series of paired-sample t-tests were conducted to compare the results from the pre-test and the post-test. This study further used ANOVAs to compare scores of the post-test in the intervention and control groups. Finally, a descriptive analysis was used to analyse the subjective appraisal items.
Results
GPDGA and psychological distress at pre-test and post-test tests
Comparison of grief processing and psychological distress scores at pre-test and post-test for COA in the intervention and control groups.
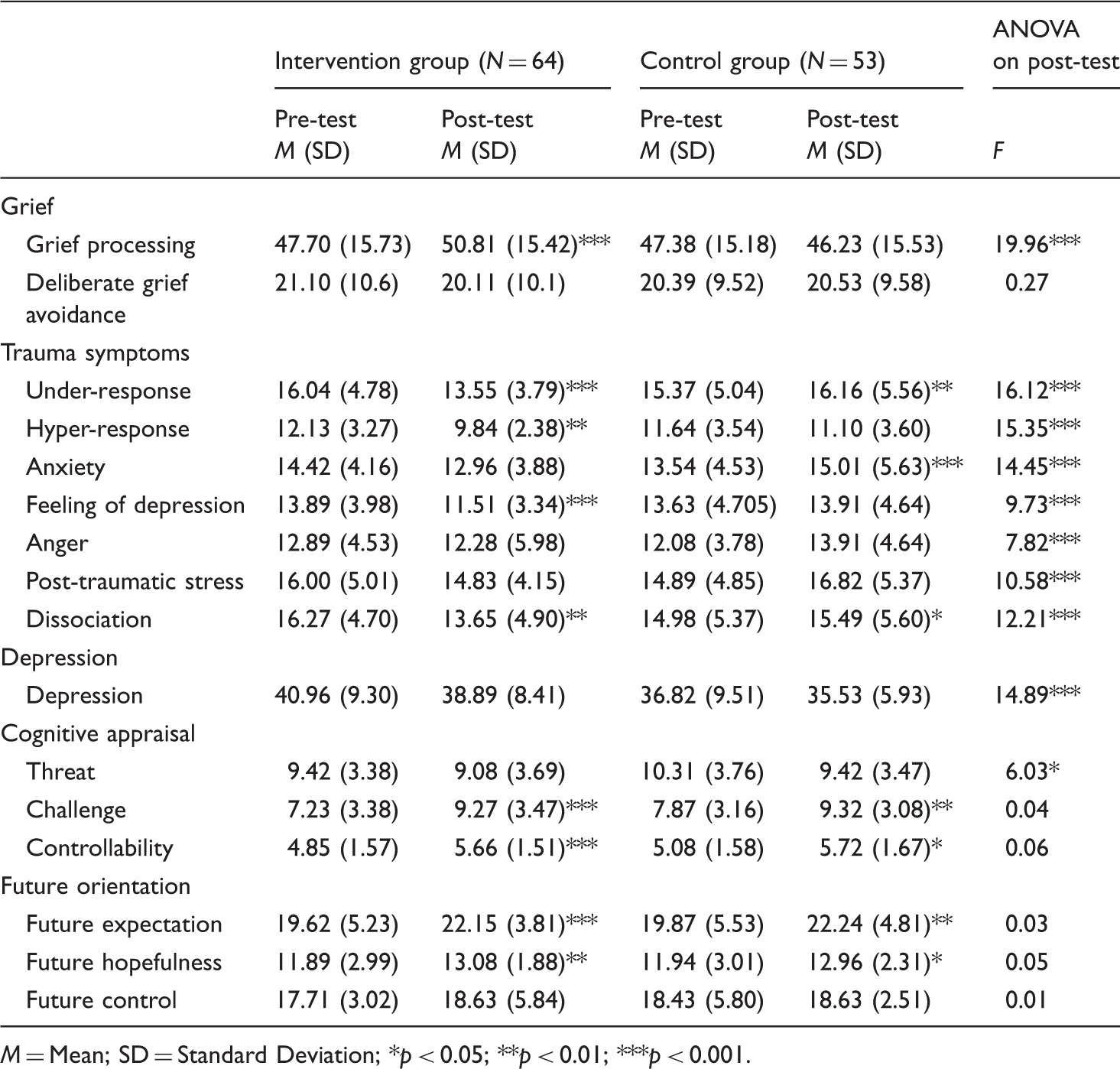
M = Mean; SD = Standard Deviation; *p < 0.05; **p < 0.01; ***p < 0.001.
