
Abstract
Anxiety sensitivity (AS), defined as the extent to which individuals believe that anxiety-related sensations have harmful consequences, is associated with smoking processes and poorer clinical outcomes among trauma-exposed smokers. Yet the specific mechanisms underlying this association are unclear. Smoking-specific avoidance and inflexibility is a construct implicated in multiple manifestations of mood regulation that may underlie smoking behavior. The current study examined the explanatory role of smoking-specific avoidance and inflexibility in terms of the relation between AS and indices of smoking behavior among trauma-exposed smokers. The sample consisted of 217 treatment-seeking adult smokers (44% female; M age = 37.8; SD = 13.2; age range: 18-65 years), who were exposed to at least one lifetime Criterion A trauma event (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR] Criterion A for trauma exposure). Bootstrap analysis (5,000 re-samples) revealed that AS was indirectly related to the (a) number of cigarettes smoked per day, (b) number of years being a daily smoker, (c) number of failed quit attempts, and (d) heaviness of smoking index among trauma-exposed smokers through its relation with smoking-specific avoidance and inflexibility. These findings provide initial evidence suggesting that smoking-specific avoidance and inflexibility may be an important construct in better understanding AS–smoking relations among trauma-exposed smokers. Future work is needed to explore the extent to which smoking-specific avoidance and inflexibility account for relations between AS and other smoking processes (e.g., withdrawal, cessation outcome) in the context of trauma and smoking comorbidity.
One in 10 smokers have a lifetime history of posttraumatic stress disorder (PTSD; Lasser et al., 2000) and significantly more are trauma exposed (Feldner, Babson, & Zvolensky, 2007). The relations between smoking, traumatic event exposure, and posttraumatic stress (PTS) symptoms are bi-directional and clinically relevant. For example, trauma-exposed individuals compared with individuals without clinical or subclinical PTSD are more likely to be current smokers (Acierno, Kilpatrick, Resnick, Saunders, & Best, 1996), smoke at higher rates (Beckham et al., 1995), and maintain greater levels of tobacco dependence (McClernon et al., 2005). Conversely, higher smoking rates and tobacco dependence levels are related to an increased risk for PTS symptoms among trauma-exposed people (Beckham et al., 1997).
Although smoking and PTS symptoms commonly co-occur and influence one another, there has been little work focused on the underlying explanatory processes of smoking among trauma-exposed smokers.
There is little empirical understanding of the factors among trauma-exposed smokers that govern smoking severity. Yet recent work has suggested anxiety sensitivity (AS), defined as the fear of arousal-related physical and psychological sensations (McNally, 2002; Reiss & McNally, 1985), may be an important explanatory construct in terms of better understanding the smoking–trauma association. This cognitive-based construct is distinguishable empirically and theoretically from trait or state anxiety symptoms and other negative affect states (e.g., depression; Rapee & Medoro, 1994; Zvolensky, Schmidt, & Stewart, 2003). Extant AS research suggests that it serves as a transdiagnostic risk factor for both smoking and trauma, resulting in poorer outcomes in both domains. For example, higher levels of AS are related to greater odds of early lapse (Brown, Kahler, Zvolensky, Lejuez, & Ramsey, 2001) and relapse during quit attempts (Zvolensky, Bonn-Miller, Bernstein, & Marshall, 2006; Zvolensky, Stewart, Vujanovic, Gavric, & Steeves, 2009) as well as increased PTSD symptoms (Keogh, Ayers, & Francis, 2002).
A developing line of research has focused on the role of experiential avoidance and cognitive inflexibility in the maintenance of various forms of psychopathology, including substance use disorders (Chawla & Ostafin, 2007; Hayes, Luoma, Bond, Masuda, & Lillis, 2006; Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Rooted in negative-reinforcement theories of behavior, experiential avoidance is a cognitive–affective regulatory process wherein individuals are unwilling to experience or remain in contact with aversive internal experiences (e.g., thoughts, emotions, memories, bodily sensations, images) and attempt to control the frequency or form of the experiences and the contexts in which they occur. Cognitive inflexibility, however, reflects a lack of ability to disengage attention from one task to another, and thereafter update new task sets (Mayr & Keele, 2000; Monsell, 2003). Specific to smoking, one’s tendency to inflexibly escape or reduce distressing smoking-relevant thoughts, feelings, and bodily sensations is related to the maintenance of smoking (Gifford, 2001, 2002). In fact, decreases in smoking-specific avoidance and inflexibility are associated with increased likelihood of smoking abstinence after treatment (Gifford et al., 2004; Gifford et al., 2011). In addition, research using the Avoidance and Inflexibility Scale (AIS; Gifford, 2001, 2002; Gifford et al., 2002), which taps smoking-specific avoidance and inflexibility, indicates that this construct is related to smoking withdrawal/craving (Farris, Zvolensky, & Schmidt, 2014) and likelihood of abstinence during a quit attempt (Gifford et al., 2004; Zvolensky, Yartz, et al., 2008).
