
Abstract
There exists uncertainty for clinicians over how the separate subcomponent processes of psychological flexibility, a core construct of the Acceptance and Commitment Therapy model, interact and influence distress experienced. The present study (N = 567) employed latent class analysis to (a) identify potential classes (i.e., subgroups) of psychological flexibility based on responses on measures of key subcomponent process and (b) examine whether such classes could reliably differentiate levels of self-reported psychological distress and positive and negative emotionality. We found three distinct classes: (a) High Psychological Flexibility, (b) Moderate Psychological Flexibility, and (c) Low Psychological Flexibility. Those in the Low Psychology Flexibility class reported highest levels of psychological distress, whereas those in the High Psychological Flexibility class reported lowest levels of psychological distress. This study provides a clearer view to clinicians of the profile of the broader spectrum of the psychological flexibility model to facilitate change in clients.
Keywords
Psychological flexibility is at the core of the Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999, 2012) model of behavior change and is defined as the “ability to contact the present moment more fully as a conscious human being, and to change or persist in behavior when doing so serves valued ends” (Hayes, Luoma, Bond, Masuda, & Lillis, 2006, p. 6). The polar opposite to psychological flexibility is termed psychological inflexibility, characterized by a behavioral pattern of excessive control of a person’s thoughts, feelings, and emotions, with a tendency to avoid unpleasant internal experiences at the expense of more effective or valued actions (Levin et al., 2014; but see Kashdan & Rottenberg, 2010, for a caveat on framing flexibility and inflexibility as opposing ends of a psychological continuum). As put by Renshaw (2018), psychological well-being is supported and maintained by psychologically flexible behavior, whereas the development of mental health difficulties is facilitated by psychologically inflexible behavior.
Enhancing a client’s psychological flexibility has been a key goal of ACT-based intervention studies (e.g., Berghoff, McDermott, & Dixon-Gordon, 2018; Fledderus, Bohlmeijer, Fox, Schreurs, & Spinhoven, 2013; Gloster, Meyer, & Lieb, 2017; Simon & Verboon, 2016; Twohig, Plumb-Vilardaga, Levin, & Hayes, 2015). Moreover, Gloster, Klotsche, Chaker, Hummel, and Hoyer (2011) reported that psychological flexibility “adds to the explanation of clinically relevant variables, such as functioning and impairment, beyond well-validated measures of depression, anxiety, and stress as well as anxiety sensitivity and neuroticism” (p. 976). Indeed, Gloster et al. (2017) found that psychological flexibility moderated a wide variety of stressors in a large Swiss sample, and proposed that increasing psychological flexibility could be a desirable and achievable public health target.
Psychological flexibility is a broad, overarching construct comprised of six distinct subprocesses: acceptance, cognitive defusion, self-as-context, present-moment awareness, values clarification, and committed action (Hayes et al., 2006). At the other end of the spectrum, psychological inflexibility comprises experiential avoidance, cognitive fusion, self-as-content, lack of present-moment awareness, lack of values, and lack of commitment to action (Levin et al., 2014). Whereas much research, as noted above, has focused on targeting the overarching construct of psychological flexibility/inflexibility, a growing body of evidence illustrates the utility of individual component subprocesses of psychological inflexibility as potentially useful explanatory concepts in terms of how people cope with psychological distress and suffering in a wide variety of domains (e.g., Bardeen & Fergus, 2016; Chawla & Ostafin, 2007; Levin, Hildebrandt, Lillis, & Hayes, 2012; Monestès et al., 2018; Trindade, Ferreira, & Pinto-Gouveia, 2018).
Experiential avoidance is the most widely researched component of psychological inflexibility (e.g., Bardeen, Fergus, & Orcutt, 2013; Gerhart, Baker, Hoerger, & Ronan, 2014; Karekla & Panayiotou, 2011; Monestès et al., 2018). It is defined as behavior that attempts to “alter the frequency or form of unwanted private events, including thoughts, memories, and bodily sensations, even when doing so causes personal harm” (Hayes, Pistorello, & Levin, 2012, p. 981). Experiential avoidance has been linked to a wide range of clinically relevant phenomena (Chawla & Ostafin, 2007; Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). For example, experiential avoidance has been found to be a key process in emotional disorders (Spinhoven, Drost, de Rooij, van Hemert, & Pennix, 2014), depressive symptoms (Kashdan, Breen, Afram, & Terhar, 2010), binge eating (Lillis, Hayes, & Levin, 2011), body image disturbance (Blakey, Reuman, Bucholz, & Abramowitz, 2017), social anxiety (Kashdan et al., 2010; Kashdan et al., 2013), chronic pain (Karademas et al., 2017), anxiety sensitivity and stress and anxiety (Bardeen et al., 2013; Bardeen, Fergus, & Orcutt, 2014), trauma (Lewis & Naugle, 2017), and post-traumatic stress (Kashdan & Kane, 2011; B. L. Thompson & Waltz, 2010). Indeed, there have been a number of proposals for the potential of experiential avoidance to serve as a generalized transdiagnostic measure for psychopathology (e.g., Lewis & Naugle, 2017; Monestès et al., 2018; Spinhoven et al., 2014; but see also Levin et al., 2014, for a similar claim for psychological inflexibility more generally).
According to Gillanders et al. (2014), cognitive fusion is conceptualized as a unidimensional construct on a continuum from cognitive fusion to cognitive defusion. A client’s level of cognitive fusion is characterized by the extent to which they believe that their negative thoughts are literally true. A particular difficulty is that, asides from the psychological distress that believing (i.e., being fused with) negative and emotionally upsetting thoughts may cause individuals, cognitive fusion often leads to acting in accordance with such problematic thoughts. More explicitly, cognitive fusion is the process in which the content of their thoughts comes to exert excessive control over individuals, leads to difficulty in tracking experiences outside of the actual content of those specific thoughts, and feels restricted and compelled to act on what the thoughts say they should do as (McCracken, Barker, & Chilcot, 2014). To help counteract the process of cognitive fusion, the aim of cognitive defusion, therefore, is to discompose the troublesome functions of negative thoughts by establishing non-literal contexts for the client to observe their thinking as a dynamic ongoing process (Luoma & Villatte, 2012). This faciltates defusion, or cognitive distancing, rather than only encountering the world as organized through their thoughts. Cognitive fusion and defusion have been found to help account for, among other clinical problems, approach-avoidance coping with stress (Donald, Atkins, Parker, Christie, & Guo, 2017), psychological coping with inflammatory bowel disease (Trindade et al., 2017), suicidal ideation (Roush, Brown, Mitchell, & Cukrowicz, 2017), depression (Bardeen & Fergus, 2016), and body image dissatisfaction and eating disorders (Ferreira, Palmeira, & Trindade, 2014).
Committed action is generally conceived as flexible persistence in goal-directed behavior (Hayes et al., 2006; Scott, McCracken, & Norton, 2016). As a component of ACT, it has most notably been successfully applied in the treatment of chronic pain patients (McCracken & Morley, 2015). Generally speaking, however, it is a relatively understudied sub-component process of psychological inflexibility. Encouragingly, Trindade, Marta-Simoes, Ferreira, and Pinto-Gouveia (2018) examined committed action in both a healthy population and a sample with breast cancer, suggesting promising utility for this subcomponent of psychological flexibility as a therapeutic target. In terms of the present study with the focus on the psychological inflexibility model, it could be more helpfully conceptualized as lack of committed action, or simply inaction.
