
Abstract
Psychologists in schools can play an important role in developing policies and programs to promote healthy eating habits. This study analyses the contributions of family socioeconomic status, peer influence (schoolmates’ food consumption), and school-based nutrition interventions to explain adolescent eating behaviors. Data were obtained from the 2014 Health behaviour in school-aged children survey in Spain, with a sample of 6,851 adolescents (11- to 16-years-old). The results suggest that school-based healthy-eating programs could improve by considering parental education level and by implementing interventions focused on the peer social network. Policies that limit access to unhealthy products in schools – rather than simply offering healthy foods alongside unhealthy products – could be more effective.
Background
Adolescence is a critical developmental stage in which rapid physical growth increases the body’s demand for energy and nutrients (Awnetwant & Jackson, 2014). An inadequate intake of fruits and vegetables, and a frequent consumption of drinks or food with high sugar content, have been related to a wide range of illnesses such as high blood pressure, cerebrovascular and cardiovascular diseases, cancer, osteoporosis, caries, iron-deficiency anemia or a lower resistance to infections (WHO, 2003a). In addition, healthy eating behaviors established during adolescence continue into adulthood (Lien, Lytle, & Klepp, 2001; Williams, Holmbeck, & Greenley, 2002) and therefore have long-term benefits (Woodward, Oliphant, Lowe, & Tunstall-Pedoe, 2003) such as preventing chronic diseases (WHO, 2003a), including obesity, currently one of the most worrying and frequent diseases during adolescence (Niemeier, Raynor, Lloyd-Richardson, Rogers, & Wing, 2006; Schröder et al., 2014).
Likewise, given the body’s sensitivity to variations in the availability of nutrients, metabolic changes occur when fasting is prolonged more than normal, leading to fatigue that not only interferes with physical and muscular performances, but also in different cognitive aspects such as lack of concentration, diminished capabilities in speech, expression, memory, creativity and problem solving, besides psychosocial issues and moodiness (Hill, 1995; Rampersaud, Pereira, Girard, Adams, & Metzl, 2005). In this sense, it has been proven that skipping breakfast is much more habitual than skipping lunch or dinner (Woodruff, Hanning, Lambraki, Storey, & McCargas, 2008). Additionally, skipping breakfast has been related to an increase in consumption of high caloric food later during the day, as well as obesity among adolescents (Bauer, Larson, Nelson, Story, & Neumark-Sztainer, 2009; Elgar, Roberts, Moore, & Tudor-Smith, 2005).
International agencies recommend three or more servings of fruit a day and only a moderate and occasional consumption of candy and soft drinks (WHO, 2003b). However, only a small percentage of adolescents follow these recommendations. As adolescents get older they tend to reduce their frequency of breakfast (Affenito, 2007; Niemeier et al., 2006), fruit, and vegetable consumption (Diethelm et al., 2012; Taut et al., 2015), while simultaneously increasing their intake of high-caloric food, such as energy-dense snacks, candy (Diethelm et al., 2012; Piernas & Popkin, 2010; Taut et al., 2015), and soft drinks (Fismen, Samdal, & Torsheim, 2012; Lien et al., 2001; Vereecken, Inchley, Subramanian, Hublet, & Maes, 2005).
Further complicating these matters, a severe economic recession has impacted the European Union since 2008. The WHO has highlight the highest vulnerability of developed countries, especially those who have required assistance form the International Monetary Fund, as is the case of Spain (WHO, 2009). Therefore, besides an increase in unemployment rates and financial insecurity, the WHO has warned of the negative consequences for health and lifestyles due to an increase in food and fuel prices. Specifically, FAO’s 2009 State of Food Insecurity (SOFI) (FAO, 2009) highlighted how an economic crisis results in socioeconomically disadvantaged people reducing spending on education and healthcare, the amount of food consumed, and dietary diversity, in addition to increasing consumption of less expensive foods which are often lower in nutritional value. This may result in child and adolescent poverty as well as an increase in malnutrition in this population, as UNICEF (Fanjul, 2014) points out.
Despite finding a less-robust relationship between socioeconomic factors and lifestyles during adolescence than in adulthood (Hanson & Chen, 2007), results regarding nutritional habits tend to be more consistent than those for others health-related outcomes. Specifically, significant associations have been found between the family material affluence and the consumption of breakfast, fruit, vegetables, and candy (Lazzeri et al., 2016; Yannakoulia et al., 2016; Zaborskis, Lagunaite, Busha, & Lubiene, 2012). In addition, a previous Health behaviour in school-aged children (HBSC) study showed fruit consumption increasing with both family material wealth and higher parental occupational status in 28 countries, whereas the association between those indicators with soft drinks consumption was not consistent across groups (Vereecken et al., 2005). Moreover, another study showed family affluence being a significant predictor of daily fruit and vegetables consumption and breakfast intake, and cultural capital, assessed by the number of books in the household, having an independent and a strong contribution to healthy eating among adolescents (Fismen et al., 2012). Along these lines, parental education seems to play an important role in the adoption of healthier behaviors. For example, a relationship has been demonstrated between parental education level and adolescents’ fruit and vegetables consumption (Rasmussen et al., 2006), soft drink intake (Totland et al., 2013) and being overweight (Koivusilta, Rimpela, & Kautiainen, 2006). However, different socioeconomic indicators have shown to have different impact on adolescents’ nutritional habits.
In addition, children’s eating behaviors are affected by socioeconomic factors through food-related parenting practices in the home (Hanson, Neumark-Sztainer, Eisenberg, Story, & Wall, 2005; Mak et al., 2013; Vereecken, Rovner, & Maes, 2010). For example, economically disadvantaged parents are less likely to buy healthy foods (Turrell, Hewitt, Patterson, & Oldenburg, 2003), and present fewer healthy dietary-behaviors (Galobardes, Morabia, & Bernstein, 2001; Giskes et al., 2009).
