
Abstract
Supporting parents in reducing challenging behavior of children with autism spectrum disorder (ASD) requires the identification of effective, feasible, and sustainable interventions. Functional communication training (FCT) is one of the most well-established interventions in the behavioral literature and is used increasingly by parents. However, there is a need for additional evaluation of the literature related to parent-implemented FCT. In the present review, we identified 26 peer-reviewed studies on parent-implemented FCT. We conducted systematic descriptive and social validity analyses to summarize the extant literature. Across studies, parent-implemented FCT was effective in reducing child challenging behavior, and in some cases, intervention outcomes maintained and generalized to novel settings and implementers. However, few studies reported fidelity data on parent implementation of FCT, and data regarding sustained use of FCT by parents were limited. Results of the social validity analysis indicate that while FCT is often implemented by natural change agents in typical settings, parent training is often provided by professionals not typically accessible to parents. These findings suggest that future research is warranted in the areas of parent training and long-term sustainability of parent-implemented FCT.
Keywords
Challenging behaviors are common among children with autism spectrum disorder (ASD) and can inhibit children’s success (Hartley, Sikora, & McCoy, 2008; Reinke, Herman, Petras, & Ialongo, 2008; Stipek & Miles, 2008). Parents of children with challenging behavior report having more unmet needs than parents of children without challenging behavior (Bromley, Hare, Davison, & Emerson, 2004). The reduction of challenging behavior for children with ASD requires access to evidence-based interventions and feasible and long-lasting reductions of challenging behavior often require parent implementation (Matson et al., 2012; Moes & Frea, 2002; Oono, Honey, & McConachie, 2013; Schindler & Horner, 2005; Symon, 2001, 2005). Parent implementation of interventions results in greater access to evidence-based interventions, thereby leading to improvement, generalization, and maintenance of child outcomes (Koegel, Schreibman, Britten, Burke, & O’Neill, 1982; Matson et al., 2012; Oono et al., 2013; Sanders & Glynn, 1981). For these reasons, it is important to support the use of parent training in research-based interventions for children with ASD (Estes et al., 2009; Marshall & Mirenda, 2002; Matson et al., 2012; Moes & Frea, 2000, 2002; Walker et al., 2009).
Functional communication training (FCT) is one of the most widely studied interventions to reduce challenging behavior, with more than 90 peer-reviewed articles supporting its efficacy (Carr & Durand, 1985; Falcomata & Wacker, 2013; Tiger, Hanley, & Bruzek, 2008; Wong et al., 2014). FCT involves (a) identifying the function or purpose of the challenging behavior, (b) teaching an alternative communicative response, (c) providing function-based reinforcement for the communicative response, and (d) withholding reinforcement following challenging behavior (Mancil & Boman, 2010; Tiger et al., 2008). Reviews of the literature indicate FCT is an evidence-based practice for children with ASD (National Autism Center, 2015; Wong et al., 2014).
Previous reviews of FCT for children with ASD suggest its efficacy (e.g., Mancil & Boman, 2010; Tiger et al., 2008; Wong et al., 2014). However, parent-implemented FCT may produce different outcomes in both child behavior and implementation fidelity. In some cases, children may engage in higher rates of challenging behavior during parent-implemented sessions (English & Anderson, 2004; Hanley, Jin, Vanselow, & Hanratty, 2014; Huete & Kurtz, 2010; Ringdahl & Sellers, 2000), which can negatively impact implementation fidelity (McConnachie & Carr, 1997). In addition, parents may be less likely than professionals to implement certain intervention components due to differences in training, time constraints, and sources of reinforcement (Feldman, Atkinson, Foti-Gervais, & Condillac, 2004; Moes & Frea, 2000, 2002; Sloman et al., 2005). Due to the complexity of parent-implemented interventions, there is a need for a focused examination of studies investigating the efficacy of parent-implemented FCT.
One factor affecting the use of parent-implemented interventions is the social validity of the intervention (Horner et al., 2005). Due to differences between parents and professional implementers, parents may deem intervention components more or less feasible and acceptable than professionals (Feldman et al., 2004; Moes & Frea, 2000, 2002; Sloman et al., 2005). Therefore, it is critical that applied researchers identify interventions that are socially valid in typical settings with typical implementers (Baer, Wolf, & Risley, 1968; Horner et al., 2005; Schwartz & Baer, 1991; Spear, Strickland-Cohen, Romer, & Albin, 2013; Wolf, 1978). The social validity of parent-implemented interventions may be particularly important as resource limitations and priority differences often exist between parents and other implementers, whose employment may be contingent on interacting with children (e.g., teachers, researchers, clinicians; Feldman et al., 2004; Moes & Frea, 2002; Sloman et al., 2005). There is a need for systematic reviews of parent-implemented interventions to evaluate the social validity of the intervention.
