
Abstract
Social skills interventions are critical for promoting social, emotional, and behavioral competence for students with or at risk of emotional and behavioral disorders (EBD) and autism spectrum disorders (ASD). This single-case meta-analysis examined the effects of social skills interventions (SSIs) for students with EBD and ASD. Effect sizes were calculated for 78 cases across 25 included studies using a nonparametric effect size, Baseline Corrected Tau. The overall weighted mean effect size of 0.54 suggested a moderate effect across the 25 studies. The overall weighted mean effects for studies reporting maintenance and generalization data were 0.68 and 0.37, respectively. Potential moderators examined (disability, intervention design, intervention delivery, methodological quality) were not significant. As such, they did not moderate the outcomes for participants. We conducted a post hoc analysis and hypothesized that between-study differences may be more meaningful than the similarities shared by participants in the same moderator groups. Implications are discussed on using SSIs to address the social, emotional, and behavioral challenges of students with or at risk of EBD and ASD.
The social, emotional, and behavioral challenges posed by students with emotional and behavioral disorders (EBD) and autism spectrum disorders (ASD) are a common issue in school-based settings (Forness, Freeman, Paparella, Kauffman, & Walker, 2012; H. M. Walker, Colvin, & Ramsey, 1995; S. Wang, Cui, & Parrila, 2011). Students with EBD exhibit externalizing problems and antisocial behaviors that include a conduct-related issues, failure to abide by rules, defiance of authority, conflicts with peers, and an avoidance of responsibility, as well as internalizing problems such as anxiety, depression, and withdrawal (Bradshaw, Schaeffer, Petras, & Ialongo, 2010; Forness et al., 2012; Sprague, Sugai, & Walker, 1998). Challenging social, emotional, and behavioral problems are characteristic of students with ASD as well, particularly those who are higher functioning (S. Wang et al., 2011). For example, it is not uncommon for individuals with ASD to experience social skills deficits, aggression, self-injurious behavior, and the inability to regulate or appropriately adjust their behaviors (e.g., McDougle, 2016). Although the etiology is different, these behavioral challenges can impede social, behavioral, and academic progress for both students with EBD and ASD.
Social Skills Interventions (SSIs)
SSIs are critical for promoting social, emotional, and behavioral competence for students with EBD and/or ASD. Social skills are critical to promoting social, emotional, and behavioral competence (Gresham, 2015). Gresham (2015) described social skills as being “academic enablers” and competing problem behaviors as “academic disablers” (p. 101). Moreover, social skills have been conceptualized as consisting of skill-based or performance-based deficits (Gresham, Sugai, & Horner, 2001; H. M. Walker, Ramsey, & Gresham, 2004). According to this social–behavioral model (Gresham, 1981, 1985, 2018), students have either not learned a particular social skill (namely, skill deficit), or they have learned the skill but do not perform it (namely, performance deficit). Conceptually, SSIs have developed over time from an intervention focus on discrete behavioral skills (e.g., eye contact) to now include social, cognitive, and emotional constructs and can be categorized into at least three areas: (a) social interactions, (b) prosocial behavior, and (c) social–cognitive skills (Gresham, 2015). Both group and single-case research designs have been used to evaluate SSIs for children and youth with EBD and/or ASD. Previous meta-analytic reviews on SSIs have included studies using single-case research designs for students with EBD (Mathur, Kavale, Quinn, Forness, & Rutherford, 1998) and students with ASD (e.g., Bellini, Peters, Benner, & Hopf, 2007; N. Schneider, Goldstein, & Parker, 2008; S. Wang et al., 2011; S. Wang, Parrila, & Cui, 2013). Others reviewed group designs that used SSIs for students with EBD (e.g., Ang & Hughes, 2002; Beelmann, Pfingsten, & Lösel, 1994; Cook et al., 2008; Quinn, Kavale, Mathur, Forness, & Rutherford, 1999). P. Wang and Spillane (2009) reviewed both single-case research (SCR) and group studies for students with ASD.
There are a number of narrative and quantitative reviews summarizing SSIs that collectively point to SSIs as being effective in promoting the acquisition and performance of social skills for students with or at risk of EBD (Cappadocia & Weiss, 2011; Flynn & Healy, 2012; Gillis & Butler, 2007; Gresham, 1981, 1985; Gresham & MacMillan, 1997; Maag, 2006; Reichow, Volkmar, & Cicchetti, 2008; White, Keonig, & Scahill, 2007). The meta-analyses of group design studies evaluating the effects of SSIs for students with or at risk of EBD have reported low to moderate effect sizes (Ang & Hughes, 2002; Beelmann et al., 1994; Cook et al., 2008; Quinn et al., 1999; B. H. Schneider, 1992). For example, B. H. Schneider (1992) reported an overall average effect size of r = .40 across 79 reviewed studies for participants that included children and youth described as “withdrawn,” “aggressive,” “at-risk,” and “unpopular with peers” (p. 368). In the meta-analysis by Beelmann et al. (1994), larger effect sizes were reported for problem-solving measures (g = .78), whereas smaller effect sizes were reported for behavior ratings (g = .26) of students with externalizing and internalizing behaviors, and those described as “at-risk” (p. 263). Later meta-analyses also reported a range of outcomes. Quinn et al. (1999) reported an overall effect size of d = .20 across 35 group design studies for students with EBD, whereas Ang and Hughes (2002) analyzed 38 studies on SSIs for antisocial youth with an overall effect size of ∆ = .62. Cook et al. (2008) synthesized the meta-analytic literature on SSIs for secondary students with or at risk of EBD. Their study included five meta-analyses and reported an overall weighted mean effect size of r = .32, indicating two thirds of students with or at risk of EBD (compared with one third of students in control groups) showed improvements following intervention.