While socioeconomic status explains some of the variance in eating behaviors, adolescence marks a time of increased independence (Lytle & Kubik, 2003) with important implications regarding food choices (Niemeier et al., 2006). Children’s eating behaviors are increasingly affected by their school environment and their peers as they mature (Story, Neumark-Sztainer, & French, 2002; Williams et al., 2002). Social networks can negatively affect adolescent eating behaviors (Fletcher, Bonell, & Sorhaindo, 2011; Sawka, McCormack, Nettel-Aguirre, & Swanson, 2015). However, findings reported by the TEMPEST study, a European research project, showed an association between peer encouragement of healthy eating and consumption of healthy food in adolescents from 10- to 17-years-old (Stok, De Vet, De Wit, Luszczynska, Safron, & De Ridder, 2015). In a review of recent literature (Stok, De Vet, De Ridder, & De Wit, 2016), the authors identified the influential reference groups for adolescent eating behaviors and the types of food more likely to be influenced by social norms. For example, whereas for boys, popularity in school has been associated with increased consumption of high-calorie foods (De La Haye, Robins, Mohr, & Wilson, 2010), girls are more sensitive to social pressure regarding dieting and eating disorders (Lieberman, Gauvin, Bukowski, & White, 2001; Mackey & La Greca, 2007; Shroff & Thompson, 2006). Regarding age, Stok et al. (2016) showed that the influence of peers in eating habits may be developed in early adolescence, increasing during adolescence and early adulthood but decreasing during adulthood. In addition, Lieberman et al. (2001) also showed differences in how girls are influenced by their peers in dieting and disordered eating, specifically that girls with an earlier average age of menarche are more vulnerable to the influence of their peers. Regarding the role of school in moderating the influence of peers on eating habits, some differences have also been found (De La Haye et al., 2010 Mackey & La Greca, 2007). However, although variables such as school socioeconomic status, availability of food products, or school policies have been proposed as factors causing this variation, results are not clear about the school variables that increase peer influence in adolescent eating behaviors.
Adolescents spend much of their day in school where they are more vulnerable to peer pressure and where most of their unhealthy eating take place (Briefel, Wilson, & Gleason, 2009). Therefore, school has been identified as the primary social context for improving eating behaviors (Arriscado, Muros, Zabala, & Dalmau, 2014; Avery, Bostock, & McCullough, 2015), and psychologists in schools can promote health in children and adolescents, as well as in their families (Nastasi, 2001). Despite the inconsistent results of research addressing the effectiveness of school programs promoting healthy behaviors (Larson, Wall, Story, & Neumark-Sztainer, 2013; Luszczynska et al., 2016), the World Health Organization in their ‘School policy framework: Implementation of the global strategy on diet, physical activity and health’ (WHO, 2008) recommends minimum nutrition standards for healthy adolescent eating behaviors in school. These guidelines include increasing availability of healthy food, subsidizing food programs for low-income families, health education for school personnel, and controlling the availability of products in vending machines.
Purpose
Given this evidence, and an increase in inequalities in Spain due to the recession (Shachmurove & Shachmurove, 2011), it is important to examine socioeconomic status and adolescent eating behaviors, as well as the role of the schools in health promotion. Furthermore, environmental and modifiable factors need to be considered to develop effective healthy-eating interventions. This research examines the contributions of different factors which influence adolescent eating behaviors: (1) age and gender, (2) family socioeconomic status, (3) influence of peer food-consumption, and (4) school-based nutrition interventions.
Methods
Data were obtained from the Health Behaviour in School-aged children (HBSC) cross-sectional survey. The HBSC study is an international alliance supported by the World Health Organization (WHO), which collects data in more than 40 countries across Europe and North America. The survey is conducted every four years with the aim of understanding young peoples’ health-related behaviors, well-being, and developmental contexts.
Study design, sample, and data collection
A representative sample of 11- to 16-year-old Spanish adolescents, who participated in the Spanish HBSC study in 2014 and who responded to all items of the variables analysed, was selected for this research. The variable with the lowest response rate was parental occupation (85.4% regarding father and 88.7% regarding mother); however, response rates for parental education level and family material affluence were above 90%, similar to the rest of the variables analysed. The sample comprised 6,851 students, with a mean age of 13.79 years (SD = 1.68) and with a balanced representation of boys and girls (46.2% boys and 53.8% girls). A total of 371 educational centers, in which the adolescents were enrolled, also participated in this study.
The survey adhered to the HBSC international coordination team’s established recommendations, referenced in the 2013/2014 international report (Inchley et al., 2016), that the questionnaire be self-completed, administered in schools under teacher supervision, with guaranteed participant anonymity.
Assessments and measures
A questionnaire designed by the HBSC that explores adolescents’ health, lifestyles, and characteristics of their developmental contexts was utilized for this study (Inchley et al., 2016). This instrument consists of a standardized questionnaire which adheres to an international protocol allowing for cross-national comparisons. An overview of the method, questionnaire content, or data collection can by found in Roberts et al. (2009). Methodological details of the HBSC study in Spain are meticulously described in Moreno et al. (2016a, 2016b). Key measures of socioeconomic level and eating behaviors, as well as gender and age items, were selected.
A complementary questionnaire (HBSC-School-level Questionnaire, SLQ), developed within the framework of the HBSC 2009/2010, was used to evaluate school characteristics (Griebler et al., 2009). The HBSC-SLQ was completed by a key informant from each participating school (a member of the board of directors or a teacher involved in health-related activities at school). Both questionnaires were approved by the University of Seville Ethics Committee, certifying compliance with fundamental ethics requirements in Spain and the EU for research on humans. Informed consent was obtained from the schools, legal guardians, and the students.