From the pre-test to post-test, the intervention group experienced significant increased in grief processing (p < 0.001), challenges (p < 0.001), controllability (p < 0.001), future expectations (p < 0.001), and hopefulness (p < 0.01) and decreased in under-response (p < 0.001), hyper-response (p < 0.01), feelings of depression (p < 0.001), and dissociation (p < 0.01).
At post-test, the control group experienced significant increases in under-response (p < 0.01), anxiety (p < 0.001), dissociation (p < 0.05), challenges (p < 0.01), controllability (p < 0.05), future expectations (p < 0.01), and hopefulness (p < 0.05).
Compared to the control group, the intervention group scored significantly higher for grief processing (p < 0.001) and significantly lower on all of the trauma symptom subscales (p < 0.001) and threat (p < 0.05) in the post-test.
Furthermore, age group ( ≥ 13 vs 12≤) and gender difference in variables in both intervention group and control group were analysed using ANOVA in the pre-test and post-test, however, there were no significant differences between the age groups and gender groups. Refer to Table 2 for the specifics related to these analyses.
Changes in the intervention group in subjective appraisal items
Subjective appraisal items concerning changes in the intervention group.
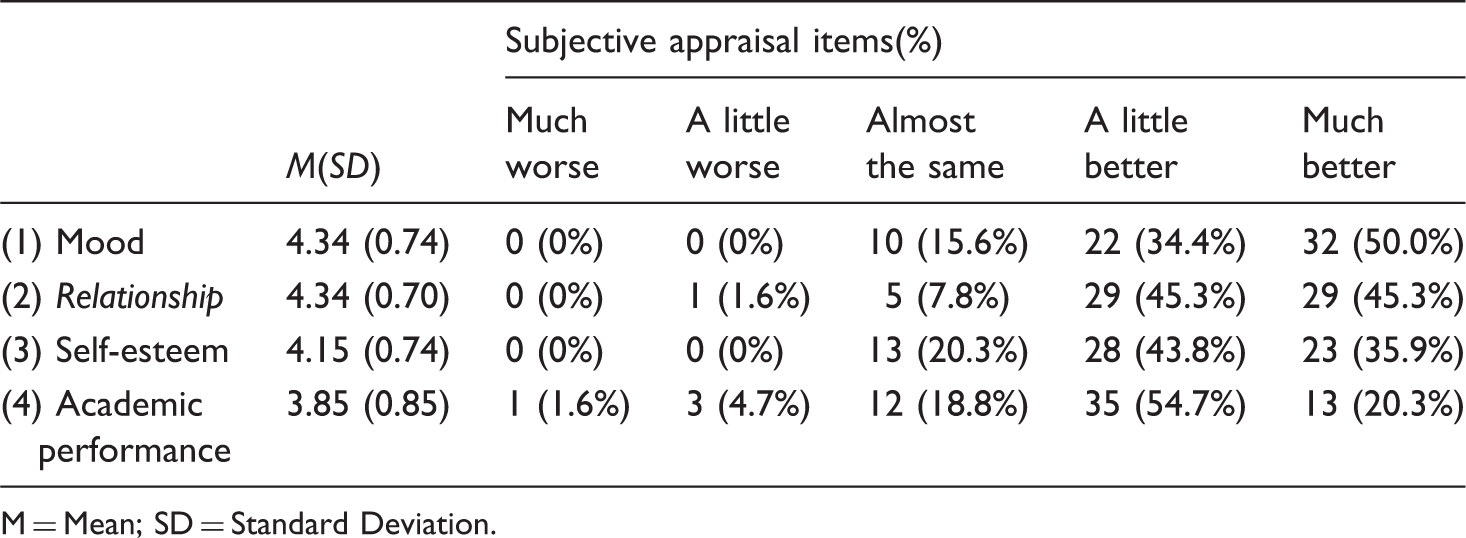
M = Mean; SD = Standard Deviation.
Psychological intervention effectiveness on subjective appraisal items
Subjective appraisal of the effectiveness of psychological intervention.