Despite past work, it is presently unknown whether and how smoking-specific avoidance and inflexibility impacts the actual smoking behavior of trauma-exposed smokers in terms of smoking severity (e.g., heaviness of smoking). Moreover, although AS is associated with smoking behavior and experiential avoidance (Kämpfe et al., 2012; Leventhal & Zvolensky, 2014; Zvolensky, Bogiaizian, Salazar, Farris, & Bakhshaie, 2014), it is unclear whether smoking-specific avoidance and inflexibility may explain the relation between AS and smoking severity among trauma-exposed smokers. With this background, the primary aim of the present research was to examine whether smoking-specific avoidance and inflexibility explains the relation of AS and smoking severity among trauma-exposed smokers. It was hypothesized AS would have a significant indirect effect on smoking severity through its relation with smoking-specific avoidance and inflexibility. Smoking severity was indexed via (a) number of cigarettes per day, (b) number of years being a daily smoker, (c) number of failed quit attempts, and (d) heaviness of smoking index (see Figure 1).
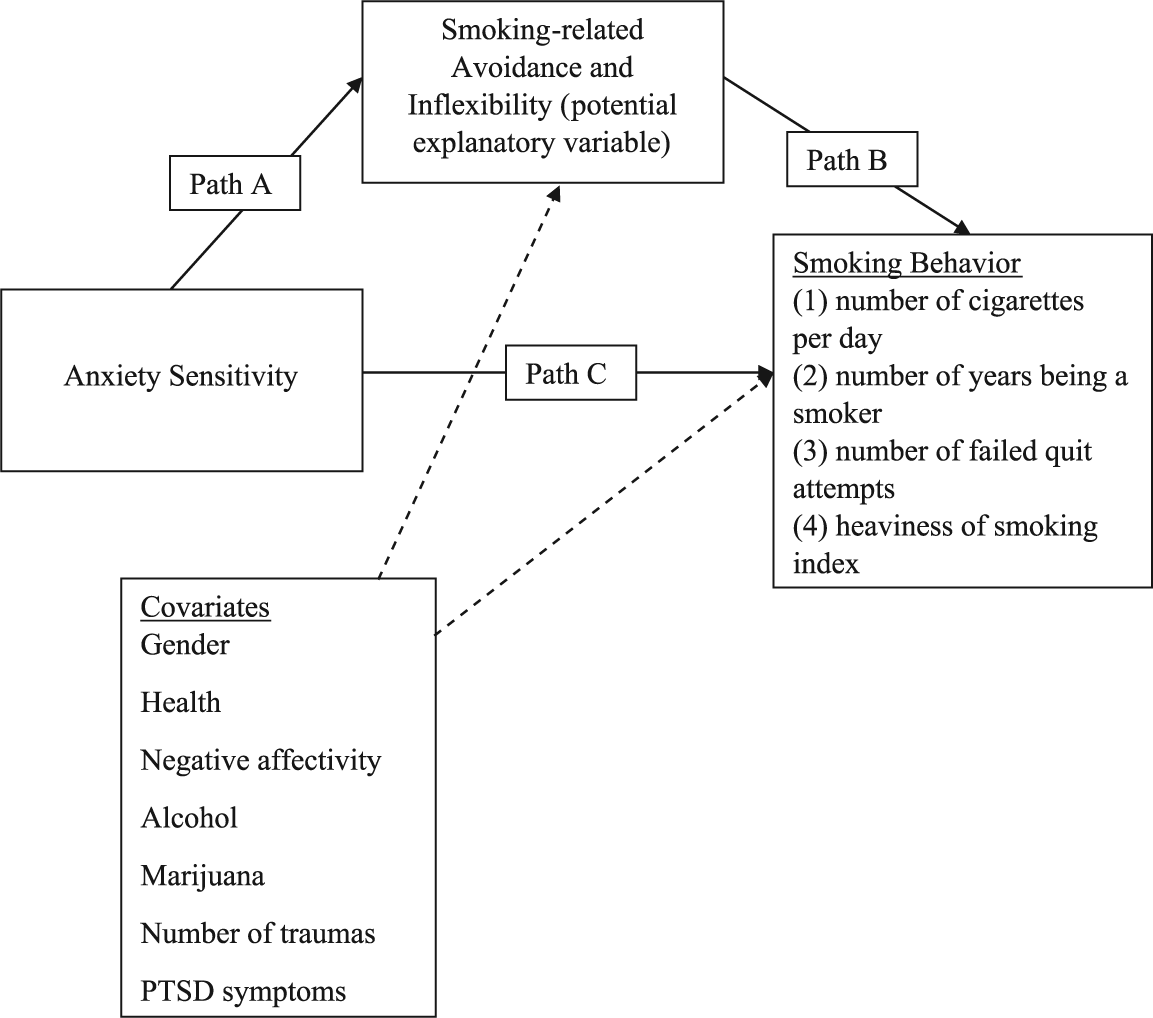
Proposed model: Smoking-related avoidance and inflexibility as a potential explanatory variable in the association between anxiety sensitivity and smoking behaviors among trauma-exposed daily smokers.
Method
Participants
The sample consisted of 217 treatment-seeking adult smokers (44% female; M age = 37.8; SD = 13.2; age range: 18-65 years), who were exposed to at least one lifetime traumatic event. This study is a secondary analysis of data from a larger study (completed) examining the efficacy of two smoking cessation interventions: a novel four (weekly) session smoking cessation behavioral intervention that focused on vulnerability to panic (Panic-Smoking Program) and a standard four (weekly) session smoking cessation program (Bakhshaie et al., 2014; Funk, Zvolensky, & Schmidt, 2011).