The following specific measures about eating behaviors were employed:
Children were asked about their weekly consumption of breakfast, fruit, candy, and soft drinks. Breakfast consumption was assessed by asking the respondents ‘How often do you usually have breakfast (more than a glass of milk or fruit juice)?’, with eight possible responses ranging from never to every day. The overall weekly frequency of breakfast consumption was recoded, identifying adolescents who regularly eat breakfast (1 = daily, 0 = less than daily). In the case of fruit, candy, and soft-drink consumption, the three specific questions were ‘How many times a week do you eat…?’, with the three variables fruit/candy/sugary soft drinks, including seven possible responses ranging from never to more than once a day, every day. Regular fruit consumption was identified by the responses every day and more than once a day, every day (1 = daily, 0 = less than daily). For the questions on candy/soft-drink consumption, the response categories were recoded, identifying irregular consumption by the responses never and once a week (0 = less than once a week, 1 = two or more days a week).
In research collecting dietary intake data on the individual level, questions about food frequency have demonstrated to be a useful tool for ranking individuals by food intakes, allowing groups with high and low intakes to be compared (Biró, Hulshof, Ovesen, Amorim, & Group, 2002). Therefore, breakfast and fruit consumption responses were dichotomized as: Less than daily and daily, following the recommended dietary guidelines (WHO, 2003; World Health Organization, 2006) to consider the consumption of these products as healthy patterns. For candy and soft drink consumption, the dichotomization was done identifying those at greatest risk—regular consumers— compared with adolescents who consumed these products irregularly. Since less than twice a week has been considered an acceptable consumption of these products (i.e. candy and soft drinks), these questions were dichotomized into less than twice a week and twice a week or more, as previous research have done (Bere, Glomnes, te Velde, & Klepp, 2008; Janssen, Katzmarzyk, Boyce, King, & Pickett, 2004).
Peer eating behaviors were calculated using the responses to these questions about the weekly consumption of breakfast, fruit, candy, and soft drinks. The entire sample was grouped according to school, allowing us to obtain a measure for eating behaviors of all students in every school. Following the dichotomization of responses, peer eating behaviors were calculated by the percentage of adolescents in each school that meet the criteria for daily consumption of the aforementioned products.
The following specific measures about socioeconomic status were employed in this study:
Parental education level. Assessed by the question: ‘What level of education do your father and mother have?’, classified in three levels: (0) no studies or elementary education; (1) secondary education; (3) bachelor’s degree or higher education.
Parental occupation status
Obtained by asking respondents about parental employment status at the time of the survey and, if employed, place of employment and job functions. The information was coded following the International standard classification of occupations (ISCO-08) (Wolfe, 2015). The original nine-level ISCO was recoded into three categories: High (e.g. managers, professionals; ISCO 1-3), middle (e.g. services and sales workers, skilled agricultural, forestry, and fishery workers; ISCO 4-6), and low (e.g. craft workers, plant and machine operators; ISCO 7-9). An additional category, ‘unemployed’, was included.
Family material wealth
Assessed using the Family affluence scale (FAS III). A global score was calculated as the sum of the individual item scores (Currie et al., 2008): ‘Does your family own a car, van, or truck?’ (0 = no; 1 = yes, one; 2 = yes, two or more); ‘Do you have your own bedroom for yourself?’ (0 = no; 1 = yes); ‘How many computers does your family own (including laptops and tablets, not including game consoles and smartphones)?’ (0 = none, 1 = one, 2 = two, 3 = more than two); ‘How many bathrooms (room with a bath/shower or both) are in your home?’ (0 = none, 1 = one, 2 = two, 3 = more than two); ‘Does your family have a dishwasher at home?’ (0 = no; 1 = yes); ‘How many times did you and your family travel out of Spain for a holiday/vacation last year?’ (0 = not at all, 1 = once, 2 = twice, 3 = more than twice). The responses were recoded into three groups: Low (0–6); medium (7–9), and high family-wealth (10–13).
The following questions regarding school-based interventions for healthy eating were selected from the HBSC-SLQ: ‘Does your school carry out health promoting measures to build students’ competencies in nutrition and healthy eating?’; ‘Does your school have a formally established health promotion team or a working group on health promotion to carry out health promotion activities/measures?’; ‘Does your school have a policy to limit the consumption of candy, chips, and soft drinks among students?’; and ‘At your school, can students buy from vending machines or at the school store, cafeteria, or snack bar…’. For this question a list of different products was offered and the responses were grouped according to healthy products (fruit, vegetables, and dairy products) and unhealthy products (chocolate, candy, biscuits, cakes, pizza, and potato chips). All the response categories were dichotomized according to their availability (1 = yes, 0 = no).
Results
Statistical analysis
Descriptive statistics of continuous variables are presented as means and standard deviations, and absolute frequencies and percentages are described for categorical variables. Multiple logistic regression analyses were used to examine differences in eating behaviors that can be independently explained by (1) gender and age (Model 1); (2) parental educational level, parental occupational status, and family material wealth (Model 2); (3) peer behavior (Model 3); and (4) school measures and programs (Model 4). The probability of daily/frequent breakfast, fruit, candy, and sugary soft-drink consumption associated with all these factors was determined using the Odds Ratios (ORs) with 95% confidence intervals (CIs).
Multiple linear regression analyses were used to analyse the influence of school-based health measures and interventions on the students’ dietary behaviors, controlling for gender, age, and the socioeconomic status of the adolescents. The significance was tested from the standardized regression coefficientsβ (Beta) with 95% confidence intervals (CIs). For each regression model, R2 coefficient was calculated, and the increase in R2 values are indicated. A statistical test was also performed for all variables to examine if the R2 was significant, and F statistic tests were performed for each of the regression coefficients to determine the significance of the regression coefficients. The associated p values are presented in both analyses, and values lower than 0.05 were considered significant. All analyses were performed using the IBM SPSS Statistics 22.
Characteristics of the sample
Descriptive characteristics of the sample population.
