
Abstract
Iraq and Afghanistan war veterans experience significant rates of posttraumatic stress disorder (PTSD) and other trauma-related mental health conditions. Understanding how specific PTSD symptomatology affects physical health and psychosocial functioning may be useful in improving the conceptualization of PTSD nosology and informing treatment approaches for this population. Confirmatory factor analytic evidence supports four-factor models of PTSD symptoms that classify emotional numbing and/or dysphoria symptoms as a distinct PTSD symptom cluster, and these symptoms appear to be related to poorer psychological adjustment among returning Iraq and Afghanistan war veterans. This review briefly describes current conceptualizations of numbing/dysphoria symptoms of PTSD and summarizes research on the factor structure of PTSD symptoms. Then, the literature on the influence of numbing/dysphoria symptoms on physical and psychological health among these veterans is reviewed, and implications for treatment and directions for future research are presented.
The majority of U.S. military service members returning from combat operations in Iraq and Afghanistan report high levels of combat exposures, including receiving incoming enemy fire, seeing or handling dead bodies, knowing someone who was injured or killed, and/or killing an enemy combatant (Hoge, Auchterlonie, & Milliken, 2006; Hoge et al., 2004; Maguen et al., 2010). As a result of their exposure to combat and other types of traumatic events (e.g., military sexual trauma) during service, returning veterans are at significant risk for developing trauma-related mental health conditions, such as posttraumatic stress disorder (PTSD), major depressive disorder (MDD), and substance use disorders (Hoge et al., 2004; Hoge et al., 2006; Seal, Bertenthal, Miner, Sen, & Marmar, 2007). Estimated rates of PTSD among Iraq and Afghanistan military personnel following deployment vary from 6.2% to 12.9%, depending on the branch of service and location of deployment (Hoge et al., 2004). Considerable rates of PTSD have also been documented among recently returning veterans with mental health diagnoses seeking care at Veterans Affairs (VA) health care facilities (i.e., 12%-13%; Seal et al., 2007; Stecker, Fortney, Owen, McGovern, & Williams, 2010). Given the prevalence of PTSD among Iraq and Afghanistan veteran populations, efforts aimed at enhancing our understanding of the impact of specific PTSD symptomatology on physical health and psychosocial functioning, and identifying effective and appropriate psychological interventions for this population, are of great importance.
Although current diagnostic criteria for PTSD fall into three symptom clusters (i.e., reexperiencing, avoidance/numbing, and hyperarousal; American Psychiatric Association [APA], 2000), confirmatory factor analytic evidence has garnered support for a four-factor model of PTSD symptoms, which contains a distinct cluster of PTSD symptoms generally referred to as either emotional numbing or dysphoria symptoms (Elhai & Palmieri, 2011; King, Leskin, King, & Weathers, 1998; Simms, Watson, & Doebbeling, 2002). Given recent evidence bolstering the superiority of a four-factor model of PTSD (Elhai & Palmieri, 2011), proposed modifications to the current diagnostic classification of PTSD have recognized numbing/dysphoria symptoms as a unique feature of the disorder (APA, 2010). Findings from recent studies of trauma-exposed populations have demonstrated positive associations between numbing and dysphoria symptoms of PTSD and distress-related outcomes, such as chronicity of distress, impaired interpersonal functioning, and lower overall quality of life (e.g., Clapp, Beck, Palyo, & Grant, 2008; Ruscio, Weathers, King, & King, 2002; Thompson et al., 2004). Moreover, a number of recent investigations of Iraq and Afghanistan veteran populations have distinguished numbing/dysphoria symptoms of PTSD as prominent and significant features of posttraumatic distress (e.g., Jakupcak et al., 2010a; Pietrzak, Goldstein, Malley, Rivers, & Southwick, 2010). Accordingly, there is some indication that greater severity of numbing or dysphoria symptoms may be associated with poorer postdeployment adjustment and may be a useful target for treatment interventions among combat veterans.
The present review examines the empirical literature on the correlates of dysphoria/numbing symptoms of PTSD among Iraq and Afghanistan war veterans. This review’s focus on veterans from recent conflicts was largely driven by practical, rather than theoretical, considerations. Although the difficulties associated with numbing/dysphoria features of PTSD presented herein are likely germane to broader trauma populations, the majority of recent research bearing on emotional numbing, especially factor analytic modeling studies that inform the present review, have been conducted among veteran populations. Furthermore, our focus on Iraq and Afghanistan veterans, as opposed to other combat groups, provides some assurance that the posttraumatic adjustment issues under consideration were not influenced by chronic maladaptive coping strategies or secondary conditions that can emerge long after combat exposure. First, a brief description of the current three-factor and, more recently proposed, four-factor models of PTSD are presented. Then, current conceptualizations of numbing/dysphoria symptoms of PTSD are discussed, and the associations between clusters of PTSD symptoms and clinical outcomes among Iraq and Afghanistan war veteran samples are reviewed. Particular attention is devoted to the impact of numbing/dysphoria symptoms on physical and psychological health outcomes among combat veterans from recent conflicts. In the remaining sections, implications for treatment and suggestions for potentially useful evidence-based treatment interventions are presented. Last, methodological limitations of previous investigations are highlighted and directions for future research are offered.
