
Abstract
Research has documented a number of acute and chronic stressors unique to the fire service. Due to the rise in mental health concerns in firefighters, there has been increased awareness of the negative effects of unmanaged stress. The present study employed a behavioral-analytic model to construct a brief screening measure of stress for this population: the Firefighter Assessment of Stress Test (FAST). Psychometric properties of the FAST were evaluated using data from active-duty firefighters throughout the United States. Results indicated the FAST has good internal reliability (α = 0.89), as well as good convergent and discriminant validity. Also, the factor structure of the FAST revealed three significant subscales reflective of stress associated with responding to calls, administrative difficulties, and being overworked. Scoring and interpretation guidelines were established to suggest when further assessment is warranted. The FAST offers a brief and valid method of self-assessment of current stress levels in firefighters. Information obtained from the FAST (i.e., overall stress level and domains) has the potential to facilitate more immediate identification and recognition of stress in firefighters than what has been possible to date. Moreover, heightened awareness of stress and its effects will hopefully culminate in expanded efforts directed toward stress reduction and intervention for firefighters and their families.
Firefighters respond to a variety of physically and psychologically challenging situations (Mitani et al., 2006; Norwood & Rascati, 2012). These high stress situations include: fire suppression, rapid intervention of emergency medical care, directing and planning rescue efforts, and body recovery (Del Ben et al., 2006). Due to improved fire prevention methods, departments have increasingly taken on new responsibilities, such as medical aid calls, vehicle extrications, and incidents involving hazardous materials. The frequency and initial ambiguity of these calls create a stressful environment that has been shown to take a mental and physical toll (Kales et al., 2007; Meyer et al., 2012). Indeed, over the past two decades, researchers in the fields of physical, occupational, and mental health have documented this population’s increased risk for negative stress-related sequelae (e.g., injury, disease, burnout, and suicide; Guidotti, 1992; Paiva et al., 2016; Smith et al., 2018; Stanley et al., 2018). Further, there are a number of acute and chronic occupational stressors firefighters encounter. Acute stressors include irregular physical exertion, toxin exposure, excessive heat, and dehydration (Jahnke et al., 2012; Landrigan et al., 2004). Chronic stressors include shift work activity, irregular sleep cycles, financial strain, and exposure to critical incidents (Barger et al., 2015; Beaton & Murphy, 1993; Beaton et al., 1998).
For first responders, occupational stress is inherent in their job; however, the long-term effects of unmanaged stress can have detrimental effects on their wellbeing (Pignataro, 2013). Chronic stress can contribute to a deterioration of overall physical health with an increased risk of high blood pressure (Bautista et al., 2019; Lagraauw et al., 2015), headaches (Martin, 2016), gastrointestinal problems (Kolacz & Porges, 2018; Sexton et al., 2017), muscle tension (Wieckiewicz et al., 2017), sleep disturbances (Straud et al., 2018; Wolkow et al., 2015), weight fluctuation (Vicennati et al., 2009), metabolic syndromes (Garbarino & Magnavita, 2015), weakened immune system (Glaser & Kiecolt-Glaser, 2005), and cardiac disease (Brotman et al., 2007; Kivimäki & Kawachi, 2015).
Research has linked stress to the three leading physical causes of death in the general population: heart disease, stroke, and cancer (Cohen et al., 2007; Heron, 2016). Two of these, heart disease and cancer, are prevalent causes of mortality in firefighters (Jalilian et al., 2019; LeMasters et al., 2006). In fact, approximately one-half of all firefighter fatalities are the result of a cardiac condition (Sen et al., 2016). Additionally, stress has serious implications for firefighter safety practices and behavior. Specifically, studies have demonstrated an association between stress and the occurrence and frequency of occupational injuries (Kim et al., 2016; Smith et al., 2018; Tomei et al., 2015).
Extant research has demonstrated the link between stress and mental health problems such as depression, posttraumatic stress disorder (PTSD), substance use and suicide in firefighters (Komarovskaya et al., 2014; Smith et al., 2018; Straud et al., 2018; Walker et al., 2016). For example, Haddock et al. (2012) found that nearly 50% of career and volunteer firefighters reported binge drinking in a 1-month period. Also, investigations in this area show that firefighters who report greater stress demonstrate a higher level of PTSD symptomatology (Lee et al., 2014; Walker et al., 2016), with 16% to 24% of them experiencing PTSD during their career (Norwood & Rascati, 2012). Moreover, suicide risk has been found to be significant in this population with 46.8% of firefighters reporting suicidal ideation and 15.5% indicating at least one suicide attempt during their career (Antonellis & Thompson, 2012; Henderson et al., 2016; Stanley et al., 2015). Further, work-related stress in firefighters is associated with burnout, job dissatisfaction, firefighter safety outcomes, increased absenteeism, and heightened turnover rate (Mitani et al., 2006; Smith et al., 2018).
Despite the burgeoning evidence of the negative impact of stress in firefighters, few extant measures assess this problem. Beaton and Murphy (1993) developed the Sources of Occupational Stress Scale (SOOS), a 57-item measure examining sources of occupational stress in firefighter/EMTs and firefighter/paramedics. Items were included based on a review of the literature and modified after consultations with firefighter and paramedic organizations. Items were rated based on the degree to which they were “bothersome” on a Visual Analogue Scale (0 = lightly bothered to 100 = extremely bothered). Fourteen distinct subscales of occupational stress were identified.
Kimbrel et al. (2011) used content analysis to explore the 14 factors identified by Beaton and Murphy (1993) resulting in the development of a 14-item unidimensional measure of occupational stress (SOOS-14). While these instruments represent a step in the right direction, there are limitations. First, the items for the SOOS and SOOS-14 were developed over two decades ago. Given the job changes in the fire service over this period (e.g., different types of call-outs, advances in technology, and policy changes; Sheridan, 2019), assessments using current, updated stressful situations may be warranted. Second, the SOOS was composed of 14 factors of occupational stress, while the SOOS-14 was unidimenstional in nature. This wide range of dimensionality may limit the clinical utility of either measure. For example, calculating 14 subscale scores could be cumbersome and time-consuming for direct use by firefighters. Additionally, an overall occupational stress construct does not disentangle the primary facets of occupational stress impacting firefighters the most. Beyond these instruments, measures of stress specifically for use with firefighters are not available.
The purpose of the present study was to address this void by designing and empirically validating a stress screening measure tool for firefighters. The Firefighter Assessment of Stress Test (FAST) was constructed to detect and quantify stress in fire rescue personnel. Goals of the FAST were to: (1) identify unique stressors in the fire service, (2) provide a valid screening tool for the self-assessment of stress, and (3) develop an interpretive guide that provides information regarding whether further evaluation and possible intervention are warranted. It was expected that development of a short, easily administered stress survey would be a useful evaluation tool for the early detection of stress and related difficulties in fire rescue personnel.