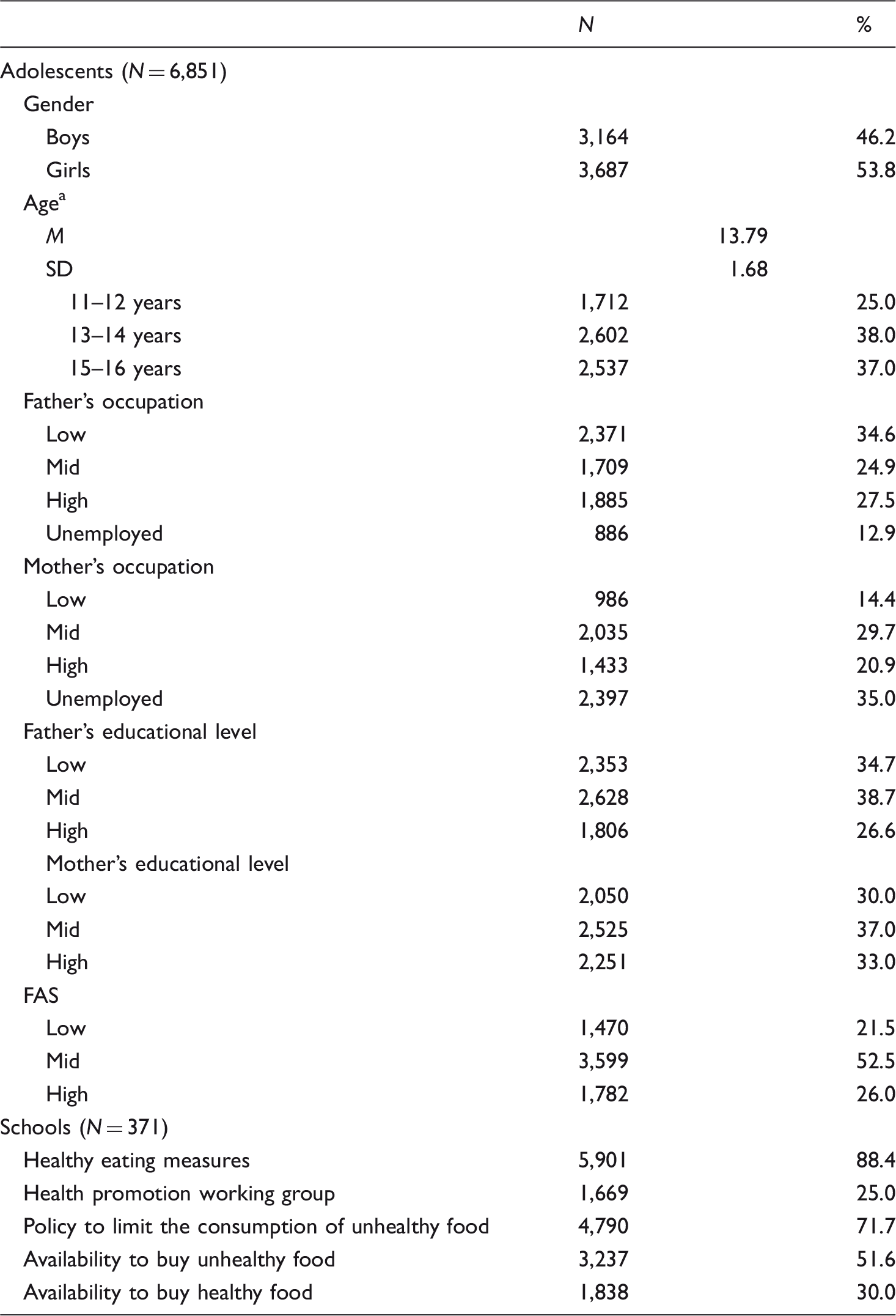
Note: FAS = family affluence scale; M = Mean; SD = standard deviation.
11–12 years (5th and 6th grades, Elementary school), 13–14 years (1st and 2nd year, Obligatory Secondary Education), 15–16 years (3rd and 4th year, Obligatory Secondary Education).
As shown in Table 1, 88.4% of the schools have measures to promote healthy eating, and approximately 70% have a policy to limit the consumption of candy, chips, and soft drinks among students. However, only 25% of the schools have a formally established health promotion team, and while 52% of the schools have unhealthy products available to students, only 30% of the schools make healthy products available.
Influence of individual, family, peer, and school factors in adolescent eating behaviors
Percentage of daily/frequent consumers (%) of breakfast, fruit, candy and soft drinks by age, gender and socioeconomic position.