Contact with the present moment (or more simply, present-moment awareness) is similar to many conceptualizations of mindfulness in the clinical literature (e.g., Brown & Ryan, 2003; Kabat-Zinn, 2003). It focuses on the assertion that we spend too much of our time thinking about an imagined future we have not yet experienced or ruminating about a past we cannot change. The result of this excessive focus on the constructed future or the past means that we lose connection to our direct and current experience (Luoma & Villatte, 2012). ACT encourages contact with the present moment via a strong emphasis on an ongoing and flexible awareness of a person’s current and direct experiences (i.e., psychological and environmental events), without negative judgments, evaluations, or maladaptive comparisons (Luoma & Villatte, 2012). With respect to the current study, lack of contact with the present moment reflects a tendency to be stuck in a constructed future or conceptualized past that does not allow for the disruption of unhelpful ruminative cycles as there is no mental space or quietude to allow for more flexible and adaptive response to life’s prevailing difficulties or challenges.
Two further less well-studied subcomponents of the psychological inflexibility model are self-as-content and lack of values. For the purposes of the present study, the lack of well-validated and empirically supported measures of self-as-content and values at the time of data collection means that we will not assess those two subcomponents of psychological inflexibility.
While acknowledging the burgeoning evidence supporting the validity of some measures assessing individual components of the psychological inflexibility model, Scott, McCracken, and Norton (2016) asserted that there was a clear necessity to examine the inter-relationships of component processes in a more focused manner. A few studies have examined the interaction of two or more components of psychological inflexibility (e.g., Bardeen & Fergus, 2016; Hapenny & Fergus, 2017; Roush et al., 2017; Tyndall, Waldeck, Riva, Wesselmann, & Pancani, 2018). Such studies represent an important step in furthering our understanding of how the psychological inflexibility model functions as a theoretical account of psychological distress and lower emotional well-being. In particular, ACT theory suggests that experiential avoidance and cognitive fusion could be conceptualized as a “pair” that influence emotional regulation (Hayes, Strosahl, et al., 2012; see also Francis, Dawson, & Golijani-Moghaddam, 2016). Bardeen and Fergus (2016), for example, explored the interactive effect of experiential avoidance and cognitive fusion with regard to symptoms of anxiety, depression, and posttraumatic stress. Bardeen and Fergus highlighted a particular risk factor for prolonged psychological distress, and the potential for the development of psychopathology more generally, as the combination of high experiential avoidance and high cognitive fusion.
In the context of psychological distress from perceived ostracism, Tyndall, Waldeck, Riva et al. (2018) unpacked Waldeck, Tyndall, Riva, and Chmiel’s (2017) finding that psychological inflexibility moderates distress from perceived ostracism with an examination of the interaction effect of cognitive fusion and experiential avoidance. Tyndall et al. reported that, rather than the expected interaction effect, a structural equation model analysis found that experiential avoidance alone moderated the psychological distress from perceived ostracism over a period of 6 months. Such findings indicate that we have much to learn about how the psychological inflexibility model functions as subcomponent processes may interact in expected or unexpected ways.
Scott et al. (2016) conducted confirmatory factor analyses on a number of core processes of the ACT model of psychological inflexibility with respect to health and well-being related outcome measures in chronic pain patients. More specifically, they administered the original Acceptance and Action Questionnaire (Hayes et al., 2004), the Cognitive Fusion Questionnaire (CFQ; Gillanders et al., 2014), and Committed Action Questionnaire (CAQ-8; McCracken, Chilcot, & Norton, 2015) along with a measure of “decentering” which is somewhat related to the ACT model components of cognitive defusion (see Bernstein et al., 2015) and present-moment awareness. Scott et al. reported that as there was an observed saturation of items across these measures, in that there was a significant load on one general factor they referred to as “openness,” this suggests that these separate measures do not reliably measure the unique portions of variance relating to purportedly distinct component processes that the model predicts. Moreover, Scott et al. found that there appeared to be two distinct components of decentering and committed action within the overall model. In a somewhat similar vein, Hayes, Villatte, Levin, and Hildebrandt (2011) proposed that within the overarching psychological flexibility model, there were three pairs or dyads of the original six components comprising (a) acceptance and defusion (i.e., open), (b) present-moment awareness and self-as-context (i.e., aware), and (c) values and committed action (i.e., active). Thus, it is not particularly clear as to whether the psychological flexibility/inflexibility model is comprised of six distinct processes, or fewer overlapping processes (e.g., either two or three processes).
To help address concerns regarding the underlying conceptual structure of the ACT model (e.g., Christodoulou, Michaelides, & Karekla, 2018; Scott et al., 2016; Vowles, Sowden, & Ashworth, 2014), the present study proposes that a latent class analysis (LCA; Hagenaars & McCutcheon, 2002) of core components of the psychological inflexibility model could potentially elucidate the inter-relationships among ACT processes more clearly. Such a powerful analytic technique would potentially provide a clearer view of the psychological inflexibility model than we have seen in the literature to date as it could help isolate and identify significantly different classes of psychological inflexibility. In other words, LCA is a person-centered statistical technique that can help identify subgroups of individuals who share common characteristics (Djelantik, Smid, Kleber, & Boelen, 2017) according to how they respond on different component measures of the psychological inflexibility model. Furthermore, importantly, the LCA technique can indicate whether these profiles predict levels of self-reported psychological distress or emotional well-being.
The present study focused on a LCA of subcomponent inter-relationships within the broader construct of psychological inflexibility by including measures of the following core ACT component processes: (a) experiential avoidance (Brief Experiential Avoidance Questionnaire [BEAQ]), (b) cognitive fusion (CFQ), (c) lack of present-moment awareness (Five-Facet Mindfulness Questionnaire [FFMQ-SF]), and (d) lack of commitment to action (CAQ-8); along with (e) the omnibus measure of psychological inflexibility and experiential avoidance (Acceptance and Action Questionnaire–II [AAQ-II]) itself. More specifically, the LCA examined these particular subcomponents of the psychological inflexibility model with respect to levels of positive and negative emotionality and overall self-reported psychological distress (i.e., depression, anxiety, and stress). Thus, the first aim of the present study was to discover if it was possible to identify significantly different subgroups (i.e., latent classes) of psychologically flexible or inflexible individuals based on a number of core constructs of the ACT model. The second aim was to examine if the different classes of psychological flexibility could meaningfully discriminate levels of self-reported depression, stress, anxiety (i.e., psychological distress), and positivity and negative emotionality. To the best of our knowledge, the present study is the first to explore classes or subgroups of psychological inflexibility. Finally, while an examination of sociodemographic variables is not typically a concern in research on psychological flexibility, studies using the LCA technique often explore relationships among sociodemographic variables and the latent classes of interest (e.g., Djelantik et al., 2017; Lenferink, de Kejser, Smid, Djelantik, & Boelen, 2017). Thus, as there was no substantive previous literature to suggest particular effects of sociodemographic variables on psychological flexibility, no specific a priori predictions were made. Notwithstanding, the present study used the LCA technique to examine potential associations between psychological flexibility class membership and sociodemographic variables of gender, relationship status, and education level.
Method
Participants
The sample (N = 557; 354 women, 203 men) were recruited using an online survey distributed through emails to university networks within the United Kingdom and websites designed for academic research data collection (e.g., http:///www.findparticipants.com). The participants ranged between 18 and 73 years of age (Mage = 27; SD = 11). The sample consisted mostly of American (49.2%) and British (15.4%) residents. The majority of participants were of White racial identity (83%) and employed in a broad array of industries. More specifically, participants reported that they were employed mostly within the health and social care industry (21%), education (15%), computer industry (10%), office and administration support (8%), sales (7%), government (6%), and arts and entertainment media (4%). Before data collection began, the study gained approval by the University of Chichester Research Ethics Committee.