Studies often provide information regarding consumer report as a measure of social validity (e.g., Dunlap, Ester, Langhans, & Fox, 2006; Hanley et al., 2014; Wacker et al., 2011). It is important to consider many components of an intervention, in addition to consumer opinion, to fully assess an intervention’s social validity (Horner et al., 2005; Reichow, Volkmar, & Cicchetti, 2008; Spear et al., 2013). Previous reviews of the functional analysis literature (Gardner, Spencer, Boelter, DuBard, & Jennett, 2012) and function-based intervention literature (Lane, Kalberg, & Shepcaro, 2009) have evaluated social validity using the definition described in Horner et al. (2005). Both Horner et al. (2005) and Reichow et al. (2008) provide multicomponent definitions that can be used to evaluate the extent to which intervention studies meet social validity standards. Studies that meet these criteria provide convincing evidence of an intervention’s efficacy in natural contexts. It is important to evaluate the extent to which the current body of literature in parent-implemented FCT for children with ASD has demonstrated that the intervention is likely to be used in natural settings, without outside support.
There have been a number of systematic reviews of FCT (e.g., Falcomata & Wacker, 2013; Hagopian, Boelter, & Jarmolowicz, 2011; Mancil, 2006; Tiger et al., 2008). In addition, Fettig and Barton (2014) evaluated the quality of the parent-implemented function-based intervention research. However, their review was restrictive in terms of inclusion criteria (limited age range for child participants) and the search terms were relatively narrow, with the inclusion of “parents” as part of the search terms. Broader search terms and inclusion criteria may have yielded a larger number of relevant studies. In addition, the authors focused on a single feature of social validity, parent report. A more comprehensive analysis of social validity using a multi-component definition would enhance our understanding of parent-implemented FCT. The purpose of the present review was to synthesize and evaluate the research on parent-implemented FCT to decrease challenging behavior in children with ASD. The study addressed the following research questions:
Method
To answer these research questions, the present study employed the following steps: (a) systematic search and identification of articles meeting the inclusion criteria, (b) descriptive synthesis of the studies, and (c) an analysis of the social validity of the current intervention procedures.
Systematic Search Procedures
A database search and ancillary searches were used to identify articles that evaluated parent-implemented FCT to decrease challenging behavior of children with ASD. A research librarian and expert in systematic reviews advised the lead author regarding the search procedures. The systematic search was conducted in March 2016 with no restrictions on date, publication type, or language. Synonyms of FCT (“FCT,” “functional communication training,” or “functional equivalence training”) were used to identify articles in the following educational and psychology databases: PsycINFO, ERIC (EBSCO), Psychology and Behavioral Sciences Collection, Academic Search Complete, Education Source, and Education Full Text. Based on consultation with the research librarian and the comprehensive nature of Academic Search Complete, the term “FCT” was not used in the search in Academic Search Complete database. After removing duplicates, these search terms yielded 416 unique articles.
We next reviewed the titles and abstracts of all 416 articles identified through the systematic search. If the abstract and title indicated the article evaluated the use of FCT as an intervention, the article was kept for further review. A total of 155 articles were excluded based on the title and abstract. The remaining 261 articles were then evaluated based on four inclusion criteria: (a) FCT was employed as an intervention to decrease challenging behavior, (b) a parent implemented one or more intervention sessions in which data were collected on parent and/or child behavior, (c) one or more child participants had a diagnosis of ASD, (d) the article was published in a peer-reviewed journal, and (d) the article was in English. FCT was defined as differential reinforcement based on the function of the child’s challenging behavior, provided contingent upon an appropriate communicative response. Parent was defined as (a) an individual described as the parent or legal guardian or (b) an individual who was described as the child’s primary caregiver (e.g., grandparent), but was not a professional caretaker for the child (e.g., staff member at a group home). Articles must have specified that one or more child participants had a diagnosis of autism, ASD, autistic disorder, Asperger syndrome, high-functioning autism, pervasive developmental disorder (PDD), or pervasive developmental disorder-not otherwise specified (PDD-NOS; Wong et al., 2014). If the study also included participants who did not have a diagnosis of ASD, it was included as long as the data for the participant(s) with ASD could be distinguished. After applying these criteria, 241 articles were excluded. The database search yielded 20 included peer-reviewed articles.
