
Abstract
Technology-aided programs have been reported to help persons with disabilities develop adaptive responding and control problem behavior/posture. This study assessed one such program in which choice of stimulus events was used as adaptive responding for three adults with multiple disabilities. A computer system presented the participants stimulus samples. For each sample, they could perform a choice response (gaining access to the related stimulus whose length they could extend) or abstain from responding (making the system proceed to the next sample). Once choice responding had strengthened, the program also targeted the participants’ problem posture (i.e., head and trunk forward bending). The stimulus exposure gained with a choice response was interrupted if the problem posture occurred. All three participants successfully (a) managed choice responses and access to preferred stimuli and (b) gained postural control (i.e., reducing the problem posture to very low levels). The practical implications of those results are discussed.
Keywords
Introduction
A primary concern about persons with intellectual and sensory-motor disabilities who are in a wheelchair is their low level of activity engagement (Anderson & Heyne, 2010; Gaskin, Andersen, & Morris, 2012; Lancioni, Sigafoos, O’Reilly, & Singh, 2013; Rimmer & Marques, 2012; Shih, 2011; Tam, Phillips, & Mudford, 2011; Taylor & Hodapp, 2012). Given their motor impairment and tendency to be passive, they remain dependent on others for any interaction with the environment and access to environmental stimulus events (Hassiotis et al., 2011; Lancioni, Sigafoos, et al., 2013; Rigby, Ryan, & Campbell, 2011). This condition is greatly unsatisfactory because it emphasizes their marginality (absence of a role) and fails to ensure that they receive adequate stimulation inputs. For example, they might be provided with excessive or insufficient levels of stimulation; they might also receive stimulation that is low in their range of preferences. One approach to alleviate this situation may involve the use of microswitches (i.e., sensors that can be activated with minimal motor behaviors) generally linked to computer devices (Holburn, Nguyen, & Vietze, 2004; Lancioni, Sigafoos, et al., 2013; Lancioni, Singh, O’Reilly, Sigafoos, & Oliva, 2014; Mechling, 2006; Tam et al., 2011). Such technology may empower the persons to successfully engage with preferred environmental stimulation on their own (Lancioni et al., 2014).
A second concern about a number of these persons is their display of problem behaviors (e.g., hand mouthing and eye poking) or problem postures (e.g., head forward bending) (Hayes, McGuire, O’Neill, Oliver, & Morrison, 2011; Lambrechts & Maes, 2009; Lancioni et al., 2008; Lancioni, Sigafoos, et al., 2013; Lancioni, Singh, et al., 2013; Poon, 2012; Poppes, van der Putten, & Vlaskamp, 2010). The negative implications of problem behaviors such as hand mouthing or eye poking can be physical and social/adaptive. Indeed, those behaviors can produce sores and infections, interfere with adaptive responses, and damage the persons’ social image (Lancioni, O’Reilly, et al., 2013). Problem postures can have similarly negative implications. For example, head and trunk forward bending can (a) contribute to weaken the persons’ neck, chest, and stomach muscles with adverse respiratory and alimentary consequences, and (b) hinder their adaptive responding and social image (Lancioni, Singh, et al., 2013). Conventional strategies to deal with problem behaviors and postures include, among others, differential reinforcement of alternative behaviors, differential reinforcement of other behavior, noncontingent reinforcement, and response cost (Kazdin, 2001; Pierce & Cheney, 2008).
Over the last decade, encouraging evidence has been reported about the possibility of targeting both types of concerns within single technology-aided programs that combine a computer system with microswitches for monitoring adaptive responding and problem behavior/posture (Lancioni, O’Reilly, et al., 2013; Lancioni, Singh, et al., 2013; Lancioni et al., 2008; Lancioni, Singh, et al., 2007). For example, Lancioni, O’Reilly, et al. (2013) successfully used one such program to help a 19-year-old man enhance his pointing to visual cues on a computer screen and decrease his hand mouthing. The microswitches for monitoring the pointing response and hand mouthing (i.e., optic sensors on the computer screen and at the man’s neck) were linked to a computer system that regulated all stimulation events. During the initial phase of the program, the man received stimulation for each pointing response, irrespective of his problem behavior. During subsequent phases of the program, stimulation was available only for pointing responses performed in the absence of the problem behavior. Moreover, such stimulation lasted the scheduled time only if the problem behavior did not appear during the stimulation interval. Whenever it did, the stimulation was interrupted. Lancioni, Singh, et al. (2013) successfully used a similar program to help a 10-year-old child increase his interaction with objects and reduce his head forward tilting.