Participants were deemed eligible for enrollment in the parent study if they (a) were between 18 and 65 years, (b) were a daily smoker for at least 1 year, (c) currently smoked a minimum of eight cigarettes per day, and (d) reported motivation to quit smoking within the next month. Participants were excluded based on the following criteria: (a) current (past month) use of pharmacotherapy for smoking cessation (except the nicotine patch, which participants were allowed to use during the cessation treatment; i.e., nicotine replacement therapy), (b) limited mental competency and inability to provide informed, voluntary, written consent, (c) endorsement of current or past psychotic-spectrum symptoms via structured interview screening, (d) current suicidality or homicidality, (e) history of significant medical condition, and (f) planning to move in the next 6 months.
For the present investigation, on a theoretical basis, a subsample of parent study was chosen from participants who (a) completed the baseline assessments, (b) reported at least one lifetime Criterion A trauma event (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR] Criterion A for trauma exposure; American Psychiatric Association [APA], 2000]), and (c) had a breath carbon monoxide level of ≤4 parts per million as an objective measure of smoking status (Deveci, Deveci, Açik, & Ozan, 2004; Middleton & Morice, 2000).
Measures
Demographics Questionnaire
Demographic information collected included gender, age, and race.
Structured Clinical Interview–Non-Patient Version for DSM-IV (SCID-I/NP)
Diagnostic assessments of past year Axis I psychopathology were conducted using the SCID-I/NP (First, Spitzer, Gibbon, & Williams, 2007), which was administered by doctoral-level staff or trained research assistants. A random selection of 12.5% of interviews were evaluated (M.J.Z.) for accuracy; there were no cases of diagnostic disagreement.
Smoking History Questionnaire (SHQ)
The SHQ is a self-report questionnaire used to assess smoking history (e.g., onset of daily smoking) and pattern (e.g., number of cigarettes per day; Brown, Lejuez, Kahler, & Strong, 2002). In the present study, the SHQ was used to describe the sample in terms of smoking history and patterns of use. In addition, we used the following items as criterion variables: “Average number of cigarettes smoked during last week” (i.e., smoking rate), “Number of years being a daily smoker,” and “Number of failed quit attempts.”
Fagerström Test for Cigarette Dependence (FTCD)
The FTCD is a six-item scale that assesses individual smokers’ tobacco dependence (Heatherton, Kozlowski, Frecker, & Fagerström, 1991). Scores range from 0 to 10, with higher scores reflecting high levels of physiological dependence on cigarettes. The FTCD has shown adequate internal consistency, positive relations with key smoking variables (e.g., saliva cotinine), and high test–retest reliability (Heatherton et al., 1991). In the present sample, the FTCD total score internal consistency Cronbach’s alpha was .58. For the current study, we used the following items as criterion variables: “How many minutes after you wake do you smoke your first cigarette?” (latency to first cigarette of the day), and “How many cigarettes a day do you smoke?” Both items are scored between 0 and 3. Consistent with previous research (Etter, Duc, & Perneger, 1999), these two items were summed to create a “heaviness of smoking index.”
Carbon monoxide (CO) analysis of breath samples
Biochemical verification of smoking status was completed by CO analysis of breath samples. Expired air CO levels were assessed using a Carbon Monoxide Monitor (Model 3110; Spirometrics, Inc., Auburn, ME, USA).
Medical history form
Current and lifetime medical illnesses and current use of prescribed medication were assessed using a medical history checklist. For current and lifetime medical illnesses, a composite variable was computed for the present study as an index of tobacco-related medical illnesses. Items in which participants indicated having ever been diagnosed (respiratory disease, asthma, heart problems, and hypertension, all coded 0 = no, 1 = yes) were summed to create a total score (observed range from 0 to 4), with greater scores reflecting the presence of multiple markers of tobacco-related illnesses.
Alcohol Use Disorders Identification Test (AUDIT)
The AUDIT is a 10-item self-report measure developed to identify individuals with problematic drinking (Babor, de la Fuente, Saunders, & Grant, 1992). Its score ranges from 0 to 30, with higher scores reflecting more problematic drinking. The AUDIT’s psychometric properties are well documented. In the current investigation, the AUDIT total score internal consistency was good (Cronbach’s α = .89).
Marijuana Smoking History Questionnaire (MSHQ)
The MSHQ is a self-report measure that assesses marijuana smoking rate (lifetime and past month), age of onset at initiation, years of being a regular marijuana smoker, and other descriptive information (e.g., number of attempts to discontinue using marijuana; Zvolensky, Bonn-Miller, et al., 2006). This questionnaire has been used successfully in the past as a descriptor of history of marijuana use (Bonn-Miller, Zvolensky, & Bernstein, 2007; Zvolensky, Bonn-Miller, et al., 2006). In the present study, the item asking about the number of marijuana smoked during the past 30 days (past-month marijuana use) was utilized. The scores for this item range from 0 = no use to 8 = more than once a day.
Positive and Negative Affect Scale (PANAS)
The PANAS is a self-report measure asking participants to rate the extent to which they experience each of 20 different feelings and emotions (e.g., interested, nervous) based on a Likert-type scale that ranges from 1 (very slightly or not at all) to 5 (extremely; Watson, Clark, & Tellegen, 1988). The measure yields two factors (negative and positive affect) with strong psychometric properties (Watson et al., 1988). The Negative Affectivity subscale (PANAS-NA) was used in the current study (Cronbach’s α = .87).
