
Abstract
Living with a person who experiences mental health problems can have an adverse effect on well-being. The aim of this study is to evaluate the effectiveness of a psychological treatment for relatives of people with mental health problems, byusing an interrupted time-series design. The sample comprised 20 individuals, who completed assessment measures at baseline and 6 months later. Sixteen of these participants then received the treatment and were assessed again at the end of the program. There were no significant changes in outcomes between the baseline and the second assessments done 6 months later and there were significant improvements in well-being following treatment The program shows promise as a treatment for relatives of people with mental health problems and therefore warrants further evaluation in more controlled studies.
Introduction
Families often provide essential community support for people affected by severe mental health problems such as schizophrenia and related disorders. In at least 80% of cases, family members are the primary carers of people with mental health problems, usually in their own homes (Bayés, Arranz, Barbero, & Barreto, 1997). Living with a family member who has severe mental health problems can be very stressful and it is well established that there are high levels of burden in this group of relatives (Martens & Addington, 2001). Research shows that children, parents, brothers, and partners of the people with severe and/or chronic mental health problems are at increased risk of developing mental health problems themselves and show higher rates of emotional disorders (American Academy of Child and Adolescent Psychiatry, 2002; Barrowclough & Tarrier, 1992; Kuipers, Onwumere, & Bebbington, 2010; Palacios-Espinosa & Offir Jiménez-Solanilla, 2008; Rodríguez, Padilla, Caballero, & Rodríguez, 2002; Sánchez del Hoyo & Sanz, 2004; Slade, 2009). Studies suggests that as many as 65% of carers undergo substantial changes in their lives and experience a significant decline in their physical and psychological health. Up to 20% of these individuals will also develop a clinical profile known as “burnout” or “caregiver stress syndrome” (Bayés et al., 1997).
Common sources of stress include patients’ psychiatric symptoms, disruptive behaviors, relatives’ lack of understanding of the patients’ behaviors, patients’ denial of problems, changes in the quality of relationships with patients, disagreements among family members, social marginalization, a lack of support, and financial and legal strains. Relatives also often face difficulties with the health system in terms of accessing services and receiving adequate information about diagnoses and treatments. Furthermore, the patient’s progressive dependence can result in restriction of freedom and loss of past lifestyles. High levels of stress and burden are not only problematic for relatives themselves but they may also have a negative impact on the patients’ living environment and exacerbate symptoms, thus adding a further source of stress (Castle, McGrath, & Kulkarni, 2000; London School of Economics, 2012; Stefani, Seidmann, Pano, Acrich, & Bail Pupko, 2003; Treanor, Lobban, & Barrowclough, 2011).
The potential demands associated with caregiving and the high levels of burden and distress in samples of caregivers highlight the need for increasing support for relatives in their caring role. Currently many family interventions have been developed with the aim of reducing expressed emotion (Budd & Hughes, 1997) or patients’ symptoms by working with caregivers (Perlick et al., 2010). Today, there is a greater emphasis within clinical services on supporting service users and relatives through a process of recovery, and family intervention models have been elaborated to reflect this emphasis. These interventions have typically been delivered in a group format withmultiple caregivers (Perlick et al., 2010), or with individual families including the patient (McFarlane, Dixon, Lukens, & Lucksted, 2003).
Although there is a good evidence base for family interventions in terms of patient outcomes, there is still limited evidence about the effectiveness of programs targeting relatives’ mental health or carers’ well-being; however, the majority of those studies that do assess carers outcomes have found positive results (Lobban et al., 2013). A recent review identified 11 key components of successful family interventions across 50 individual studies (Lobban et al., 2013) evaluating an intervention to support relatives against a control group and in which outcomes for the relatives were reported.
The aim of this study was to run a pilot evaluation of an intervention specifically targeting relatives’ emotional needs, which incorporates key components identified by the recent review. The intervention is delivered in clinical practice on an individual basis. After the intervention, we predicted improvements in the evaluated measures, and significant differences in symptoms were expected to be seen. An additional aim was to study the natural course of relatives’ psychological well-being in the absence of an intervention.
Method
Design
We used an interrupted time-series design. Twenty participants were assessed at baseline and then 6 months later. Following this second assessment, 16 of the participants received the intervention and were assessed again post-treatment.
Participants
The pilot study sample comprised 20 participants seeking psychological support who responded to a call for volunteers made via the local media. The program was provided at no charge to the participants.
Inclusion criteria were (a) aged 18 years or over; (b) living with a person diagnosed by a psychiatrist from a public mental health system, with severe mental health problems, including psychotic disorders, bipolar disorders, severe depression, and addictive disorders; (c) no history of severe mental problems; and (d) informed consent.