The Factor Structure of PTSD
Current Three-Factor Model of PTSD
To meet diagnostic criteria for PTSD, current nosology, as outlined in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000), requires exposure to a traumatic event in which one “experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others” and resulted in a response characterized by “intense fear, helplessness or horror” (i.e., Criterion A; APA, 2000, p. 467). In addition, individuals must exhibit a requisite number of symptoms that comprise three distinct symptom clusters: reexperiencing, avoidance, and arousal. The first cluster, reexperiencing (i.e., Criterion B), comprises symptoms of persistent trauma-related recollections, such as recurrent and intrusive distressing trauma-related thoughts or memories, recurrent dreams of the traumatic event, acting or feeling as if the events were reoccurring, and intense psychological distress or physical reactivity at exposure to internal or external trauma-related cues (APA, 2000). The second symptom cluster, avoidance or numbing (i.e., Criterion C), is characterized by efforts to avoid trauma-associated thoughts, feelings, conversations, activities, places, or people, an inability to recall important aspects of the trauma, diminished interest in activities, feelings of detachment from others, restricted range of affect, and a sense of a foreshortened future (APA, 2000). Cluster 3, arousal (i.e., Criterion D), includes impaired sleep, irritability or outbursts of anger, impaired concentration, hypervigilance, and an exaggerated startle response (APA, 2000).
Proposed Four-Factor Models of PTSD
Results from recent confirmatory factor analytic investigations have garnered support for a four-factor model of PTSD symptoms, as opposed to the traditional three-factor model outlined in DSM-IV (4th ed.; APA, 1994). Specifically, empirical evidence has supported two distinct four-factor models of PTSD symptoms, referred to, respectively, as the emotional numbing and dysphoria models (see Figure 1). King and colleagues (1998) found support for a four-factor emotional numbing model consisting of the traditional reexperiencing and hyperarousal factors, which correspond to Clusters B and D in DSM-IV, and separate avoidance and numbing factors comprised of symptoms drawn from Cluster C. In King et al.’s (1998) model, behavioral avoidance symptoms (i.e., Criteria C1-C2) are distinguished from emotional numbing symptoms (i.e., Criteria C3-C7). In contrast, the dysphoria four-factor model proposed by Simms et al. (2002) differs from the emotional numbing model in that the newly identified dysphoria cluster consists of the aforementioned emotional numbing symptoms (i.e., Criteria C3-C7) and three hyperarousal symptoms (i.e., Criteria D1-D3; sleep disturbance, irritability/anger, and difficulty in concentrating). The reexperiencing factor (Criterion A) is retained, analogous to DSM-IV, whereas the avoidance and hyperarousal factors each consist of two symptoms (i.e., Criteria C1-C2 and Criteria D4-D5, respectively).