Development of the FAST
The FAST was developed using the Behavioral-Analytic Model of test construction and additional widely accepted approaches to validating psychological instruments (American Educational Research Association et al., 1999; Freedman et al., 1978; Furr, 2018; Van Hasselt et al., 1985, 2008). This model of test construction utilizes the specific target population in the instrument formulation process and is based on distinct behavioral and environmental interactions (e.g., a stress reaction in response to a challenging/difficult situation; Goldfried & D’Zurilla, 1969; Van Hasselt et al., 2003). The Behavioral-Analytic Model consists of five major steps: (1) Situational Analysis, (2) Item Development, (3) Response Enumeration, (4) Response Evaluation, and (5) Instrument Construction. Descriptions of these steps and procedures employed in the construction of the FAST are described below.
Situational Analysis
In this initial phase, 50 firefighters from a large, urban local department were asked to identify real-world situations firefighters find stressful. Participants were given potential categories in which firefighters may experience an increase in stress levels: (1) Responding to Calls, (2) Administration, (3) Personal Life, (4) Peers, and (5) Health (Beaton, & Murphy, 1993; Shreffler et al., 2011). Each participant in the situational analysis phase was asked to formulate a minimum of five situations they find stressful based on their occupational experience. Firefighters were not restricted to these categories and were encouraged to formulate scenarios outside these five areas. A total of 200 responses was collected and 32 subthemes were classified.
Item Development
This step involved identifying duplicate scenarios, consolidating scenarios, and removing extraneous scenarios from the 200 responses to create 50 real-world stressful situations for firefighters. These scenarios were then formed into written items using clear and concise language. Some examples of items are: “Dispatch informs you of a call involving a man with chest pains, but when you arrive on scene you find a female with several gunshot wounds”; “You are dispatched to an unknown pediatric trauma”; “You are concerned that your co-worker will make a wrong decision during an emergency call.”
Response Enumeration
To ensure the items generated from the previous step were both commonly endorsed and included a range of stress severity (i.e., mildly stressful to extremely stressful), a second group of firefighters empirically evaluated the items. The first phase of Response Enumeration included 100 firefighters from a local department rating each of the 50 scenarios on two scales. One rating scale evaluated the likelihood that a firefighter respondent would encounter the situation depicted in the scenario. The second scale evaluated the difficulty/level of stress intensity of each situation would personally be for each firefighter. Both of these scales utilized a 4-point Likert scale, ranging from 1 = Not at all difficult/likely to 4 = Extremely difficult/likely. Participating firefighters also had the opportunity to provide additional written feedback on the items. A Content Validity Ratio (CVR; Lawshe, 1975) was calculated to determine the level of agreement among the firefighters regarding the “Likelihood” and “Difficulty” of each item’s scenario occurring. The CVR is a direct linear transformation of firefighter’ ratings of importance, with higher CVR’s indicating a greater agreement that an item’s content is valid. A total of 25 items that met the CVR cut-off of 0.70 were retained.
Cognitive interviews
As a second phase of Response Enumeration, two waves of Cognitive Interviews (CIs) were conducted to ensure items were clearly understood with the intended interpretation by the potential respondents (i.e., firefighters). A CI is a verbal probing technique that investigates the process through which the participant understood the questions and how they arrived at their choice for each specific response option. It provides information regarding the match between the psychological processes the participants actually used versus the process the researcher expected them to use (Furr, 2018). If these processes are not consistent, scores may not be interpreted as intended. This method is considered one of the key facets to improve construct validity when developing a new instrument (Furr, 2018). Ten firefighters were recruited for each wave of CIs, independent of previous participants. Research Assistants followed a semi-structured interview guide, consisting of a series of open-ended questions (e.g., “Was there anything confusing about the item?”; “What do you think this question is asking?”) to elicit the firefighters’ comprehension and/or interpretation of each item, as well as their feedback in their response option rating for “Likelihood” and “Difficulty.” Raters were trained by doctoral level Clinical Psychologists with expertise in psychometrics to conduct CIs via the use of role-plays. Researchers were not permitted to conduct CIs until competency was demonstrated in understanding the goals of a CI as well as consistency in conducting the interviews. After reviewing firefighters’ feedback from the first wave of CIs, modifications to the items were made based on a consensus from the research team. For example, the wording of a question might have changed to evoke a different timeframe. A second wave of CIs was then conducted to test changes made during the first wave. Participating firefighters were provided a $30 gift card for participation.
Response Evaluation
The purpose of this phase was to identify the best subset of scenarios for use as items in the FAST. To accomplish this goal, questionnaire items were modified one final time by evaluating the pattern of responses based on “Likelihood” and “Difficulty” feedback as well as qualitative information gathered during the CIs. Frequency distributions of the ratings of each scenario were calculated, and a minimum number of finalized items (25 items total) were retained, with a balance of mild, moderate, and severe stressful situations.
Instrument Construction
The final Firefighter Assessment of Stress Test (FAST) consisted of 25 situational items (see Table 1). Empirical evaluation of the FAST was completed using an Supplemental Online Survey Platform. Various fire departments, both volunteer and full time, across the nation were recruited to ensure a representative number of small, medium, and large departments from different regions of the country for validation purposes (Crocker & Algina, 2006). Firefighters who consented to participate completed a series of psychological measures (see Measures section) and the FAST. Researchers then validated the FAST using comprehensive psychometric analyses of all retained items as well as optimal cut-off scores to differentiate levels of firefighter stress.
Firefighter Assessment of Stress Test Descriptives (N = 134).