The programs so far reported have targeted simple forms of adaptive responding (e.g., pointing to or touching specific objects) leading to preselected types of stimulation and then combined them with control of problem behavior/posture. Simple forms of adaptive responding may be most suitable for participants in the profound intellectual disability range. Participants in the moderate/severe intellectual disability range could use more advanced forms of adaptive responding (e.g., operating stimulus choices; Lancioni et al., 2011). Such responding would be more suitable to their level of functioning and more appreciated in their daily context. This study assessed a program in which choice of stimulus events was used as adaptive responding for three adults with multiple disabilities. Once this responding had strengthened, the program also targeted the participants’ problem posture (i.e., head and trunk forward bending).
Method
Participants
The participants (Alan, Brandon, and Stacey) were 42, 37, and 23 years old, respectively, had congenital encephalopathy with spastic tetraparesis or hip and legs impairments, spent their day in a wheelchair, and attended centers for persons with intellectual and multiple disabilities. While in their wheelchairs, their head and trunk tended to be bent forward (i.e., problem posture). Alan was diagnosed with severe visual impairment (but was known to watch and enjoy cartoons), was able to speak using a number of simple recurrent sentences concerning daily events and people interacting with him, and understood spoken sentences concerning daily events and preferred activities. Psychological reports indicated that his intellectual disability was in the moderate to severe range, with an age equivalent for communication of about 5 years (i.e., Vineland Adaptive Behavior Scales: Interview Edition; Sparrow, Balla, & Cicchetti, 1984). He was typically involved in self-care and occupational/recreational activities (e.g., music, swimming, and outdoor excursions) and in physiotherapy.
Brandon presented with total blindness, but produced and understood a number of simple sentences related to daily situations. Psychological reports indicated that his condition (i.e., level of intellectual disability and communication) was similar to that of Alan. As for Alan, Brandon’s daily activities involved self-care and recreational/occupational engagement and physiotherapy. Stacey was totally blind and did not possess any speech abilities. Yet, she was credited with the ability to understand a number of words/phrases connected with preferred stimuli and caregiver’s procedures (e.g., grooming activities). Her positive/affirmative responses to caregiver’s questions related to those stimuli and procedures involved small smiles. Her negative/refusal responses consisted of lack of reactions. Psychological reports rated her level of intellectual disability to be in the severe range. Like the other participants, she also was exposed to a routine of self-care and occupation/recreational activities and physiotherapy.
All three participants were known to have strong interest in music and songs and to have preferences among the large variety of musical pieces available to them. Based on this evidence, families and staff had suggested the use of a technology-aided program that would allow them to make music choice responses (i.e., to determine what to listen to on their own). Once these choice responses had been consolidated, control of the problem posture could be added within the program conditions. Legal representatives had signed a formal consent for the participants’ involvement in the study, which had been approved by a scientific and ethics committee.
Setting, Choice Response, Problem Posture, and Stimuli
Sessions were conducted in a quiet room of the centers that the participants attended. The participants sat in their wheelchairs throughout all sessions. The response for making choices consisted of pushing on a pressure microswitch located to the participants’ left, in line with their wheelchairs’ back. Such a response was viable for all participants and incompatible with the problem posture. Indeed, it required the participants to move their trunk and head upward. The problem posture was defined as head and trunk forward bending. Specifically, it was recorded when the distance between the participant’s shoulders and the upper edge of the wheelchair’s back exceeded 10 cm. Such a distance was automatically monitored via an optic microswitch (i.e., optic sensors placed at the edge of the wheelchair’s back). The stimuli presented to the participants during the sessions consisted of a variety of songs considered to be preferred as well as a few music/song items considered non-preferred. The distinction between preferred and non-preferred was based on previous, systematic observations of the participants’ reactions in relation to brief samples of those stimuli and staff reports (Lancioni et al., 2011). The participants were provided with 7 to 11 sets of 15 stimuli, whose presentation was rotated across sessions. Each set included 12 preferred stimuli and three non-preferred stimuli. The non-preferred stimuli were added as checks for verifying the participants’ choice purposefulness. Purposefulness was implied if the participants showed general avoidance of the non-preferred stimuli and responding to the others (Lancioni et al., 2011).