Anxiety Sensitivity Index–3 (ASI-3)
The ASI-3 (Taylor et al., 2007) is an 18-item measure derived, in part, from the Anxiety Sensitivity Index (ASI; Reiss, Peterson, Gursky, & McNally, 1986). Respondents indicate the extent to which they are concerned about possible negative consequences of anxiety-related symptoms (e.g., “It scares me when my heart beats rapidly”). Responses are rated on a 5-point Likert-type scale ranging from 0 (very little) to 4 (very much) and summed to create a total score. The ASI-3 has sound psychometric properties among smokers (Farris et al., 2015). In the current study, internal constancy was excellent (Cronbach’s α = .90).
AIS
The AIS is a 13-item self-reported measure that assesses the link between internal (affective) triggers and smoking (smoking-related avoidance and inflexibility; Gifford et al., 2004). Respondents are asked how they respond to different feelings that encourage smoking (e.g., stress, fatigue), difficult thoughts that encourage smoking (e.g., “I need a cigarette”), and bodily sensations that encourage smoking (e.g., “physical cravings or withdrawal symptoms”). Example of items are “How important is getting rid of [thoughts/feelings/sensations]?” “How likely is it you will smoke in response to [thoughts/feelings/sensations]?” and “To what degree must you reduce how often you have these [thoughts/feelings/sensations] in order not to smoke?” Items are rated on a 5-point Likert-type scale (1 = not at all to 5 = very much), with higher scores reflecting more avoidance and inflexibility when facing difficult smoking-related feelings, thoughts, and sensations. The AIS has displayed good reliability and validity in past work (Farris, Zvolensky, DiBello, & Schmidt, 2015; Gifford et al., 2004). In the present study, the AIS total score was used as proposed mediator variable that showed excellent internal consistency (Cronbach’s α = .94).
Posttraumatic Diagnostic Scale (PDS; Foa, 1995)
The PDS is a 49-item self-report instrument designed to assess trauma exposure and the presence of PTS symptoms based on DSM-IV-TR criteria (APA, 2000). Respondents report whether they have experienced any of the 13 traumatic events (e.g., “natural disaster,” “sexual or non-sexual assault by a stranger”), including an “other” category, and then indicate which event was most disturbing. The PDS assesses Criterion A trauma exposure as well as the frequency of 17 past-month PTSD symptoms for the most disturbing event endorsed (scored 0-3, with 0 signifying not at all/only once and 3 signifying 5 or more times a week/almost always). The severity score of PTS symptoms for PDS is calculated by summing its items (score range of 0-51). The PDS has evidenced generally excellent psychometric properties (Foa, Cashman, Jaycox, & Perry, 1997), including high internal consistency (α = .92) and high test–retest reliability (κ = .74). The PDS was found to have 82% agreement with the SCID-I with regard to PTSD diagnosis (Foa et al., 1997) and good convergent validity (αs = .73, .79) with related measures of depression and anxiety (Foa, 1995). The PDS was utilized to (a) index traumatic event exposure consistent with PTSD Criterion A, (b) establish the total number of trauma exposure types (derived by summing the number of traumatic event types endorsed), and (c) assess PTS symptom severity. In the current study, internal consistency was good (Cronbach’s α = .87).
Procedure
The study participants were adult daily smokers recruited from the community to participate in a large, multisite randomized controlled clinical trial examining the efficacy of two smoking cessation interventions. After responding to study advertisements, individuals were scheduled for an in-person, baseline assessment to evaluate study eligibility. Following written informed consent, participants were interviewed using the SCID-I/NP and completed a computerized self-report battery. The study protocol was approved by the institutional review boards at relevant institutions. The current study is based on secondary analyses of baseline (pre-treatment) data for a subset of the sample, which was selected on the basis of complete data for all studied variables.
Data Analytic Strategy
To test the study hypotheses, bootstrapping techniques were conducted through INDIRECT Macro (Preacher & Hayes, 2008), a computational tool for observed variable mediation analysis. As a non-parametric method, bootstrapping estimates the sampling distribution of an estimator based on re-sampling with replacement. The indirect effects (mediation pathway) were computed for each of the samples, resulting in an empirically generated sampling distribution (Bollen & Stine, 1990; Shrout & Bolger, 2002). We conducted separate models for each criterion variable with AS as the predictor and smoking-related avoidance and inflexibility as a potential mediator (see Figure 1). Covariates included gender, tobacco-related medical illness, alcohol consumption, negative affectivity, past month use of marijuana, PTS symptoms, and number of traumatic event type exposures. Coefficient of determination (R2) was utilized to index the fit of each model. R2 (the square of the coefficient of multiple correlation) measures how well the regression line correlates with the real data (i.e., model fit; Draper & Smith, 1998). We calculated the semi-partial correlations to depict the correlation between the predictor and the criterion variable after removing common variance with other predictors (residualized predictor; Draper & Smith, 1998). Five thousand bootstrap re-samplings were conducted to detect the indirect effects of the proposed predictor on criterion variables through the proposed explanatory variable (i.e., the product of the “beta coefficients” of “Path a” [predicting smoking-related avoidance and inflexibility from AS] and “Path b” [predicting each of the criterion variables from smoking-related avoidance and inflexibility]; i.e., Path ab; Figure 1). Moreover, using multiple regression, the beta coefficients for Paths “c” (the direct path from AS to each criterion variable) and “c’” (the direct path from AS to each criterion variable after controlling for smoking-related avoidance and inflexibility as mediator of the models) were calculated.