Measures
A semi-structured interview was designed to elicit sociodemographic variables, illness characteristics, and variables related to the cohabitation with the mentally ill family member.
The Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1992; Spanish version by González de Rivera, 2002) is a self-administrated assessment of general psychopathology. It consists of 90 questions that are answered on a 5-point Likert-type scale, ranging from 0 (none) to 4 (very much). It measures nine areas of symptoms: somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. It also provides three indices (Global Severity Index [GSI], Positive Symptom Total [PST], and Positive Symptom Distress Index [PSDI]) that reflect the overall severity of the person’s symptoms. Test–retest reliability is .70 and alpha coefficient is .90. The SCL-90-R has been shown to be sensitive to therapeutic changes and may therefore be used for either single or repeated assessments (Derogatis & Unger, 2010).
The State–Trait Anxiety Inventory (STAI) is a commonly used measure of trait and state anxiety (Spielberger, Gorsuch, & Lushene, 1970). It is also often used in research as an indicator of caregiver distress (Lobban et al., 2013). The STAI consists of 20 items assessing trait anxiety and 20 items assessing state anxiety. All items are rated on a 4-point scale (e.g., from almost never to almost always). Higher scores indicate greater anxiety. Internal consistency coefficients for the scale have ranged from .86 to .95; test–retest reliability coefficients have ranged from .65 to .75 over a 2-month interval (Gros, Antony, Simms, & McCabe, 2007).
The Beck Depression Inventory–II (BDI-II) is a 21-item self-administered inventory designed to measure the intensity of depressive symptoms in adults and adolescents (Beck, Steer, & Brown, 1996). Respondents are asked to indicate which statement best describes how they felt during the past 2 weeks including today. Items are rated on a 4-point (0-3) scale, with total scores obtained by summing the ratings for all items. Scores ranging from 0 to 9 are indicative of minimal depression, scores that fall between 10 and 18 are considered to reflect a mild level of depression, scores of 19 to 28 are considered moderate, and a score ranging from 29 to 63 is labeled severe. Test–retest reliability is .75 and the alpha coefficient is .82 (Beck, Steer, & Carbin, 1998).
The Maladjustment Scale (Escala de Inadaptación; Echeburúa, Corral, & Fernández-Montalvo, 2000) is a self-administrated scale. It consists of six items that are answered on Likert-type scales, ranging from 0 (none) to 5 (very much). The scale reflects the degree to which stressful situations affect different areas of the person’s daily life: work, social life, leisure, relationship, and family life. Total scores range from 0 to 30, with higher scores indicating greater maladjustment. A score greater than 2 on each item denotes maladjustment. The cutoff point of the full scales is therefore 12. The alpha coefficient is .94 (Echeburúa et al., 2000).
The Stress Coping Questionnaire (SCQ; Cuestionario de Afrontamiento del Estrés [CAE]; Sandín & Chorot, 2003) is a self-administrated assessment questionnaire evaluating seven styles of coping focused on the solution of the problem (FSP), negative self-targeting (NST; self-criticism), positive reappraisal (PR), open emotional expression (OEE), avoidance (AVD), seeking social support (SSS), and religion (RLG). It consists of 42 questions that are answered on 5-point Likert-type scales, ranging from 0 (never) to 4 (almost always). Each subscale ranges from 0 to 24 with higher scores on each subscale indicating greater use of that style. The alpha coefficient is .85.
The Rosenberg Self-Esteem Scale (RSE; Rosenberg, 1965) is a self-administrated scale with 10 items designed to measure self-esteem. The alpha coefficient for the scale is .92. Test–retest reliability over a period of 2 weeks reveals correlations of .85 and .88, indicating excellent stability (Robins, Hendin, & Trzesniewski, 2001). The cutoff point of this instrument is 29 (Ward, 1977).
Treatment
The treatment consisted of 10 weekly individual sessions, which were of 1 hr duration. The program was psychologically supported on a cognitive-behavioral approach.