Technology and Sessions
The technology included a computer system with specific software, and the aforementioned microswitches for the choice response and the problem posture. The computer system served for presenting the stimuli available for the sessions and recording the data. Each session included a set of 15 stimuli (see above). The system presented a sample of each stimulus for about 5 s, and frequently accompanied it with a verbal expression such as “Like it?” during the baseline and the first 8-12 intervention sessions (see “Experimental Conditions and Data Recording” section). If the participants made a choice response (i.e., activated the pressure microswitch) within 6 s from the end of the sample, the computer system recorded the response only (i.e., baseline) or recorded the response and presented the sample-related stimulus for up to 20 s (i.e., intervention phases). A new response within 6 s from the end of a stimulus event led the system to present a new stimulus event that was the continuation or repetition of the previous one (i.e., intervention phases). Abstention from microswitch activation after a stimulus sample or the end of a stimulus event led the system to pause for about 10 s and then present the next stimulus sample of the set available for the session. Generally, two or three sessions occurred per day. A session lasted until all stimulus samples available had been presented or a 40-min period had elapsed, whichever came first.
Experimental Conditions and Data Recording
Each participant was exposed to an ABB1BB1 sequence followed by a post-intervention check (Barlow, Nock, & Hersen, 2009; Lancioni, Singh, et al., 2013). The A represented a baseline phase serving to provide data on the frequency of stimulus samples met with choice responses and the percentage of session time with the presence of the problem posture. The first B phase was directed at establishing successful choice responses. During the sessions of this phase, data recording concerned the (a) frequencies of stimulus samples met with choice responses, (b) frequencies of stimulus events occurred (i.e., stimulus activations caused by choice responses performed in relation to stimulus samples and after the end of previous stimulus events), (c) percentage of session time with the presence of the problem posture, and (d) length of the sessions. The first B1 phase served to extend the intervention to the control of the problem posture (i.e., stimulus events could be interrupted by the occurrence of the problem posture). During the sessions of this phase, data recording concerned the four measures mentioned for the B phase. The second B and B1 phases presented conditions matching those of the initial B and B1 phases and served to determine the relevance of the B1 conditions in promoting postural control. During every fourth session of the second B1 phase, the participants’ indices of happiness (i.e., smiles and excitement expressions) were also recorded (Dillon & Carr, 2007). The same measure was also recorded during 12 10-min control (non-activity) sessions, which were spread across the length of the second B1 phase. The first four measures were automatically recorded via the computer system. Indices of happiness were recorded by research assistants, according to a partial interval system, in which every 10-s observation interval was followed by a 5-s scoring period (Kazdin, 2001). Interrater reliability on indices of happiness was checked in half of the second B1 sessions and of the control sessions in which such measure was recorded (by dividing the intervals with agreements by the total number of intervals and multiplying by 100). The percentages of agreement varied within the 80-to-100 range, with means exceeding 90 for all participants.
Baseline (A)
The participants were provided with the computer system and both microswitches. The computer system presented the stimulus samples and recorded the data as described above. Choice responses were never followed by stimulus events. Prior to each of the four sessions available, the participants were verbally and physically guided to produce a choice response.
Intervention (B)
During the first B phase, conditions were as in the baseline except that (a) a choice response occurring after a stimulus sample led to a 20-s presentation of the matching stimulus (i.e., a stimulus event) and (b) a choice response occurring at the end of a 20-s stimulus event led to a new stimulus event that was the continuation or repetition of the previous one. Stimulus events lasted for the scheduled 20 s, irrespective of problem posture. The phase included 22 sessions for Alan and Stacey and 42 sessions for Brandon. Brandon’s larger number of sessions was due to the fact that they were shorter (i.e., included fewer responses) than those of the other participants (see “Results” section). Those intervention sessions were preceded by one to three practice sessions, during which the participants were guided to produce their choice response (and thus experience the consequences of it) (a) in relation to various samples of preferred stimuli (see above) and (b) after the end of a few 20-s stimulus events (Lancioni, Singh, et al., 2013).
Intervention (B1)
Conditions were as during the B phase with one basic exception. A stimulus event lasted the scheduled 20 s only if the problem posture did not appear during that period. In case it did, the stimulus event was interrupted. This phase (a) included 18 sessions for Alan and Stacey and 31 sessions for Brandon (see B phase), (b) ended after a large reduction of the problem posture had been recorded, and (c) was preceded by one or two practice sessions helping the participants familiarize with the new condition.