A bootstrap confidence interval (CI) of Path ab that does not include zero provides evidence of a significant indirect effect (Hayes, 2009; Preacher & Hayes, 2008). This significant indirect effect is the only criterion required for assessing the mediator function (Hayes, 2009, 2013). Based on recommendations for reducing Type I error (Fritz, Taylor, & MacKinnon, 2012; Hayes & Scharkow, 2013), percentile-based (PB) CIs were used. Completely standardized indirect effects for each significant indirect pathway were presented (Preacher & Kelley, 2011). Finally, the theoretical models for each outcome variable were compared with two alternative models. In alternative Model 1, the proposed predictor and explanatory variables were reversed for each of the five criterion variables; and in alternative Model 2, each criterion variable was proposed to explain the relation between AS and smoking-related avoidance and inflexibility. Comparing alternative models with alternate variable sequences is suggested in cross-sectional studies examining statistical mediation effects as an additional test of the hypothesized order of influence among the study variables in the absence of a prospective study design (Chmura Kraemer, Kiernan, Essex, & Kupfer, 2008; Judd & Kenny, 2010; Preacher & Hayes, 2008).
Results
Descriptive data for all variables included in the models are presented in Table 1. The ethnic distribution of the sample was as follows: 82.8% identified as White/Caucasian, 9.6% as Black/non-Hispanic, 0.8% as Black/Hispanic, 2.8% as Hispanic, 0.8% as Asian, and 3.1% as “Other.” Within the sample, 46.4% met criteria for at least one current (past year) Axis I diagnosis; the most common diagnoses were social anxiety disorder (10.9%), major depressive episode (4.9%), PTSD (4.0%), and generalized anxiety disorder (4.3%). Participants reported smoking an average of 17.2 cigarettes per day (SD = 10.2), smoking their first cigarette at 14.80 years of age (SD = 3.9), and smoking regularly at 17.3 years of age (SD = 4.0). The average score on the FTCD (Heatherton et al., 1991) was 5.2 (SD = 2.3), indicating moderate levels of tobacco dependence (M of breath CO = 21 parts per million, SD = 11.4). AS and smoking-related avoidance and inflexibility were significantly positively correlated with number of cigarettes per day (r = .40, p < .01). Smoking-related avoidance and inflexibility was significantly positively correlated with number of cigarettes per day (r = .18, p < .01) and heaviness of smoking index (r = .14, p < .05).
Zero-Order Correlations Among Theoretically Relevant Variables.
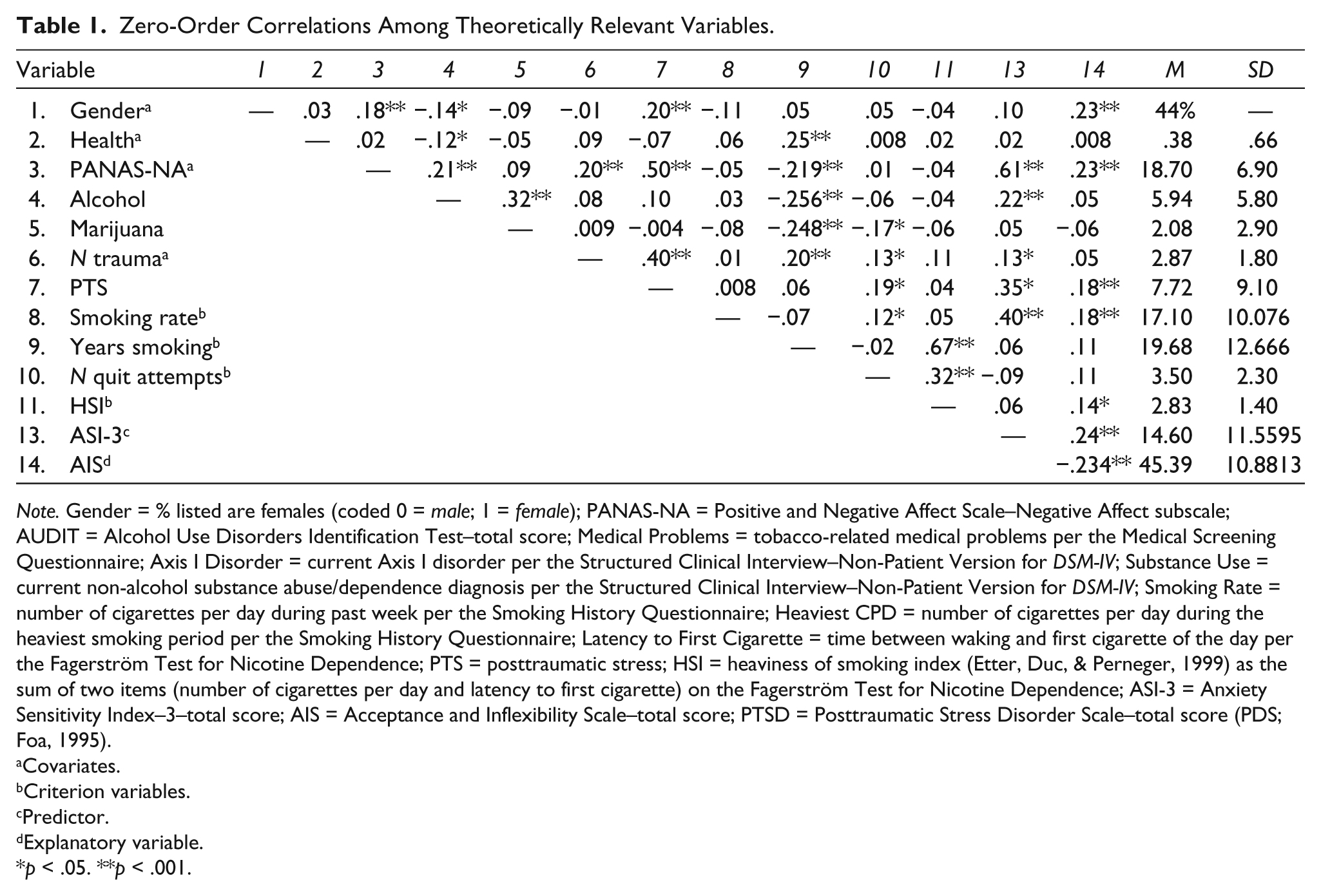