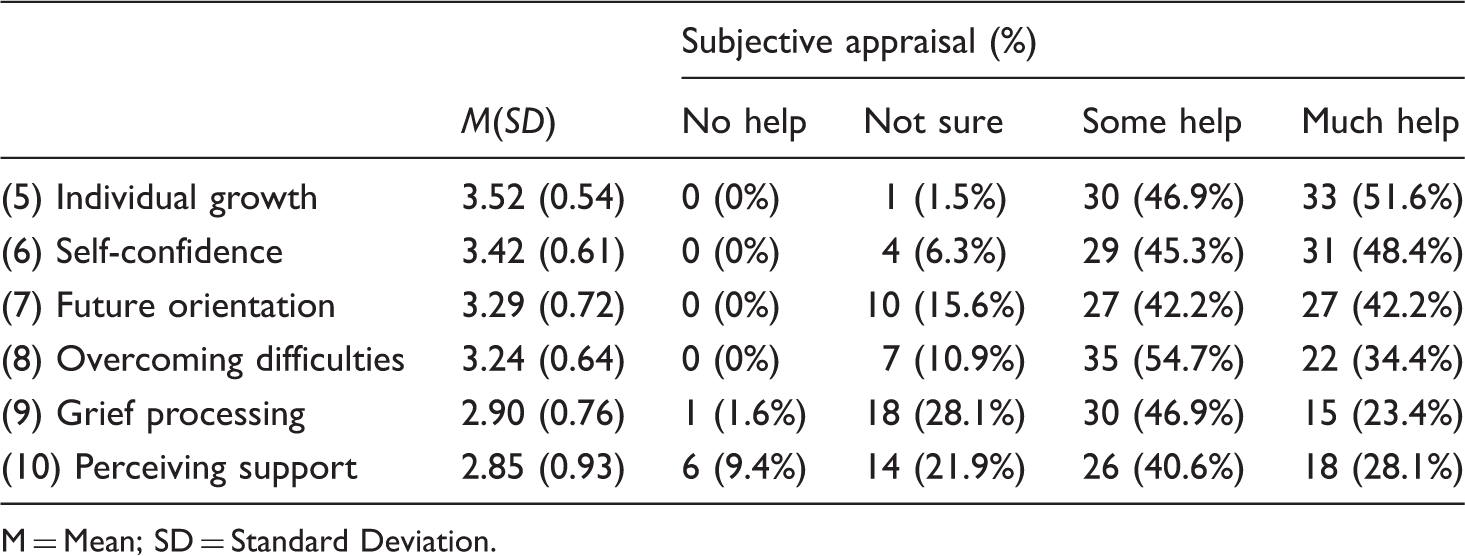
M = Mean; SD = Standard Deviation.
For the last question, 52 (98.1%) of the COA in the intervention group chose ‘Yes’ in response to ‘Are you willing to participate in similar activities in the future?’. This response demonstrates that they expressed their willingness to attend similar activities in the future.
Discussion
The psychological intervention based on grief processing contributed to the grief processing and psychological distress reduction in COA. After controlling for the differences in depression levels on the pre-test between the intervention and control groups, the intervention group showed a significant increase in grief processing and significant decrease in both trauma symptoms and the threat of cognitive appraisal at the three-month post-test. This finding showed that grief-processing-based psychological intervention played an important role in COA’s ability to effectively process grief, reduce trauma symptoms, and feel hopeful about the future. The psychological intervention also greatly improved mood, relationships, self-esteem, and academic performance and helped with individual growth, building self-confidence, overcoming difficulties, and perceiving support. Considering that 98% of the participants expressed their willingness to continue to participate in such psychological intervention, participants acknowledge the effectiveness of such intervention.
Grief-processing-based psychological intervention focusing on the last stage of grief processing provided an opportunity for COA to express their suppressed grief and depressed emotion (Dowdney, 2008). During the psychological intervention, COA commemorated their deceased parents by drawing a family picture, writing letters to parents, and remembering what parents had done for them. Taking part in the psychological intervention, COA could still feel the love from parents. Furthermore, COA who attended the psychological intervention did not feel alone any more after knowing that almost all of them suffered from the pain of losing parents by sharing their grief in the group (Webb, 2011). After finishing the psychological intervention, COA could talk about their parents’ ‘secret’ with their peers, and they could help and support each other to process the grief (Dowdney, 2008). Taking part in psychological intervention also allowed the COA to learn how to address problems by themselves and to perceive support from others (Kumakech et al., 2009). Thus, COA who received the psychological intervention had significantly decreased trauma symptoms and more hope about the future.