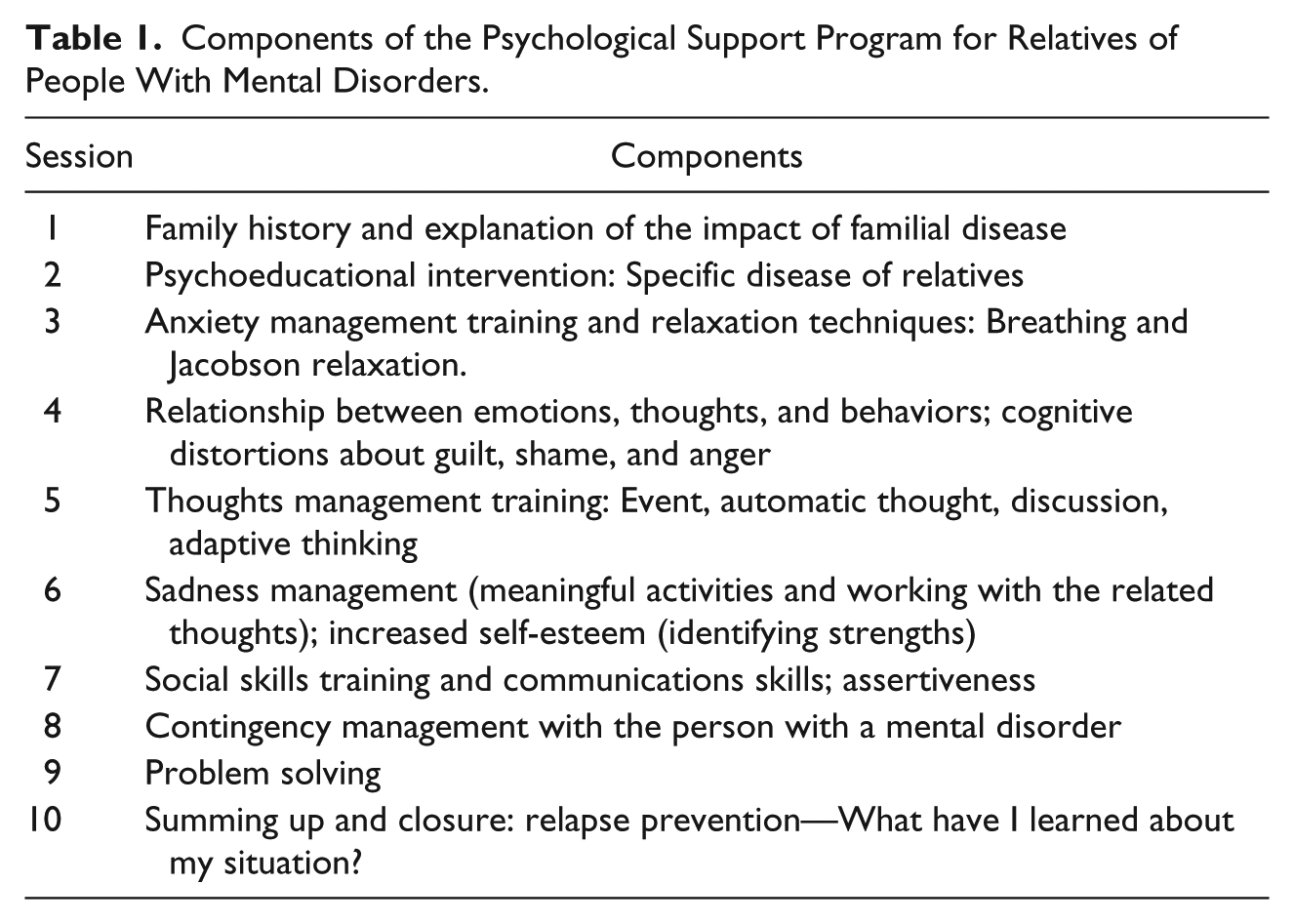
It was delivered by the first author. Participants were all provided with workbooks to use during sessions and between-session homework tasks were assigned. The intervention was tailored to the specific needs of each participant. The intervention comprised 9 of 11 key components identified by Lobban et al. (2013)(psychoeducation, managing problem behaviors, setting realistic expectations, problem-solving training, communication training, stress management for relatives, challenging and unhelpful beliefs, relapse prevention, emotional support). We also included other additional elements that were of potential therapeutic value such as family history and discussion of the impact of having a family member diagnosed with mental health problem, deep breathing and relaxation techniques, work on the cognitive biases associated with emotions such as guilt, shame, anger, and sadness, improving self-esteem by identifying strengths and improving assertiveness. The intervention concluded with a closing session focused on “What have I learned about my situation?” The program is summarized in Table 1.
Components of the Psychological Support Program for Relatives of People With Mental Disorders.
Procedure
The treatment program was carried out in the Unit of Clinical Psychology of the Basque Country University between 2010 and 2012. The study was approved by the University Ethics Committee.
Following informed consent, in which anonymity and confidentiality were emphasized, initial assessments were carried out over two sessions. After a period of 6 months without treatment, the sample was assessed again to verify whether the passing of the time had generated any change in the measures. The third assessments were carried out after treatment. All assessments and treatment sessions were carried out individually by the first author. All the questionnaires were self-reported.