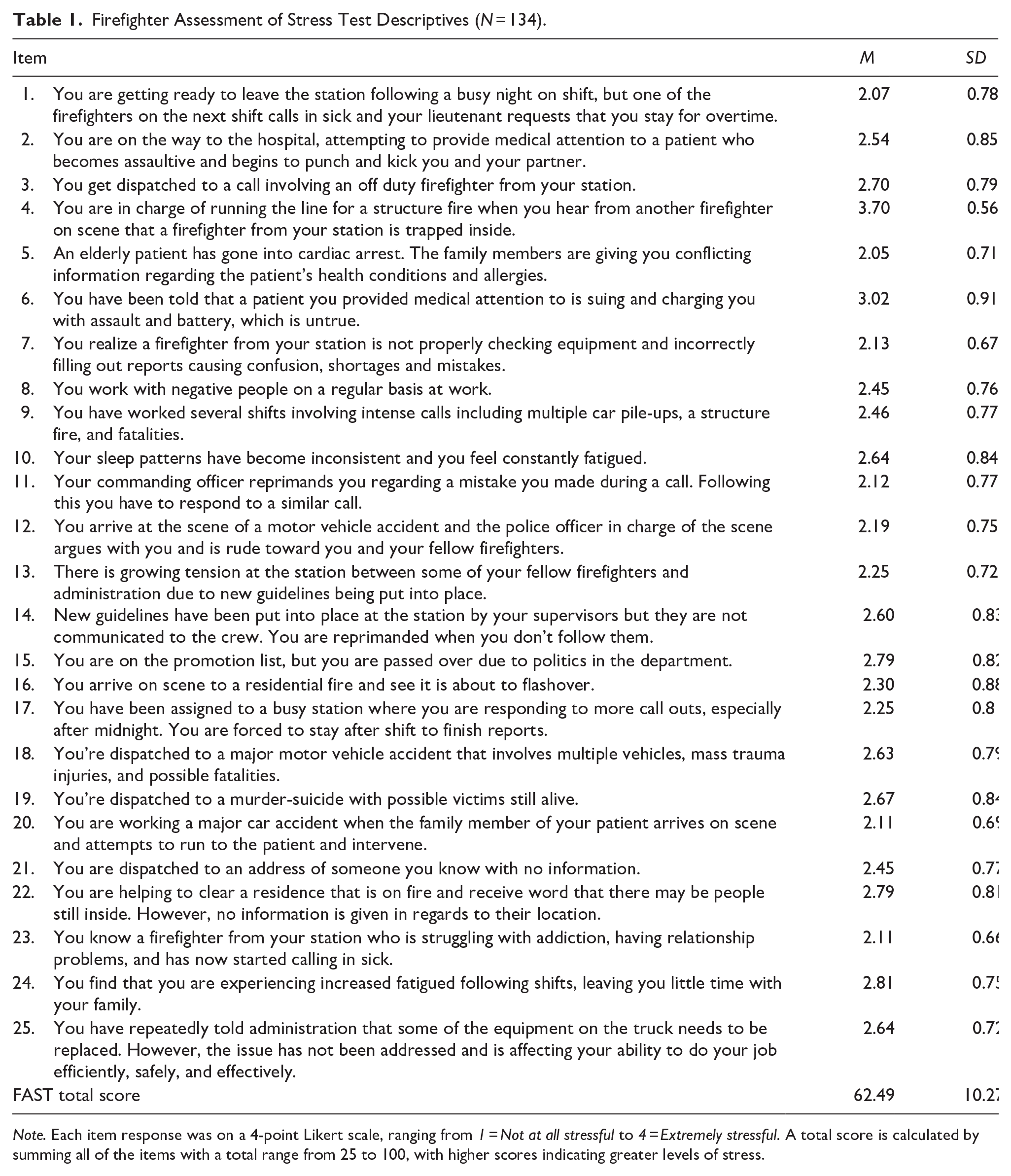
Note. Each item response was on a 4-point Likert scale, ranging from 1 = Not at all stressful to 4 = Extremely stressful. A total score is calculated by summing all of the items with a total range from 25 to 100, with higher scores indicating greater levels of stress.
Validation of the FAST
Participants
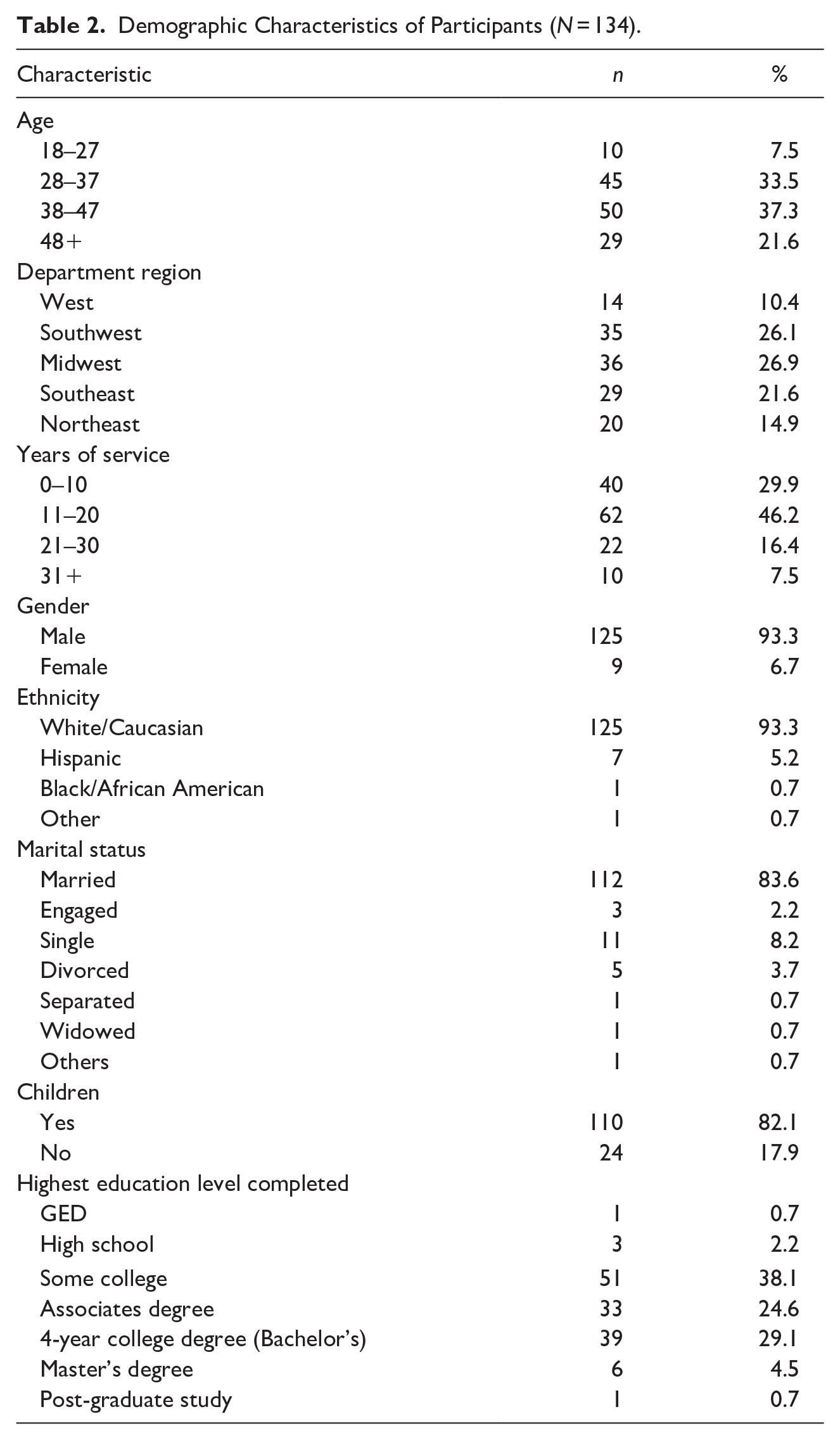
Participants included 134 adult career firefighters throughout the U.S. (see Table 2 for Demographic Characteristics of Participants). The study was inclusive of all active-duty firefighter personnel and no exclusionary criteria were applied. The majority of participants were between 33 to 37 years of age (21.6%) and 38 to 42 years of age (21.6%), followed by 43 to 47 years of age (15.7%), and 48 to 52 years of age (13.4%). Almost half (46.2%) of the sample reported having served as a firefighter for 11 to 20 years. Although the majority of the sample was male (93.3%) and Caucasian (93.3%), this demographic breakdown is consistent with national statistics (Evarts & Stein, 2019). A majority of firefighters indicated they were married (83.6%) and had children (82.1%). Respondents reported completing some college (38.1%), obtaining an Associate’s degree (24.6%), or earning a Bachelor’s degree (29.1%).