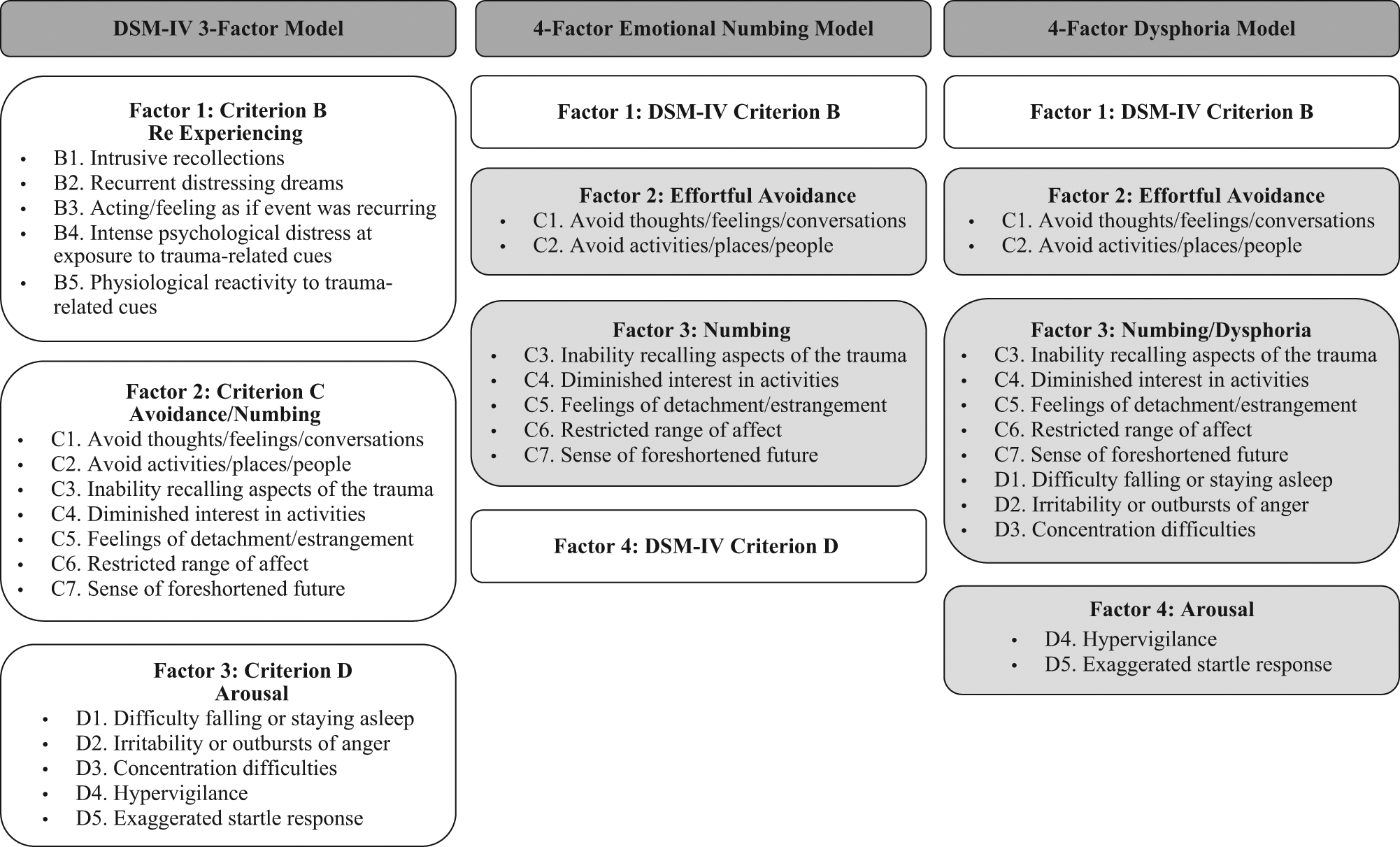
Factorial models of PTSD symptoms
Factor analytic investigations have replicated findings bolstering the emotional numbing (e.g., Asmundson et al., 2000; Cox, Moata, Clara, & Asmundson, 2008; King et al., 1998; Palmieri & Fitzgerald, 2005) and dysphoria (e.g., Baschnagel, O’Conner, Colder, & Hawk, 2005; Palmieri, Weathers, Difede, & King, 2007; Simms et al., 2002) four-factor models of PTSD. In addition, recent studies have examined the factor analytic structure of PTSD among Iraq and Afghanistan veteran and active duty samples, with some providing validation for the emotional numbing model (Mansfield, Williams, Laurel, & Babeu, 2010; McDonald et al., 2008) and others offering support for the dysphoria model (Engdahl, Elhai, Richardson, & Frueh, 2011; Meis, Erbes, Kaler, Arbis, & Polusny, 2011; Pietrzak et al., 2010). Most investigations utilized forms of measurement that contain the 17 PTSD symptoms outlined in DSM-IV, which suggests consistency across measurement. However, this is an inherent limitation, as the factor analytic studies do not account for other forms of common trauma sequelae (e.g., substance use, depression, interpersonal deficits; Elhai & Palmieri, 2011) There is a general consensus that both four-factor models are suitable and superior to the traditional three-factor model outlined in DSM-IV (Elhai & Palmieri, 2011); however, there remains some disagreement as to which four-factor model best classifies the symptoms that characterize PTSD.
It is important to note that seemingly different conceptual models (i.e., numbing vs. dysphoria conceptualizations) may not be fundamentally dissimilar. Although factor analytic studies have yielded slightly different symptom clusters, the dysphoria and numbing models converge on a core subset of symptoms: (C3) inability to recall an important aspect of the trauma, (C4) markedly diminished interest or participation in significant activities, (C5) feeling of detachment and estrangement from others, and (C6) restricted range of affect (e.g., unable to have love feelings; APA, 2000). What seems to differentiate the models is whether DSM Criteria D1 to D3 (i.e., sleep disturbance, irritability/anger, and difficulty concentrating) are included.
Regardless of the ultimate empirical and conceptual superiority of the numbing versus the dysphoria model, it seems sufficiently clear that any “numbing” or dampening of emotional response is likely confined to positive emotionality among most individuals with PTSD. PTSD is by definition characterized by extremes of fear and/or anxiety, is highly comorbid with depression (Ikin, Creamer, Sim, & McKenzie, 2010; Momartin, Silove, Manicavasagar, & Steel, 2004), and finally, one of the defining symptoms of PTSD according to the DSM-IV is increased anger and irritability. As such, negative emotionality does not seem to be dampened or restricted; quite the opposite, PTSD is a disorder characterized by excesses in negative emotionality.