Data Analysis
SPSS 20.0 was used for analyzing the data. Data were analyzed using t-test statistics. We calculated the effect size (Cohen’s d) to estimate the magnitude of differences between the variables. Clinically significant change was also calculated using Jacobson’s clinical significance analysis (Jacobson & Truax, 1991). The reliable change index (RCI) is a statistic that determines the magnitude of change score necessary for a given self-report measure to be considered statistically reliable.
Jacobson and Truax (1991) calculate a RCI for each individual based on the pretreatment score (Xpre), the post-treatment score (Xpost), and the standard error of the difference between two scores (Sdiff). The RCI equals the difference between a participant’s pre-test and post-test scores, divided by the standard error of the difference. The change is considered reliable, or unlikely to be the product of measurement error, if the change index (RCI) is greater than 1.96. Cutoff scores are established for placing participants into one of four categories: recovered (>1.96), improved (1–1.96), unchanged (0.1–1), or deteriorated (<0), depending on the directionality of the RCI and whether the cutoff score was met. When the individual has a change score greater than 1.96, it is assumed that the individual has recovered (McGlinchey, Atkins, & Jacobson, 2002; Ogles, Lunnen, & Bonesteel, 2001).
Results
Sample Characteristics
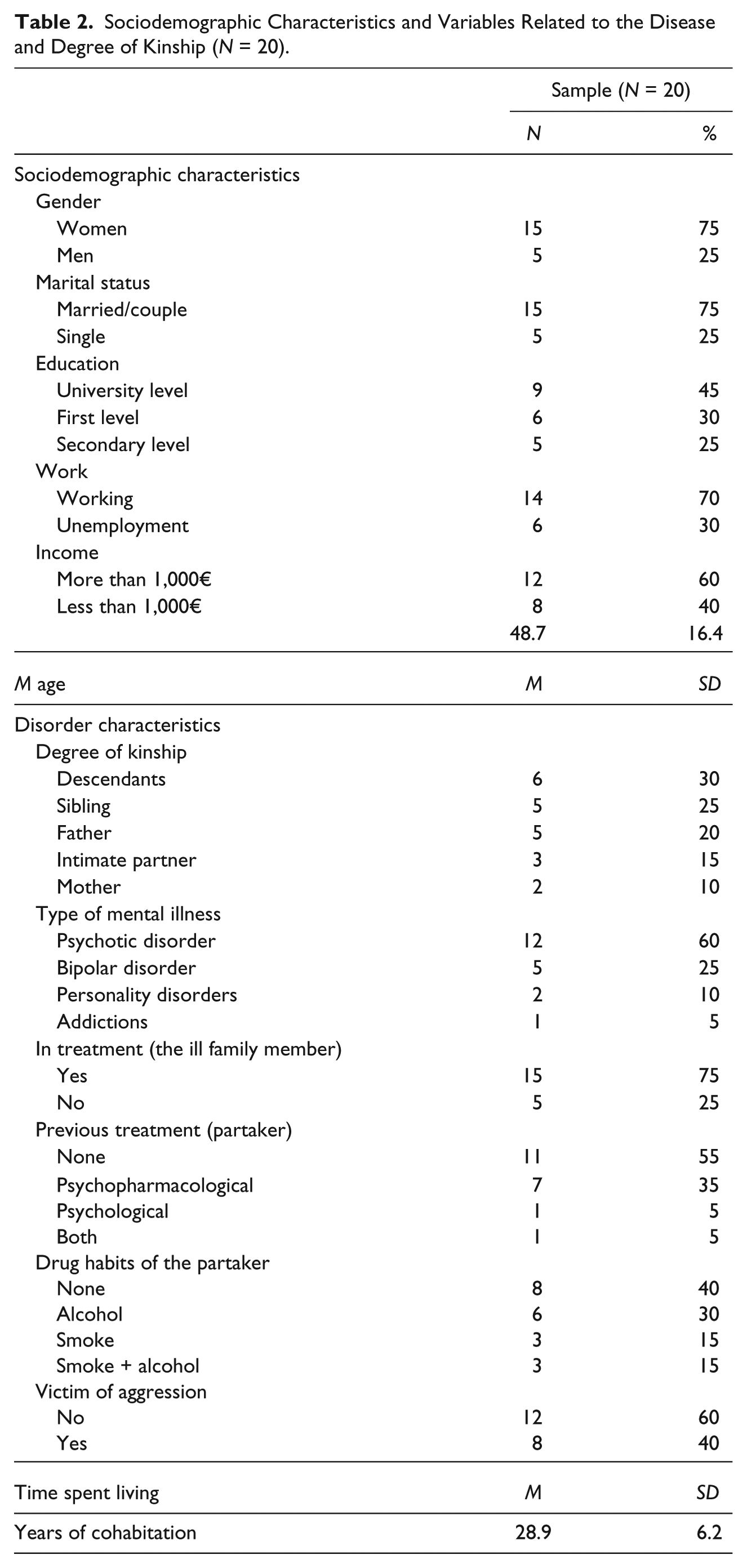
The sample characteristics are summarized in Table 2.