Demographic Characteristics of Participants (N = 134).
Procedures
A total of 115 fire departments were initially contacted via telephone and/or email to recruit potential participants. Contacts were given an explanation of the study and its procedures, informed that participation is voluntary, compensation would be provided, and the Supplemental Online Survey Link with instructions for completion. Of the 115, 14 departments agreed to distribute the Supplemental Online Survey to its members. Once firefighters accessed the survey, they were provided with a description of the survey and the choice to review the informed consent form, which delineates all aspects of the study. Those who did not wish to participate had the option to indicate (by clicking ‘No’) that they did not wish to participate. Participants who indicated that they were interested in participating (by clicking ‘Yes’) were directed to complete a battery of demographic and mental health questionnaires. Participants were provided the option to receive compensation in the form of a $20 Amazon gift card by entering their email following completion of the Supplemental Online Survey. In order to maintain participants’ anonymity, all data were de-identified. This study was approved by the Institutional Review Board (IRB) of Nova Southeastern University.
Measures
Demographic questionnaire
Participants reported on sociodemographic characteristics (e.g., age, race, gender, and martial status), and fire department service (e.g., region, years of service).
Perceived Stress Scale
The Perceived Stress Scale (PSS) is a 10-item measure, rated on a 5-point Likert scale (0 = Never to 4 = Very Often), developed to evaluate the degree to which individuals view their life as stressful during the past month (Cohen & Williamson, 1988). The questions are general in nature and relatively free of content targeted toward any specific groups (e.g., “In the last month, how often have you found that you could not cope with all the things that you had to do?”). Cohen and Williamson (1988) reported that the PSS-10 exhibited good reliability (α = 0.78). Mitchel et al. (2008) also found PSS-10 scores to exhibit good convergent validity and reported some evidence of concurrent validity. A total score is calculated by summing all item responses (range 0–40), with higher scores reflecting a greater level of stress. In the current sample, the PSS demonstrated good internal consistency reliability (α = 0.89).
The PTSD Checklist-Civilian
The PTSD Checklist-Civilian (PCL-C) is a 17-item self-report measure designed to assess PTSD severity based closely on DSM-IV criteria (Weathers et al., 1993). Respondents rate each item from 1 (not at all) to 5 (extremely) to indicate the degree to which they have been impacted by that particular symptom over the past month (e.g., “Repeated, disturbing dreams of a stressful experience from the past?”). The PCL-C is applied to any traumatic event the respondent might have experienced. Estimates of internal consistency have been found to range from 0.94 (Blanchard et al., 1996) to 0.97 (Weathers et. al., 1993). Evidence for convergent validity was found in the high correlations (r = 0.75) between PCL-C total scores and scores obtained on a well-established measure of PTSD (Clinician Administered PTSD Scale; Blanchard et al., 1996). The PCL-C demonstrated good internal consistency reliability within the sample (α = 0.93).
The Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II) is a self-report instrument that measures the presence and severity of depressive symptoms (Beck et al., 1996). It was designed to match the criteria for depressive disorder established in the DSM-IV. It contains 21 items that cover specific domains and presents four statements labeled 0, 1, 2, or 3 which the respondent has to circle based on how he/she has been feeling for the last two weeks. Osman et al. (1997) reported that reliability estimates for the total BDI-II score resulted in an alpha coefficient of 0.90, similar to the high alpha index reported in the BDI-II manual (Beck et al., 1996). Osman et al. (1997) also found evidence of convergent and construct validity, and that BDI and factor scales were strongly associated with general and specific depressive symptoms. Cronbach’s alpha was 0.89 in the current study.
The Drug Abuse Screening Test-20
The Drug Abuse Screening Test-20 (DAST-20) is a 20-item self-report measure designed to screen for drug abuse and associated problems (Skinner, 1982). It yields a total score ranging from 0 to 20 by summing all items that are endorsed in the direction of increased drug problems. Higher scores indicate greater problems or consequences relating to drug use. Yudko et al. (2007) found satisfactory estimates of internal consistency, ranging from α = 0.74 to 0.95 across various studies. For the present study, DAST-20 scores demonstrated good internal consistency reliability (α = 0.78).
Marlowe-Crowne Social Desirability Scale
The Marlowe-Crowne Social Desirability Scale (MCSDS) is a 33-item measure examining the tendency to present oneself in a favorable light (i.e., “defensiveness”; Crowne & Marlowe, 1960). This measure was included because it has been found that first responder populations often under report difficulties (Coman & Evans, 1991; Sewell, 1981) and, therefore, are susceptible to a social desirability bias when answering self-report measures in research. Examples of items on this measure are “I have never intensely disliked someone” and “I never make a long trip without checking the safety of my car.” Higher scores reflect a tendency toward greater social desirability. Crowne and Marlowe (1960) reported a Kuder–Richardson internal consistency coefficient of 0.88 on 39 undergraduates, and a test–retest reliability of 0.89 for 31 of these students who completed the questionnaire one month later. Validation data for 39 undergraduates include correlations of 0.40 and 0.54 with the Minnesota Multiphasic Personality Inventory (MMPI) Correction and Lie scales, respectively (Crowne & Marlowe, 1960). Cronbach’s alpha for the current study was 0.81.
Data Analytic Plan
Descriptive statistics were used to describe the sample’s demographic characteristics and firefighter-specific characteristics. A comprehensive psychometric analysis of all retained items was conducted to establish reliability and validity of the FAST. Internal consistency of the FAST was examined by calculating Cronbach’s α. Construct validity (convergent and discriminant validity) was determined by conducting Pearson product-moment correlations to establish the relative strength of the associations of total scores from the FAST with the PSS, PCL-C, BDI-II, and DAST-20. An Exploratory Factor Analysis (EFA) was carried out to ascertain the internal structure (i.e., dimensionality) of the FAST. All statistical analyses were conducted using SPSS version 26.