Note. Gender = % listed are females (coded 0 = male; 1 = female); PANAS-NA = Positive and Negative Affect Scale–Negative Affect subscale; AUDIT = Alcohol Use Disorders Identification Test–total score; Medical Problems = tobacco-related medical problems per the Medical Screening Questionnaire; Axis I Disorder = current Axis I disorder per the Structured Clinical Interview–Non-Patient Version for DSM-IV; Substance Use = current non-alcohol substance abuse/dependence diagnosis per the Structured Clinical Interview–Non-Patient Version for DSM-IV; Smoking Rate = number of cigarettes per day during past week per the Smoking History Questionnaire; Heaviest CPD = number of cigarettes per day during the heaviest smoking period per the Smoking History Questionnaire; Latency to First Cigarette = time between waking and first cigarette of the day per the Fagerström Test for Nicotine Dependence; PTS = posttraumatic stress; HSI = heaviness of smoking index (Etter, Duc, & Perneger, 1999) as the sum of two items (number of cigarettes per day and latency to first cigarette) on the Fagerström Test for Nicotine Dependence; ASI-3 = Anxiety Sensitivity Index–3–total score; AIS = Acceptance and Inflexibility Scale–total score; PTSD = Posttraumatic Stress Disorder Scale–total score (PDS; Foa, 1995).
Covariates.
Criterion variables.
Predictor.
Explanatory variable.
p < .05. **p < .001.
Participants met criteria for an average of 3.1 traumatic event types, as reported on the PDS (Foa, 1995). In terms of the nature of traumatic events, 65% of the participants reported experiencing a serious accident, explosion, or fire; 40.9% of the participants reported experiencing a natural disaster; 36.1% of the participants reported experiencing non-sexual assault by a family member or someone known; 34.9% of the participants reported experiencing non-sexual assault by a stranger; 30.2% of the participants reported experiencing sexual contact with someone 5 or more years older before the age of 18; 26% of the participants reported experiencing a life-threatening illness; 26% of the participants reported experiencing an “other” traumatic event (e.g., unexpected death of a loved one); 17.2% of the participants reported experiencing sexual assault by a family member or someone known; 17.2% of the participants reported experiencing sexual assault by a stranger; 13% of the participants reported experiencing imprisonment; 5.3% of the participants reported experiencing military combat or a war zone; and 5.3% of the participants reported experiencing torture.
Table 2 shows beta coefficients for Paths a, b, c, c’, and ab for each criterion variable. Overall, with the exception of smoking rate, the direct effects of AS on other criterion variables (Paths c and c’) were not significant (see Table 2). Considering the defining role of Path ab in detection of indirect effects, this path will be discussed for each model below.
Results From Regression Models Predicting Smoking-Related Avoidance and Inflexibility From Anxiety Sensitivity and Each Criterion Variable From Anxiety Sensitivity and Smoking-Related Avoidance and Inflexibility.