Measures
AAQ-II
The AAQ-II (Bond et al., 2011) is a seven-item measure of psychological inflexibility. Participants responded to items using a 7-point Likert-type scale from 1 (not at all true) to 7 (completely true; α = .93). Sample items include “My painful memories prevent me from having a fulfilling life” and “I’m afraid of my feelings.” Test scores on the AAQ-II have demonstrated good internal consistency and test–retest reliability in community samples (Bond et al., 2011).
CFQ
The CFQ (Gillanders et al., 2014) is a seven-item measure of cognitive fusion that assesses the tendency for people to struggle and become entangled with distressing thoughts. Participants responded to items using a 7-point Likert-type scale from 1 (not at all true) to 7 (completely true; α = .87). Sample items include “I struggle with my thoughts” and “I tend to get very tangled up in my thoughts.” The CFQ has demonstrated good internal consistency and construct validity in community samples (Gillanders et al., 2014).
BEAQ
The BEAQ (Gámez et al., 2014) is a 15-item measure of experiential avoidance, and was developed with separate student, community, and patient samples. Participants responded to items using a 6-point Likert-type scale from 1 (strongly disagree) to 6 (strongly disagree; α = .87 in the present study). The BEAQ has demonstrated good internal consistency and construct validity (Gámez et al., 2014). Sample items include “The key to a good life is never feeling any pain” and “I would give up a lot not to feel bad.”
CAQ-8
The CAQ-8 (McCracken et al., 2015) is an eight-item measure of committed action, a component process of psychological flexibility that entails flexible persistence in goal-directed behavior. Participants responded to items using a 7-point Likert-type scale from 0 (never true) to 6 (always true; α = .62). Sample items include “I prefer to change how I approach a goal rather than quit” and “If I felt distressed or discouraged, I let my commitments slide.” Analyses of the CAQ-8 have demonstrated good internal consistency and construct validity (McCracken et al., 2015).
FFMQ-SF
The FFMQ-SF (Bohlmeijer, ten Klooster, Fledderus, Veehof, & Baer, 2011) was developed as a brief version (24 items) of the original 39-item FFMQ (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006). The FFMQ-SF assesses five facets of mindfulness including observing, describing, acting with awareness, non-judging, and non-reactivity. Items were scored on a 5-point Likert-type scale ranging from 1 (never or very rarely true) to 5 (very often or always true). Sample items include “I find it difficult to stay focused on what’s happening in the present-moment” and “Usually when I have distressing thoughts or images, I can just notice them without reacting.” The FFMQ-SF has demonstrated good internal consistency and construct validity (Bohlmeijer et al., 2011). For the purposes of the present study, we used the FFMQ-SF as a unidimensional measure to help ensure stable parameters for the analyses and increase interpretability of the solution. The internal consistency was low to moderate (α = .60).
International–Positive and Negative Affect Schedule–Short Form (I-PANAS-SF)
The I-PANAS-SF is a 10-item measure of affectivity, with five items assessing positive and five items assessing negative affectivity (E. R. Thompson, 2007). Items were scored on a 5-point Likert-type scale ranging from 1 (never) to 5 (always). The I-PANAS-SF has demonstrated good internal consistency, temporal stability, construct validity, and cross-cultural factorial invariance (E. R. Thompson, 2007). Sample items include a response to the following question: “Thinking about yourself and how you normally feel, to what extent do you generally feel?” in terms of a particular term such as “Ashamed” and “Nervous.” Internal consistency for positive (α = .80) and negative affectivity (α = .81) was good.
Depression Anxiety and Stress Scales (DASS-21)
To assess psychological distress, participants completed 21 items from the DASS-21 (Lovibond & Lovibond, 1995). The DASS-21 has been demonstrated to have sufficient construct validity in non-clinical samples (Henry & Crawford, 2005). Participants rated the frequency and severity of experiencing psychological distress in the last week. The items were rated on a 4-point Likert-type scale, where 0 represented did not apply to me at all and 3 represented applied to me very much or most of the time (α = .93). Sample items include “I felt down-hearted and blue” and “I felt I was close to panic.”
Procedure
All seven self-report measures were uploaded to the Internet with Qualtrics online survey system. Participants were emailed a link to the webpage and responded to standard demographic questions and clicked on a forced-choice informed consent confirmation question to proceed. A randomization function on Qualtrics was chosen which selected the order of presentation of each of the seven measures at random. Participants completed all seven measures in one logged-in session. There were no missing data as a forced-choice function was activated to ensure each item was responded to before moving on to the next item.
Data Management and Analysis
Profiles were identified though a LCA (for an overview, see Hagenaars & McCutcheon, 2002). LCA is a technique that tests whether the scores on a set of variables can define homogeneous subgroups of individuals (i.e., classes) that are similar in the levels of these variables, thus identifying different profiles. Typically, several LCA solutions that differ in number of classes extracted are evaluated. The LCA was ran on the composite scores of the AAQ-II, CFQ, BEAQ, CAQ-8, and FFMQ, to identify groups of individuals based on the constructs measured by these instruments.
The best solution (i.e., the best number of classes) was determined from both a statistical and a theoretical standpoint. The following statistical indices were considered: (a) the Bayesian information criteria (BIC), which is a measure of model fit; (b) entropy, which is a measure of certainty of the classification; (c) posterior probability of the classes, which indicates the precision of individual classification. A lower value of the BIC and values of entropy and posterior probabilities close to 1.00 indicate good fit of the solution. In addition, (d) the Lo–Mendell–Rubin adjusted likelihood ratio test (LMR) and (e) the bootstrapped likelihood ratio test (BLRT) were used to directly compare two solutions, one with k classes and the other one with k – 1 classes. A non-significant probability value associated to the 2-times log-likelihood difference tested by the LMR and BLRT indicates that the narrower solution (i.e., k – 1 classes) does not fit the data significantly worse than the wider one (i.e., k classes), hence it should be preferred.
Statistical indices provide the basis for model selection, but the evaluation of the optimal LCA solution highly depends on theoretical considerations concerning the interpretability and meaningfulness of the profiles, as well as parsimony of the solution and absence of classes with too few members. Once the best LCA solution was determined, psychological and sociodemographic variables were compared among the identified profiles. Specifically, between-subjects ANOVAs were used to detect differences in the levels of depression, anxiety, stress, positive emotions, negative emotions, and age, whereas contingency tables and chi-square test were used to investigate gender (males vs. females), education level (high school or lower vs. higher than high school), and relationship status (singles vs. in a relationship). The LCA was performed using the statistical software Mplus, version 7 (Muthén & Muthén, 2012), whereas the ANOVAs, contingency tables, and chi-square tests were performed using SPSS, version 24 (IBM Corp., 2016).
Results
Before conducting LCA, the composite scores of AAQ-II, CFQ, BEAQ, CAQ, and FFMQ were scaled to facilitate the interpretation of the profiles. Specifically, we converted the scores to a 0 to 100 range, where 0 indicated the lowest and most maladaptive level of a construct and 100 the highest and most adaptive one. Note that this strategy was employed simply to make the output (i.e., comparing levels of the constructs among classes) more readable in that it allows for greater clarity in viewing which constructs are higher or lower than others. If we had ran the same analysis on the original scales, the relationships between the constructs would remain the same, yielding solutions with the same entropy and classes composed of the same participants.