Intervention (B)
Conditions were as in the first B phase, but only six or nine intervention sessions occurred with no prior practice sessions.
Intervention (B1)
Conditions were as in the first B1 phase, but 55 to 104 intervention sessions occurred with no prior practice sessions. Moreover, data collection also included indices of happiness.
Control sessions
Twelve 10-min control sessions were available parallel to the second B1 phase (i.e., to determine the impact of B1 conditions on indices of happiness). During the control sessions, each of which was separated of at least 45 min from the nearest B1 session, the participants were in their wheelchairs without specific activity engagement.
Post-intervention check
Following the end of the second B1 phase, the participants continued to receive sessions such as those available within that phase. Ten of those sessions occurring 10 weeks after the end of the second B1 served as post-intervention check (i.e., performance maintenance check).
Results
The participants’ baseline and intervention data are summarized in Figures 1 to 3. The white squares and black circles of the upper panels of the figures represent mean frequencies of preferred stimulus samples met with choice responses and mean frequencies of stimulus events occurred per session over blocks of sessions, respectively. The gray squares of the lower panels of the figures indicate mean percentages of session time with the presence of the problem posture within the same blocks of sessions. Two blocks are used for the baseline phase, and three blocks for each of the B and B1 phases. Within each phase, the blocks are equivalent in numbers of sessions included as specified by the numerals above the symbols of the upper panels.
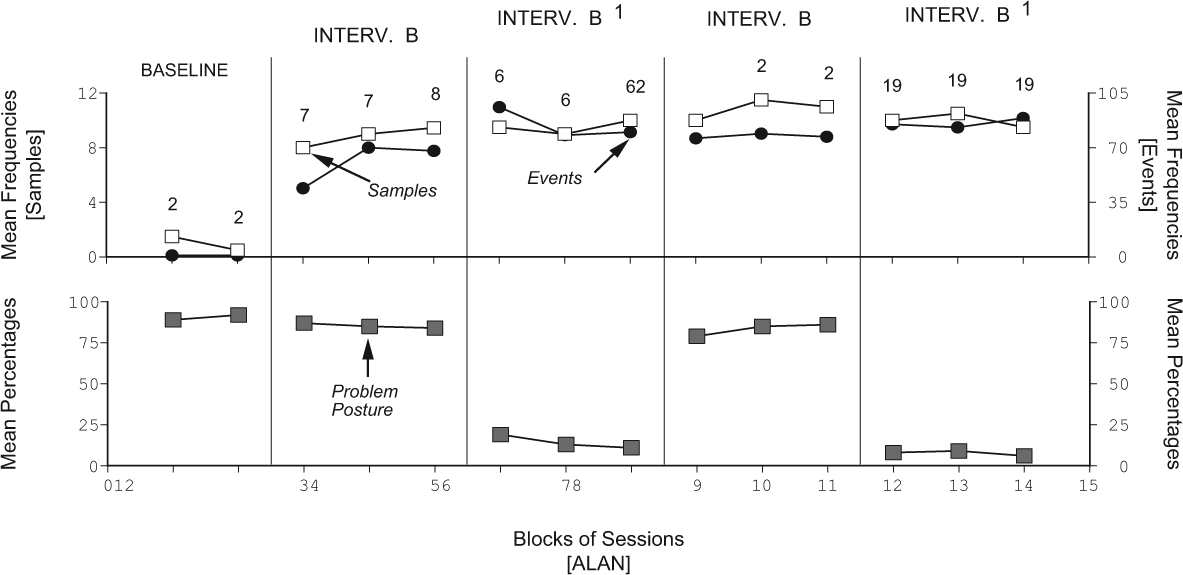
Alan’s data. The numeral above the last point of the first B1 should be 6 (rather than 62). The “2” should be shifted above the first point of the following B phase.