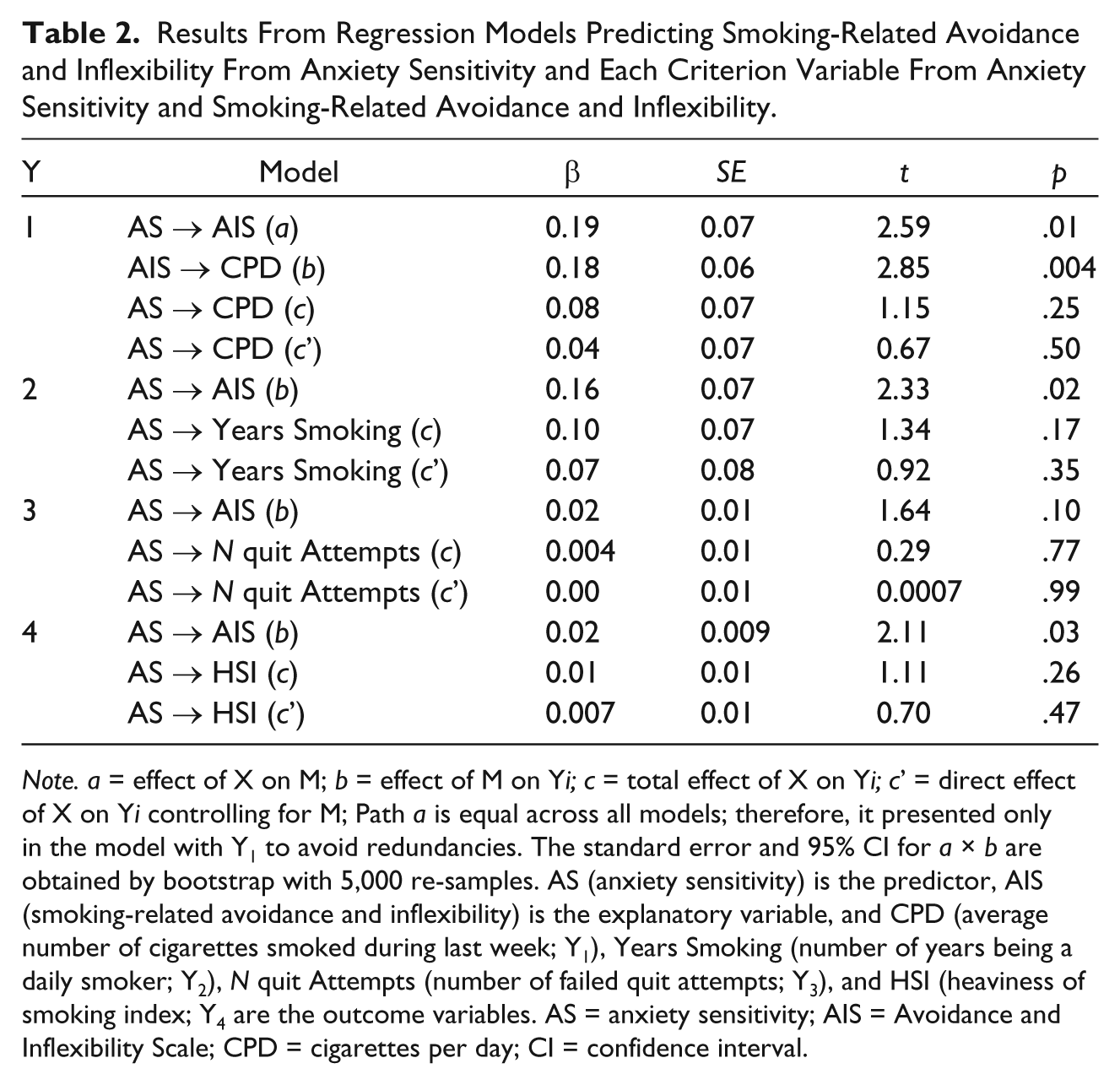
Note. a = effect of X on M; b = effect of M on Yi; c = total effect of X on Yi; c’ = direct effect of X on Yi controlling for M; Path a is equal across all models; therefore, it presented only in the model with Y1 to avoid redundancies. The standard error and 95% CI for a × b are obtained by bootstrap with 5,000 re-samples. AS (anxiety sensitivity) is the predictor, AIS (smoking-related avoidance and inflexibility) is the explanatory variable, and CPD (average number of cigarettes smoked during last week; Y1), Years Smoking (number of years being a daily smoker; Y2), N quit Attempts (number of failed quit attempts; Y3), and HSI (heaviness of smoking index; Y4 are the outcome variables. AS = anxiety sensitivity; AIS = Avoidance and Inflexibility Scale; CPD = cigarettes per day; CI = confidence interval.
Regarding the number of cigarettes per day, bootstrap analysis (5,000 re-samples) revealed a positive significant indirect effect in the proposed model (point estimate = .035, PB 95% CI [.007, .090]; completely standardized indirect effect = 0.08). Moreover, results of bootstrap analysis (5,000 re-samples) of the alternative models excluded the possibility of mediation in these directions (point estimate = .007, PB 95% CI [−.01, .03], and point estimate = .018, PB 95% CI [−.005, .08], for alternative Models 1 and 2, respectively).
For the number of years being a daily smoker, bootstrap analysis (5,000 re-samples) revealed a positive significant indirect effect in the proposed model (point estimate = .0033, PB 95% CI [.005, .085]; completely standardized indirect effect = 0.03). Moreover, results of bootstrap analysis (5,000 re-samples) of the alternative models excluded the possibility of mediation in these directions (point estimate = .011, PB 95% CI [−.03, .046], and point estimate = .016, PB 95% CI [−.002, .05] for alternative Models 1 and 2, respectively).
Regarding the number of failed quit attempts, bootstrap analysis (5,000 re-samples) revealed a positive significant indirect effect in the proposed model (point estimate = .005, PB 95% CI [.001, .014]; completely standardized indirect effect = 0.05). Moreover, results of bootstrap analysis (5,000 re-samples) of the alternative models excluded the possibility of mediation in these directions (point estimate = −.0068, PB 95% CI [−.0069, .0055] and point estimate = .0025, PB 95% CI [−.015, .03] for alternative Models 1 and 2, respectively).
Finally, for the heaviness of smoking index, bootstrap analysis (5,000 re-samples) revealed a positive significant indirect effect in the proposed model (point estimate = .004, PB 95% CI [.0007, .011]; completely standardized indirect effect = 0.03). Moreover, results of bootstrap analysis (5,000 re-samples) of the alternative models excluded the possibility of mediation in these directions (point estimate = .0010, PB 95% CI [−.0006, .0036] and point estimate = .012, PB 95% CI [−.008, .05] for alternative Models 1 and 2, respectively).