Identification of Profiles
Table 1 reports the fit indices of the six LCA models that were run extracting two, three, four, five, and six classes, namely, Models K2, K3, K4, K5, and K6, respectively. The result of the BLRT test was not taken into account in the evaluation of the optimal number of classes because it always supported the wider solution between two competing models; thus, it was considered uninformative. No more than six classes were estimated because the non-significant probability associated to the LMR that compared K6 and K5 models indicated that five classes (i.e., Model K5) were sufficient to explain our data and one more class was not really needed. Moreover, the BIC yielded by K6 was higher than that of K5, confirming that five classes were better than six classes and lead to the exclusion of K6 as a possible candidate for the optimal solution. Among the remaining four models, K5 yielded the lowest BIC and the LMR indicated that it performed significantly better than K4. However, two main reasons led to the exclusion of K5 as the optimal solution. First, it showed the lowest entropy and posterior probabilities, revealing a lower certainty and precision of the classification compared with that of the other solutions. Second, the class with the lowest posterior probability accounted for only 6.3% of the sample, suggesting that this model was not parsimonious. After the exclusion of K5, the lowest BIC was associated to K4, but, again, its entropy, posterior probabilities, and the LMR test indicated that Model K3 performed better than K4. Finally, the comparison between K3 and K2 did not provide clear indications about which of these two models should be preferred from a statistical perspective. Indeed, the LMR test and the BIC supported the three-class solution, whereas entropy and posterior probabilities favored the two-class solution.
The Results of the Latent Class Analysis.
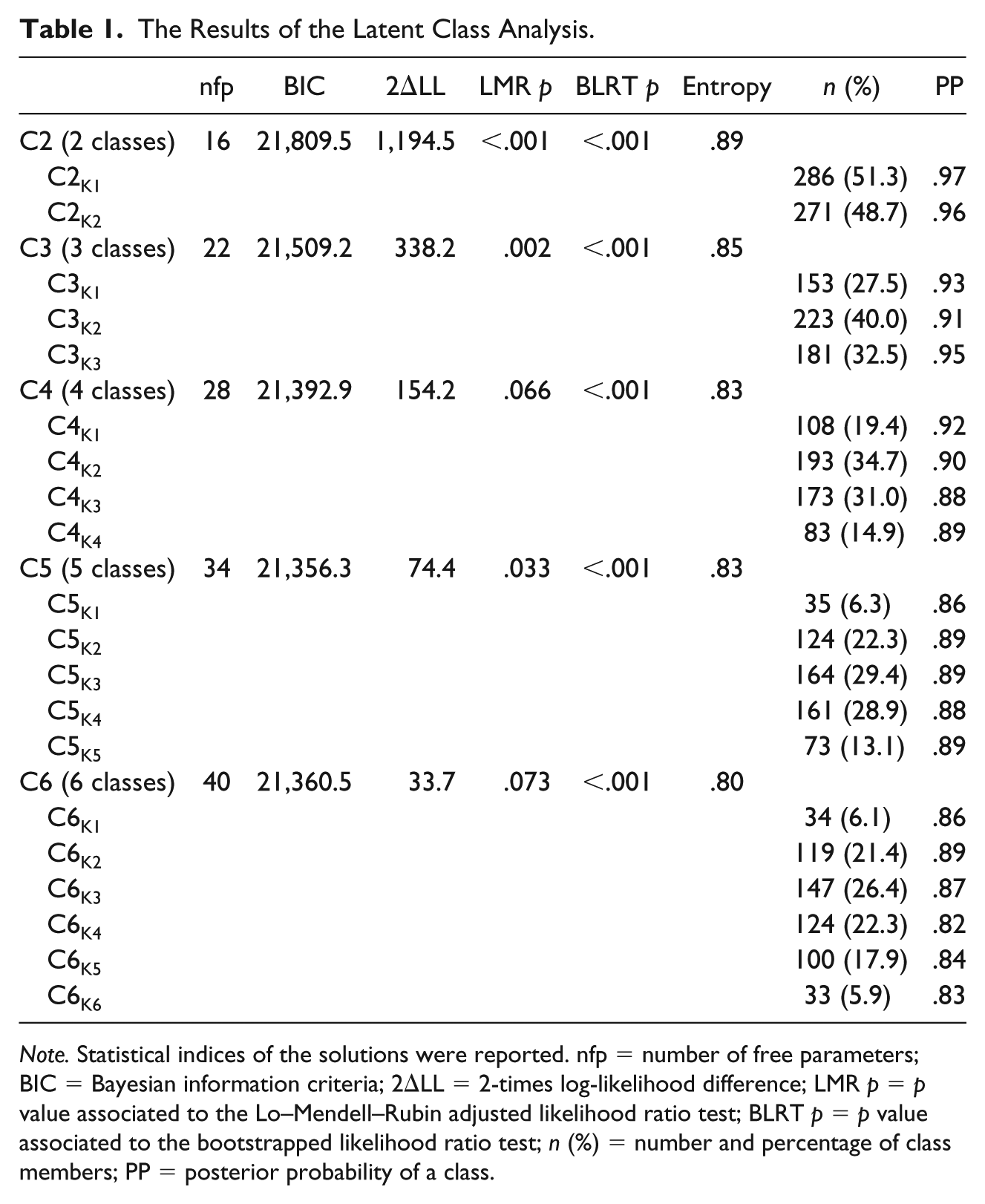
Note. Statistical indices of the solutions were reported. nfp = number of free parameters; BIC = Bayesian information criteria; 2ΔLL = 2-times log-likelihood difference; LMR p = p value associated to the Lo–Mendell–Rubin adjusted likelihood ratio test; BLRT p = p value associated to the bootstrapped likelihood ratio test; n (%) = number and percentage of class members; PP = posterior probability of a class.
Thus, a qualitative evaluation of the profiles that emerged from K3 and K2 was necessary. C1K2 and C2K2 were qualitatively similar to C1K3 and C3K3, respectively, but they differed in quantitative terms. Indeed, C1K2 and C1K3 drew highly comparable trajectories, even though C1K2 variable means were higher than those of C1K3. Similarly, C2K2 and C3K3 were qualitatively comparable, but C2K2 variable means were lower than those of C3K3. By contrast, the trajectory of C2K3 was in between those of C1K3 and C3K3, and it was qualitatively different from the trajectories that emerged in the two-class model. A contingency table between the two solutions (i.e., K2 and K3) provided an explanation about what happened moving from the three- to the two-class solution. Indeed, no members of C3K3 were also included in C1K2 and no members of C1K3 were also members of C2K2. This is the reason behind the similarities between the two pairs of classes mentioned above (i.e., C1K2-C1K3 and C2K2-C3K3).