Results
Internal Structure
To determine the factorial structure (i.e., number of factors) of the FAST, an exploratory factor analysis (EFA) using an oblique rotation (promax) was performed. A parallel analysis using EFA methodology (i.e., Monte Carlo simulation) was employed to determine the number of statistically significant factors to retain (see Figure 1; Hayton et al., 2004). Results revealed three significant factors accounting for 47.02% of the instrument’s variance. The 14-items that comprise the first factor reflect stress associated with responding to calls (λ = 7.28), accounting for 29.13% of the shared variance. The seven items that comprise the second factor reflect stress associated with administrative duties and departmental politics (λ = 2.76), accounting for 11.04% of the shared variance. Finally, the four items that comprise the third factor reflect stress relating to being over-worked (λ = 1.71), accounting for 6.86% of the shared variance (see Table 3 for specific factor loadings). As expected, there was a correlation between the factors (r12 = 0.47; r13 = 0.38; r23 = 0.50), suggesting presence of a second order factor of Overall Firefighter Stress. These findings suggest there are 3 subscale scores (i.e., stress attributable to responding to calls, administrative stress, and stress attributable to being over-worked) and a full scale score that can be measured by the FAST.
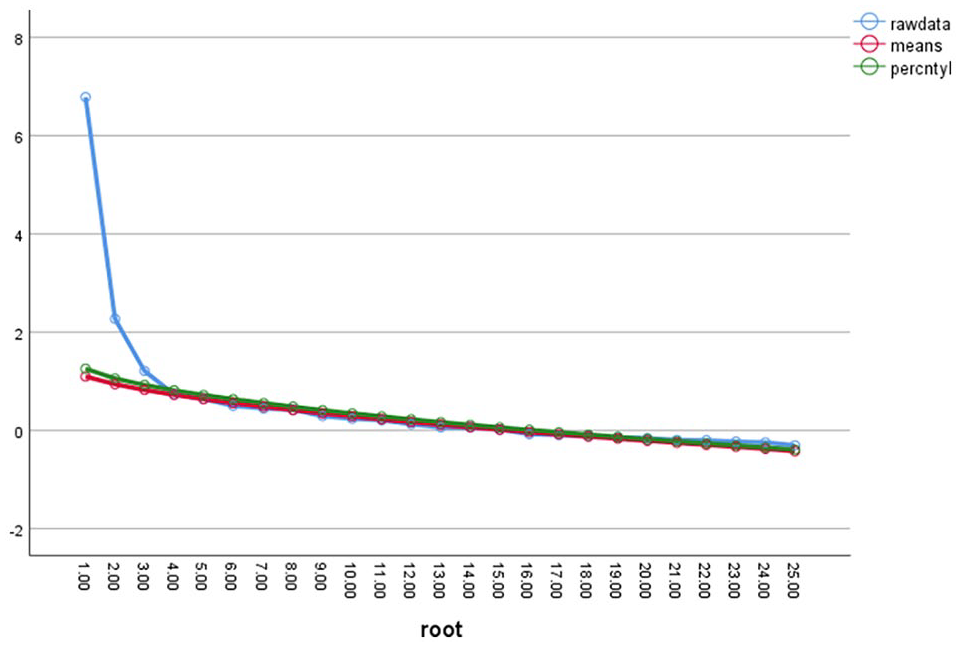
Sequence plot of parallel analysis.
Factor Loadings for Exploratory Analysis With Promax Rotation of FAST Items.
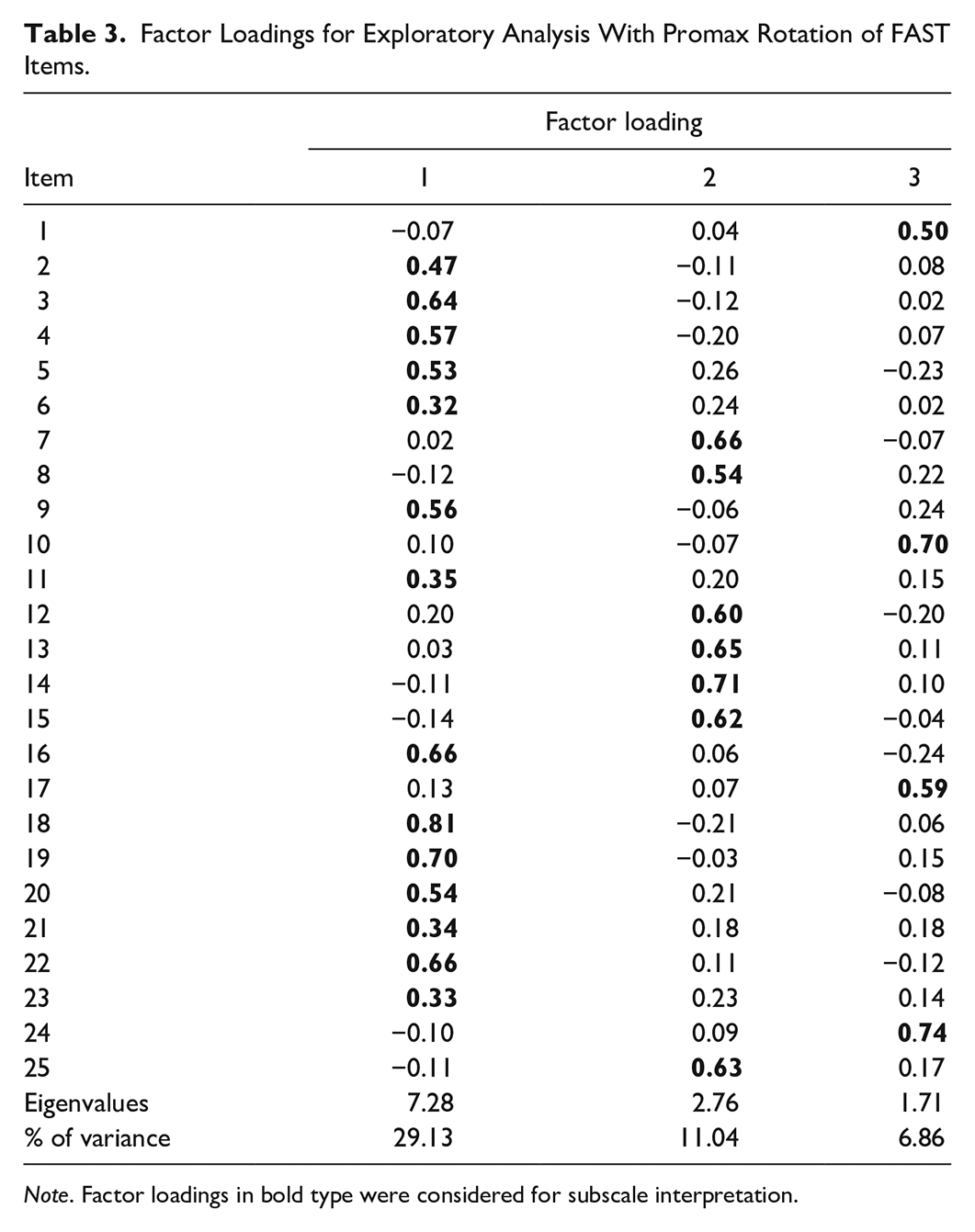
Note. Factor loadings in bold type were considered for subscale interpretation.