Discussion
The pattern of observed results was consistent with expectation. The effect of AS on number of cigarettes per day, years being a daily smoker, number of failed quit attempts, and heaviness of smoking index was significantly explained by smoking-specific avoidance and inflexibility. Moreover, the observed effects were evident above the effects of gender, tobacco-related illnesses, alcohol and cannabis use, negative affectivity, number of traumatic event types, and PTS symptoms. Thus, the observed effects cannot be attributed to the variance accounted by these factors. These findings provide empirical evidence of the incremental explanatory effect of smoking-specific avoidance and inflexibility in the relation between AS and smoking severity among trauma-exposed smokers. These results are in line with past research implicating smoking-specific avoidance in difficulties with quitting (Bricker, Wyszynski, Comstock, & Heffner, 2013; Erskine, Georgiou, & Kvavilashvili, 2010; Gifford et al., 2011) and uniquely extend it to the trauma-exposed population. Together, these data suggest that the transdiagnostic construct of AS has an indirect effect on smoking severity, which depends, in part, on the degree to which a trauma-exposed smoker responds to aversive internal cues with smoking-specific avoidance and inflexibility. We attempted to improve confidence in the observed model by evaluating two alternative explanatory models (Alternative Model 1: AS as the explanatory variable in the relation between smoking-related avoidance and inflexibility and each criterion variable, and Alternative Model 2: each criterion variable as the explanatory variable in the relation between smoking-related avoidance and inflexibility and AS). The results of these models excluded the possibility of a significant indirect path in these directions. Still, future prospective modeling of the temporal ordering of these construct is warranted for a better understanding of the nature of these relationships.
Although not a primary focus of the investigation, a number of observations warrant brief comment. First, AS and smoking-specific avoidance and inflexibility were interrelated, but distinct constructs (5.7% of shared variance; see Table 1). Second, smoking-specific avoidance and inflexibility was also related, but empirically distinct from the criterion variables (between 2.0% and 3.2 % of shared variance; Table 1). These observations collectively add to a growing empirical literature documenting the construct validity of smoking-specific avoidance and inflexibility.
The present findings may serve to conceptually inform the development of specialized intervention strategies for trauma-exposed smokers with elevated AS. Existing AS-reduction programs for smoking cessation have provided empirical support for incorporation of cognitive-behavioral skills that address sensitivity to internal cues (e.g., interoceptive exposure; Zvolensky, Bogiaizian, et al., 2014; Zvolensky, Yartz, Gregor, Gonzalez, & Bernstein, 2008). The current data provide further evidence on the clinical utility of targeting AS to enhance psychological flexibility related to smoking to address maladaptive smoking cognitions and facilitate change in the smoking behavior of trauma-exposed smokers. Acceptance-based techniques (e.g., experiential awareness, openness, willingness, mindfulness, cognitive diffusion) have shown promise in efforts to reduce smoking-related avoidance and inflexibility (Gifford & Lillis, 2009; McCallion & Zvolensky, 2015). It may therefore be useful to integrate such skills into existing cognitive-behavioral AS-reduction smoking cessation programs of trauma-exposed smokers.
There are a number of limitations to the present study that warrant consideration. First, due to the cross-sectional nature of the methodological design, as noted earlier, we cannot isolate the temporal relationships between the examined constructs. Considering this limitation, other possible interpretations, such as smoking behavior explaining the individuals’ higher levels of AS and smoking-related avoidance and inflexibility, cannot be completely ruled out. Future investigations are needed to determine the directional effects of these relations. Second, the present study sample consisted of community-recruited, trauma-exposed smokers with moderate levels of tobacco dependence. Future work might extend the current model to lighter and heavier smoking populations to ensure the generalizability of the findings to other segments of the trauma-exposed smoking population. Third, the current study used self-report instruments as the primary assessment strategy. Future work could therefore benefit by including a multi-method assessment approach, thereby reducing concerns about the role of method variance in the observed relations. For example, it would be useful to examine the present relations in response to emotional states elicited in real time via emotion-provocation tasks. Fourth, the sample used for the present study was comprised of a relatively homogeneous group of treatment-seeking smokers. In light of the evidence for the ethno-racial differences in underlying processes of smoking among trauma-exposed smokers (Wilson et al., 2014), future research is needed to evaluate these processes among an ethnically/racially diverse sample of smokers. 1 Finally, the sample reported mild mean levels of PTS symptoms, despite reporting exposure to potentially traumatic life events. This sample may thus represent a particularly resilient group of individuals exposed to potentially traumatic events who either did not develop clinically significant PTS or who remitted from clinically significant PTS. Future work might extend this research to clinical samples with PTSD.
Overall, the present study serves as an initial investigation into the nature of the association between AS, smoking-specific experiential avoidance, and smoking severity among treatment-seeking trauma-exposed smokers. Future work is needed to explore the extent to which smoking-specific experiential avoidance accounts for relations between AS and other smoking processes (e.g., withdrawal, cessation outcome) to further clarify theoretical models of trauma-related emotional vulnerability and smoking.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Institutes of Health (NIH) grant awarded to Drs. Michael J. Zvolensky and Norman B. Schmidt (R01-MH076629-01A1).