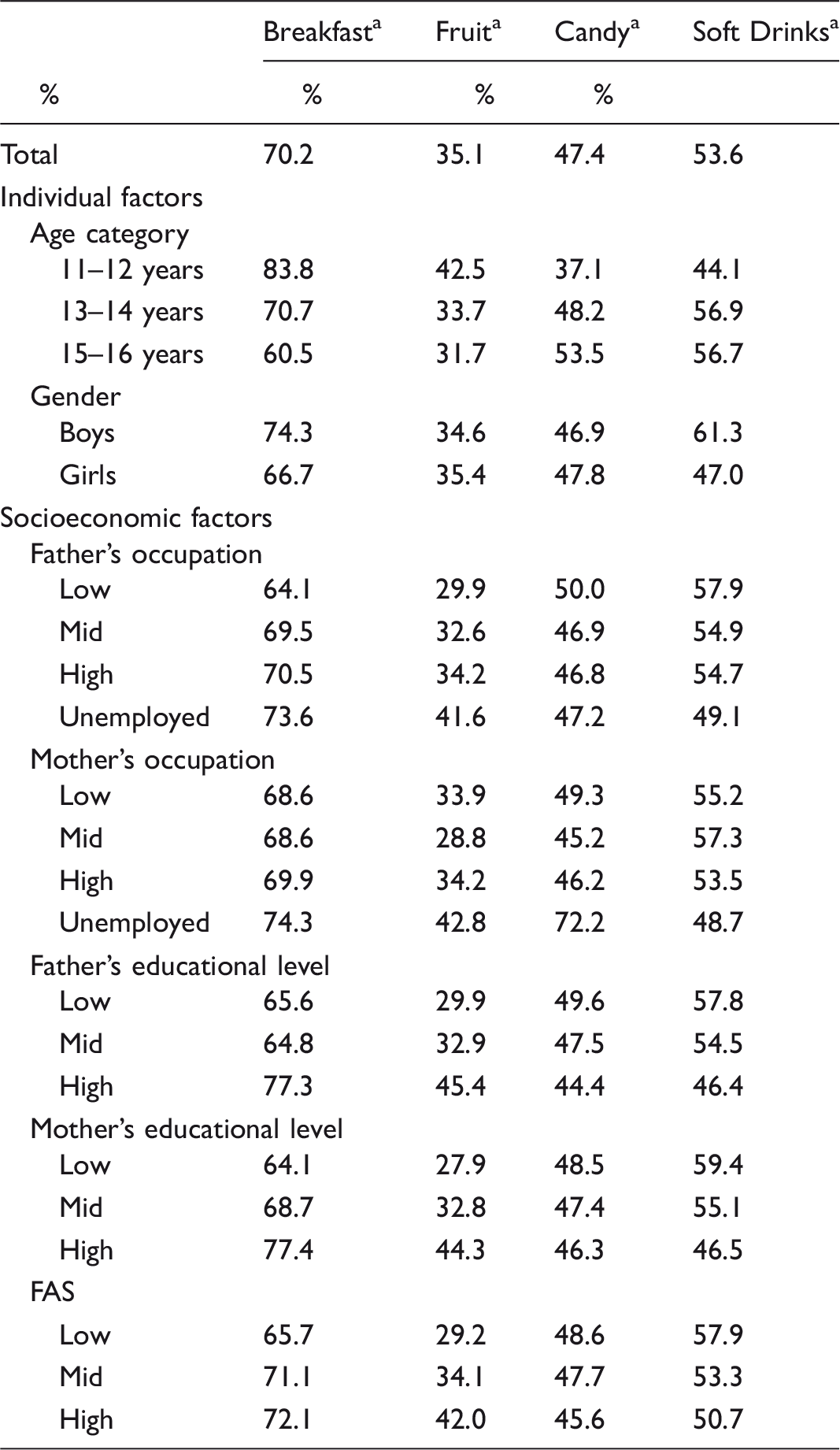
Note: FAS = family affluence scale.
The percentages represent the consumption of breakfast and fruit daily or more than daily, and the consumption of candy and soft drinks more than two days at week in all categories.
Effects of gender and age on adolescent eating behaviors
Logistic regression analyses predicting daily breakfast, fruit, sweet and soft drink consumption a from individual factors, family socioeconomic status and peer influence.
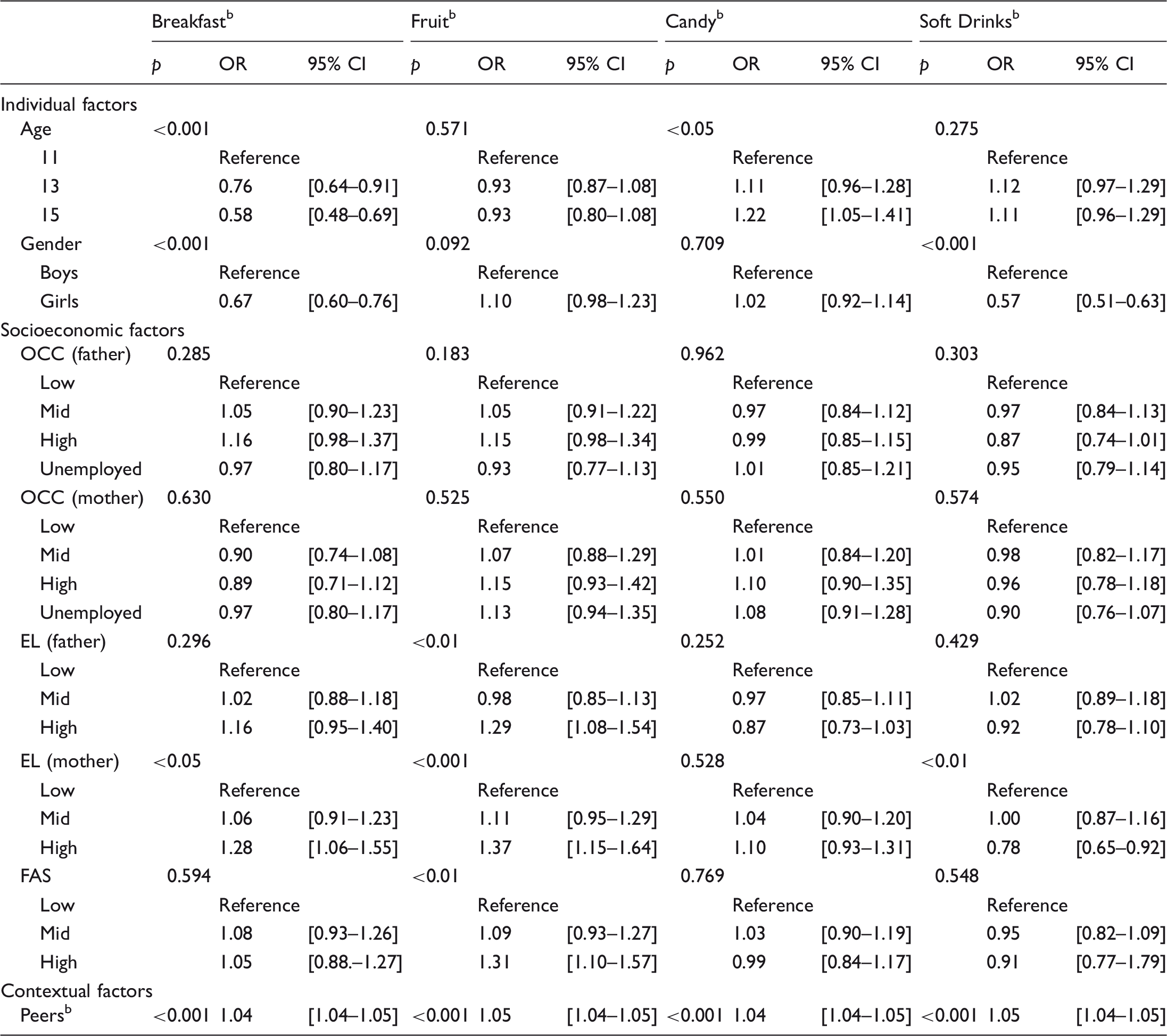
Note: CI = confidence interval; EL = educational level; FAS = family affluence scale; OCC = occupational status; OR = odds ratio.
