
Abstract
Successful feeding intervention ultimately requires generalization and adoption of treatment into the home. Treatment models, however, differ regarding how and when caregivers are integrated into care delivery process. Some treatments involve a primary model of parent training with caregivers serving as co-therapist at the onset of intervention, while others involve a complimentary model where a therapist delivers the intervention and caregiver training occurs once the child’s behavior is stable. This review systematically evaluates the evidence-base regarding behavioral feeding intervention for children with autism spectrum disorder (ASD), with a specific focus on interventions involving parent training. Results provide further evidence regarding the potential benefits of behavioral intervention to improve feeding concerns in ASD, while also highlighting growing attention to documenting and/or evaluating parent training within the treatment literature. Important questions remain regarding factors guiding the use of a primary or complimentary model of parent training.
Children with autism spectrum disorder (ASD) exhibit impairments in social communication interactions and restricted, repetitive behaviors (American Psychiatric Association, 2013). In addition to these core features, children with ASD may experience a variety of other difficulties including externalizing behavior (e.g., aggression, self-injury, and tantrums; Dominick et al., 2007), sleep disturbance (Cortesi et al., 2010; Hoffman et al., 2006), toileting problems (Kroeger & Sorensen-Burnworth, 2009), and feeding difficulties (Ledford & Gast, 2006) that may require intervention. These behavioral co-morbidities complicate daily living, hold adverse health consequences, and lead families to seek treatment to remediate symptoms and improve overall quality of life. Prior reviews support treatments that involve a behavioral framework built on the principles of applied behavior analysis (ABA) to teach new skills, reinforce appropriate behaviors, and extinguish inappropriate or problematic behaviors (Betz & Fisher, 2011; Campbell, 2003).
Behavioral treatments target problems of social importance through live observation and systematic changes to the environment to drive change while also programing for implementation of the intervention in socially important settings (Baer et al., 1987). Caregivers are central in this process as agents of change; first, in identifying the problem of social importance and subsequently adopting and carrying out the intervention in socially important settings (e.g., the home and/or community). It is the caregiver, after all, who will be responsible for assuring treatment gains endure post-intervention. As such, training caregivers to accurately deliver intervention is critical to ensure successful generalization and maintenance of treatment gains post-intervention. With this in mind, caregiver involvement and training during behavioral interventions, in general, has been cited as highly variable and inconsistently reported within field of ASD (Bearss et al., 2015; Gerow et al., 2018).
The term parent training encompasses a wide array of applications in terms of involvement and format (Bearss et al., 2015). To provide clarity, Bearss et al. (2015) developed a taxonomy classifying the role of parents in parent training programs for children with ASD. According to this taxonomy, parent training programs are classified as either parent support or parent mediated. Parent support programs provide parents with information and knowledge about ASD that indirectly benefit the child (i.e., care coordination, psychoeducation). In contrast, parent mediated programs actively engage the parent to promote behavior change for the child and, thus, provide direct benefit to the child in terms of improved day-to-day functioning. Parent-mediated programs can be categorized as primary or complementary depending on who serves as the primary agent of change in the program. Specifically, in primary programs, caregivers facilitate the treatment from the outset of treatment whereas in complementary programs, a therapist initially conducts the treatment and subsequently involves caregiver when deemed clinically appropriate.
Previous reviews on treatment for feeding disorders in children with ASD have focused on summarizing effective behavioral treatment components, (e.g., shaping, fading, escape extinction, differential reinforcement) and documenting the benefits of intervention (e.g., Ledford & Gast, 2006; Ledford et al., 2018; Marshall et al., 2015; Sharp et al., 2010). In general, these reviews tend to show positive outcomes associated with behavioral intervention, particularly in terms of improving acceptance of new foods. A general consensus emerging from prior reviews, however, is the need for more research on the feasibility, social validity, and generalizability of treatment. For example, Ledford and Gast (2006) emphasized that results from empirical studies are jeopardized if treatment is not continued by parents, teachers, and other “indigenous implementors” (i.e., individuals who provide care or services to children and who will be responsible for implementing intervention beyond the clinic setting). Ledford et al. (2018) reported that researchers (versus indigenous implementors) most often delivered treatment in a clinic rather than the target setting (e.g., home, school). This line of research, however, provides little clarity regarding the extent and type of training caregivers receive during the intervention process.