Several reviews of SSIs have focused on students with ASD. Bellini et al. (2007) used percent of nonoverlapping data (PND; Scruggs, Mastropieri, & Casto, 1987) to analyze 55 single-case design studies researching SSIs for children with ASD resulting in a mean PND of 70%. P. Wang and Spillane (2009) reviewed 36 single-case and two-group design studies that included students with ASD. They found PNDs of 67.21% for social stories, 60.69% for peer-mediated, 84.25% for video modeling, and 100% for cognitive-behavioral training. N. Schneider et al. (2008) used the percentage of all nonoverlapping data points (PAND; Parker, Hagan-Burke, & Vannest, 2007) and the Phi statistic to calculate an overall effect size. An average weighted Phi of .71 was found for peer-mediated SSIs for students with ASD. Two single-case meta-analyses on SSIs for students with ASD used hierarchical linear modeling (HLM) to examine outcomes across multiple social skills studies (S. Wang et al., 2011; S. Wang et al., 2013). Both studies indicated that SSIs were effective in improving the social behavior of children with ASD, reporting γ = 1.27 (S. Wang et al., 2011) and γ = 1.40 (S. Wang et al., 2013).
In general, the previous reviews and meta-analysis point to greater effects for students with ASD than EBD. Mathur et al. (1998) was the only review that conducted a meta-analysis of single-case research that included both students with EBD and ASD. A total of 64 studies were included with 283 students with or at risk of EBD and students with ASD. The mean PND across all studies was 62% (SD = 33%).
Several meta-analyses identified differential effects for SSIs based on a number of variables including theoretical approach, intervention type, group composition, intervention strategy, implementation format, disability, and school level (Ang & Hughes, 2002; Bellini et al., 2007; Cook et al., 2008; Mathur et al., 1998; B. H. Schneider, 1992; P. Wang & Spillane, 2009). With regard to outcome measures, greater intervention effects were reported for promoting social interaction skills than communication skills (Mathur et al., 1998). Few reviews reported the effects of SSIs on maintenance or generalization. However, P. Wang and Spillane (2009) reported mean PND effect sizes for those single-case studies that included maintenance and generalization and reported an overall maintenance PND of 78.5% (range = 38%-100%), and an overall generalization of 80.95% (range = 40%-100%). In addition, Bellini et al. (2007) reported a range of maintenance effects (n = 25; PND M = 80%, range = 17%-100%) and lower generalization effects (n = 15; PND M = 53%, range = 17%-100%).
Single-Case Meta-Analysis
Single-case research relies on direct and systematic replication to build an evidence base for a particular practice or intervention (Horner et al., 2005). Meta-analysis procedures are increasingly being applied to single-case designs to empirically evaluate the external validity and generalizability of research using single-case designs (Kratochwill & Levin, 2014). An individual single-case design has strong internal validity but weak external validity (Horner et al., 2005), and meta-analytic procedures provide a well-established method of aggregating individual studies. However, there is no consensus about the best method for the data analysis of single-case studies. Several statistical methods (nonoverlap, regression based, etc.) are currently promoted for the quantitative analysis of single-case studies, each with unique strengths and limitations. One popular effect size statistic recommended for single-case meta-analysis is Tau-U, a modified form of Kendall’s rank order correlation Tau (Parker, Vannest, & Davis, 2011; Parker, Vannest, Davis, & Sauber, 2011; Vannest, Parker, Gonen, & Adiguzel, 2016). Tau-U has been adopted in a number of single-case meta-analyses (e.g., Bowman-Perrott et al., 2013; Dart, Collins, Klingbeil, & McKinley, 2014; Whalon, Conroy, Martinez, & Werch, 2015). However, a number of limitations have been noted by Tarlow (2017b) regarding the original Tau-U statistic. Notably, the baseline trend correction for the original Tau-U was found to produce inflated effect size estimates and “out-of-bounds” results, with Tau coefficients regularly falling outside of the −1 to +1 range. Tarlow introduced an improved rank correlation effect size statistic, Baseline Corrected Tau, which was designed to improve upon the Tau-U limitations.