Moreover, according to reports from orphanage leaders and teachers, these children were much more outgoing and adept at expressing themselves to others after psychological group interventions. Rather than suppressing their feelings, they were more open about sharing their emotions with others and actively reaching out to others to assist them in expressing their feelings.
However, during the post-test, the intervention group showed no decrease in deliberate grief avoidance. This insignificant change might be due to the impact of traditional culture (Jerome, 2011). Generally, Chinese culture does not encourage the open expression of grief and only approves of the expression of grief in ritualized ways (Tomori, 2000). Thus when expressing their grief in ways not recognized by Chinese culture, children were encouraged to study hard and do well in their studies as the best way to commemorate their parents (Lin, 2007).
Although the COA in the control group did not receive any psychological intervention, their psychological distress was reduced and their cognitive appraisal and hopefulness toward the future improved. This result might be due to an improvement in their life condition. However, improvement in the control group was not noticeable across all study variables but was randomly distributed in a few areas of psychological distress.
Conclusions and limitations
This pilot study contributes to demonstrating the effectiveness of grief-processing programs in COA by following intervention and control groups longitudinally. Our findings provide strong support for increasing COA’s grief processing and hopefulness toward the future and for reducing their psychological distress. Hopefully, we speculate that this grief-processing-based psychological intervention might benefit children who are orphaned in other ways and who have difficulty in expressing grief.
Several limitations of the current study should be considered. First, children were not randomly assigned to the intervention or control groups. Second, the post-test was conducted only three months after the psychological intervention, and hence, long-term effects of psychological intervention need further examination. Third, participants were all selected from two orphanages in central China, and the findings may not be generalizable to other locations and cultures.
Implications for school psychologists
The majority of children who grieve do not know how to cope with the strong feelings associated with their loss, nor do they have the resources and the wherewithal to seek counseling on their own. Noting children’s needs, school psychologists must be prepared to help children whose parents are deceased. Noting the underlying root of unresolved grief, professionals must monitor children’s behaviors, such as school drop-out, high absenteeism, withdrawal from social interactions and friendships, angry outbursts, decrease in academic achievement (lower grades), depression and anxiety, etc. School psychologists must be able to identify students who are struggling. Interventions must be offered in order to address these students’ underlying needs at the earliest opportunity.
Considering supportive activities, students typically enjoy engaging in game playing, drawing family pictures, writing a letters to their deceased parent, and saying their farewells to their parents (helping provide a sense of closure). Particularly, for children who have limited language ability, verbalizing their painful grief may be more challenging. Therefore providing activities may be a strategy to help these children deal with their grief (LeVieux, 1993).
No matter which coping skills we rely upon when dealing with grief, the most important strategies school psychologists can provide are a series of opportunities to address grief. Additionally, school psychologists must assure children that these strong feelings are typical for all of us, and are particularly painful when associated with a parent’s death. When children feel sadness and pain, it is important to talk about memories the loved one. Children need to know that caring adults are available to answer questions and to provide emotional support.
Negotiating the trials of life is especially challenging for children whose parents are deceased, particularly when their parents die from a disease with negative connotations, such as HIV/AIDS. This research highlights the importance of offering children opportunities to process their grief. Rather than avoiding emotional topics and focusing solely on academic learning, schools must provide more activities that promote grief processing efforts. These opportunities are critical in promoting children’s expressions of bereavement and encouraging their processing of grief. By providing a safe place to talk about death and grief, the experience of bereavement can be normalized across time and decrease many of the negative outcomes related to unresolved grief (Tomori, 2000).
Footnotes
Acknowledgements
The study described in this report was supported by the AIDS Prevention Work Council Grant 05-III-3 from the State Department of China. The authors of this article extend their thanks and appreciation to the principals, caregivers, and teachers of the two orphanages. The authors would like to take this opportunity to especially extend their thanks and appreciation to the children who shared their feelings and experiences related to their grief.