Sociodemographic Characteristics and Variables Related to the Disease and Degree of Kinship (N = 20).
Comparison Between the First and the Second Assessments
In comparison with rates in the general population, participants had scores well above the 80th percentile in all indexes of the SCL-90-R at both the baseline and the 6-month assessments. Overall, the sample also had mild levels of depression, high levels of anxiety, and high maladjustment. The self-esteem level was quite low, below the cutoff found in the general population.
We found no statistically significant differences on any of the measures between the baseline and the 6-month assessments (see Table 3).
Comparison Between the Baseline and the Second Assessments (N = 20).
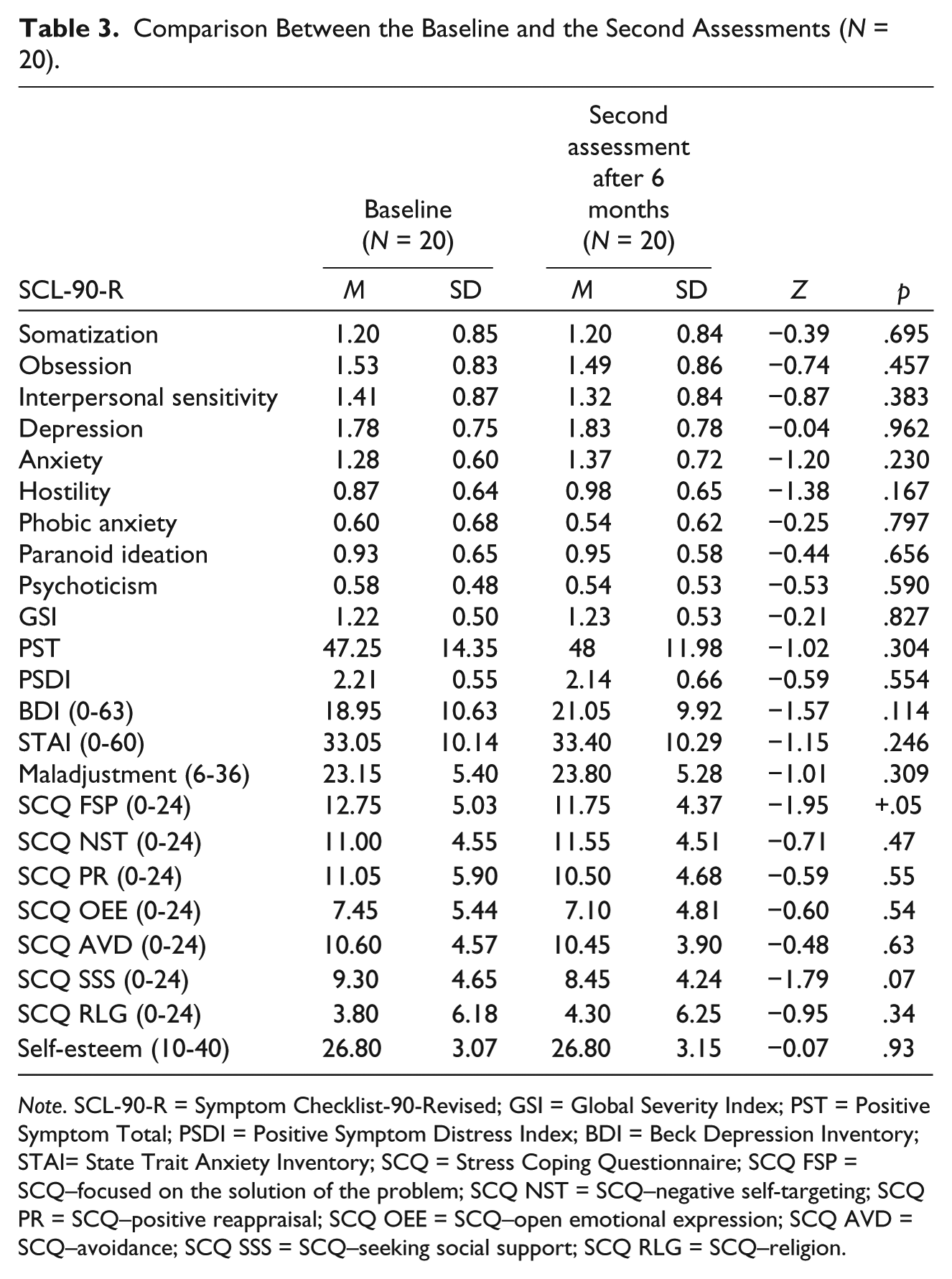
Note. SCL-90-R = Symptom Checklist-90-Revised; GSI = Global Severity Index; PST = Positive Symptom Total; PSDI = Positive Symptom Distress Index; BDI = Beck Depression Inventory; STAI= State Trait Anxiety Inventory; SCQ = Stress Coping Questionnaire; SCQ FSP = SCQ–focused on the solution of the problem; SCQ NST = SCQ–negative self-targeting; SCQ PR = SCQ–positive reappraisal; SCQ OEE = SCQ–open emotional expression; SCQ AVD = SCQ–avoidance; SCQ SSS = SCQ–seeking social support; SCQ RLG = SCQ–religion.