Purpose and Research Questions
The purpose of this meta-analysis was to evaluate the overall effectiveness of single-case studies from 1998 to 2018 investigating SSIs for students with or at risk of EBD and ASD who display challenging social, emotional, or behavioral problems. Hutchins, Burke, Hatton, and Bowman-Perrott (2016) previously conducted a quality review extending the research conducted by Mathur et al. (1998) where the methodological quality of single-case social skills intervention studies from 1998 to 2014 was evaluated. The goal of the current study was to extend this prior quality review and focus on the effects of the SSIs included in Hutchins et al.’s (2016) study. Previous meta-analyses on SSIs have reported low to moderate effect sizes (Ang & Hughes, 2002; Cook et al., 2008; Mathur et al., 1998; Quinn et al., 1999). There has only been one single-case meta-analysis to date that specifically focused on SSIs that included both students with EBD and ASD (Mathur et al., 1998). The following research questions were examined:
Method
Study Identification
The initial pool of studies for this meta-analysis was developed from the quality review by Hutchins et al. (2016) of the single-case SSIs literature from 1998 to 2014. This data set was updated with an electronic search of psychology and educational databases (PsycINFO, ERIC, Academic Search Complete, and Education Full Text) to identify social skills intervention research from 1998 through 2018. Two sets of search terms were combined with the Boolean phrase AND. The first set of terms included behavioral disorders, emotional disorders, seriously emotionally disturbed, disruptive behavior, social behavior problems, antisocial behavior, autism, social behavior problems OR conduct disorders. The second set of terms included social skills training, social skills instruction OR social skills interventions. The search identified one additional article, resulting in a total of 24 articles published between 1998 and 2018 to be included in the current meta-analytic review (see Figure 1).
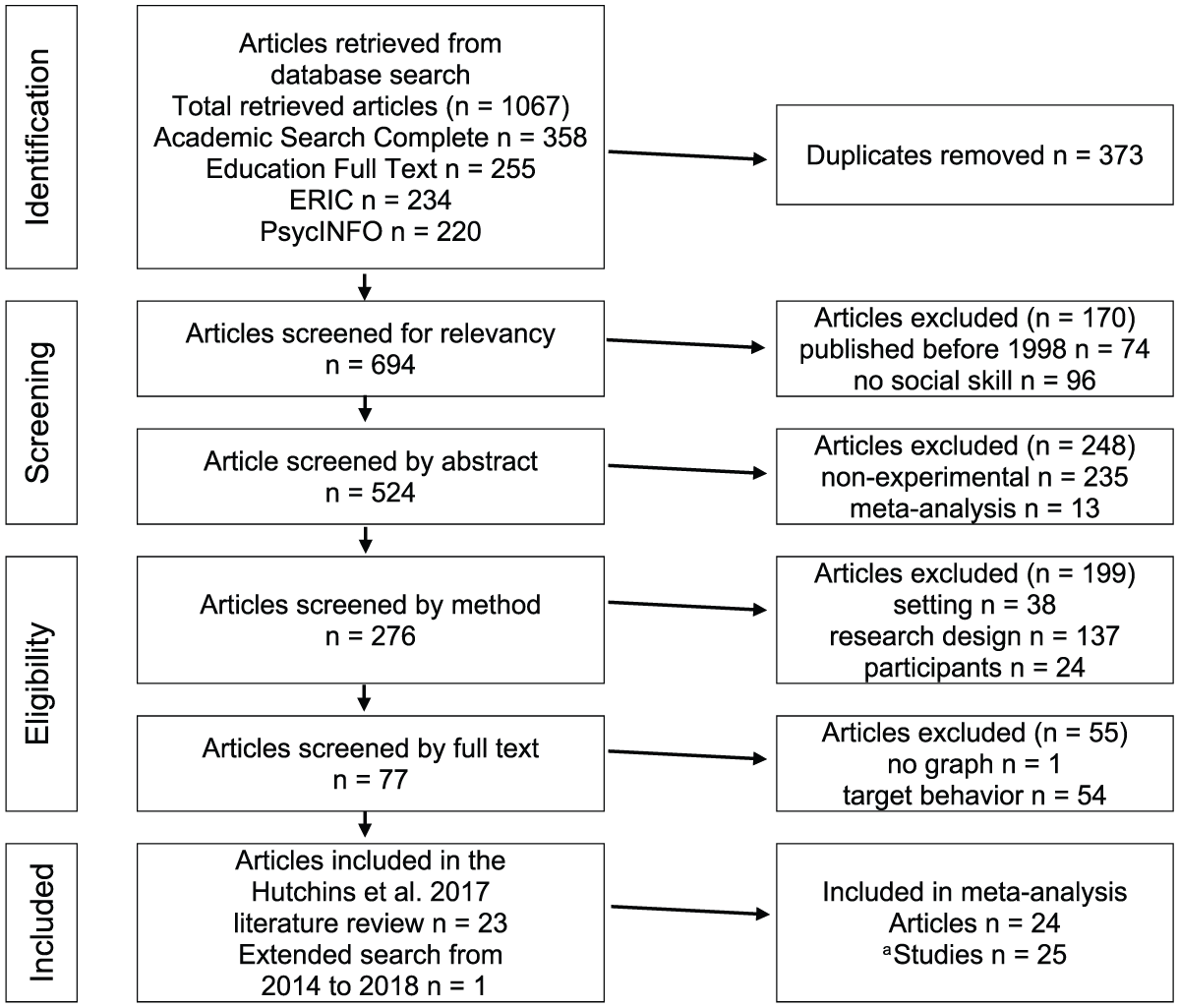
Article selection flowchart.