Reliability
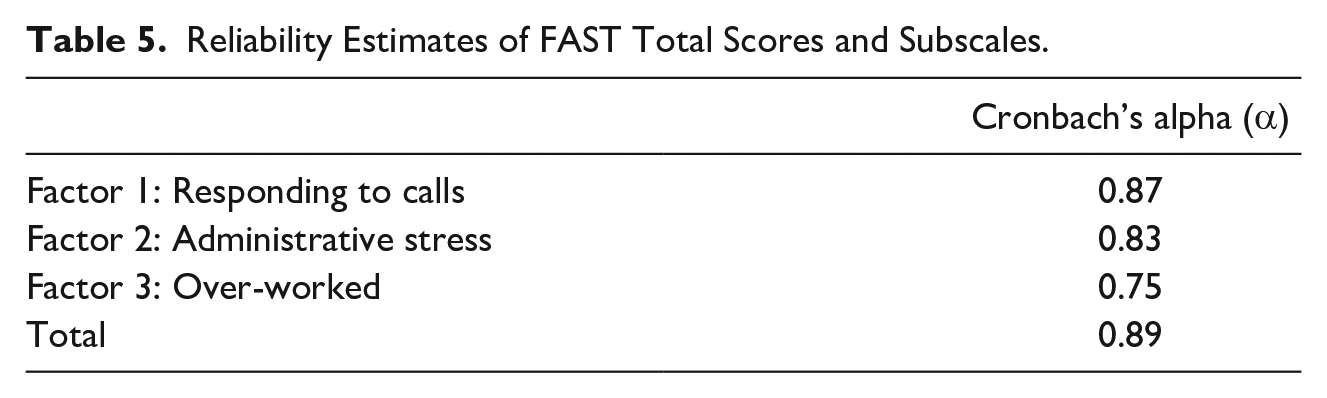
The internal consistency reliability of the FAST was α = 0.89, indicating good internal consistency reliability. All items meaningfully contributed to the reliability estimate. Each of the items was positively correlated with the Total Score, indicating each item had good discriminative power (see Table 4 for further details on inter-item correlation). Reliability for each of the identified subscales ranged from 0.75 to 0.87, all within an acceptable range (see Table 5 for reliability estimates of each subscale).
Inter-Item Correlations of FAST Items and Total Score.

Note. **Correlation significant at the p = .01. *Correlation significant at the p = .05.
Reliability Estimates of FAST Total Scores and Subscales.
Validity
To establish convergent and discriminant validity of the FAST, pearson correlations were conducted to assess the relationship between the total score of the FAST and the total score of previously validated measures. Table 6 provides the correlations between the FAST, PSS, PCL-C, BDI-II, DAST-20, and MCSDS. It was hypothesized that FAST total scores would be more strongly correlated with other measures of stress (i.e., PSS and PCL-C) than measures of depression (i.e., BDI-II), and would not be correlated with measures of problematic drug use (DAST-20). The total scores of the FAST were positively associated with the PSS (r = 0.42, p < .001), PCL-C (r = 0.40, p < .001), and BDI-II (r = 0.33, p < .001), which provides evidence of convergent validity. Additionally, the total score was not significantly correlated with the DAST-20 (r = −0.09, p = .28), providing evidence of discriminant validity. As expected, there was a weak, negative association between FAST total scores and MCSDS scores (r = −0.17, p = .044), which may indicate firefighters were more likely to report lower levels of stress if they scored higher on social desirability.
Correlation Matrix of FAST, BDI-II, PSS, DAST-20, and PCL-C.
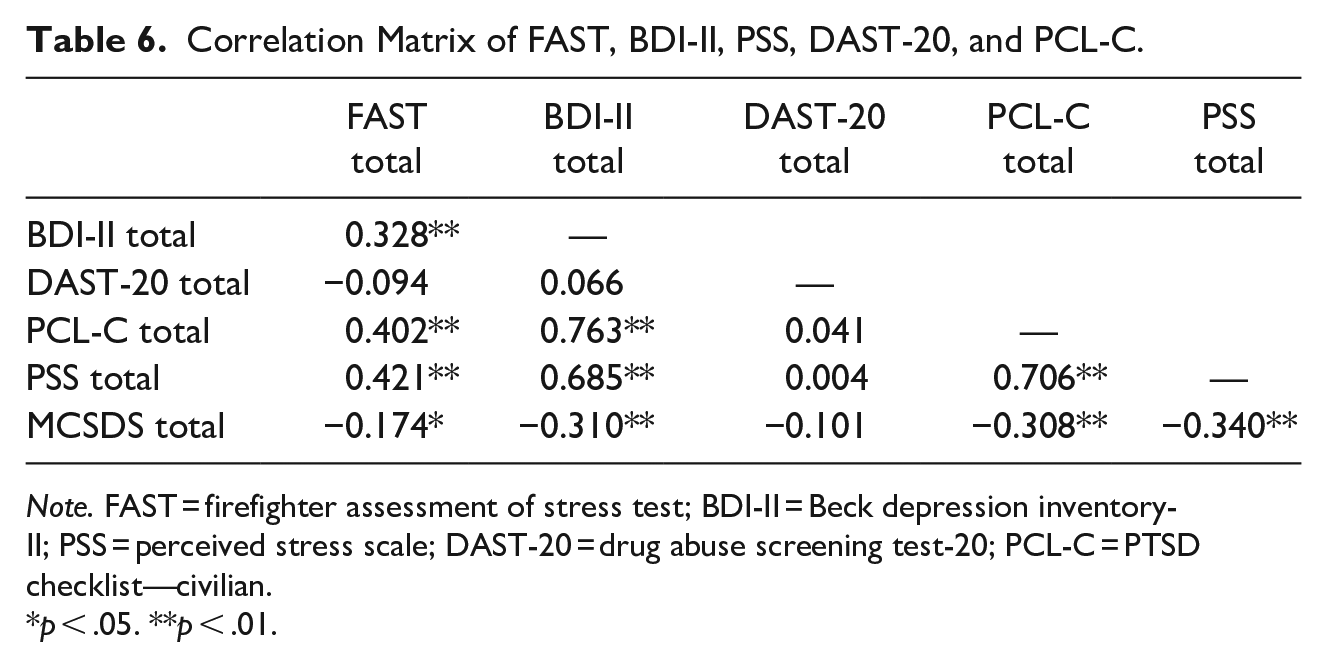
Note. FAST = firefighter assessment of stress test; BDI-II = Beck depression inventory-II; PSS = perceived stress scale; DAST-20 = drug abuse screening test-20; PCL-C = PTSD checklist—civilian.
p < .05. **p < .01.