Results of Treatment
Our cognitive-behavioral treatment (CBT) support program was associated with a significant reduction in psychopathology, symptoms of maladjustment, and maladaptive coping, and with an improvement in more adaptive coping and self-esteem (see Table 4)
Psychopathological Features and Psychological Resources Results Between the Second and the Post-Treatment Assessments.
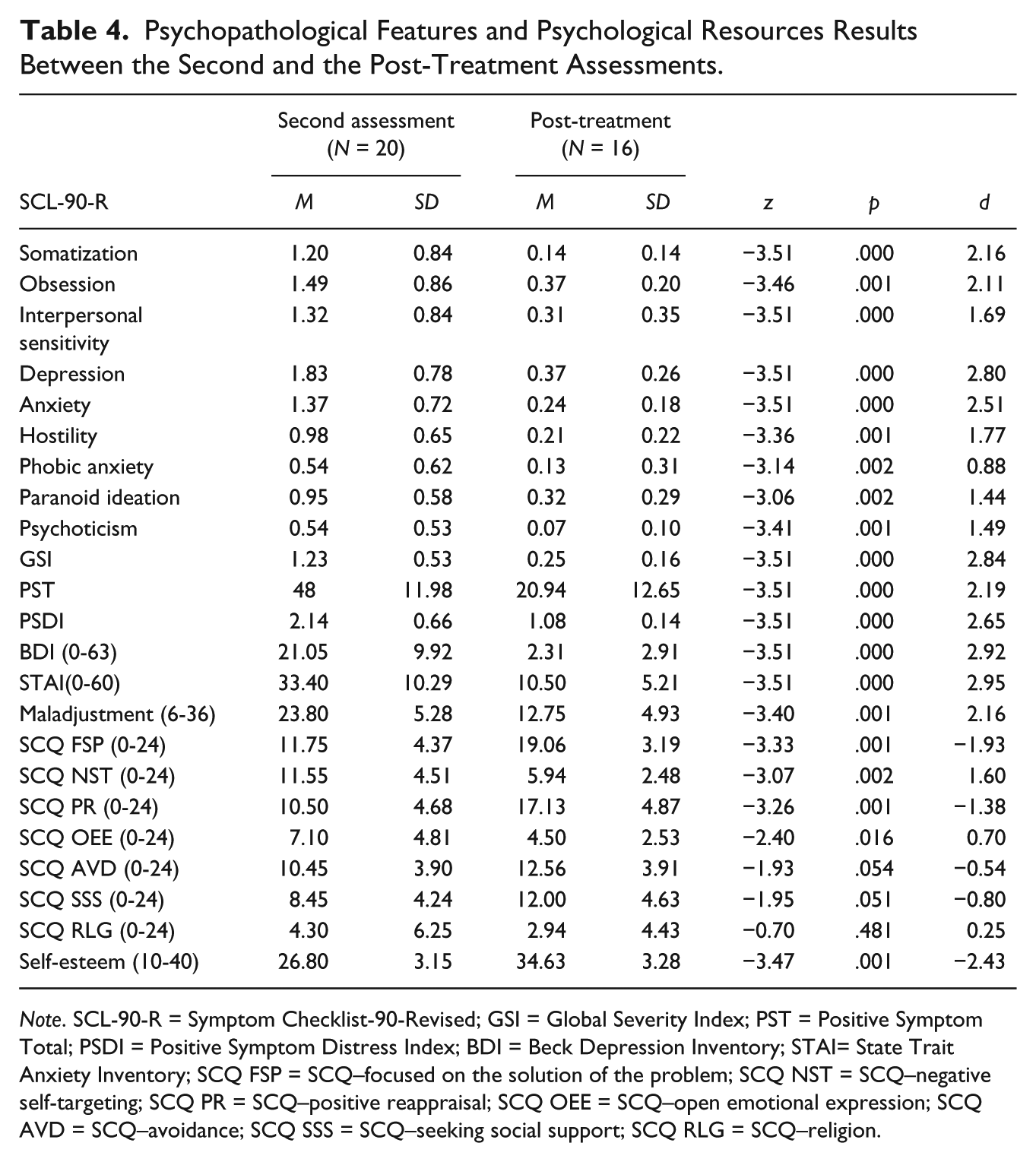
Note. SCL-90-R = Symptom Checklist-90-Revised; GSI = Global Severity Index; PST = Positive Symptom Total; PSDI = Positive Symptom Distress Index; BDI = Beck Depression Inventory; STAI= State Trait Anxiety Inventory; SCQ FSP = SCQ–focused on the solution of the problem; SCQ NST = SCQ–negative self-targeting; SCQ PR = SCQ–positive reappraisal; SCQ OEE = SCQ–open emotional expression; SCQ AVD = SCQ–avoidance; SCQ SSS = SCQ–seeking social support; SCQ RLG = SCQ–religion.