Inclusion and Exclusion Criteria
A total of 25 studies across 24 articles were included in this meta-analysis. Studies were included if (a) the study was conducted in a school setting; (b) the participants were described as children or youth with or at risk of EBD or as ASD who exhibited challenging social and behavioral problems; (c) the intervention implemented was based on teaching social skills; (d) the primary outcome measures assessed school- or classroom-based social behaviors; (e) they used single-case design methodology; and (f) they were written in English, conducted in the United States, and published in a peer-reviewed journal between 1998 and 2018. Although often valuable for examining the “gray literature,” dissertations and unpublished manuscripts were excluded and only published studies were considered for review that had undergone a peer review process. Because the focus of this study was on school-based settings, studies were also excluded if they were conducted in clinical facilities or in the home environment, or if the dependent measures did not include school- or classroom-related behaviors, use a group design, or did not report on experimental findings (e.g., systematic literature reviews, editorials, commentaries, or practitioner guides).
Study Coding
Information was extracted for coding moderators. Potential moderator variables evaluated in the present study were (a) disability, (b) intervention design, (d) intervention delivery, and (e) methodological quality. The coding scheme from Hutchins et al. (2016) was used in the current meta-analysis. Disability was coded as identified with/at risk of EBD or identified with ASD. Intervention design refers to the individualization of the SSIs to the student. Interventions were considered individualized if they were created specifically for the student and matched social skills taught to the student’s social skill deficits (i.e., problem behavior). Studies implementing established social skills curricula which taught a variety of social skills were coded as general SSIs. Intervention delivery was coded as alone or combined. Studies in which social skills training was the only intervention implemented were considered stand-alone SSIs and were coded alone. Studies in which SSIs were combined with other strategies such as self-monitoring, cueing, group contingency, or other forms of reinforcement were considered combined SSIs. Overall methodological quality ratings were coded as yes if the study met What Works Clearinghouse (WWC) design standards with or without reservations (Kratochwill et al., 2013), and no if the study did not meet design standards. Additional details on the methodological quality review process can be found in Hutchins et al. (2016).
Data Extraction
Numerical values for each graphed data point were extracted to format graphed data into comma separated files and calculate effect sizes between phase contrasts. A digitizing computer software program was used to extract graphed data from the included articles (GetData, 2012). For each study, the figures containing graphed data for measures of outcome variables were cropped and uploaded into the software program. Once uploaded, and the scale of the X and Y axes were set, values for each data point were extracted and exported into an Excel spreadsheet and formatted for analysis. Values were rounded to the nearest whole number when necessary. Excel spreadsheets containing extracted data were then categorized by baseline and intervention phases. Data for maintenance and generalization phases were also categorized where applicable.
Reliability
Reliability for article selection, descriptive coding, methodological quality coding, and effect size calculations were assessed. Simple percent agreement and Cohen’s Kappa, a more conservative measure of reliability adjusting for chance agreement (Suen & Ary, 1989), were calculated for each area of reliability. Simple percent agreement was calculated by dividing the sum of agreements by the total number of agreements plus disagreements multiplied by 100. Cohen’s Kappa was calculated using the Vassar stats website (Lowry, 2001). Percent agreement above 80% and Cohen’s Kappa values above .60 are considered acceptable (Kratochwill et al., 2013). Percent agreement and Cohen’s Kappa for article selection, descriptive coding, and methodological quality were 90% and .81, 87% and .70, and 100% and 1.0, respectively.
Data Analyses
Baseline Corrected Tau was used for effect sizes and was calculated with the R statistical software package (R Core Team, 2017) using syntax by Tarlow (2017a). It is noted that an online calculator for Baseline Corrected Tau is also available and yields the same results as the R syntax (http://ktarlow.com/stats/tau; Tarlow, 2016). Random-effects models were used to aggregate the 78 participant effect size estimates, both within their respective 25 studies and for one overall weighted mean. Four subgroup effects were also analyzed as moderators with random-effects models. R syntax adopted from Borenstein, Hedges, Higgins, and Rothstein (2009) was used to aggregate the data (Tarlow & Brossart, 2018). Before aggregating effect size estimates, Tau values were transformed to z statistics and mean z values were transformed back to Tau for reporting and interpretation (Kendall, 1962; D. A. Walker, 2003). The signs (+/–) of effect sizes were reversed so that positive effects sizes indicated improvement, regardless of whether intervention outcome reflected increasing or decreasing behavior. The random-effects meta-analyses yielded two heterogeneity statistics, Q and I2. Q tests the null hypothesis that between-participant variability is due only to sampling error. I2 indicates the percentage of observed between-participant variance beyond what would be expected from sampling error. When Q is statistically significant, and/or when I2 is large, there is reason to suspect participants are not homogeneous and may have been sampled from different populations. Subgroup (i.e., moderator) analyses tested the effect of (a) disability, (b) intervention design, (d) intervention delivery, and (e) methodological quality. Random-effects models with pooled variance (τ2) yielded Q*between and R2 statistics. The Q*between statistic may be interpreted similarly to an analysis of variance (ANOVA) F test. Statistically significant Q*between values indicate subgroup differences (i.e., moderator effects) are unlikely to be explained by sampling error. The R2 statistic indicated the proportion of variance (τ2) explained by the moderator variable, analogous to the ANOVA η2 (Borenstein et al., 2009). Intervention effect sizes and moderator analyses were all calculated using the first baseline-to-intervention phase contrast (i.e., A to B phase contrast). In cases where reversal designs (e.g., ABAB) were used, only the first A to B contrast was used to calculate an effect size. However, when data were available, effect sizes were calculated for maintenance (M) and generalization (G) probes with A to M phase contrasts and A to G phase contrasts, respectively. Ten studies with a total of 34 participants reported maintenance data, and three studies with a total of 11 participants reported generalization data. Maintenance and generalization effect sizes were aggregated within each study, and overall mean maintenance and generalization effects were estimated.