The purpose of this review is to provide a description of studies published on behavioral intervention that: (a) focused on a feeding intervention, (b) targeted children with ASD, and (c) involved parent training. As our review will show, few studies have been published that meet these criteria, and so we conducted a detailed, descriptive analysis of participants, treatment setting, what was conducted, by whom, and with what outcomes. We then discuss what the needed next steps are for applied behavior analysts to consider in future programs involving parents.
Method
Search Strategy and Inclusion Criteria
Following the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement, this review involved a systematic search of APA PsycInfo, MEDLINE, and CINAHL through the EBSCOhost database search engine between 1968 and October 2021. The search focused on English language and peer-reviewed studies. The search parameters included key words regarding the patient population (e.g., “autism”), treatment (e.g., “intervention”) and feeding concern (e.g., “food selectivity”) inserted into the key word fields utilizing Boolean operators and truncation (Table 1). We also completed a reference search of the final pool of articles to identify additional studies for consideration.
Key Words Used in Database Search by Category.
For inclusion in this review, studies had to meet the following criteria: (a) the sample focused on a pediatric population (birth—18 years old), (b) the study involved a group of children (five or more) with ASD, (c) the treatment involved a behavioral intervention to improve the variety or volume of food consumed, and (d) parent training was conducted at some point in the treatment process. Inclusion criteria also focused on US-based treatments. The review excluded studies involving both children with and without ASD but not reporting outcomes specific to the ASD cohort. The review also excluded interventions specifically evaluating medication management in the treatment of the feeding concerns. The first and second authors independently searched the literature, reviewed and screened potential articles, and reached consensus on final pool of studies included in this review.
Data Extraction, Variables Coded, and Reliability
Data extraction involved a standardized database and coding process. Coders extracted data on the following five categories: (a) summary of study and sample characteristics, (b) treatment delivery and approach to intervention, (c) target of intervention and measurement approach, (d) description of interventionist, child involvement, and caregiver training, and (e) treatment outcomes and interpretation. For summary of study and sample characteristics, data extraction included the location of the study, delivery setting details, study design, inclusion criteria (if reported), sample size, child demographics, and ASD diagnostic criteria. Data extraction specific to the treatment delivery and approach to intervention focused on delivery format (i.e., group or individual), treatment implementation setting, treatment name, involvement of other disciplines, delivery frequency (e.g., daily, weekly), session/meal duration, length of treatment, and whether or not follow-up support was offered. Target of intervention and measurement approach focused on the stated target of feeding intervention and the measurement approach (e.g., caregiver satisfaction, Brief Autism Mealtime Behavior Inventory [BAMBI; Lukens & Linscheid, 2008], direct observation). For description of interventionist, child involvement, and caregiver training, the coding process documented the primary interventionist, child involvement in treatment process, and parent training methodology based on the Bearss et al. (2015) framework. For treatment outcomes and interpretation, coding collected data feasibility metrics, method of evaluating effectiveness (e.g., visual analysis of data; statistical significance), social validity analyses, and summary of the study results. In articles that included multiple participants or groups of participants, data extraction focused exclusively on data related to participants with ASD.
To assess agreement on the final articles identified in the database search, two authors independently conducted the same search in the APA PsycInfo, MEDLINE, and CINAHL databases as described above. Both searches generated the same number of articles (See Figure 1 for PRISMA flow diagram for search process). Interobserver agreement focused on extracted data from identified articles. The research team independently double-coded all data extracted during the review process. The double-entered data allowed for the calculation of percent agreement (i.e., item agreement/item agreement + item disagreement × 100). Coder agreement was 98% (range: 96%‒100%). To further ensure the accuracy, the team reached consensus on all areas of discrepancy highlighted during the inter-rater analysis.