To identify additional articles not obtained in the initial database search, we (a) reviewed the reference lists of included articles, (b) conducted a hand-search of the Journal of Applied Behavior Analysis, and (c) reviewed articles from seven previous literature reviews pertaining to FCT (Durand & Moskowitz, 2015; Falcomata & Wacker, 2013; Fettig & Barton, 2014; Hagopian et al., 2011; Heath, Ganz, Parker, Burke, & Ninci, 2015; Mancil, 2006; Tiger et al., 2008). The same inclusion criteria were applied to evaluate the additional articles from these ancillary searches. Eight additional articles were identified for inclusion, for a total of 28 articles. The first author then reviewed the 28 articles for overlap in participants. If articles included the same participants or if the data for unique participants could not be disaggregated, the more recent article was excluded from the present study. Two articles were removed due to overlap in participants or not presenting sufficient data to identify the unique participants’ data (Lindgren et al., 2016; Wacker et al., 2011). One participant participated in both Mancil, Conroy, Nakao, and Alter (2006) and Mancil, Conroy, and Haydon (2009), and one participant participated in both Schieltz et al. (2010) and Schieltz et al. (2011). Each participant’s data from the most recent article were not included in the analysis. Therefore, 26 articles were included in the review.
Data Extraction
Descriptive information
To summarize relevant features of the studies, descriptive information was collected from each study. Child participant information included (a) number of participants, (b) age, and (c) gender. Data were gathered on information provided about the parents’ relation to the child. Data collected on methodological characteristics included the (a) setting, (b) parent involvement in the assessment and intervention, and (c) implementation fidelity data reported. The setting for each study was recorded as home, community, school, clinical, or research setting. The rater also recorded the extent to which the parent was involved in the FBA. Specifically, the rater recorded whether or not the study included an interview, direct observations, and/or a functional analysis as part of the FBA. For each component included in the FBA, the rater recorded whether or not the parent was involved in that component. The rater counted the parent as involved in the interview if parents were interviewed as part of the FBA. The rater counted the parent as involved in the observation if the parent(s) interacted with the children as part of the observation. The rater counted the parent as involved in the functional analysis if the parent(s) implemented some or all of the functional analysis sessions. The rater recorded whether or not the parent was involved in the development of the intervention and whether the parent implemented some or all of the intervention sessions. The rater counted the parent as involved in the development of the intervention if the study indicated parent preference, input, and/or interviews were used to develop the intervention procedures. Finally, the rater recorded any parent implementation fidelity data reported in the study, including the percentage of sessions in which parent implementation fidelity was recorded, the average implementation fidelity, and the extent to which parents implemented sessions independently.
Social validity
To assess the social validity of parent-implemented FCT, researcher-adapted operational definitions of the social validity criteria presented in Horner et al. (2005) and Reichow et al. (2008) were developed (see Table 1 for social validity definitions). This social validity evaluation contained 10 components. Of the 10 components, four items were included in both the Horner et al. (2005) and Reichow et al. (2008) criteria, four items were included only in the Reichow et al. (2008) criteria, and two were included only in the Horner et al. (2005) criteria. The criteria assessed the extent to which the intervention was implemented in typical contexts with typical resources, the social validity of the dependent variables and outcomes, parents’ implementation of the intervention, and parent satisfaction.