Results
Participant and Study Characteristics
Twenty-five studies across 24 articles published between 1998 and 2018 were analyzed. Studies included 78 participants with the majority of participants identified as male (85%, n = 66). Although race/ethnicity was not reported for 23 participants (29%), African American (32%, n = 25) and Caucasian (33%, n = 26) were the two ethnic groups with the greatest representation. All studies involved students with behavioral difficulties with 20 participants (26%) at risk of EBD, 28 participants (36%) identified with EBD, and 31 participants (38%) with ASD. The majority of students were educated in special education settings including specialized schools for students with disabilities (44%, n = 34), followed by general education settings (38%, n = 30). Fifteen of the participants (19%) were educated in both special education and general education settings, and more than half (53%, n = 42) of the interventions implemented were individualized to the participant. Multiple baseline designs were the most commonly used experimental design (68%, n = 17), followed by reversal/variation designs (16%, n = 4), and mixed designs (16%, n = 4). Finally, 11 studies (41% of participants; n = 32) evaluated the effect of SSIs on the increase of social skill behaviors, five studies (17% of participants, n = 13) evaluated the effect of SSIs on the decrease of problem behaviors, and nine studies (42% of participants, n = 33) collected data to evaluate the simultaneous increase of social skill and decrease of problem behavior.
Mean Effect Size of Social Skills Interventions
Random-effects means were first calculated to aggregate the participant effect size estimates within each of the 25 studies (six studies had only one participant). Mean effect sizes ranged from 0.22 to 0.75. The study-level mean effects were statistically significant for all but three studies. The random-effects mean for all 78 participants was Baseline Corrected Tau = 0.541, 95% confidence interval (CI) = [0.486, 0.591], p < .001. This is equivalent to a Cohen’s d effect size of 2.240. The weighted mean effects are summarized in Table 1. Heterogeneity statistics for the overall mean effect were statistically significant (Q = 453.93, p < .001) and indicated a large amount of variance among participants’ intervention effect sizes that were not explained by sampling error (I2 = 0.83). It was therefore expected that some moderator variable(s) accounted for this heterogeneity. Maintenance and generalization effect sizes are summarized in Table 2. The weighted mean effect sizes for all studies with maintenance (n = 10) and generalization (n = 3) data were statistically significant. The overall mean effect size for maintenance data (n = 34 participants) was Baseline Corrected Tau = 0.679, 95% CI = [0.630, 0.722], p < .001. The overall mean effect size for generalization data (n = 11 participants) was Baseline Corrected Tau = 0.369, 95% CI = [0.210, 0.506], p < .001.
Within-Study Random-Effects Meta-Analyses.
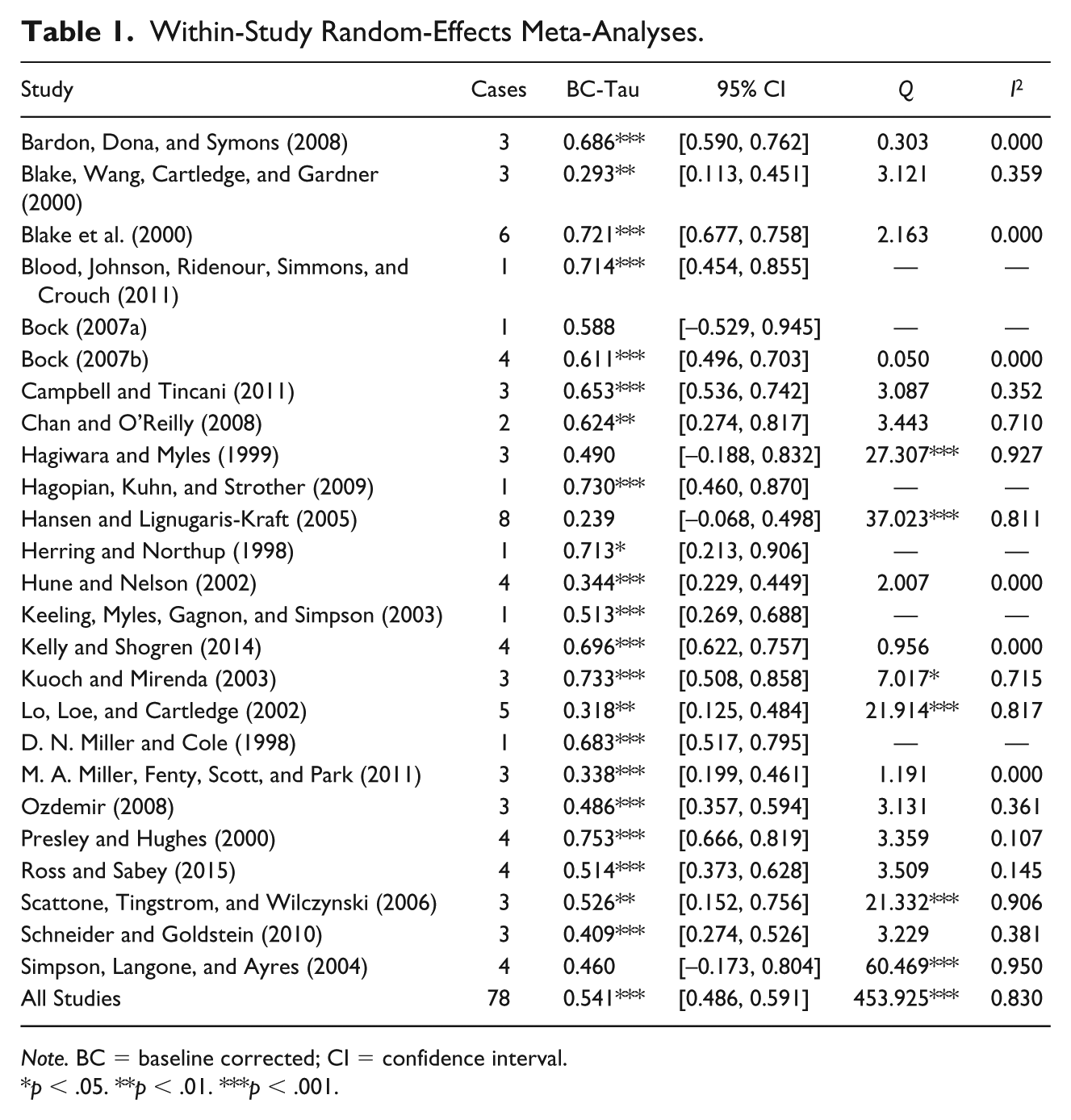
Note. BC = baseline corrected; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Maintenance and Generalization Effect Sizes.