Scoring and Interpretation Recommendations
Based on the psychometric evaluation, a score for each of the three subscales (i.e., stress attributable to responding to calls, administrative difficulties, and being over-worked) along with a total score should be calculated. Higher scores on the first subscale suggest an individual has higher levels of stress associated with responding to calls. Additionally, higher scores on second subscale would suggest that an individual has higher levels of stress related to administrative or departmental difficulties. Higher scores on the third would imply the individual is experiencing greater stress relating to being over-worked. Finally, a higher overall total score would indicate an increased level of firefighter stress (see Figure 2 for histograms of distribution of scores for each factor and total scores for our sample). The interpretive guide of total scores, provided in Table 7, was based on evaluating the distribution of mean scores relative to the response categories. For example, individuals with raw scores that correspond with an average rating of 2 (somewhat stressful) across the items were described as experiencing mild levels of stress. Subscale scores can provide additional information regarding the area in which the firefighter is experiencing the most stress. Of note, these are general guidelines not intended to be diagnostic in nature. Regardless of the score, firefighters are encouraged to seek mental health services when stress is a problem in their life. The interpretations provided are estimates of severity of stress intended to aid firefighters in understanding their current levels of stress.
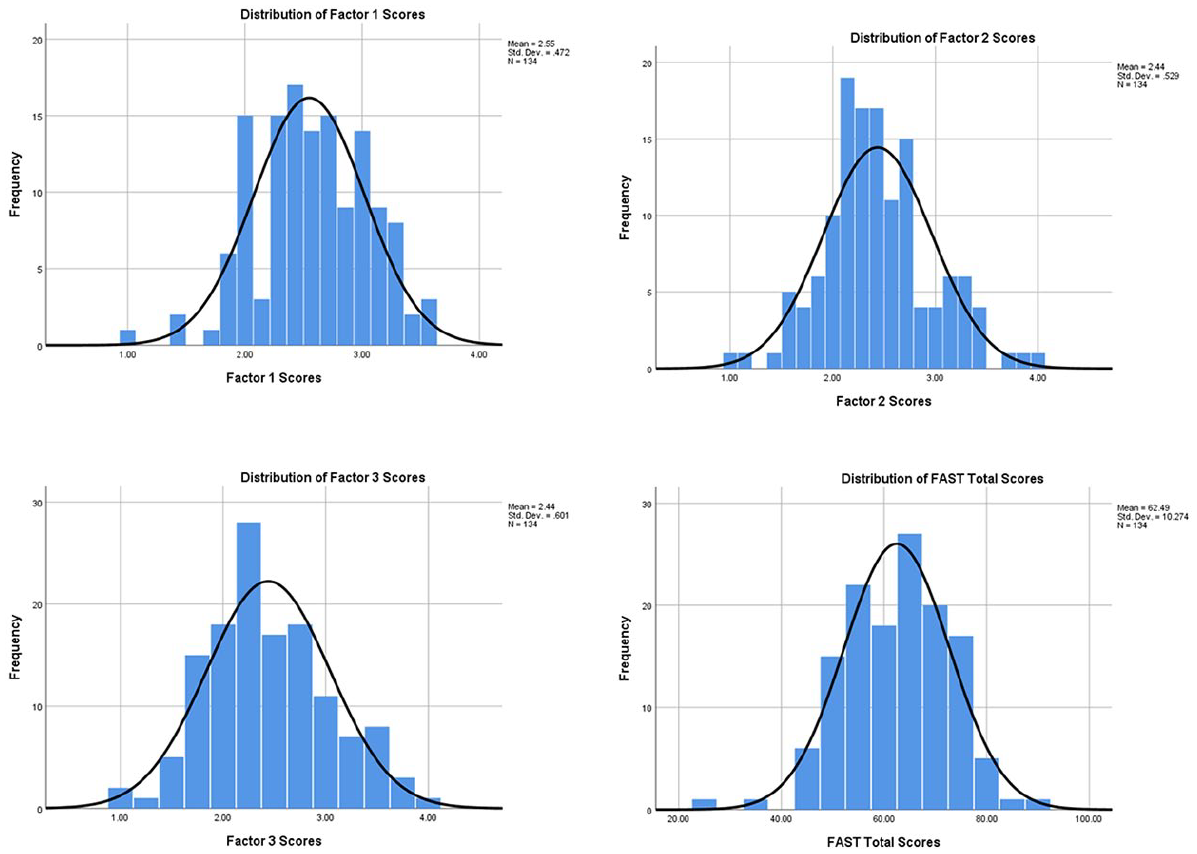
Distribution of average scores for factor 1, factor 2, and total scores. Factor 1 responses reflect stress associated with calls. Factor 2 represents stress associated with administrative issues. Total scores range from 25 to 100, with higher totals reflecting greater levels of stress.
Interpretive Guide and Scoring Recommendations of FAST.
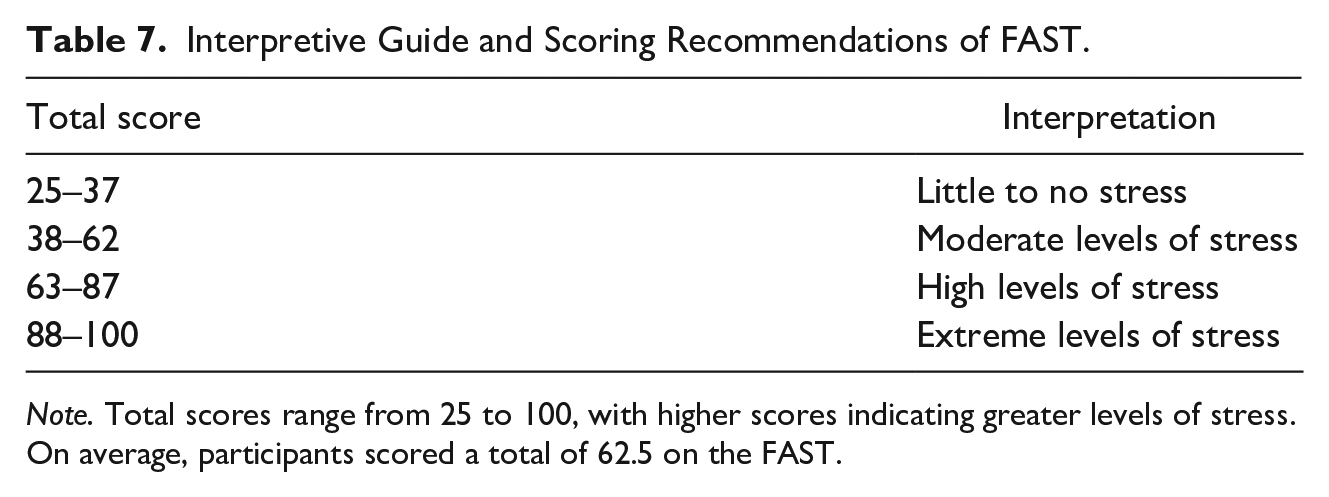
Note. Total scores range from 25 to 100, with higher scores indicating greater levels of stress. On average, participants scored a total of 62.5 on the FAST.