Researcher-Adapted Definitions of Social Validity Quality Indicators Based on Horner et al. (2005) and Reichow, Volkmar, and Cicchetti (2008).
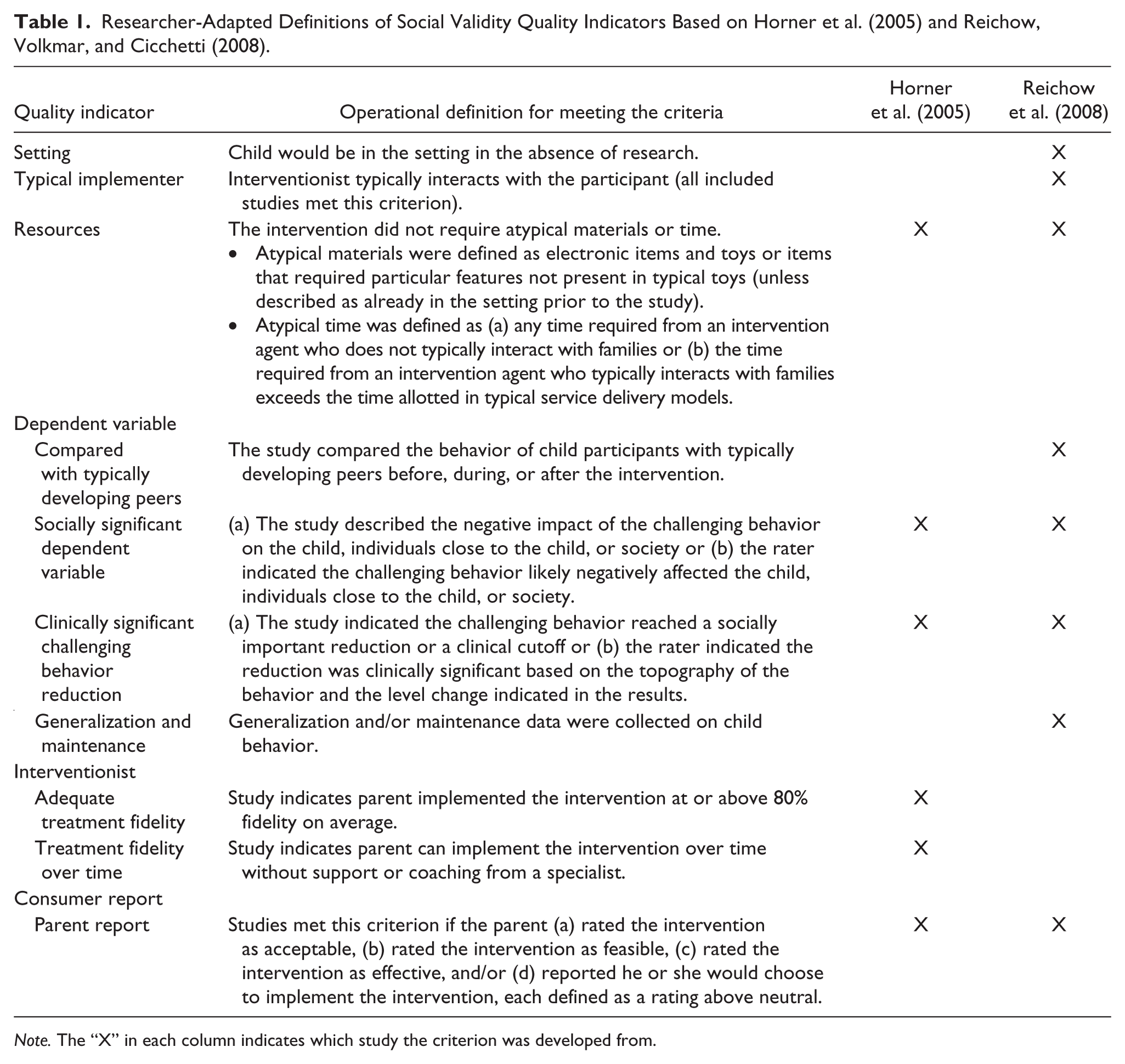
Note. The “X” in each column indicates which study the criterion was developed from.
The extent to which the intervention was implemented in typical contexts and with typical resources was assessed to evaluate the feasibility and sustainability of the intervention. More specifically, interventions were evaluated based on the following three criteria: (a) natural context, (b) typical implementer, and (c) typical resources. Studies met the natural context criterion if the intervention occurred in a setting that the child typically attended in the absence of research. Studies met the typical implementer criterion if the implementer typically interacted with the child outside of the research context. Due to the inclusion criteria for the present review, each of the included studies met this social validity criterion. Studies met the typical resources criterion if the family typically had access to the materials and the parent trainers needed to implement the intervention, outside of the context of research.
The social validity of the outcomes may affect the extent to which typical implementers choose to implement the intervention. The social validity of the target child behavior and the outcomes produced by the intervention were assessed using the following four criteria: (a) comparison with typically developing peers, (b) socially important dependent variable, (c) clinically significant reduction in challenging behavior, and (d) data on generalization and maintenance. Studies met the comparison with typically developing peers criterion if the target child’s performance was compared with the performance of typically developing peers either prior to and/or following the intervention. Studies met the socially important dependent variable criterion if the study described the impact of the target child behavior on the child, individuals close to the child, and/or society or if the rater indicated the challenging behavior likely negatively affected the child, individuals close to the child, and/or society. Studies met the clinically significant reduction criterion if the change in child behavior met a predefined clinical criterion, the study described the importance of the change in behavior, and/or the rater indicated the reduction was clinically significant based on the topography of the behavior and the level change indicated in the results. Studies met the data on generalization and maintenance criterion if the results section included data assessing generalization and/or maintenance of child behavior change.
Parent’s accurate implementation of the intervention and opinion about the intervention were evaluated, due to their possible impact on parents’ use of the intervention over time. Parents’ implementation of the intervention was evaluated based on the following two criteria: (a) adequate parent implementation and (b) implementation over time. Studies met the adequate parent implementation criterion if parent implementation data indicated that the parent implemented the intervention with 80% accuracy or higher on average. Studies met the implementation over time criterion if the parents implemented the intervention independently and accurately over time. Studies met the criterion related to parents’ satisfaction if they reported that the parent (a) rated the intervention as feasible, (b) rated the intervention as effective, and/or (c) indicated he or she would choose to implement the intervention. The parent had to select above a neutral rating on the item(s) for the study to meet the criterion.