In contrast to the above findings, we found significant differences between the second and the post-treatment assessment. The sample in the post-treatment moment had experienced a statistically significant improvement in their symptoms on SCL-90-R and in depression and anxiety symptoms, as well as a reduction in maladjustment. This is corroborated by the effect size, which was very high according to Cohen’s criteria.
We found significant increases in adaptive coping, such as in coping FSP, positive reappraisal, and seeking social support, and significant decreases in less adaptive methods of coping, such as negative self-targeting, open emotional expression, and religion. We also found statistically significant improvements in self-esteem. The effect size of the differences was high again, according to Cohen’s criteria.
Clinical Significance: Reliable Change Index
Between the baseline and the second evaluation, after 6 months without treatment, only two subjects (5th and 18th) improved on the waiting list, while the remainder deteriorated (see Table 5).
Reliable Change Index.
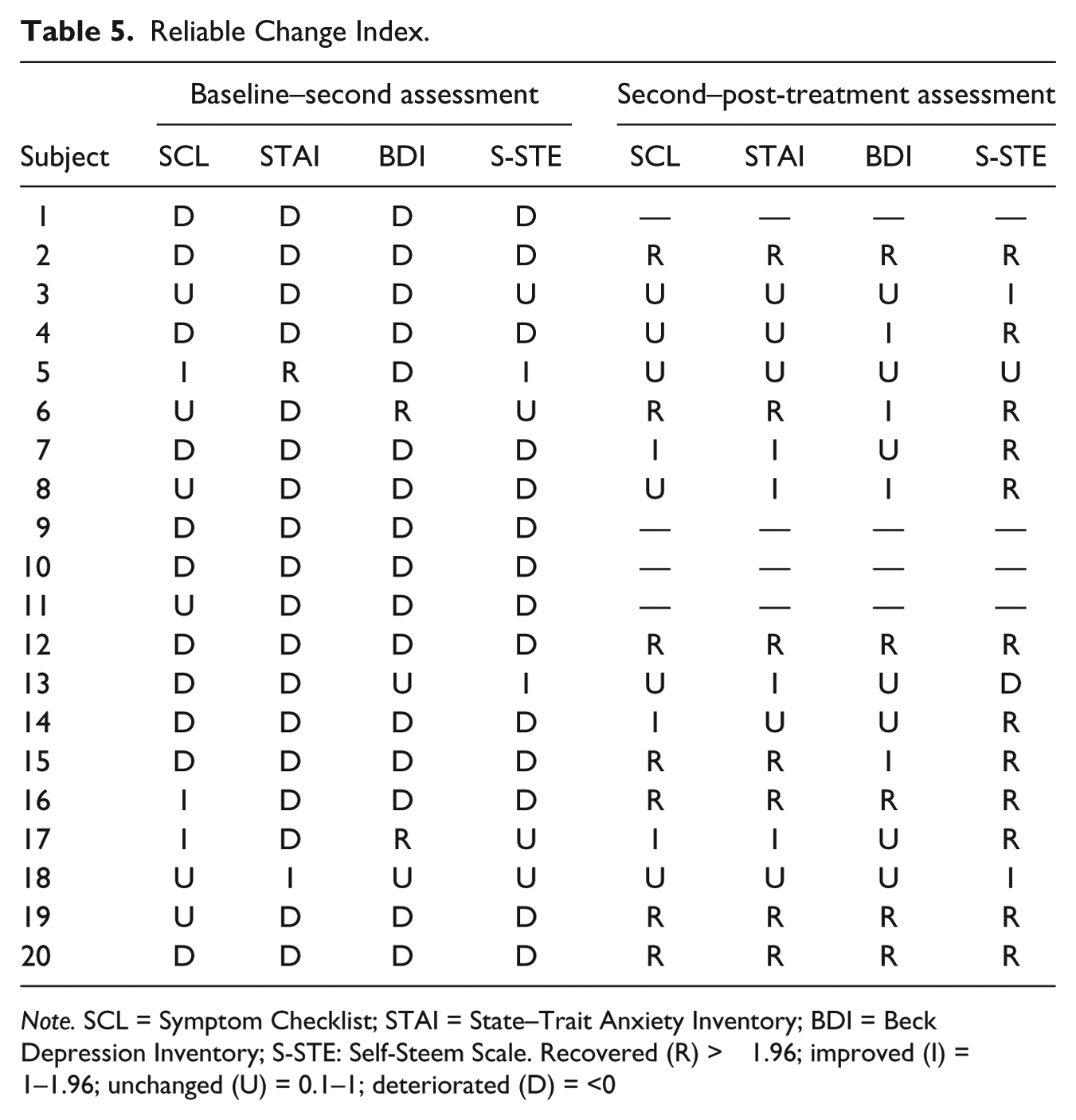
Note. SCL = Symptom Checklist; STAI = State–Trait Anxiety Inventory; BDI = Beck Depression Inventory; S-STE: Self-Steem Scale. Recovered (R) > 1.96; improved (I) = 1–1.96; unchanged (U) = 0.1–1; deteriorated (D) = <0
There were four participants who opted not to receive the treatment as they reported that they felt worse during the waiting period and wanted to seek a more immediate treatment.