Discussion
The purpose of the present study was to develop and empirically validate a self-assessment instrument measuring stress in firefighters: the Firefighter Assessment of Stress Test (FAST). This was accomplished via a behavioral-analytic model of test construction. Using this approach, several steps were taken to ascertain stressful situations specifically relevant to the experiences of firefighters. Results indicated the FAST has good internal reliability, as well as good convergent and discriminant validity. Also, the factor structure of the FAST revealed three significant subscales reflective of stress associated with responding to calls, administrative difficulties, and being overworked. Scoring and interpretation guidelines were established to suggest when further assessment is warranted. The FAST offers a brief and valid method of self-assessment of current stress levels in firefighters.
Historically, mental health problems have been viewed as a sign of weakness, failure or personal defect due to the masculine role perpetuated in the fire service (Henderson et al., 2016). Additionally, firefighters report concerns regarding confidentiality and clinician understanding of fire culture, particularly when services are provided by the department, such as an Employee Assistance Program (EAP), as it is thought to be a potential threat to their career. Thus, the traditional approach has been to ignore these issues. With consideration of traditional stigma and barriers, the FAST was developed to be administered as a self-assessment screening tool, allowing firefighters to complete the measure independently. Scoring and interpretation guidelines were developed to facilitate the private evaluation of a firefighter’s current levels of stress. It is anticipated that this self-administration method may lead to increased utilization of such measures. Consequently, firefighters’ can autonomously detect and respond to high levels of stress, reducing the possibility of negative outcomes. The authors’ acknowledge continued work needs to be done to address the larger context of attitudinal change surrounding mental health and the development of the FAST is an initial step in this direction. Future research should examine the acceptance and utilization of the FAST to demonstrate the efficacy of self-administered assessments despite the cultural stigma.
There are several advantages to employing a systematic model of test construction that incorporates stressful situations identified by the relevant target group. By allowing the target population (i.e., firefighters) direct involvement in the process, content validity is increased, thus, improving the accuracy of the interpretations drawn from the results of this measure (Furr, 2018). In addition to providing data regarding the current levels of firefighter stress, the FAST identified the three above-mentioned subfactors of stress experienced by firefighters. Subscales point to which specific aspects of the job a firefighter finds particularly stressful. With this information, mental health providers can better identify prevention and intervention strategies to improve the firefighter’s coping abilities for such situations.
Several limitations of this investigation warrant mention. First, this study utilized self-report measures. Given the cultural stigma of mental health, it is possible participants may have under-reported the severity of their mental health problems. However, the researchers attempted to assess for effects of social desirability using the MCSDS. Further, our sample may not be entirely representative of the fire service. National data indicate that approximately 35% of all firefighters are career firefighters, while 65% are volunteers (Haynes & Stein, 2017; U.S. Fire Administration, 2020). A majority of departments contacted to participate were composed of career Firefighter Emergency Medical Technicians (EMT)/Paramedics. Thus, the current sample may not reflect experiences of volunteer firefighters. However, it should be noted that the firefighters in this study are fairly consistent demographically with national fire department statistics. Nationally, 50.7% of firefighters are between 30 and 49 years of age, and approximately 7% are female (Haynes & Stein, 2017). Second, there was no direct comparison between the FAST and previously developed measures of firefighter stress (i.e., SOOS-14), thus the incremental validity of the FAST is unknown. However, based on examination of construction methods and content of each measure, the FAST measures stress utilizing stressful scenarios, whereas the SOOS-14 examines stress level by how ‘bothersome’ various sources of stress have become over the past 10 shifts. Thus, each measure adds unique value in the assessment of firefighter stress. Third, the present study only included a single sample to evaluate psychometric properties of the FAST. Consequently, we were unable to conduct a confirmatory factor analysis to confirm the presence of a higher order factor, justifying the use of a total score. Nevertheless, the relatively strong correlations between the three factors provide evidence of a second-order factor representing Overall Firefighter Stress.
It is also worth mention that firefighters have the potential to experience extraordinary stressors outside of their unique, everyday occupational experiences. For example, as this paper is written, firefighters across the globe are responding to the coronavirus pandemic. As such, it is possible the situations firefighters may find stress levels have shifted. While the FAST does not directly assess stress relating to such situational stressors (e.g., natural disaster, mass shooting, global health crisis), it is expected that many of the items (e.g., “You are getting ready to leave the station following a busy night on shift, but one of the firefighters on the next shift calls in sick and your lieutenant requests that you stay for overtime”) would be impacted by situational elevations in stress, as they are indirectly related. Additionally, the goal of the FAST was to identify common stressors that are uniquely experienced by firefighters and provide a tool to aid in the assessment of stress. In order for the instrument to be universal and applicable for day-to-day experiences, such extraordinary events were not included.
Due to firefighters’ historic negative cultural stigma associated with seeking mental health services, it is imperative that firefighters become aware of, and proactive in, monitoring their stress levels as an initial step in preventing or reducing them. Assessment and screening tools validated within this unique population are needed in order to better identify stress and subsequent related disorders. The FAST is a practical tool that is easily accessible and relevant to the experiences of firefighters, fire service administrators, and clinicians, alike. Ideally, the FAST would be implemented as a prevention tool. Firefighters would complete the measure on a regular basis to assess their current stress level and monitor changes. This would allow them to be more informed regarding whether to seek appropriate services, if necessary. To further bolster the findings from this study, future research should examine the predictive validity of the FAST.
While the FAST is designed as a self-assessment tool, it may be used in other settings. For example, it has potential value in serving as a useful and valid device for clinicians working with firefighters to: (1) assess changes in stress over time and (2) determine factors contributing to their current symptom presentation. Further, with increased implementation of peer support programs, the FAST can provide team members with an instrument for assessing the severity of their peers’ current stress. The established cutoffs can serve as a guide for referral to services when this appears necessary. Information obtained from the FAST (i.e., overall stress level and domains) has the potential to facilitate more immediate identification and recognition of stress in firefighters than what has been possible to date. Given the burgeoning body of evidence showing that firefighters are at risk for stress-related disorders, such instruments are urgently needed. Moreover, heightened awareness of stress and its effects will hopefully culminate in expanded efforts directed toward stress reduction and intervention for firefighters and their families.
Supplemental Material
sj-pdf-1-bmo-10.1177_0145445520986137 – Supplemental material for A Behavioral-Analytic Model for Assessing Stress in Firefighters
Supplemental material, sj-pdf-1-bmo-10.1177_0145445520986137 for A Behavioral-Analytic Model for Assessing Stress in Firefighters by Bailee B. Schuhmann, Sarah N. Henderson, Ryan A. Black, Vincent B. Van Hasselt, Kristin Klimley Margres, Estefania V. Masias and Todd J. LeDuc in Behavior Modification
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nova Southeastern University President’s Faculty Research and Development Grant (Index No. 33549). The funding source had no involvement in study design, collection, analysis or interpretation of data, or preparation of this article for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.