The defining symptoms that have historically characterized emotional numbing in PTSD (symptoms C3-C7) imply—or in the case of symptom C6—explicitly reference reductions in positive emotions. Litz and Gray (2001) maintain that pretraumatic emotional repertoires are in fact accessible to individuals with PTSD and that emotional numbing symptoms are instead a product of inhibited emotional expression rather than a limited capacity to feel and express emotions, a position supported by veterans’ reports of strategically withholding emotional expressions (Roemer, Litz, Orsillo, & Wagner, 2001). Accordingly, true broad-based emotional numbing does not seem to be characteristic of PTSD. Instead, dampening of positive emotionality is central to the numbing associated with PTSD. Litz and Gray (2001) have theorized that reexperiencing symptoms of PTSD may result in a predisposition that necessitates more intense stimulation of positive affectivity to access the full range of emotional behaviors. Hence, individuals with PTSD may be more likely to respond at lower threshold intensity to negative cues, whereas positive stimuli may need to be of greater intensity to elicit positive emotional responses. Despite debate over the appropriateness of the term, because the word numbing has been ubiquitously used in the literature to describe these more circumscribed deficits, we follow suit in this review by adopting conventional terminology and using the term numbing/dysphoria to describe these deficits.
Findings regarding the factor analytic structure of PTSD symptoms have been taken into consideration for the proposed modifications to the diagnostic classification of PTSD in the upcoming version of DSM, DSM-V. Anticipated changes to the diagnostic classification of PTSD include the addition of a fourth symptom cluster, which has been described as “negative alterations in cognitions and mood” that are associated with the traumatic event (APA, 2010). Symptoms anticipated to comprise the novel cluster include many of the factor-analytically derived numbing symptoms from prior investigations (i.e., inability recalling important aspects of the trauma, diminished interest/participation in activities, feelings of detachment or estrangement, and inability to experience positive emotions; APA, 2010). The proposed cluster will also likely include other commonly observed trauma sequelae, such as persistent and exaggerated negative expectations about one’s self, others, or the world; persistent distorted perceptions of blame about the cause or consequences of the traumatic event; and a pervasive negative emotional state (e.g., fear, horror, anger, guilt, or shame; APA, 2010). Accordingly, it is likely that numbing/dysphoria symptoms will remain an important feature of PTSD and will remain a valuable target for psychological interventions.
Impact of Numbing/Dysphoria Symptoms on Iraq and Afghanistan Veterans
Evidence suggesting a relationship between numbing/dysphoria symptoms of PTSD and poorer psychological adjustment has been documented among diverse trauma populations such as motor vehicle accident survivors (Clapp et al., 2008; Taylor et al., 2001), Cambodian refugees (Palmieri, Marshall, & Schell, 2007), women exposed to intimate partner violence (Krause, Kaltman, Goodman, & Dutton, 2006), individuals indirectly exposed to the September 11 terrorist attacks (Baschnagel et al., 2005), and veteran populations (e.g., Ruscio et al., 2002). Among samples of combat veterans, severity of numbing/dysphoria symptoms has been linked to a number of important indicators of psychological adjustment, such as interpersonal functioning (e.g., Riggs, Byrne, Weathers, & Litz, 1998; Ruscio et al., 2002); violent behavior (Maguen, Stalnaker, McCaslin, & Litz, 2009); increased risk of developing comorbid psychological conditions, such as depression and other anxiety disorders (Kashdan, Elhai, & Frueh, 2006); and quality of life (Lunney & Schnurr, 2007). As will be reviewed below, there are unique problems and deficits associated with this particular symptom domain.
A literature search was conducted utilizing the PsycINFO database and was limited to articles published in peer-reviewed scholarly journals printed in English. Search terms PTSD, numbing, dysphoria, and veterans were utilized. All empirical investigations that examined the correlates of PTSD symptom clusters according to three- and four-factor models of PTSD (i.e., avoidance, numbing, and/or dysphoria) among samples of Iraq and Afghanistan veterans were included in the present review. To date, eight studies have examined the influence of numbing/dysphoria symptoms of PTSD on physical health-risk behaviors, interpersonal functioning, and other indicators of psychological distress and global functioning among returning Iraq and Afghanistan veteran populations. All studies utilized measures of PTSD symptom severity that exclusively contained the 17 symptoms that comprise DSM-IV criteria for PTSD and grouped them according to the three- or four-factor models of PTSD.
Physical Health-Risk Behaviors
Two investigations have found support for a positive relationship between PTSD numbing symptoms and physical health-risk behaviors among recently returning Iraq and Afghanistan veterans. Cook, Jakupcak, Rosenheck, Fontana, and McFall (2009) examined the relationship between smoking and PTSD symptom clusters according to the four-factor numbing model among Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans referred for VA mental health services. Accounting for depression, higher total PTSD symptom severity significantly predicted heavy smoking, and furthermore, veterans who endorsed higher levels of emotional numbing symptoms were more likely to report being a heavy smoker (≥20 cigarettes per day) than a nonsmoker. No other significant associations were found between veterans’ reported smoking status and levels of the other PTSD symptom clusters.