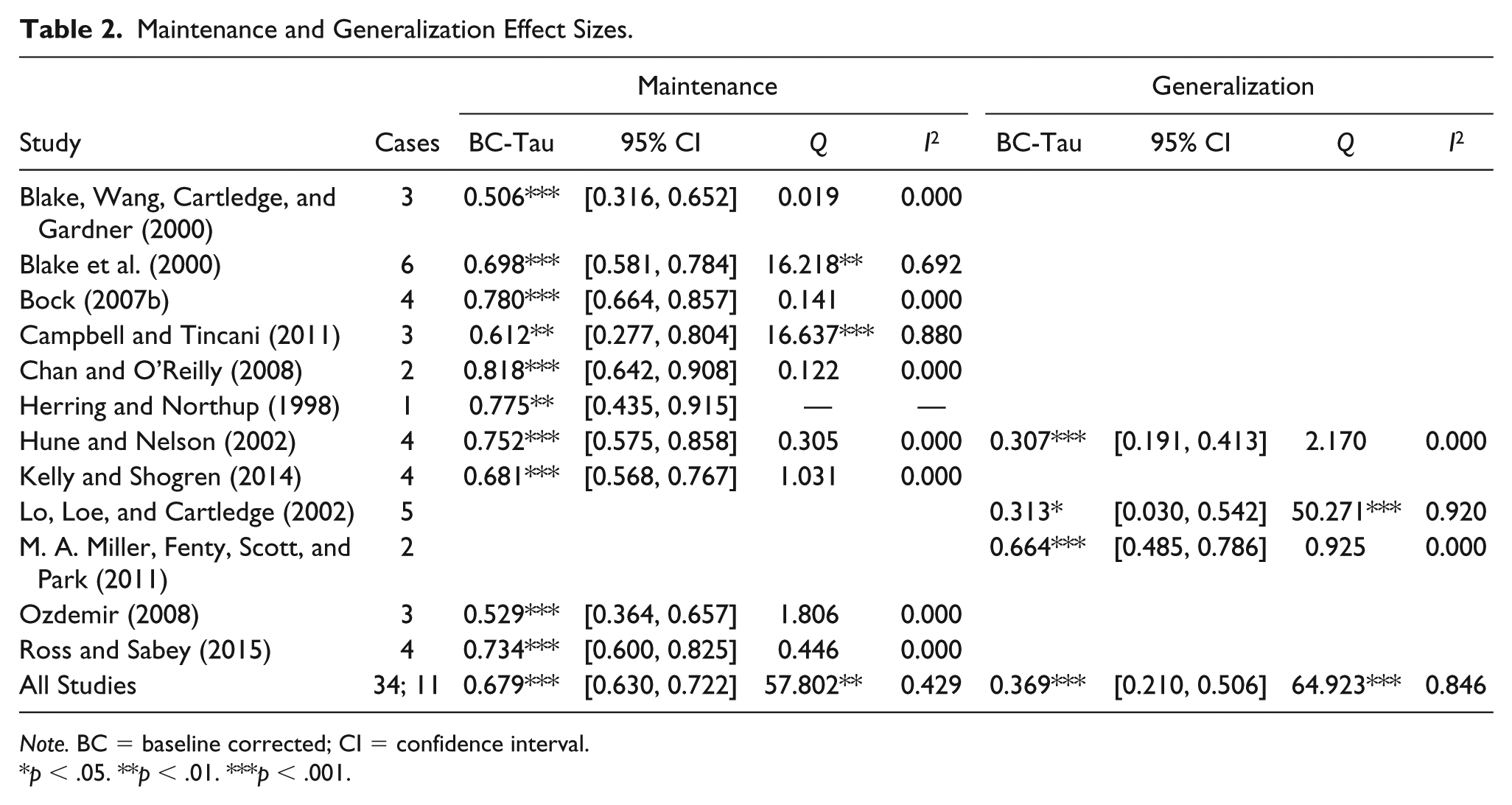
Note. BC = baseline corrected; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Moderator Analyses
Disability
Two disability categories were tested for between-group differences: students with or at risk of EBD (n = 46) and students with ASD (n = 32). There was no statistically significant difference between the two groups (Q*between = 0.418, p = .441). Disability type did not account for any proportion of variance among the participants’ effect sizes, R2 = .000 (see Table 3).