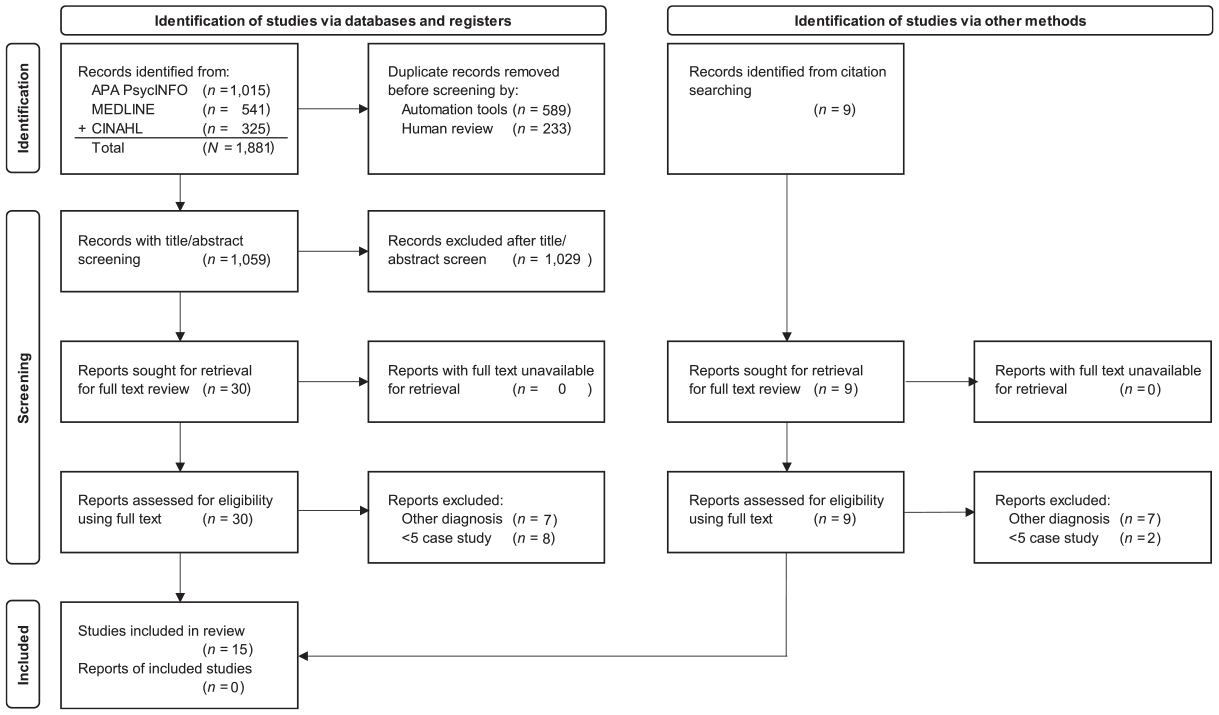
PRISMA 2020 flow diagram for database and citation search during the systematic review.
Data Analysis
Data analysis remained at the descriptive level involving summary statistics (e.g., percentages) organized by extraction categories. This permitted the exploration of commonalities and differences in treatment approach/setting, parent training, and response to intervention reporting across identified studies.
Results
Summary of Studies and Sample Characteristics
The search yielded 12 articles from a pool of 1,059 possible studies. Table 1 presents an overview of each study and sample characteristics. All interventions were delivered at a clinic; 9 of the 12 studies (75%) took place in a clinic described as specializing in the assessment and treatment of pediatric feeding disorder. The identified studies employed a variety of research design methodology (Table 2). This included three studies (25%) involving a randomized clinical trial (RCT), four (33%) involving a retrospective chart review, two (17%) involving an open trial, two (17%) using a hybrid model combining single case research design and RCT methodology, and one (8%) involving a single case research design. Collectively, the studies included 209 total children with ASD receiving a feeding intervention. The samples size per study ranged from 6 to 46. When reported, males represented the majority of cases (range: 71%‒100%). In general, the pool of studies appeared to involve a relatively young cohort of patients (10 years of less).
Summary of Study and Sample Characteristic by Study.