The categories considered for eating behaviours represent the percentage of adolescents who performed the eating behaviour at least daily in the case of breakfast and fruit, and two or more days at week in the case of candy and soft drinks. bPeers represents the percentage of schoolmates in each participant school that performed the eating behaviour considered daily (for breakfast and fruit) or two or more days a week (for candy and soft drinks).
Effects of socioeconomic factors on adolescent eating behaviors
The aggregated socioeconomic indicators in the model were a significant predictor when controlling for gender and age (see Table 3). Different associations were found between the socioeconomic indicators considered and the eating behaviors. Parental education level showed the highest association with adolescent eating behaviors. Adolescents whose father has a high educational level were significantly (p < 0.01) more likely to eat fruit daily than those whose fathers have a low educational level (OR 1.29). The mother’s education level significantly predicted daily breakfast (p < 0.05), daily fruit (p < 0.001), and frequent soft-drink consumption (p < 0.01). In fact, mother’s high education level was the most important predictor of breakfast (OR 1.28) and fruit consumption (OR 1.37), as well as of the lower frequency of soft-drink consumption (OR 0.78). In addition, adolescents from families with high material affluence were significantly more likely to eat fruit every day (p < 0.001) than those from less affluent families (OR 1.31). No significant effects were found between father and mother’s occupation and eating behaviors after controlling the effects of parental educational level and family affluence.
Peer effect on adolescent eating behaviors
In the next step, the peer (schoolmates) eating behaviors were added to the model (see Table 3). Statistically significant associations (p < 0.001) were found between the adolescents’ breakfast, fruit, candy, and soft-drink consumption with respect to their peers’ breakfast (OR 1.04), fruit (OR 1.05), candy (OR 1.04), and soft-drink (OR 1.05) consumption at the same school, controlling for gender, age, and socioeconomic status.
School effect on adolescent eating behaviors
The multiple logistic regression model, shown in Table 3, only presents the contribution of the three blocks of variables considered in individual, family, and peer contexts. In the last step, aggregated school variables (Block 4) did not add anything to the model in any case nor for any equation. Changes in Nagelkerke from block 3 to 4 and the Chi-square test showed no significant differences in breakfast (
Multiple linear regressions for the independent associations between measures/programs carried out by the schools and eating behaviours of students at the same school.
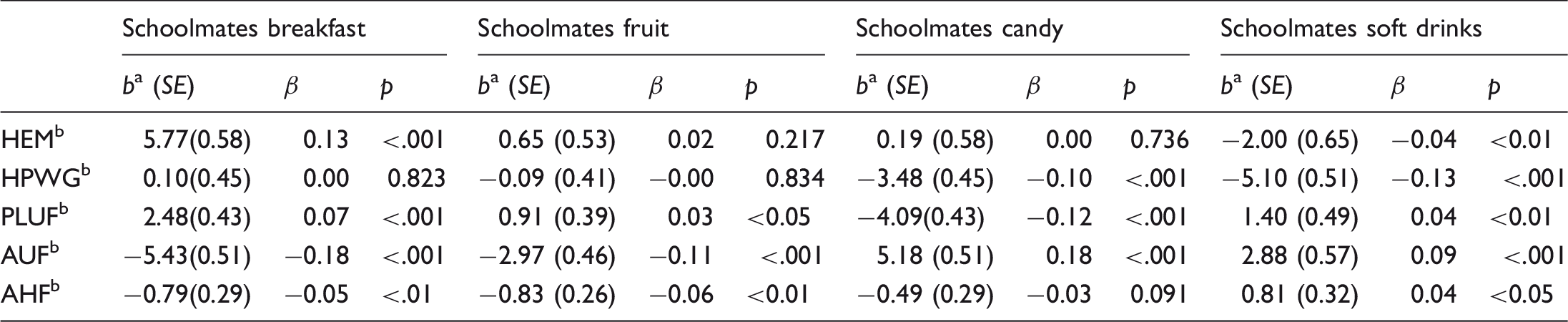
Note: AHF = availability to buy healthy food; AUF = availability to buy unhealthy food; HEM = healthy eating measures; HPWG = health promotion working group; PLUF = policy to limit the consumption of unhealthy food.
b, unstandardized regression coefficients representing an increase (or a decrease) in the percentage of daily/frequently breakfast, fruit, candy and soft drink consumers at the same school associate with the measures and programs for healthy eating habit promoted by the schools. bMultiple linear regression analysis was adjusted for age, gender and socioeconomic status.