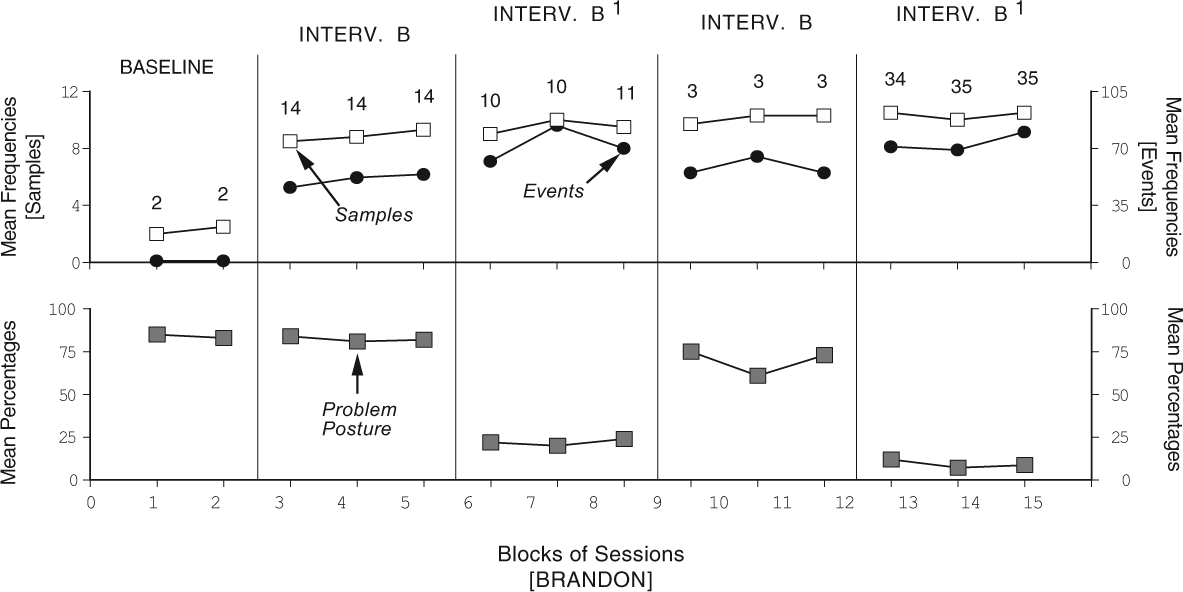
Brandon’s data plotted as in Figure 1.
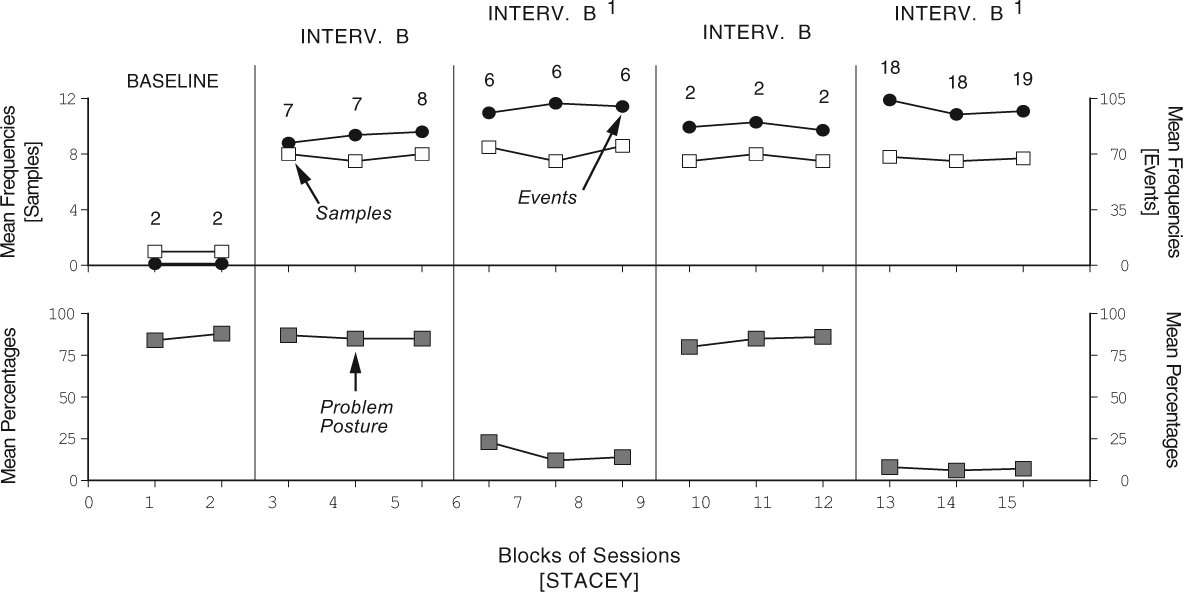
Stacey’s data plotted as in Figure 1.