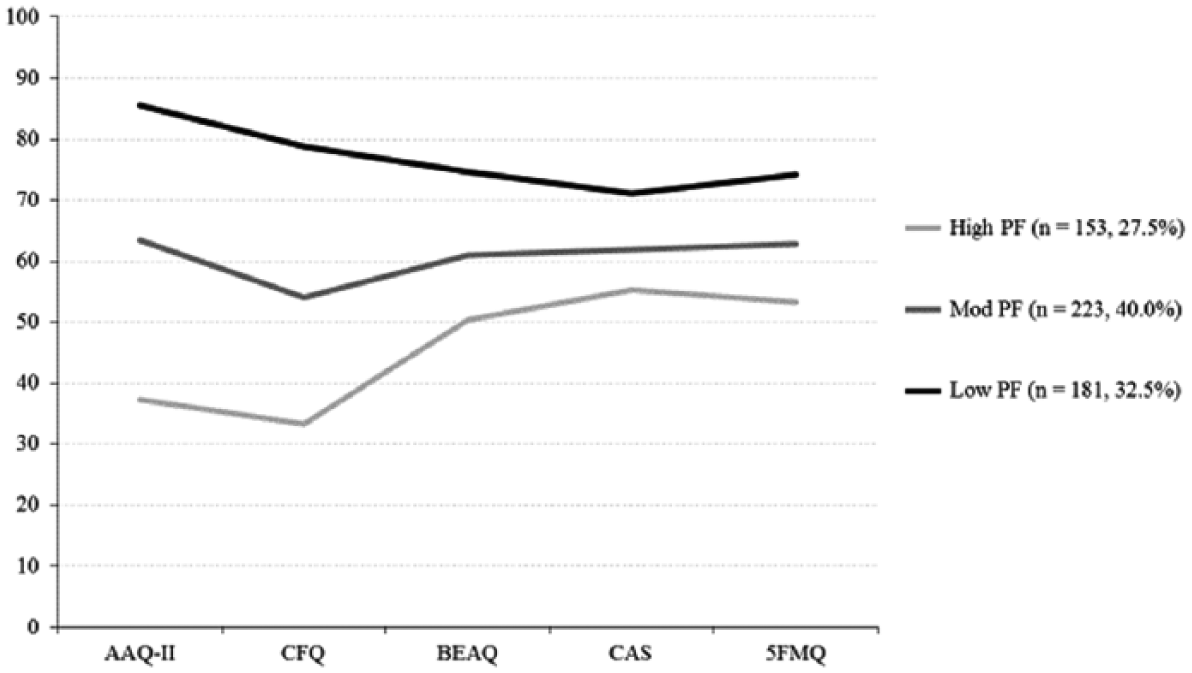
However, both the K2 classes included a high proportion of cases that were then classified in class C2K3 and that moved close and softened their trajectories compared with those of C1K3 and C3K3. In particular, C1K2 consisted of 53.5% of C1K3 members and 46.5% of C2K3 members, whereas C2K2 consisted of 66.8% of C3K3 members and 33.2% of C2K3 members. In other words, the qualitatively new profile observed in K3 (i.e., C2K3) was split in about two halves that joined C1K3 and C3K3 and formed C1K2 and C2K2 in the two-class solution. Given the uniqueness of C2K3’s trajectory and the higher discrimination between C1K3 and C3K3 compared to that between their counterparts C1K2 and C2K2, the three-class solution (i.e., K3 model) was considered the best model to explain our data (see Figure 1; Table 2).
The results of the three-class model “K3.”
The Means and Standard Deviations Across the Five Measures in the Three-Class Model Solution.
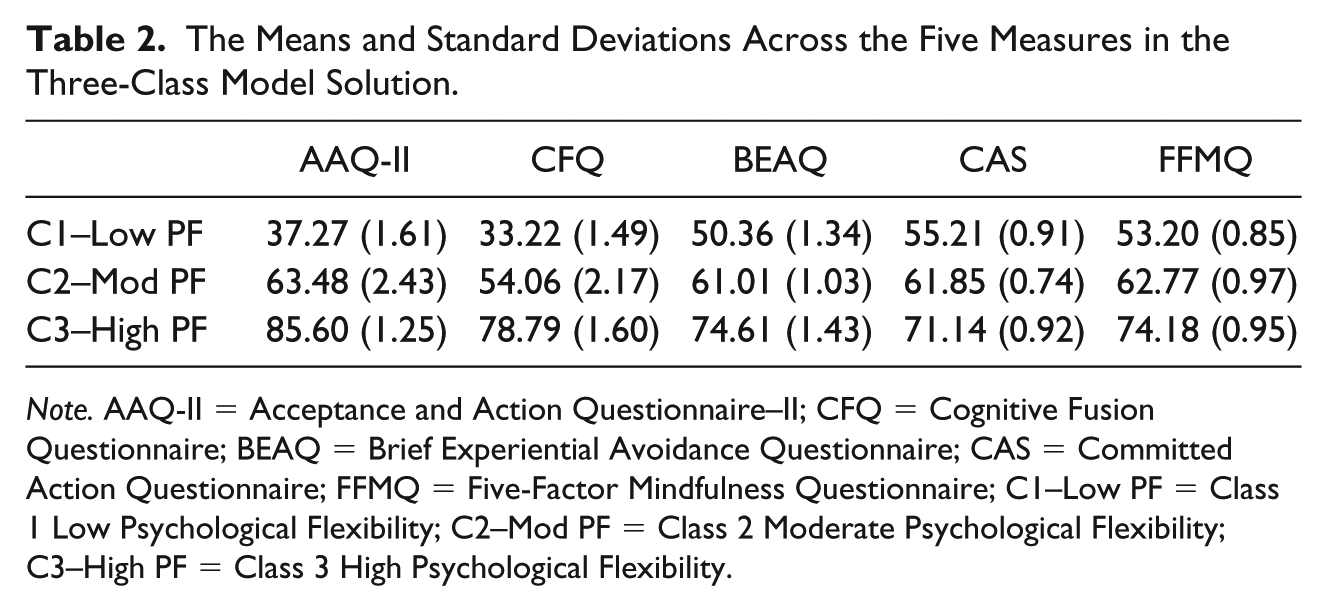
Note. AAQ-II = Acceptance and Action Questionnaire–II; CFQ = Cognitive Fusion Questionnaire; BEAQ = Brief Experiential Avoidance Questionnaire; CAS = Committed Action Questionnaire; FFMQ = Five-Factor Mindfulness Questionnaire; C1–Low PF = Class 1 Low Psychological Flexibility; C2–Mod PF = Class 2 Moderate Psychological Flexibility; C3–High PF = Class 3 High Psychological Flexibility.
Differences Among the Profiles of Psychological Flexibility
Psychological variables
The between-subjects ANOVA yielded significant results for all the psychological variables, indicating that the profiles differed for the levels of depression, F(2, 554) = 214.7, p < .001, η2 = .44; anxiety, F(2, 554) = 118.9, p < .001, η2 = .30; stress, F(2, 554) = 163.0, p < .001, η2 = .37; positive emotions, F(2, 554) = 67.3, p < .001, η2 = .20; and negative emotions, F(2, 554) = 262.4, p < .001, η2 = .49. Figure 2 shows means and standard errors of the variables for each profile. A series of Bonferroni post hoc tests was performed to detect differences among profiles. The results revealed that all the pairwise comparisons were significantly different, p < .001. Specifically, Class 3 (denoted as Low Psychological Flexibility; 32.5%) showed the highest level of depression, M = 18.58, SD = 5.10; anxiety, M = 15.03, SD = 4.52; stress, M = 18.61, SD = 4.41; negative emotions, M = 20.58, SD = 4.29; and the lowest level of positive emotions, M = 17.84, SD = 4.54; Class 1 (denoted as High Psychological Flexibility; 27.5%) showed the lowest level of depression, M = 9.26, SD = 2.76; anxiety, M = 8.93, SD = 2.21; stress, M = 10.81, SD = 3.08; and negative emotions, M = 11.24, SD = 2.68; and the highest level of positive emotions, M = 23.62, SD = 4.27; finally, Class 2 (Moderate Psychological Flexibility; 40%) showed intermediate levels of depression, M = 13.04, SD = 4.25; anxiety, M = 11.43, SD = 3.81; stress, M = 14.14, SD = 4.21; negative emotions, M = 14.87, SD = 4.03; and positive emotions, M = 20.63, SD = 4.77.