As we observe in Table 4, schools that implement health-promoting measures to build student competencies in nutrition significantly increase the probability of a student’s (considered as a group according to school) daily breakfast consumption (β = 0.13; p < 0.001), and significantly decrease the probability of frequent soft-drink consumption (β = −0.04; p < 0.01). Formally established health-promotion teams at school significantly decrease students’ consumption of candy (β = −0.10; p < 0.001) and soft drinks (β = −0.13; p < 0.01). Policies limiting the consumption of candy, chips, and soft drinks at schools significantly increase the students’ consumption of breakfast (β = 0.07; p < .001), fruits (β = 0.03; p < 0.05), and soft drinks (β = 0.04; p < 0.01), and significantly decrease candy consumption (β = −0.12; p < 0.001). Schools with unhealthy products available for students to buy were significantly associated (p < 0.001) with students’ unhealthy eating behaviors, showing decreasing breakfast (β = −0.18) and fruit (β = −0.11) and increasing candy (β = 0.18) and soft-drink consumption (β = 0.09) among the students. However, having healthy products available was significantly associated (p < 0.01) with decreasing fruit consumption (β = −0.06) and increasing soft-drink consumption (β = 0.04). These unexpected finding will be addressed in the discussion.
Discussion
This study, using data from a nationally representative sample in Spain, highlights the importance of promoting healthy eating behaviors among adolescents. As our findings show, only 35.1% of adolescents in Spain eat fruit daily, approximately 30% do not consume breakfast daily, and 50% eat candy and consume soft drinks two or more days a week. Influential factors for adolescent eating behaviors were examined.
Age and gender differences in eating behaviors
The results of this study show that psychologists in schools – in collaboration with families, pediatricians, politicians and other in-school professionals such as teachers, administrators, lunch director, wellness committee, and other related service personnel – when designing school based-interventions to promote healthy eating habits among adolescents can improve their effectiveness by considering the age and gender of the participants. For example, adolescents age 13-years-old and older tend to adopt some unhealthy eating behaviors, consistent with previous findings that older adolescents present lower breakfast and higher candy consumption (Diethelm et al., 2012; Niemeier et al., 2006; Taut et al., 2015). Thus, primary prevention programs at age 12-years-old or earlier could be more effective than when implemented later.
In addition, results showed that boys present higher rates of soft-drink consumption, also confirmed by other studies (Moreira et al., 2010; Schröder et al., 2014) and in line with findings that show unhealthier eating habits in boys (Inchley, Todd, Bryce, & Currie, 2001; Vereecken et al., 2015; Voráčová, Sigmund, Sigmundová, & Kalman, 2015). However, even though girls usually show healthier food choices, they were less likely to eat breakfast daily, also confirmed by prior research (Bialowolski & Weziak-bialowolska, 2014; Ramos, Brooks, García-Moya, Rivera, & Moreno, 2013). Girls tend to show a higher prevalence of body-image concerns (Rolls, Fedoroff, & Guthrie, 1991), which is related to non-appropriate diet-controlling behaviors such as skipping breakfast (Timlin, Pereira, Story, & Neumark-Sztainer, 2008). Intervention programs for health promotion, or at least some of their components more related to psychological contents, should consider the unique needs of boys and girls. Specifically, whereas popularity in school-friend networks has been associated with certain obesity-related behaviors, such as consuming energy-dense snacks, with boys being more influenced by their peers in snack and fast-food consumption (De La Haye et al., 2010), girls have shown to be more sensitive to social pressure regarding dieting and eating disorders (Lieberman et al., 2001; Mackey & La Greca, 2007; Shroff & Thompson, 2006).
Socioeconomic status and nutrition
Different relationships have been found between the distinct socioeconomic dimensions for predicting healthy adolescent eating behaviors (Fismen et al., 2012; Galobardes et al., 2001; Turrell et al., 2003). Considering the effects of parental educational level and family material wealth, neither parent’s occupational status was significant. Adolescents from families with high material affluence were more likely to eat fruit daily (Fismen et al., 2012). Other findings show both parental occupational status and family affluence as independent predictors of fruit consumption among adolescents; however, parental education level was not considered (Vereecken et al., 2005). These results could be explained by food prices, as less affluent families have to consider cost when choosing food. Candy and high-fat food provide cheaper calories than fruit or other nutritious foods. Measures to reduce the price of healthy products have been shown to increase healthy food consumption (French, 2003).
Parental education level was the strongest indicator associated with food consumption and showed an independent effect from family affluence. In addition, maternal education was the strongest predictor of healthy food-related behaviors among adolescents, as confirmed by earlier studies (Hupkens Knibbe, & Drop, 2000; Moreira et al., 2010). Parental education, and especially maternal educational level, has been consistently associated with children and adolescents’ dietary choices (Fisher, Mitchell, Smiciklas-Wright, & Birch, 2002; Kastorini et al., 2016). Mothers with a higher education level tend to consume healthier products, value health above cost in their food choices, and present less permissive parenting practices (Hupkens, Knibbe, & Drop, 2000; Moreira et al., 2010; Vereecken, Keukelier, & Maes, 2004). In addition, parental education level has an important effect on health by promoting access to resources, knowledge, and social structures that foster health and well-being (McLaughlin et al., 2011). Educational programs such as those offering information about nutritional topics, can reinforce education received at school, as well as supply resources such as how to look for quality information. In the document Social Determinants of Health: Solid Facts (Wilkinson & Marmot, 2003) health risks in children have demonstrated reductions through improvements in the educational levels of parents and children, offering an example of the direct benefits of health and education programs.
Policies and practices aimed at promoting healthy eating in schools should also consider the influence of socioeconomic inequalities on adolescent eating behaviors, provide nutritional information, and consider the important nurturing role that mothers play in their children’s diet (Dalma et al., 2016) while reinforcing the father’s role in promoting healthy eating habits among their children.