During the baseline phase, the mean frequencies of stimulus samples the participants met with choice responses were below three per session (see left ordinate of the upper panels). The mean frequencies of stimulus events occurred were zero, as no consequences were available for those responses (see right ordinate of the upper panels). The mean percentages of session time with the presence of the problem posture were above 80 for all participants (see lower panels). During the first B phase, the mean frequencies of preferred stimulus samples the participants met with choice responses were about eight or nine per session. The mean frequencies of stimulus events obtained varied from about 50 (Brandon) to about 80 (Stacey) (i.e., the participants obtained multiple repetitions/continuations of specific events by producing a new response shortly after they ended). The mean frequencies of non-preferred samples chosen per session were negligible, suggesting purposeful choice behavior. The mean percentages of session time with problem posture matched those observed during baseline. The mean lengths of the sessions (not reported in the figures) were about 26, 32, and 38 min for Brandon, Alan, and Stacey, respectively.
During the first B1 phase, the mean frequencies of preferred stimulus samples met with choice responses were comparable with those of the first B phase. The mean frequencies of stimulus events obtained varied from about 70 (Brandon) to about 100 (Stacey). These frequency increases over the means of the first B phase were largely due to the fact that many events were interrupted before the 20-s mark, because of problem posture. In fact, the mean lengths of the sessions were comparable to those recorded during the first B phase. The mean frequencies of non-preferred samples chosen per session continued to be negligible. The mean percentages of session time with problem posture dropped to below 25.
During the second B phase, data were similar to those of the first B. During the second B1 phase, data were similar to those of the first B1 phase, with an additional decrease in the mean percentages of session time with problem posture (i.e., to about or below 10). The mean lengths of the sessions were slightly below 30 min (Brandon) or about 40 min (Alan and Stacey). During this phase, the mean percentages of observation intervals with indices of happiness (not reported in the figures) were clearly above 45. The same percentages were below 10 during the control sessions. The data of the post-intervention check showed continuity with those of the second B1 phase.
Discussion
This study confirms the possibility of targeting an increase in constructive responding and a decrease in problem posture for persons with multiple disabilities, using a single technology-aided program (Lancioni, Singh, et al., 2013; Lancioni et al., 2008). While previous studies had targeted simple forms of response engagement (i.e., exclusively intended as means to access preselected stimulation), the present study taught the participants an advanced form of response engagement that allowed them to choose the stimulation that they wanted to access. The use of an advanced form of constructive responding represents an adaptation of the early programs in this area aimed at making them suitable for persons with moderate to severe intellectual disabilities (i.e., with levels of functioning higher than those of earlier participants; Mitchell, 2012; Tullis et al., 2011). Persons with moderate to severe intellectual disabilities would be expected to find the opportunity to chose among stimuli more challenging and satisfactory than simple stimulation access (Brown, Hatton, & Emerson, 2013; Carter et al., 2013; Fischer, Langner, Birbaumer, & Brocke, 2008). Choice behavior, moreover, would certainly be a more appreciated form of response engagement within their education/rehabilitation context (Agran, Storey, & Krupp, 2010; Cannella, O’Reilly, & Lancioni, 2005; Kazdin, 2001; Lancioni et al., 2011). In light of the general results, a few considerations may be relevant.
First, the program used in this study as well as earlier programs in this area can be considered (a) respectful of the participants’ stimulation requirements (desires) and general developmental conditions, and (b) consistent with the efforts of their education or rehabilitation/care contexts to increase their level of activity and constructive involvement and reduce their inappropriate posture or problem behavior. All these programs start by helping the participants develop adaptive responding to control preferred stimulation and reach a condition of enjoyment (Lancioni, O’Reilly, et al., 2013; Lancioni, Singh, O’Reilly, & Sigafoos, 2009; Szymanski, 2000). Only when this aspect has grown and consolidated, a link is made between this aspect and the problem behavior/posture. The participant is then faced with the options of (a) keeping all that he or she has discovered and is largely enjoying and (b) losing it to maintain his or her consolidated problem behavior/posture. Obviously, a participant who is highly satisfied with the environmental stimulation that he or she has learned to control would be strongly motivated to maintain it and, accordingly, would be eager to inhibit/correct any behavior or posture that may jeopardize it (Borrero et al., 2010; Catania, 2012; Lancioni et al., 2009; Lancioni et al., 2011; Lancioni, Singh, et al., 2013). In other words, the participant would exercise high levels of self-control for relatively long periods of time and repeatedly during the day with positive consequences for his or her well-being and social status (Benedick & Dixon, 2009; McDougall, Evans, & Baldwin, 2010; Singh et al., 2008; Singh et al., 2011). Regarding the issue of enjoyment, it might be important to note that the participants of this study showed signs of it (i.e., frequent indices of happiness) during B1 sessions, in which they managed great self-control.