Search Replication and Interrater Reliability (IRR)
Systematic search
To assess the reliability of the search, a second independent rater conducted the database search. For each article, an agreement was counted if both raters included or excluded the article. IRR was calculated as the number of agreements divided by the number of agreements plus disagreements multiplied by 100. The first and second raters disagreed on the inclusion of six of the 416 articles identified via the database search (IRR = 99%). All instances of disagreement were discussed by the first and second raters until a consensus was made regarding inclusion.
Descriptive table, quality indicators, and social validity
A second rater independently collected data on the descriptive information and social validity ratings for at least 25% of the included studies on each item. If the raters recorded the same information, the item was counted as an agreement. IRR was calculated as the number of agreements divided by the number of agreements plus disagreements times 100. For descriptive information, average IRR was 96% for the participants and setting, 83% for parent involvement, and 89% for parent implementation fidelity. For the social validity evaluation, average IRR was 92% for typical context, implementer, and resources; 86% for the social validity of the dependent variable; and 89% for parent implementation and opinion. The first and second raters discussed all disagreements and came to a consensus about what should be included in the table.
Results
Table 2 summarizes the participant characteristics and settings, parent involvement, and parent implementation fidelity.
Participants, Setting, Parent Involvement, and Parent Implementation Fidelity.
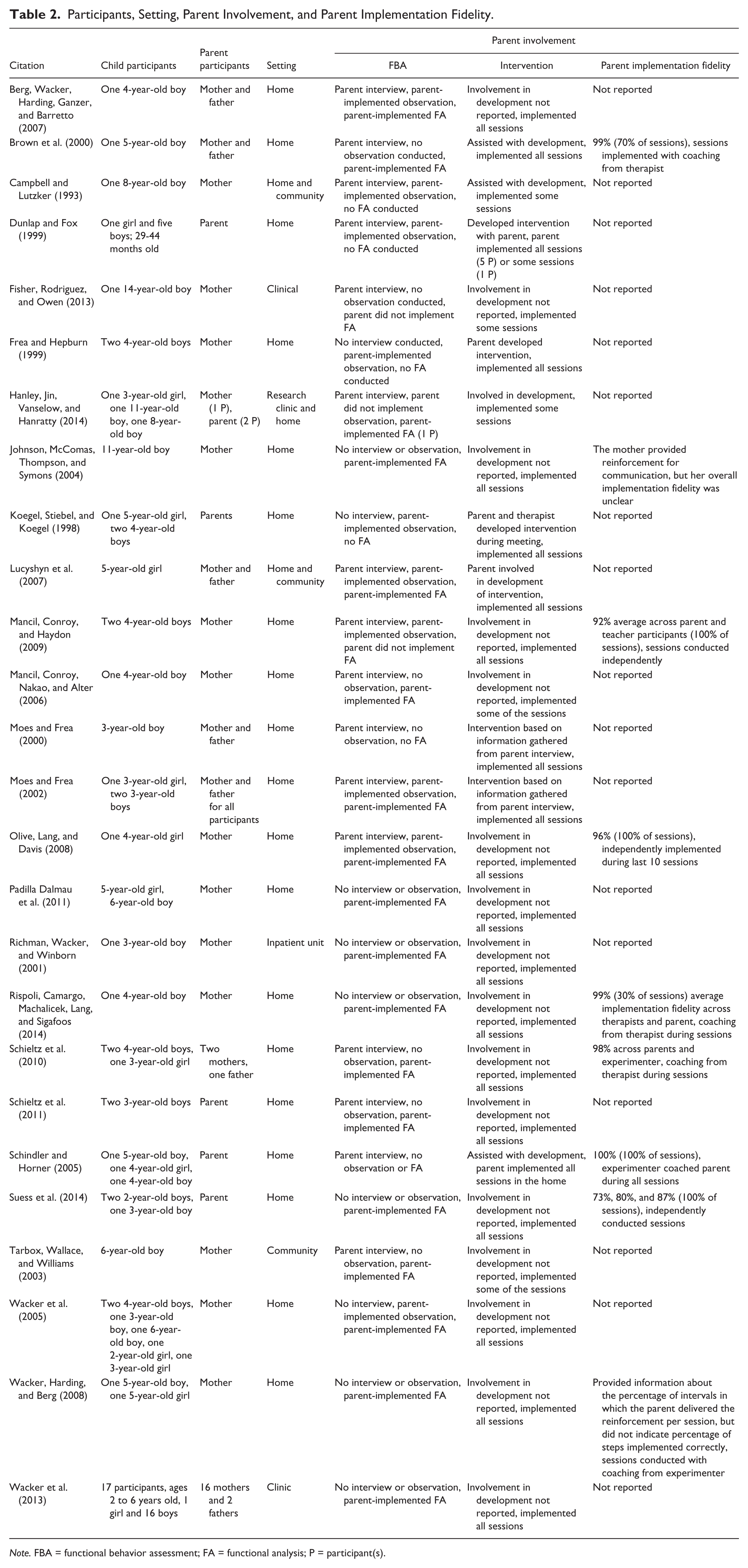
Note. FBA = functional behavior assessment; FA = functional analysis; P = participant(s).