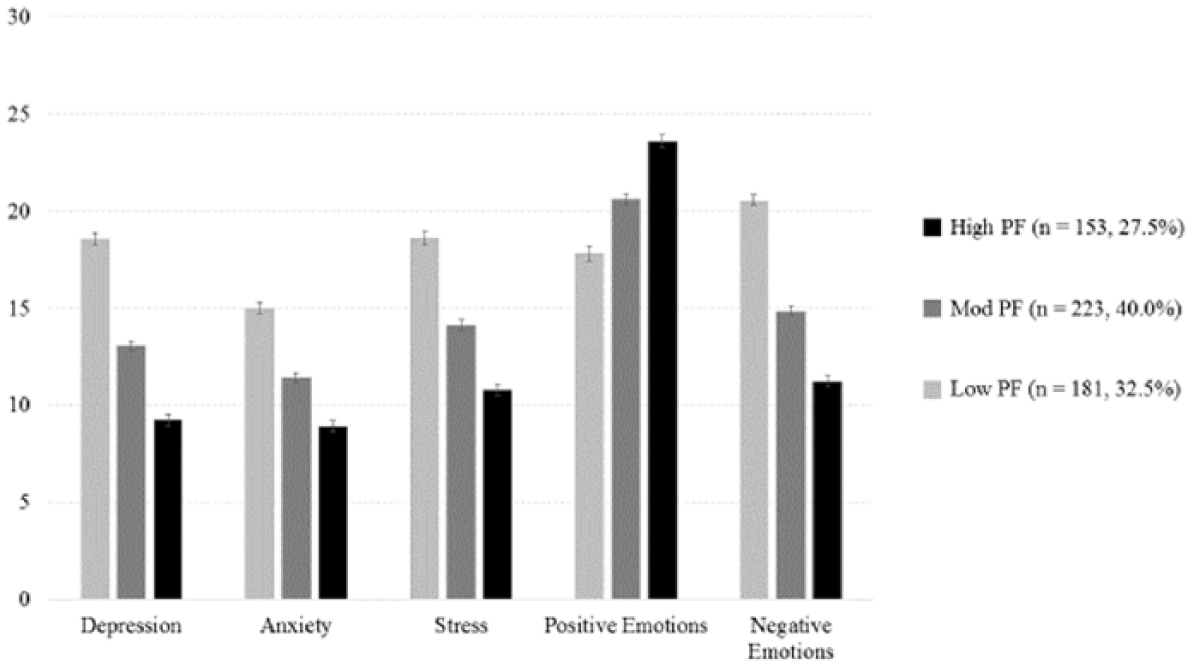
The results of the ANOVAs conducted on the psychological variables of depression, stress, anxiety (i.e., DASS-21), and positive and negative emotions (I-PANAS); means and standard errors of the K3 classes are displayed.
Sociodemographic variables
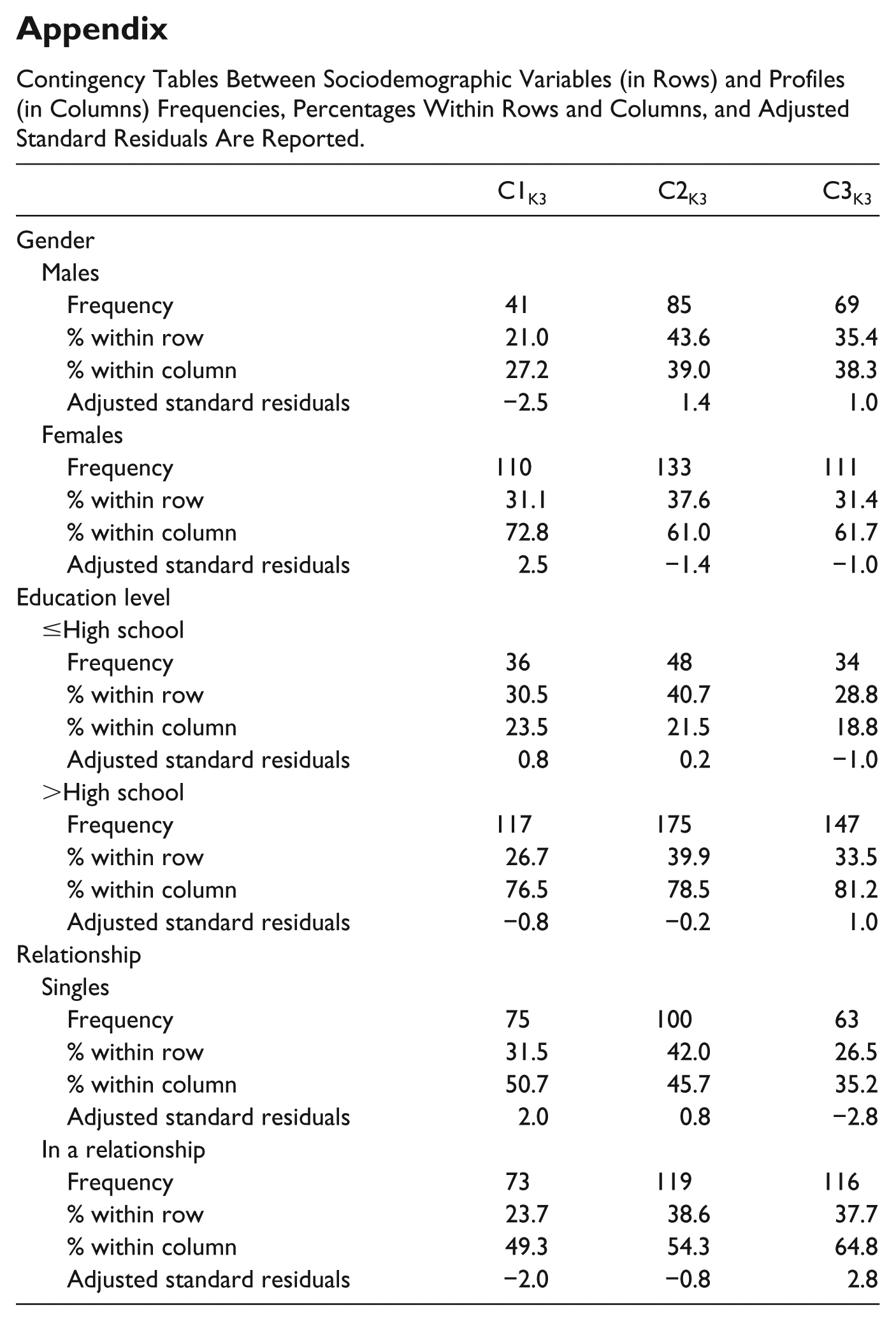
The between-subjects ANOVA on age was significant, F(2, 554) = 19.52, p < .001, η2 = .07. A Bonferroni post hoc test revealed that Class 1 (High Psychological Flexibility), M = 31.88, SD = 13.88, significantly differed from Class 3 (Low Psychological Flexibility), M = 25.39, SD = 7.91, and Class 2 (Moderate Psychological Flexibility), M = 26.20, SD = 9.37, p < .001, but no difference was detected between the two latter profiles. Concerning the other sociodemographic variables, the appendix reports contingency tables between these variables and the profiles. Gender, χ2(2) = 6.39, p = .041, and relationship status, χ2(2) = 8.53, p = .014, were significantly associated with the profiles, whereas education level was not, χ2(2) = 1.14, p = .56. Adjusted standardized residuals (ASRs) were then computed for each cell of the tables and examined to detect deviations from a random distribution of cases. Indeed, an ASR higher than 2.0 (or lower than −2.0) indicates that cases in that cell are overrepresented (or underrepresented) compared with what would be expected by chance. Concerning gender, males were underrepresented (and females overrepresented) in Class 3 (Low Psychological Flexibility). Concerning relationship, singles were overrepresented in Class 1 (High Psychological Flexibility) and underrepresented in Class 3 (Low Psychological Flexibility), whereas the opposite was observed for participants in a relationship.