Peer and school
Similar patterns were found between adolescents and their peers regarding breakfast, fruit, candy, and soft-drink consumption. Previous findings have shown the influence of peer behavior on adolescents, showing how their perceptions of their peers’ consumption of fruit, vegetables, soft drinks, and unhealthy snacks influence their own consumption of these products (Lally, Bartle, & Wardle, 2011; Perkins, Perkins, & Craig, 2010). A literature review by Salvy, De La Haye, Bowker, and Hermans (2012) analysed how mechanisms which explain peer influence in adult eating behaviors can be applied to adolescents. Three possible explanations were explored: Social facilitation by emulating the behaviors of others (Bandura, 1977); modelling based on changes in individual behaviors in the presence of others (to make a good impression on friends); and impression management, which seeks to explain an individual’s motivation to behave when in the company of others. The authors concluded that children and adolescents’ unhealthy eating behaviors increase in the presence of peers, except in situations where impression management concerns are high and where peers exhibit healthy eating behaviors.
Regarding the influence of school-based nutrition interventions, after controlling the effect of gender, age, socioeconomic status, and peer influences, our study did not show any effect on eating behaviors for individual adolescents. These results are consistent with research conducted by Blom-Hoffman and DuPaul (2003), in which the roles of school psychologists and nutrition-education programs in health promotion did not show any changes in children’s lunch-time eating behaviors. However, the influence of school-based healthy-eating interventions on the students as a group was significant, suggesting that they could be more effective when focused on the community level (for example, including group educational activities). Further research is needed to understand how social networks influence adolescent eating behaviors. As the present findings and other recent research support (Bahr, Browning, Wyatt, & Hill, 2009; El-Sayed et al., 2013; Zhang et al., 2015), social networks may help promote healthy eating behaviors in adolescents and prevent obesity.
Finally, schools where there were already measures to build student competencies in nutrition showed more healthy eating behaviors among their students when compared to those where there were no measures. For example, healthy-eating measures increase daily breakfast consumption and decrease soft-drink consumption and having a formally established health-promotion team at school decreases consumption of soft-drinks and candy. When schools have policies that limit the consumption of candy, chips, and soft drinks, our findings show that students eat breakfast and fruit more frequently and eat less candy. Supporting this, earlier research has identified an increase in healthy eating behaviors and a reduction in adolescent obesity among school children when their teachers had received training on nutrition, as well as in those attending schools with food policies (Arriscado et al., 2014; Larson et al., 2013). However, a relationship was identified between policies to limit unhealthy food in schools and a higher percentage of adolescents that frequently consume soft drinks. One possible explanation is that schools with students with high consumption of unhealthy foods tend to implement healthy-eating policies.
With respect to food availability in schools, this study has also found important factors to consider when designing interventions. Lower consumption of breakfast and fruit and higher consumption of candy and soft drinks was found in schools that have unhealthy products available. Surprisingly, lower fruit consumption and higher soft-drinks consumption was found in schools which also have healthy products available. When nutritious products are offered in the schools competing with candy, sugary soft drinks, and snacks, adolescents tend to choose unhealthy products (Briefel et al., 2009). Therefore, school policies should focus on limiting the availability of unhealthy products (forcefully) while increasing the availability of healthy products. Moreover, school interventions developed to promote healthy eating should include efforts to make healthy food more attractive and encourage the selection of healthy products over more tempting and less healthy alternatives (Adriaanse, van Oosten, de Ridder, de Wit, & Evers, 2011; Luszczynska et al., 2016).
Limitation and strengths
Some limitations should be considered when interpreting these results. Cross-sectional data does not allow for identification of causal relationships between the variables analysed. Therefore, to examine the influence of social networks on adolescent behaviors, this study considered ‘peers’ as all classmates, thereby avoiding increasing similarities when close friends are exclusively considered. For example, in studies based on friends’ eating behaviors, it is difficult to determine to what extent similarities are due to friend selection based on similar characteristics (homophile), as other research has proposed (Cohen-Cole & Fletcher, 2008; Valente, Fujimoto, Chou, & Spruijt-Metz, 2009). Therefore, longitudinal studies are needed to establish the role of eating behaviors in social-network selection and the mechanisms that explain the influence of peer food-related behaviors. Similarly, longitudinal data is required to verify the impact of school measures and interventions promoting healthy eating behaviors.
Furthermore, some methodological limitations should be mentioned. Consumption was assessed by frequency not quantity. Frequency was measured on seven-point scales but was recoded into dichotomous variables to facilitated data analysis. This reduced information diversity. Despite including different contextual factors, further research should explore how family socioeconomic status, peers, and school environment, influence adolescent eating behaviors. Moreover, future research should analyse characteristics of the social networks to identify the adolescents’ social status and the individual’s characteristics that make them more influential or influenced by others.
Nonetheless, this study has several strengths. For example, a wide range of measures were included and also different informants participated in the study. Despite the adolescents providing the information about themselves and their families, which could be viewed as a limitation, school information was provided by the members of the staff (directors, teachers, or school counsellors). Information about each individual was provided directly by the students themselves, resolving difficulties cited by other studies when evaluating peer influence in which individuals are asked about their perception of their peers (Fletcher et al., 2011). Another strength of this study was that it considered the impact of socioeconomic inequalities by including different indicators to evaluate how each impacts specific adolescent food-related behaviors. Finally, by including indicators regarding school intervention, we were able to evaluate which specific intervention characteristics make them effective or not for promoting healthy eating-behaviors.
Footnotes
Acknowledgements
We thank the participating adolescents and schools, the research assistants from the Spanish HBSC team who took part in this study and Ian Scionti and Michael Box for providing language help.
Financial Support
The 2014 edition of the HBSC study in Spain was supported by an agreement signed by the Spanish Ministry of Health, Social Policy and Equality and the University of Seville. In addition, this work was supported by the Andalusian Department of Economy, Innovation, Science and Employment (CMM, grant received in the framework of the program Incentivos a Proyectos de Investigación de Excelencia – Incentives for Research Projects of Excellence – Ref. SEJ08007). The Spanish Ministry of Health, Social Policy and Equality and the Andalusian Department of Economy, Innovation, Science and Employment had no role in the design, analysis or writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.