Participant Characteristics and Setting
Across the 26 included studies, 78 parents implemented FCT with 69 children. For nine of the child participants, two parents participated as implementers. Most of the child participants were males (n = 56; 81%), and the remaining 13 participants were females (19%). Most of the child participants were between the age of 3 and 5 years old (n = 50; 72%). The remaining child participants were younger than 36 months (n = 9; 13%), 6 to 10 years old (n = 7; 10%), or 11 to 14 years old (n = 3, 4%). There were no child participants older than 14 years old. The majority of parent implementers were mothers (n = 51; 65%), 10 were fathers (13%), and the remaining implementers were described as “parents” (n = 17; 22%).
Parent-implemented FCT took place in the home setting for the majority of studies (22 studies; 85%). In three of those studies, FCT was implemented in another setting, with two studies in a community setting and one study in a clinical setting. FCT took place exclusively in a community setting in one study and exclusively in a clinical setting for three studies.
Parent Involvement in FBA and Intervention
Studies varied in the extent to which they used interview, direct observation, and/or functional analysis as part of the FBA. However, every study involved parents in some portion of the FBA process, and parents were involved in the majority of FBA components implemented across the studies (44 out of 47 components implemented; 94%). Of the 26 included studies, 16 included interviews (62%), 11 included direct observations (42%), and 20 included a functional analysis (77%) as part of the FBA. All of the 16 studies that conducted interviews included the parent as part of the interview. Similarly, 10 of the 11 studies (91%) that conducted direct observations included parent–child interactions as part of the observations. Finally, in 18 of the 20 studies (90%) that included a functional analysis, the parent implemented some or all of the functional analysis sessions.
As reflected in this study’s inclusion criteria, parents implemented at least some of the intervention sessions for all studies. Parents implemented all intervention sessions in 21 studies (81%) and some of the intervention sessions in five studies (19%). The parent assisted with the development of the intervention in 10 of the included studies (38%). For example, in Moes and Frea (2002), the therapist conducted an interview with the parents to gather information about family routines, resources, and goals to develop an intervention plan with the family. The parents rated the intervention that was based on the parent interview as more sustainable than the intervention that was developed without input from the family. In Frea and Hepburn (1999), parents read materials on function-based interventions, then chose the alternative communication response with no input from the parent trainer.
Parent Implementation Fidelity
Approximately one third of the included studies reported information regarding parent implementation fidelity (nine studies; 35%). In seven of the nine studies, parents implemented the intervention at or above 80% implementation fidelity on average. In one of those seven studies (Suess et al., 2014), two parents implemented FCT at or above 80% implementation fidelity and one parent implemented FCT with lower than 80% implementation fidelity on average. The remaining two studies did not provide sufficient information to assess whether or not parents implemented the intervention accurately (Johnson, McComas, Thompson, & Symons, 2004; Wacker, Harding, & Berg, 2008). Three studies included sessions in which the parent implemented FCT independently (i.e., without coaching; Mancil et al., 2009; Olive, Lang, & Davis, 2008; Suess et al., 2014). In each of the studies, the parent implemented FCT with 80% implementation fidelity or above, with the exception of one of the three parents in Suess et al. (2014).
Social Validity
The social validity evaluation consisted of 10 indicators, developed based on the quality indicators described by Horner et al. (2005) and Reichow et al. (2008). Table 3 summarizes the information gathered from the studies for the social validity evaluation. Studies met about half of the social validity indicators on average (M = 5.7; range: 4 to 9).
Evaluation of Social Validity.

Note. Typical imp. = typical implementer; Comp. to TD = target child’s behavior was compared with typically developing peers; Social sig. = the target child outcome is socially significant; Sig. reduct. = the reduction in challenging behavior is clinically significant; Gen./maint. = the study reported generalization and/or maintenance of child behavior change; 80% or above = the parent implemented the intervention with 80% implementation fidelity or above; Over time = the parent implemented the intervention independently and accurately over time; “Y” indicates the study met the criterion; “N” indicates the study did not meet the criterion.