Discussion
In the present study, we aimed to identify distinct subgroups among psychologically flexible or inflexible individuals based on profiles of key constructs of the ACT model. Moreover, a further aim was to explore whether such potential classes could discriminate self-reported symptoms of psychological distress (i.e., depression, anxiety, and stress) and levels of positive and negative emotionality. Three subgroups were identified. First subgroup is High Psychological Flexibility characterized by low levels of experiential avoidance and cognitive fusion, and high levels of present-moment awareness and committed action. Moreover, the High Psychological Flexibility subgroup reported low levels of depression, anxiety, stress, and negative emotions while endorsing a high level of positive emotions. Second subgroup is Moderate Psychological Flexibility characterized by medium to moderate levels of experiential avoidance, cognitive fusion, present-moment awareness, committed action. Conjointly, the Moderate Psychological Flexibility subgroup reported moderate levels of depression, stress, anxiety, and positive and negative emotions. Third subgroup is Low Psychological Flexibility characterized by high levels of experiential avoidance and cognitive fusion and low levels of mindful awareness and committed action. Furthermore, the Low Psychological Flexibility subgroup endorsed high levels of depression, stress, and anxiety, along with high levels of negative emotions and low levels of positive emotions. Thus, our results highlight that subgroups of psychologically flexible or inflexible individuals can be clearly distinguished based on core components of the ACT model. Furthermore, each of the three classes of psychological flexibility identified here reported significantly different levels of psychological distress and positive and negative emotionality.
The present study provides support for the utility of the broad spectrum of the ACT model of psychological flexibility, rather than overreliance on single measures of psychological flexibility or inflexibility. Moreover, the current data are noteworthy clinically in that the High Psychological Flexibility class all reported DASS-21 (i.e., depression, anxiety, and stress) scores lower than 12 while the Low Psychological Flexibility class reported distress scores of 15 or over on all three DASS components. The fact that the that LCA identified a Low Psychological Flexibility group in a non-clinical sample to report scores in what is considered within a moderately distressed range highlights the potential clinical utility of the overarching construct of psychological flexibility/inflexibility (see also Gloster et al., 2017; Levin et al., 2014). It is worth noting at this point, that as is typically the case with LCA, that the labels assigned (i.e., High, Moderate, and Low Psychological Flexibility) are descriptive and cautious in their designation and scope. It is possible, of course, to generate and assign other more eye-catching labels. However, we feel that these terms best describe the three distinct classes without extrapolating beyond the data that emerged in our analyses based on what is generally reported in the empirical literature using these scales employed.
It was interesting to observe (see Figure 1) across the three separate profiles of psychological flexibility that three particular subcomponent processes—experiential avoidance, committed action, and mindfulness/contact with the present moment—were remarkably stable in that if you knew a person’s score on experiential avoidance, you could quite readily predict their score on committed action and contact with the present moment with reasonable accuracy. Likewise, if you knew a person’s level of committed action, you could quite feasibly predict their probable level of experiential avoidance and contact with the present moment. This might suggest that experiential avoidance, committed action, and present-moment awareness together form a particular cluster within psychological flexibility that likely shares an underlying latent factor. Furthermore, psychological inflexibility as assessed by the AAQ-II and cognitive fusion appeared to form a separate cluster within the overall model. This is somewhat unsurprising as the items of both the AAQ-II and CFQ have been found to load onto the same factor in certain samples (Gillanders et al., 2014; Scott et al., 2016).
There are various competing iterations of the underlying conceptual model of psychological flexibility/inflexibility in the literature (Christodoulou et al., 2018). In general terms, they are purported as (a) the six interrelating components structure outlined above with the overarching construct of psychological inflexibility (Hayes et al., 2006), (b) a three-factor structure (i.e., Hayes et al., 2011, conceptualization of three pairs or dyads of the original six components comprising acceptance and defusion, present-moment awareness and self-as-context, and values and committed action; see also Francis et al., 2016; Vowles et al., 2014), and (c) a two-factor solution consisting of mindfulness and acceptance, and commitment and behavior change (e.g., as noted earlier Scott et al., 2016, proposed a general underlying openness factor along with two distinct components of decentering and committed action; see also Villatte et al.’s, 2016, ACT OPEN and ACT ENGAGED modules). As the present study did not include measures of all six components of the psychological inflexibility model, it is not possible to fully endorse any of the three competing conceptual models. However, as noted above, what we can gauge from this LCA approach is that present-moment awareness (i.e., mindfulness) and acceptance (i.e., opposite of experiential avoidance as measured by the BEAQ) and committed action appear to form a quite stable latent cluster. This does not fit readily with Scott et al.’s distinction between decentering and committed action as separate factors within the model. As acknowledged earlier, as we did not measure self-as-content/self-as-context or values, it is difficult to elucidate which conceptual model appears to have superior explanatory power. Nonetheless, the present data (see Figure 1) seem to suggest that the component processes have a complex interrelationship that suggests there might be more support for a three- or two-factor structure. Moreover, it seems from the present study that considering experiential avoidance and cognitive fusion as a pair or dyad (e.g., Hayes et al., 2011) within the overall model might not be useful as they appear functionally distinct, at least according to the somewhat limited self-report measures of these constructs (i.e., BEAQ and CFQ).
Furthermore, it was not possible within the design of the present study (i.e., single time-point cross-sectional method) to examine any cause and effect relationship between individual subcomponents of the model and overarching construct of psychological inflexibility. As noted by Kashdan and Rottenberg (2010), among others, it is difficult to assess whether psychological inflexibility causes experiential avoidance, cognitive fusion, inaction, and so on, or whether these components cause a person to be psychologically inflexible in their behavior. This causal directionality problem remains a significant concern for theorists working with the psychological inflexibility model (Christodoulou et al., 2018). One approach that future researchers could consider employing is latent growth curve analysis with data collection at multiple time points.
There could be a case for arguing that the ACT model of psychological flexibility/inflexibility does not espouse such psychometric measures of subcomponent processes of the model as “trait-like” constructs. Thus, it could be debated that a LCA might not actually fit with how ACT processes are conceptualized or operationalized. For example, in some ACT writings, the six component processes are referred to as skills that can be altered or modified, rather than traits that are somewhat fixed (see Christodoulou et al., 2018). However, it is apparent in some recent psychometric measure developments that, for example, the measure of cognitive fusion employed here (the CFQ) was designed as a trait measure because Bolderston et al. (2018) have developed and validated a separate State Cognitive Fusion Questionnaire (SCFQ). Therefore, it is clear that at least in the manner that the measures employed in the present study were designed as instruments to assess trait-like constructs and indeed are typically utilized by researchers in the empirical literature as such, that there is ample justification for examining the psychological flexibility model with latent class approaches.