Random-Effects Moderator Analyses.
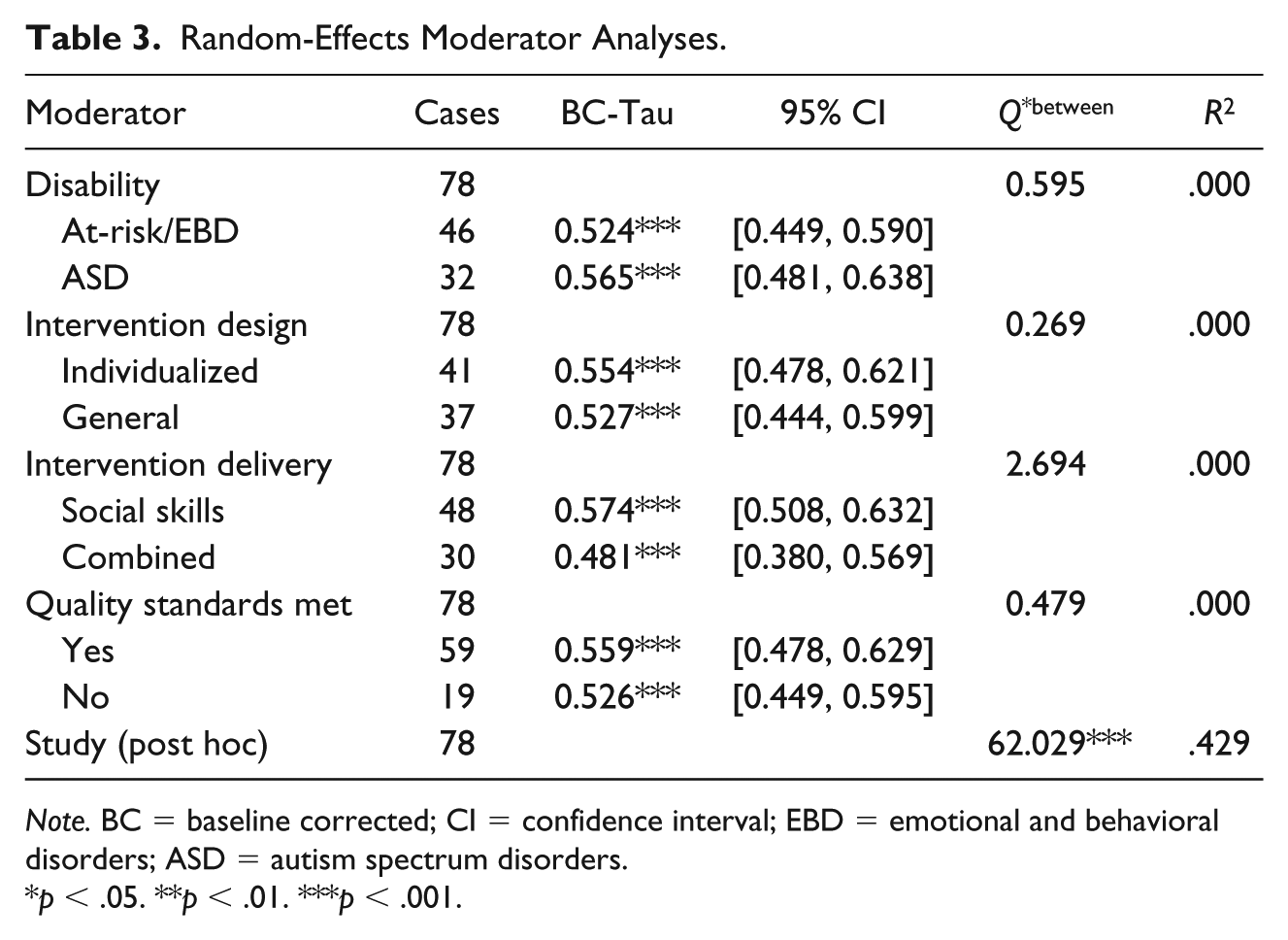
Note. BC = baseline corrected; CI = confidence interval; EBD = emotional and behavioral disorders; ASD = autism spectrum disorders.
p < .05. **p < .01. ***p < .001.
Intervention design
Two intervention design categories were tested for between-group differences: individualized (n = 41) and general (n = 37). There was no statistically significant difference between the two groups (Q*between = 0.177, p = .604). Intervention design did not account for any proportion of variance among the participants’ effect sizes, R2 = .000.
Intervention delivery
Two intervention delivery categories were tested for between-group differences: social skills (n = 48) and combined (n = 30). There was no statistically significant difference between the two groups (Q*between = 2.660, p = .101). Intervention delivery did not account for any proportion of variance among the participants’ effect sizes, R2 = .000.