Conversely, between the second and the post-treatment assessments, 75% of the treated patients were classified as R (recovered) (subjects 2,6,12,15,16,19,20) or I (improved) (subjects 4,7,8,14,17) and one was classified as D (deteriorated) (subject 13). Subjects 5th and 18th maintained the change achieved on the waiting list.
Discussion
There are only 10 previous studies describing individualized treatments specifically for relatives of people with mental health problems (Lobban et al., 2013). Generally, the most reviewed family interventions programs are in group format and are primarily psychoeducational. In addition, many of them are aimed at reducing the emotion expressed focused on the person with mental health problems and not on reducing symptoms in caregivers (Dixon et al., 2011).
The prevalence of women in the sample was much higher (approximately 75%) than men. This might reflect the possibility that the caregiving role usually falls upon women (Goodman & Tully, 2006; Kuipers et al., 2010), but it might also be that women are more likely to seek treatment. The mean length of time that patients and relatives had been living together was 29 years, and in 25% of the cases, the family member with mental health problems was not receiving any treatment. In most reviews, the median duration of untreated disorders in the last 12 months is higher; for example, for schizophrenia, including other non-affective psychosis, it is reported to be 32.2%. For affective disorders, it is reported to be 56.3% for depression and 50.2% for bipolar disorder (Kohn, Saxena, Levav, & Saraceno, 2004).
Consistent with previous studies, we found high levels of emotional distress in our sample (Barrowclough & Tarrier, 1992; Dixon & Lehman, 1995; Kuipers et al., 2010). Previous research and our waiting list control suggest that, without treatment, symptomatology remains or even worsens, thus highlighting the need to provide psychological support programs for families (Armeli, Gunthert, & Cohen, 2001; Ellis, 2001; London School of Economics, 2012; Park & Fenster, 2004).
Our CBT support program was associated with a significant reduction in psychopathology, symptoms of maladjustment, and maladaptive coping, and with an improvement in more adaptive coping and self-esteem. These results confirm the usefulness of such programs, in addition to other similar programs described in previous research (Penedo et al., 2006; Steinhardt & Dolbier, 2008; Tedeschi & Kilmer, 2005). From a clinical point of view, following treatment, 75% of the participants were considered improved. However, there were still 25% of relatives who did not show a significantly clinical improvement. Further work should identify factors associated with poor responses to the treatment and how the approach might be adapted to better meet the needs of these “non-responders.”
This study was a pilot so was limited by the small sample size, because the assessor and interventionist was the same person, and all assessed efficacy outcome measures were self-report and the participants were not blind to condition/study phase. Likewise another limitation was to have only a 6-month test–retest period to assess the natural course of symptoms. There were also no follow-up assessments to determine whether the positive findings were maintained in the long term. The promising results of this pilot do, however, justify larger and more controlled evaluations of the intervention.
In conclusion, the results of this study, although positive, should be verified by further research. This topic is of great interest due to the high prevalence rates of severe mental health problems and high levels of burden in those who care for them (National Institute for Health and Clinical Excellence [NICE], 2009). Although this is a pilot study, the results highlight that it is the program’s potential benefits in alleviating the distress of families who are living with people affected by severe mental disorders.
Footnotes
Declaration of Conflicting Interests
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research described here has been supported by a Basque Government Grant (IT-430-10) and by a scholarship of the Basque Government.