There exists some degree of uncertainty and confusion over the construct and discriminant validity of some key ACT process measures (e.g., Rochefort, Baldwin, & Chmielewski, 2018; Scott et al., 2016; Vaughan-Johnston, Quickert, & MacDonald, 2017; Wolgast, 2014), and debate over how to assess the broad overarching construct of psychological inflexibility more generally (e.g., Fergus et al., 2012; Francis et al., 2016; Renshaw, 2018). The present study provides further support for the position that the AAQ-II and the BEAQ assess experiential avoidance in different ways or might not measure the same construct (e.g., Gámez et al., 2014; Rochefort et al., 2018; Tyndall, Waldeck, Pancani, et al., 2018). The BEAQ scores were quite stable with respect to committed action and contact with the present moment across all three subgroups of psychological flexibility whereas the AAQ-II scores were the most volatile or unstable. For example, at low levels of psychological flexibility, the AAQ-II scores were lower than BEAQ scores, while at high levels of psychological flexibility, the AAQ-II scores were higher than BEAQ scores. Scores on both measures were quite similar at moderate levels of psychological flexibility though. It could be argued that the AAQ-II scores being so different from BEAQ scores at low and high levels of psychological flexibility indicate that it is a more useful measure of experiential avoidance as it might more reliably represent the level of a person’s psychological distress or well-being than the BEAQ. However, it could also be argued that the AAQ-II scores at low and high levels of psychological flexibility support Wolgast’s (2014) proposition that the AAQ-II is actually a measure of psychological distress (see also Rochefort et al., 2018’s claim that it reflects the personality trait of neuroticism) rather than experiential avoidance. A cautious interpretation from the present study is that, as the BEAQ scores fit more readily with levels of committed action and contact with the present moment, the BEAQ is the more effective or favorable measure of experiential avoidance taking the overall ACT model into account. It should be acknowledged that it might take some time for this message to permeate the field as the use of the AAQ-II to assess experiential avoidance remains deeply ingrained in the clinical and non-clinical literatures (e.g., Blakey et al., 2017; Karademas et al., 2017; Karekla & Panayiotou, 2011; Monestès et al., 2018).
While no specific a priori predictions were made regarding sociodemographic variables and psychological flexibility as there was little extant empirical literature to suggest expected differences, it was intriguing to note the higher levels of psychological flexibility among single persons than those in relationships. This interesting finding needs to be further explored in future research. Females were more likely than males to be characterized by low levels of psychological flexibility. Indeed, previous research has demonstrated that females tend to experience higher levels of psychological distress and utilize avoidant coping strategies compared with males (Matud, 2004). Furthermore, the education level achieved by an individual had no relationship to their profile of psychological flexibility. Future researchers could explore these observed gender and relationship differences in greater depth and in different contexts (e.g., specific psychological disorders) to see whether they represent a stable finding or one unique to the present study sample.
A limitation of the present study is that it relied exclusively on self-report questionnaire measures at one time point. Thus, it is possible that shared variance effects could have inflated associations between variables. A second potential limitation could be that we employed a measure of mindfulness best represented by a five-factor solution as a single measure. We acknowledge that this is not ideal, and future researchers could be encouraged to employ a different measure such as the Mindfulness Attention Awareness Scale (MAAS; Brown & Ryan, 2003) instead. A further limitation of the current study is that it did not assess self-as-content or values due to a lack of sufficient empirical support (but see Moran, Almada, & McHugh, 2018) for measures of these sub-component processes for our purposes. However, it should be acknowledged that a number of instruments have been developed and researchers could consider including measures such as the Valuing Questionnaire (Smout, Davies, Burns, & Christie, 2014) and the Self Experiences Questionnaire (Yu, McCracken, & Norton, 2016) in future LCA analyses of the psychological inflexibility model. Similarly, future research could consider alternative measures of the overarching construct of psychological flexibility such as the Comprehensive Assessment of Acceptance and Commitment Therapy (CompACT; Francis et al., 2016), the Avoidance and Fusion Questionnaire (Greco, Baer, & Lambert, 2008), or the Multidimensional Psychological Flexibility Inventory (MPFI; Rolffs, Rogge, & Wilson, 2018), rather than the AAQ-II administered here. Researchers should be mindful, however, of the fact that it is not well known, as of yet, whether adding more indicators to a LCA is a positive or negative analytic strategy (Wurpts & Geiser, 2014).
Future research could consider applying a LCA to samples in a variety of clinical domains such as social anxiety disorder, clinical depression, obsessive-compulsive disorder, eating disorders, and post-traumatic stress disorder. Indeed, a LCA with particular clinical subpopulations could potentially aid in the development of tailored therapeutic interventions for specific groups. For example, it might emerge that different psychological disorders or conditions are typically characterized by rather distinctive clusters or profiles.
In conclusion, the current study represents an important addition to the literature as the first study to identify distinct subgroups of psychological flexibility based on core constructs of the ACT model using a LCA. From a clinical perspective, this discovery was important as each of the three subgroups or classes of psychological flexibility reported significantly different levels of psychological distress and emotionality. This could aid clinicians and researchers to more accurately represent a client’s level of psychological flexibility across the broader spectrum of the ACT model, rather than the heretofore more typically reported reliance on one measure of psychological flexibility alone. Furthermore, such analyses as these could help provide clinicians with a more nuanced picture of mediation effects in ACT-based intervention studies to give a clearer picture as to which specific subcomponents of psychological flexibility drive the improvements often observed. We hope that the current study serves to stimulate much needed research on subcomponent processes within the ACT model of psychological flexibility.
Footnotes
Appendix
Contingency Tables Between Sociodemographic Variables (in Rows) and Profiles (in Columns) Frequencies, Percentages Within Rows and Columns, and Adjusted Standard Residuals Are Reported.
| C1K3 | C2K3 | C3K3 | |
|---|---|---|---|
| Gender | |||
| Males | |||
| Frequency | 41 | 85 | 69 |
| % within row | 21.0 | 43.6 | 35.4 |
| % within column | 27.2 | 39.0 | 38.3 |
| Adjusted standard residuals | −2.5 | 1.4 | 1.0 |
| Females | |||
| Frequency | 110 | 133 | 111 |
| % within row | 31.1 | 37.6 | 31.4 |
| % within column | 72.8 | 61.0 | 61.7 |
| Adjusted standard residuals | 2.5 | −1.4 | −1.0 |
| Education level | |||
| ≤High school | |||
| Frequency | 36 | 48 | 34 |
| % within row | 30.5 | 40.7 | 28.8 |
| % within column | 23.5 | 21.5 | 18.8 |
| Adjusted standard residuals | 0.8 | 0.2 | −1.0 |
| >High school | |||
| Frequency | 117 | 175 | 147 |
| % within row | 26.7 | 39.9 | 33.5 |
| % within column | 76.5 | 78.5 | 81.2 |
| Adjusted standard residuals | −0.8 | −0.2 | 1.0 |
| Relationship | |||
| Singles | |||
| Frequency | 75 | 100 | 63 |
| % within row | 31.5 | 42.0 | 26.5 |
| % within column | 50.7 | 45.7 | 35.2 |
| Adjusted standard residuals | 2.0 | 0.8 | −2.8 |
| In a relationship | |||
| Frequency | 73 | 119 | 116 |
| % within row | 23.7 | 38.6 | 37.7 |
| % within column | 49.3 | 54.3 | 64.8 |
| Adjusted standard residuals | −2.0 | −0.8 | 2.8 |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.