In another investigation, Jakupcak et al. (2010a) evaluated the relationship between PTSD symptoms according to the numbing model and alcohol misuse among veterans utilizing postdeployment VA care. A significant positive association was found between emotional numbing symptoms and alcohol misuse (OR = 1.35, 95% CIs = [1.04, 1.75]), even after accounting for depression symptom severity. No other PTSD symptom clusters were significantly associated with alcohol misuse. Numbing symptoms of PTSD may be an important factor to consider when understanding returning veterans’ engagement in health-risk behaviors. Findings suggesting a link between numbing symptoms, and smoking and alcohol misuse are of particular relevance, given their high prevalence among veteran populations (e.g., Hoge et al., 2004, Seal et al., 2007) and the negative impact of these behaviors on physical health.
Interpersonal Functioning
The influence of numbing/dysphoria on aspects of interpersonal and social functioning has received increasing attention within the PTSD literature. Three studies have found evidence supporting a link between numbing/dysphoria symptoms and poorer interpersonal adjustment among Iraq and Afghanistan veterans. Sayers, Farrow, Ross, and Oslin (2009) evaluated the relationship between PTSD symptoms and family problems among a sample of recently returning veterans referred by primary care for a mental health evaluation. Results demonstrated greater role-related readjustment problems among veterans who had a PTSD or depression diagnosis. Specifically, a PTSD diagnosis was associated with an increased likelihood of “feeling like a guest in one’s own home” and, among partnered veterans with children, feeling that children were acting afraid or not warmly toward the veteran. Findings based on a four-factor numbing model of PTSD indicated that numbing and avoidance symptoms were associated with a greater likelihood of having at least one role-related family problem (OR = 3.3, 95% CIs = [1.3, 8.1] and 2.5, 95% CIs = [1.0, 5.9], respectively).
Similarly, Erbes, Meis, Polusny, and Compton (2011) examined the relationship between couple adjustment and PTSD symptoms in returning National Guard veterans. Modeling based on a four-factor dysphoria model of PTSD revealed that dysphoria was the most important factor in explaining intimate relationship adjustment among National Guard soldiers within an initial 6-month period following their return from deployment and was the only cluster that significantly predicted relationship adjustment at a 1-year follow-up assessment period. Accordingly, dysphoria/numbing symptoms may have a negative influence on the quality of returning veterans’ intimate and family relationships.
In a related vein, Nunnink, Goldwaser, Afari, Nievergelt, and Baker (2010) investigated the impact of PTSD numbing symptoms on sexual functioning among veterans enrolling for VA care. Veterans were categorized into one of two groups representing the presence or absence of sexual problems, which were considered based on endorsement of either “impotence or other sexual problems” and/or “diminished sexual desire or function.” Significantly higher severity of overall PTSD symptoms was found among veterans who screened positively for sexual problems, and only the numbing cluster was a significant predictor of sexual functioning. Accordingly, numbing symptoms of PTSD may be an important factor to consider when evaluating veterans’ sexual functioning. However, assessment of sexual functioning was based on self-reported changes in libido. As diminished interest in sex is a common feature of depression, and most likely the dysphoric and numbing features of PTSD, compromised sexual functioning, as assessed in this investigation, may represent another aspect of negative emotionality specific to PTSD rather than an actual physical health problem.
Growing evidence supports a link between numbing/dysphoria symptoms of PTSD and poorer interpersonal functioning. Specifically, findings indicate that numbing/dysphoria symptoms may be associated with poorer quality of intimate and family relationships. However, the studies reviewed relied exclusively on veterans’ report of family problems. Future research efforts should incorporate assessments of intimate partner and family perceptions of relationship quality. Similarly, it would be useful to obtain information about the quality of veterans’ interpersonal relationships prior to deployment to determine the unique impact of PTSD symptoms on relationship functioning. Regardless, the fact that a number of interpersonal and familial deficits are associated with numbing/dysphoria rather than global PTSD symptom severity per se, suggests that this may be a particularly pernicious facet of the disorder that warrants more research and clinical attention.