Second, in line with the above, one might easily argue that the most important variable for determining the successful outcome of a program is the level of enjoyment the participant experiences via his or her adaptive responding and the environmental stimulation following it (Catania, 2012). A high level of enjoyment would be important to build solid adaptive responding and compensate for (a) the loss of the positive (automatically reinforcing) effects produced by most problem behaviors or (b) the physical cost involved in acquiring and maintaining a correct posture. Even so, one should not underestimate the intensity of the problem behavior and the severity of the problem posture. In dealing with a highly problematic posture, for example, one would probably need to proceed stepwise. Initially, it might be safe to ask the participant a partial correction of that posture. Then, one might require increasingly greater levels of correction (i.e., ensuring that this never becomes too taxing; Lancioni, Smaldone, et al., 2007). Similarly, in dealing with a pervasive problem behavior, one might add occasional instances of automatic prompting to the basic program conditions. Automatic prompting would prevent lengthy periods of problem behavior and thus ensure ample opportunities of positive stimulation contingent on the exercise of adaptive responding and control of problem behavior (Lancioni et al., 2010; Pierce & Cheney, 2008).
Third, it might be important here to pinpoint a weakness in the design of the present study. The design used, that is, ABB1BB1 (a) was adequate to determine the impact of the B1 versus the B (i.e., clarifying that the B1 was successful in adding control of the problem posture to the increase in constructive responding), but (b) provided only a basic check for the role of the B in increasing constructive responding from baseline. A complete check would have required a second A phase. For example, one could have used a sequence such as ABABB1BB1 (Barlow et al., 2009; Kennedy, 2005). A second A phase was not used in this study considering that (a) there is large scientific evidence on the importance of the B phase to increase responding (Catania, 2012; Lancioni et al., 2011), and (b) the main question to answer was the differential impact of the B1 condition (Lancioni, Singh, et al., 2013). Even so, further studies in this area would be advised to control for the impact of both the B and the B1 conditions.
Fourth, the technology package used for the study may be viewed as a practically critical component for its implementation (Dalton & Hoyt-Hallett, 2013; Lancioni et al., 2014). Indeed, it would be impossible for staff to monitor adaptive responding and problem behavior/posture simultaneously and deliver the right stimulation according to the prevailing conditions reliably. The use of technology can simplify the intervention process and make it smooth and straightforward. The microswitches can ensure consistent monitoring of adaptive responding and problem behavior/posture and trigger the computer system for highly accurate deliveries and interruptions of the stimulation events. Microswitches would need to satisfy three basic criteria; that is, they would need to be accurate in their functioning, simple to apply for staff, and easily affordable in terms of costs (Dahlin & Rydén, 2011; Lancioni, Sigafoos, et al., 2013). While those used in the present study seem to satisfy the aforementioned criteria, it would be wise to keep track of the rapid developments in the technology area and consider the possibility of adopting new, advantageous alternatives (Borg, Larsson, & Östergren, 2011; de Joode, van Boxtel, Verhey, & van Heugten, 2012; González-Ortega, Diaz-Pernas, Martinez-Zarzuela, & Antón-Rodríguez, 2014; Lancioni, Sigafoos, et al., 2013; Lui, Falk, & Chau, 2012; McNaughton & Light, 2013).
In conclusion, the results of the present study are quite encouraging as to the possibility of adjusting technology-aided programs for promoting adaptive responding and reducing problem behavior/posture in persons with moderate to severe intellectual disabilities. In spite of these results, caution is required given the fact that this study included only three participants and that previous studies in the area also involved a small number of cases. Accordingly, new research would need to extend the evaluation of the programs with additional participants and sound study designs (Barlow et al., 2009; Kennedy, 2005). Research may also involve (a) programs with new forms of adaptive responding and problem behavior/posture, and (b) social validation assessments determining the views and suggestions of staff and service providers about this type of programs (Callahan, Henson, & Cowan, 2008; Lancioni et al., 2006; Luiselli, Bass, & Whitcomb, 2010; Ripat & Woodgate, 2011; Scherer, Craddock, & Mackeogh, 2011).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.