Methodological quality
Two methodological quality categories were tested for between-group differences: participants from studies that met quality standards (n = 59) and participants from studies that did not meet quality design standards (n = 19). There was no statistically significant difference between the two groups (Q*between = 0.220, p = .489). Methodological quality did not account for any proportion of variance among the participants’ effect sizes, R2 = .000.
Between-study differences (post hoc)
After considering the poor predictive power of the four planned moderator analyses, we decided to examine the effect of study membership on participant effect size (i.e., how much variation in effect size is accounted for by characteristics of the studies themselves). It was hypothesized that between-study differences may be more meaningful than the similarities shared by participants in the same moderator groups. Indeed, there were statistically significant differences between study mean effect sizes (Q*between = 68.410, p < .001). Study membership accounted for a considerable amount of variance among participants’ effect sizes, R2 = .472.
Discussion
This study focused on examining the social skills intervention literature for students with or at risk of EBD, and students identified with ASD. This work extended previous research on SSIs from Mathur et al. (1998) and the quality review by Hutchins et al. (2016). This study addressed three main questions. First, the primary question focused on examining the overall effect of SSIs for students with or at risk of EBD and ASD. This review found a moderate overall effect across the SSIs. This finding is consistent with prior meta-analytic reviews of social skills intervention literature (e.g., Cook et al., 2008; Gresham, 2015). The effect size ranges reported in this current review ranged from relatively weak (e.g., Hansen & Lignugaris-Kraft, 2005) to moderately strong (e.g., Presley & Hughes, 2000). As illustrated in Table 1, when evaluating the social skills intervention evidence base, careful attention should be given to the specific intervention being studied.
The second question focused on the effects of SSIs on the maintenance and generalization of social skills. The finding that few social skills intervention studies collected maintenance and generalization data are consistent with previous reviews of social skills training including students with or at risk of EBD (Maag, 2006). For those studies that included maintenance and generalization data, the weighted mean effect sizes were 0.68 and 0.37. Similar to previous reports, greater effects were found for maintenance when compared with generalization of social skills. These findings suggest that some studies do have effects that maintain over time. However, generalization effects remain underexamined and problematic. Maintenance of social skills reported by Mathur et al. (1998) and Bellini et al. (2007) was greater than that reported in the current study. Generalization measures for students with ASD were found to be smaller in Bellini et al. (2007) and larger in P. Wang and Spillane (2009) than those obtained in the current study. Smaller generalization effects were reported in Mathur et al. (1998) than in this meta-analysis.
The third research question focused on the differential effects for SSIs. Previous meta-analyses have identified differential effects for SSIs based on theoretical approach, intervention type, group composition, intervention strategy, implementation format, disability, and school level. Variation effects were not found for the four moderator variables tested: disability, intervention design, intervention delivery, and methodological quality. A post hoc analysis was conducted because the moderator variables examined (e.g., disability, study quality) did not explain the observed variance, as indicated by their lack of statistical significance. As such, there may have been study-level differences that influenced the findings of this meta-analysis. In speculating reasons for the nonsignificance of the factors, it may be that factors not examined in this review (e.g., experimenter effects, type of behavior, how SSIs were delivered, how participants were sampled, and treatment fidelity) may account for the unexplained variance revealed by the post hoc analysis.
Limitations and Future Research
The following limitations and future research issues should be considered. First, Mathur et al. (1998) reported greater effects for students who were at risk of EBD than students with ASD or who were identified as delinquents. The current meta-analysis did not separate students formally identified with EBD from more “garden variety” students at-behavioral risk. Often times, there was not sufficient information to disaggregate the characteristics of the participants either (e.g., externalizing vs. internalizing). Those with formal diagnostic identifications may exhibit more problematic behavior. As the quality of reporting standards improves in the field, additional research should be conducted to disaggregate the participant characteristics of students included in SSIs. Second, differences in the effects of SSIs based on skill deficits versus performance deficits were not assessed. In part, because the information needed for this determination is not reported in the studies reviewed. Future research should examine the differential effects of social skills interventions on skill deficits or performance deficits for students with or at risk of EBD and ASD in future studies. Third, social skills and the construct of social competence encompass a wide range of skills and behaviors both in and out of school. Future research is needed to examine transfer (generalization) effects outside of school or classroom-based behaviors. Finally, participant outcomes (e.g., type of behavior such as aggression, initiating social interactions) and treatment fidelity should be examined as potential moderators in future meta-analyses. Examination of these moderators may help additional information on aspects of SSIs that are effective for children and youth with EBD and ASD.
Gresham (1998) posed the question of whether the field should “raze, remodel, or rebuild” the social skills literature. Moreover, Gresham (2015) recently noted that “about 65% of students with EBD will improve when given social skills interventions” (p. 100). Noting that much progress has been made in the research literature on SSIs, Gresham indicated that the level of improvement reported from the meta-analytic literature indicates that SSIs are not as robust as one would expect. This range of effects found in this meta-analysis is similar to previous reviews found in the social skills literature. There is clearly a range of responsiveness to SSIs. Those studies that report maintenance and generalization confirm the modest effects of transfer of social skills to other conditions. From an idiographic perspective, more attention should be given specifically to those studies that have yielded a strong response to intervention. The unique characteristics of the interventions in these studies should be attended to for the purposes of replication and implementation in applied settings. In moving forward, our hope is this current meta-analysis will assist researchers in “remodeling” the social skills intervention literature.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.