Distress-Related and Global Psychological Outcomes
Similarly, emerging evidence suggests that PTSD numbing/dysphoria symptoms may be distinctly related to a number of important aspects of global psychological functioning in Iraq and Afghanistan veteran populations. To date, there have been three studies illustrating relationships between numbing symptoms and clinical indicators of psychological adjustment. Shea, Vujanovic, Mansfield, Sevin, and Liu (2010) examined the unique contribution of the three traditional PTSD symptom clusters on several areas of psychosocial functioning, symptom severity, and subjective distress among returning OEF/OIF National Guard and Reserve veterans. Veterans’ levels of psychosocial functioning, distress, and PTSD symptom severity were assessed in addition to other Axis I mental health conditions using clinical diagnostic interviews. Results revealed that PTSD diagnosis was a unique predictor of subjective distress, social impairment, occupational functioning, global severity, global social adjustment, life satisfaction, and global assessment of functioning after accounting for other Axis I conditions. More specifically, however, in terms of the three DSM-IV PTSD symptom clusters, avoidance/numbing symptoms were the strongest predictors of interpersonal (i.e., relationship with friends), social (i.e., social impairment and global social adjustment), and occupational functioning and overall life satisfaction after controlling for other Axis I conditions. Hyperarousal symptoms most strongly predicted global severity, subjective distress, and global functioning. Reexperiencing symptoms were not uniquely predictive of any measures of functional impairment or severity. Results of this study are ambiguous and difficult to interpret due to the combining of avoidance and numbing symptoms. However, although the impact of avoidance/numbing symptoms was not examined separately, it does suggest that this collection of symptoms is particularly relevant to veterans’ overall life satisfaction and interpersonal/social and occupational functioning.
In another investigation, Guerra and Calhoun (2011) evaluated the role of numbing symptoms of PTSD and suicidal ideation in a sample of returning OEF/OIF veterans who agreed to participate in a research investigation on postdeployment mental health. Results indicated that a positive diagnosis of PTSD or MDD was uniquely associated with increased suicidality. Furthermore, logistic regression analyses revealed a significant association between PTSD diagnosis and increased suicidality in the presence and absence of MDD after controlling for combat exposure and history of suicide attempts. A nonsignificant trend indicated that higher suicidality was associated with a comorbid diagnosis of PTSD and MDD. Based on a four-factor numbing model of PTSD, numbing symptoms were the only PTSD cluster to significantly predict suicidality among PTSD-diagnosed patients (OR = 3.8). Most recently, Pietrzak and colleagues (2010) found a relationship between the dysphoria factor model of PTSD and a number of important psychosocial outcomes among a sample of OEF/OIF veterans who completed a large questionnaire battery through the mail. Specifically, dysphoria symptoms were strongly associated with a number of important mental health variables, such as greater psychosocial difficulties (i.e., family, peer, work, financial, and school difficulties), increased risk of depression and alcohol use problems, reduced psychological resilience (i.e., hardiness, purpose/control, leadership, effort/perseverance, and spirituality), reduced perceptions of postdeployment social support, increased suicidal ideation and perceptions of stigma and barriers to care, and greater mental health service utilization.
In sum, growing evidence consistently supports the notion that numbing/dysphoria symptoms of PTSD may influence a number of important aspects of Iraq and Afghanistan veterans’ psychological adjustment. In particular, results from the reviewed studies suggest that numbing/dysphoria symptoms may play a prominent role in the presence and severity of multiple aspects of psychosocial functioning such as suicidality, the presence of comorbid conditions, and mental health service utilization. In addition, results from the studies of Shea et al. (2010) and Pietrzak et al. (2010) corroborate prior findings demonstrating a link between numbing/dysphoria symptoms and significantly compromised interpersonal functioning. Reconsidering conventional PTSD symptom groupings then is not merely a matter of conceptual and definitional clarity. It would appear that this symptom cluster uniquely predicts a number of untoward and functionally impairing adjustment difficulties that can emerge in the wake of combat exposure.
Implications for Treatment
Given the prominent detrimental impacts of numbing and dysphoria symptoms of PTSD on physical health and psychological and interpersonal functioning among veteran populations, efforts aimed at improving the development and dissemination of effective treatment interventions aimed at targeting this collection of symptoms is of great importance. Prolonged Exposure (PE; Foa, Hembree, & Rothbaum, 2007) and Cognitive Processing Therapy (CPT; Resick & Schnicke, 1993) have been described as first-line treatments for PTSD by the National Center for Posttraumatic Stress Disorder (Hamblen, Schnurr, Rosenberg, & Eftekhari, 2010). The primary objective of PE is to facilitate the confrontation of avoided trauma-related stimuli via imaginary and in vivo exposure exercises, whereas CPT aims to identify and modify distorted trauma-related beliefs via in-session dialogue and between-session written exercises. Both treatment approaches have garnered considerable empirical support demonstrating their efficacy in reducing PTSD symptoms (e.g., E. B. Foa et al., 1999; Resick, Nishith, Weaver, Astin, & Feuer, 2002).
However, although effective in treating the full range of PTSD symptoms, these interventions were not specifically designed to target the emotion regulation difficulties and impaired interpersonal functioning associated with numbing/dysphoria symptoms of PTSD. Furthermore, there is some evidence to suggest that prominent numbing and dysphoria symptoms observed at treatment initiation are associated with a diminished response to cognitive-behavioral treatments for PTSD (Taylor et al., 2001). In addition, significant residual symptoms present after successful treatment in the context of PE/CPT randomized controlled trials. Therefore, although conventional PTSD treatments are associated with large effect size symptom decrements, it is clear that additional supplemental strategies should be entertained and may be useful in conjunction with existing conventional treatments for PTSD. Fortunately, a number of well-established evidence-based approaches exist that may be beneficial for veteran populations experiencing distress stemming prominently from numbing/dysphoria symptoms of PTSD. Although it may not be the case that alternate interventions should be implemented in place of or will be superior to conventional trauma-focused PTSD treatments, they may be useful adjuncts to consider.