Typical contexts and resources
Most of the studies took place in a typical context (24 studies; 92%), with a typical implementer (26 studies; 100%). All of the studies met the typical implementer indicator due to the inclusion criteria of the present review. However, only four studies met the typical resource indicator (15%; Campbell & Lutzker, 1993; Dunlap & Fox, 1999; Hanley et al., 2014; Richman, Wacker, & Winborn, 2001). This indicator required that the intervention use materials and personnel available to the family outside of the context of research. Twenty-one studies (81%) used materials that were available to the family outside of the research context. Of those 21 studies, 17 did not meet the indicator because the parent trainer was an individual who would not typically interact with the family outside of the context of research (e.g., an experimenter) or the study did not include enough information to assess whether the family would have access to the parent trainer outside of research.
Social validity of the dependent variable and outcomes
The social validity evaluation indicated that the child outcomes targeted in the studies were socially valid, with each of the studies rated as including a socially important dependent variable and rated as producing a clinically significant reduction in that dependent variable. However, only seven studies (27%) compared the behavior of the target child with the behavior of typically developing peers. Approximately half of the studies reported data on generalization and/or maintenance of intervention effects over time (15 studies; 58%). The types of generalization assessed varied by study and included generalization to a novel routine (e.g., Lucyshyn et al., 2007; Moes & Frea, 2002; Rispoli, Camargo, Machalicek, Lang, & Sigafoos, 2014), generalization to other behaviors (e.g., Schieltz et al., 2011), and generalization to novel implementers (e.g., Wacker et al., 2005). Length of maintenance probes varied widely across studies. For example, Mancil et al. (2009) included maintenance data from a 2-week follow-up visit, Moes and Frea (2002) included maintenance data from a 1-year follow-up visit, and Lucyshyn et al. (2007) included 7-year follow-up data.
Parent implementation and opinion
Few studies reported parent implementation fidelity data, suggesting that there is little evidence a typical intervention agent can implement the intervention with fidelity and over a meaningful period of time. Only seven studies (27%) indicated that the parent participant(s) implemented the intervention with fidelity. Of those studies, two demonstrated that the parents implemented the intervention independently and accurately over time (Mancil et al., 2009; Suess et al., 2014). Approximately one third of studies reported information about parent opinion (10 studies; 38%). In general, parents rated the intervention positively with regard to the extent to which he or she would choose to implement the intervention, the feasibility of the intervention, and the efficacy of the intervention. The parents in one study rated the intervention below a neutral rating for the amount of time, effort, and materials required (Schindler & Horner, 2005).
Discussion
The purpose of the present study was to synthesize the research in parent-implemented FCT for children with ASD and assess the social validity of parent-implemented FCT. The systematic database search yielded 26 articles evaluating the efficacy of parent-implemented FCT for children with ASD. These 26 studies included 69 child participants and 78 parent participants.
Descriptive Synthesis
Most of the extant literature included mothers who were taught to implement FCT with their children (typically boys) ages 3 to 5 years old. All of the studies included parents in at least one component of the FBA. Based on previous research that children are likely to engage in different patterns of behavior with parents (e.g., English & Anderson, 2004; Huete & Kurtz, 2010; Ringdahl & Sellers, 2000), the involvement of parents in the FBA process is a strength of this literature base. While parents often participated in all aspects of the FBA process and tended to implement every intervention session, few articles reported involving parents in the development of the intervention. It may be the case that authors did not report the method they used to involve parents in the development of the intervention or that interventions used have been relatively prescribed, rather than individualized based on family needs and preferences. Involving of parents in the development of FCT may lead to increased sustainability of the intervention (Moes & Frea, 2002), and it is important to report methods to incorporate parent preference, family routines, and family strengths into the development of interventions. Previous studies have typically involved parents by conducting a parent meeting or interview prior to the intervention to assess family routines, strengths, and preferences (Koegel, Stiebel, & Koegel, 1998; Moes & Frea, 2000, 2002). Future research should continue to include parents in the development of the intervention and describe the procedures used. Future research should also continue to evaluate the impact of including parents in the development of the intervention.