In certain cases, the sequential use or incorporation of alternate evidence-based treatment approaches may be particularly valuable in targeting numbing symptoms and associated impairments when working with Iraq and Afghanistan veteran populations. Treatment interventions specifically aimed at enhancing mood regulation and broadening emotional experience may be especially useful in addressing negative/restricted affect and anhedonia associated with numbing/dysphoria symptoms of PTSD. For example, behavioral activation (BA) strategies are effective at improving depression and dysphoria (Dimidjian et al., 2006; Jacobson et al., 1996), and there is preliminary support for BA as a treatment for PTSD (Jakupcak et al., 2006; Jakupcak et al., 2010b). BA strategies have also been successfully used as interventions to reduce nicotine use (MacPherson et al., 2010) and other substance abuse (Magidson et al., 2011). PTSD patients with prominent numbing/dysphoria symptoms may be taught to identify common external (e.g., interpersonal conflict or stress at work) or internal triggers (feelings of detachment, anger, or anxiety) to avoidant coping behaviors, such as smoking or alcohol/drug use, and encouraged to instead practice activation with pleasant or rewarding activities as a means to altering their mood states.
In addition, given the association between increased suicidality and numbing/dysphoria symptoms of PTSD (Guerra & Calhoun, 2011; Pietrzak et al., 2010), psychological interventions aimed at targeting emotion dysregulation may also be of particular value among recently returning veteran populations. In fact, numbing/dysphoria symptoms of PTSD have been linked to perceived emotional regulation capabilities among veterans with military-related PTSD (Price, Monson, Callahan, & Rodriguez, 2006). Therapies such as Dialectic Behavioral Therapy (Linehan et al., 2006), Skills Training in Affective and Interpersonal Regulation (STAIR; Cloitre, Koenen, Cohen, & Han, 2002), or acceptance-based emotion regulation groups (Gratz & Gunderson, 2006) have been shown to reduce high-distress behaviors, such as suicidal ideation and parasuicidal and suicidal acts of self-harm. Therapeutic strategies aimed at enhancing emotion regulation skills may be introduced early into treatment for veterans with PTSD who are at elevated risk for suicide or self-harm behaviors (Jakupcak & Varra, 2011) or used in concert with trauma-focused therapies, such as PE, to target emotional dysregulation (Becker & Zayfert, 2001; Cloitre et al., 2002; Harned & Linehan, 2008).
An advantage of interpersonally focused treatments, such as STAIR, is that they may also more optimally address the prominent relationship difficulties experienced by returning veterans, as reviewed above. Other useful interventions include evidence-based couple’s therapy approaches, such as Integrative Behavioral Couple Therapy (IBCT; Jacobson & Christensen, 1998), which focuses on increasing emotional acceptance and intimacy and creating behavior change between partners. In particular, interventions aimed at enhancing social skills and communication and may be useful in promoting improved social functioning and facilitating Iraq/Afghanistan veterans in better accessing their social support networks, contributing to their recovery from PTSD and reintegration to their communities. In fact, there is some evidence to suggest that focusing on interpersonal difficulties may yield generalized improvement across symptom clusters (Bleiberg & Markowitz, 2005). In addition, therapeutic efforts aimed at enhancing posttraumatic growth by promoting positive psychological change, such as strengthening the quality of interpersonal relationships and reprioritizing life values may also be useful, as numbing symptoms have been found to be negatively related to measures of posttraumatic growth (Hagenaars & van Minnen, 2010).
Discussion
Numbing/dysphoria symptoms of PTSD have been found to be uniquely associated with a number of adverse outcomes among Iraq and Afghanistan veteran populations. Findings from studies conducted with veterans from recent conflicts have demonstrated positive associations between numbing/dysphoria severity and greater engagement in health-risk behaviors, impaired interpersonal functioning, and poorer psychological adjustment. Specifically, some evidence suggests that numbing/dysphoria symptoms of PTSD play a significant role in the chronicity of PTSD symptoms, comorbidity with other trauma-related disorders, mental health service utilization, suicidality, and overall quality of life (Guerra & Calhoun, 2011; Pietrzak et al., 2010; Shea et al., 2010). In addition, results from a growing number of studies suggest that numbing/dysphoria symptoms play a prominent role in veterans’ interpersonal functioning, specifically in regard to the quality of intimate and family relationships (Erbes et al., 2011; Pietrzak et al., 2010; Sayers et al., 2009; Shea et al., 2010).
It is unclear whether resulting severity of PTSD-related distress and psychosocial impairment is due to the long-term effects of PTSD, such as increased avoidance or withdrawal behavior over time, or generalized disturbances in emotionality. For example, increased distress and relationship dissatisfaction may be a consequence of compromised ability of veterans with PTSD to experience positive emotions and high negative emotionality (Litz & Gray, 2001). Veterans’ increased negative emotionality may hinder their ability to communicate effectively with family members or individuals at their workplace. Similarly, high levels of negative emotion may maintain negative mood states and compromise motivation, self-efficacy, and ability to engage in other adaptive, approach-related behavior. Some evidence suggests that dysphoria symptoms may be linked to greater use of emotion-focused coping behavior (Baschnagel, Gudmundsdottir, Hawk, & Beck, 2009), which has generally been associated with increased distress in PTSD samples (e.g., Baschnagel et al., 2009; Blake, Cook, & Keane, 1992; Nezu & Carnevale, 1987; Tiet et al., 2006). Accordingly, it may be the case that veterans with marked numbing/dysphoria symptoms may engage in maladaptive behavior responses that compound difficulties over time.
Numbing/dysphoria symptoms have also been linked to smoking and alcohol misuse (Cook et al., 2009; Jakupcak et al., 2010a; Pietrzak et al., 2010). It is difficult to speak about the exact mechanisms underlying the association between numbing/dysphoria symptoms and substance use. One possible explanation may be that veterans with PTSD may utilize substances in an effort to regulate mood. For example, Litz and Gray (2001) have noted that patients with PTSD may require more intense positive stimulation to access the full range of emotional experiences. Hence, it may be the case that veterans utilize substances to induce or enhance feelings of pleasure. Alternatively, engaging in substance use may also facilitate numbing of negative emotional responses (Jakupcak et al., 2010a).
Given the significant impact of numbing/dysphoria symptoms on indicators of PTSD severity and associated measures of distress, it is necessary to ensure that numbing/dysphoria symptoms are effectively monitored and targeted in trauma-focused interventions implemented among veteran PTSD populations. Fortunately, a number of effective treatment approaches, such as PE and CPT, exist to address psychological distress associated with PTSD, which may be augmented by alternate evidence-based approaches to target numbing/dysphoria-related difficulties, such as substance use problems, difficulties with emotion regulation, and interpersonal/social functioning. However, additional research is necessary to better identify how best to implement these adjunctive evidence-based techniques in a manner that may be optimally effective in combating the range of difficulties seen with numbing/dysphoria-related distress. In addition, future research efforts should be aimed at elucidating the underlying mechanisms between poorer psychosocial adjustment and numbing/dysphoria symptoms.
As previously noted, findings from the reviewed investigations should be interpreted cautiously. A number of the investigations reviewed relied exclusively on self-report for measures of PTSD symptom severity and other outcome variables. Future investigations should utilize more comprehensive forms of assessment, such as structured clinical interviews, to avoid problems associated with the under- or overreporting of distress, health-risk behaviors, and degree of psychosocial impairment. Furthermore, because this review was specific to Iraq and Afghanistan veteran populations, it will be important for future investigations to evaluate findings presented herein with mixed methodologies and to conduct similar investigations with diverse trauma populations to ascertain the generality of findings reviewed here. In addition, all studies utilized samples comprised primarily of male veterans. Hence, results may not be generalizable to female veteran populations. Future investigations including women veterans would be particularly useful given their increased involvement in recent military operations (Street, Vogt, & Dutra, 2009). In addition, the majority of studies were cross-sectional, making it impossible to determine the direction of relationships between numbing/dysphoria symptom severity and other distress and psychosocial outcome variables. Last, although there is great similarity between numbing and dysphoria models of PTSD and they appear to represent similar constructs of PTSD-related distress, the studies reviewed did not consistently adhere to one specific four-factor model.
In sum, four-factor models of PTSD suggesting the existence of a unique emotional numbing or dysphoria symptom cluster have received considerable support, and numbing/dysphoria symptoms are likely to become increasingly important in the assessment and treatment of posttraumatic distress following upcoming modifications to the classification of PTSD in DSM-V. Similarly, emerging evidence suggests that numbing/dysphoria symptoms play an important role in the health and psychosocial functioning of Iraq and Afghanistan war veterans. Treatment interventions aimed at enhancing mood regulation and the quality of intimate and family relationships may be useful in targeting numbing/dysphoria symptoms in veterans from recent conflicts with PTSD. Future research should be directed toward understanding the mechanisms underlying the relationship between numbing/dysphoria symptoms and poorer health-risk, interpersonal, and psychological outcomes to facilitate the identification of areas for intervention.
Footnotes
Authors’ Note
The views and opinions of authors expressed herein do not necessarily reflect those of the Department of VA. Writing of this manuscript was supported by the VA Advanced Fellowship Program in Mental Illness Research and Treatment, VA Office of Academic Affiliations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of work supported by resources from the VA Puget Sound Health Care System, Seattle, Washington.