Social Validity Evaluation
Social validity criteria were applied to each study to evaluate the extent to which parent-implemented FCT is feasible given typical resources, results in important improvements in challenging behavior, can be implemented accurately by parents, and is rated as socially valid by parents. Findings from the present review indicate that typical change agents are often involved in the implementation of FCT and that parents often implement FCT in natural contexts. However, little research has evaluated the extent to which parents can be trained to implement FCT within typical service delivery models (e.g., Individuals With Disabilities Education Improvement Act [IDEA] Part C services, in-home training provided by public schools, specialized services typically accessed by families). An experimenter taught the parent how to implement FCT in the majority of studies included in this review. Only four studies included a typical parent trainer, defined as an individual the parent would have access to outside of the research context (Campbell & Lutzker, 1993; Dunlap & Fox, 1999; Hanley et al., 2014; Richman et al., 2001). It may be the case that the parents would have had access to the professionals labeled as “experimenters” outside of research. However, the current review offerred little evidence that parents have access to effective training beyond research contexts. Therefore, it remains unclear whether parent training via typical service delivery models is feasible and effective and there is a need for more research in this area.
The social validity evaluation indicated that the child behaviors targeted were regarded as important and resulted in clinically significant improvements. These data suggest that parent-implemented FCT can produce meaningful improvements in socially important outcomes. The extant literature provides evidence that child behavior change maintains over time and generalizes to new people and routines. In addition, the data from Schieltz et al. (2011) suggest that parent-implemented FCT targeting one behavior may result in a reduction in other, nontarget challenging behaviors.
The majority of the studies we reviewed offered no comparisons of the target child’s behavior to that of typically developing peers. The social importance of the dependent variable is clearer if the authors describe extent to which the child’s challenging behavior differs from that of typically developing peers. However, it is likely that the topographies of challenging behavior targeted (e.g., self-injury or aggression) for many of the participants included in this review were occurring at higher rates than would be exhibited by typically developing peers. In addition, the limited scope of this literature review (i.e., parent-implemented interventions) may have skewed these results, and studies conducted in school settings with professionals as implementers may be more likely to include a comparison with typically developing peers. Considering the necessity of selecting a socially important dependent variable, future studies should consider including assessments that indicate the extent to which child behavior differs from that of typically developing peers.
In general, parents rated the intervention as feasible and effective and indicated they would continue to implement the intervention. These data suggest that parents find FCT to be an acceptable intervention, which increases the likelihood of the continued use of FCT in the absence of professionals. However, there is limited information about parent training procedures that will result in accurate and independent implementation of FCT. Three of the studies included in this review provide data that indicate parents of children with ASD can implement FCT independently and accurately (Mancil et al., 2009; Olive et al., 2008; Suess et al., 2014). Thus, the extent to which parents can implement the intervention independently and accurately over meaningful periods of time is still relatively unknown, and there is a need for further research on this topic.
Limitations of the Present Review
A few limitations in the present review should be considered when interpreting the results. Due to the relatively narrow scope of this review, the results of the social validity evaluation may not be obtained for other parent-implemented interventions. In addition, we used a social validity rubric that has not been previously used to evaluate a body of research. However, the items were based on quality indicator rubrics that were developed by experts in the field (Horner et al., 2005; Reichow et al., 2008) and that have been used in previous reviews of the literature (Gardner et al., 2012; Lane et al., 2009; Reichow & Volkmar, 2010). A previous review of the literature was conducted on a similar topic (Fettig & Barton, 2014). However, the present study broadened the database search and expanded the evaluation of social validity. Of the 26 studies included in this review, five were included in the Fettig and Barton (2014) review. Therefore, this literature review examined a sufficiently different literature base, in addition to addressing different aspects of the literature.
Directions for Future Research
A number of directions for future research have been identified based on the results of the present review. First, there is a need for more research with fathers as implementers and with older children with ASD. Future research should also evaluate methods to include parents in the development of FCT and the impact of including families in the development of the intervention on both parent and child outcomes. There is a need to identify feasible parent training methods that result in the accurate implementation of FCT across contexts and time. In addition, future research should continue to identify and evaluate methods to incorporate parent training into typical service delivery, with parent training provided by individuals who interact with the parent outside of the research context.
Conclusions and Implications for Practice
The present study summarized a growing body of research on parent-implemented FCT for children with ASD. These findings suggest that parent-implemented FCT produces meaningful reductions in challenging behavior and that those changes tend to generalize to other situations and maintain over time. Specifically, the social validity evaluation suggests that FCT implemented by parents in typical intervention settings results in a reduction in challenging behavior. Parents report that FCT is feasible and effective and that they are likely to continue using FCT. A number of the studies in the present review involved young children who would likely qualify for IDEA Part C or Part B services (IDEA, 2004), suggesting the efficacy of parent training in FCT for this population. Based on these findings, providers who work with young children with challenging behavior should consider including parents as intervention agents to promote meaningful behavior change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.