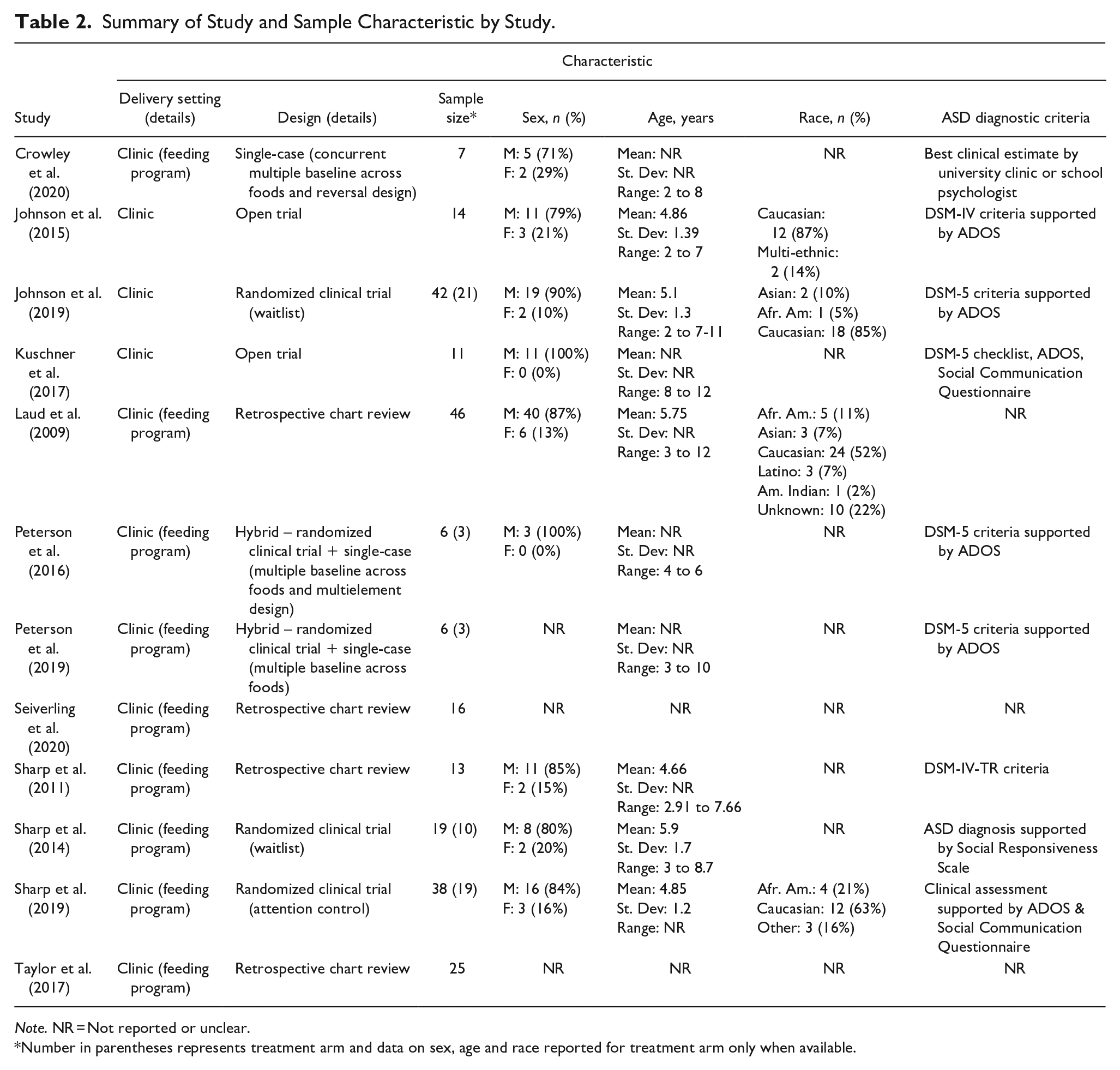
Note. NR = Not reported or unclear.
Number in parentheses represents treatment arm and data on sex, age and race reported for treatment arm only when available.
Treatment Delivery and Approach to Intervention
Eleven studies (91%) described the intervention delivery format (Table 3). Eight (67%) involved individual sessions, two (17%) involved a group format, and one study combined individual and group-based sessions. Delivery of treatment occurred in a treatment room in eight studies (53%). Two studies (17%) did not provide adequate detail to determine whether intervention occurred in an individual treatment room, however, both of these studies described treatment as occurring during admission to an intensive day treatment model of care. Four studies (33%) involved caregivers receiving parent training at a clinic and subsequently implementing the feeding intervention at home.
Description of Feeding Intervention.
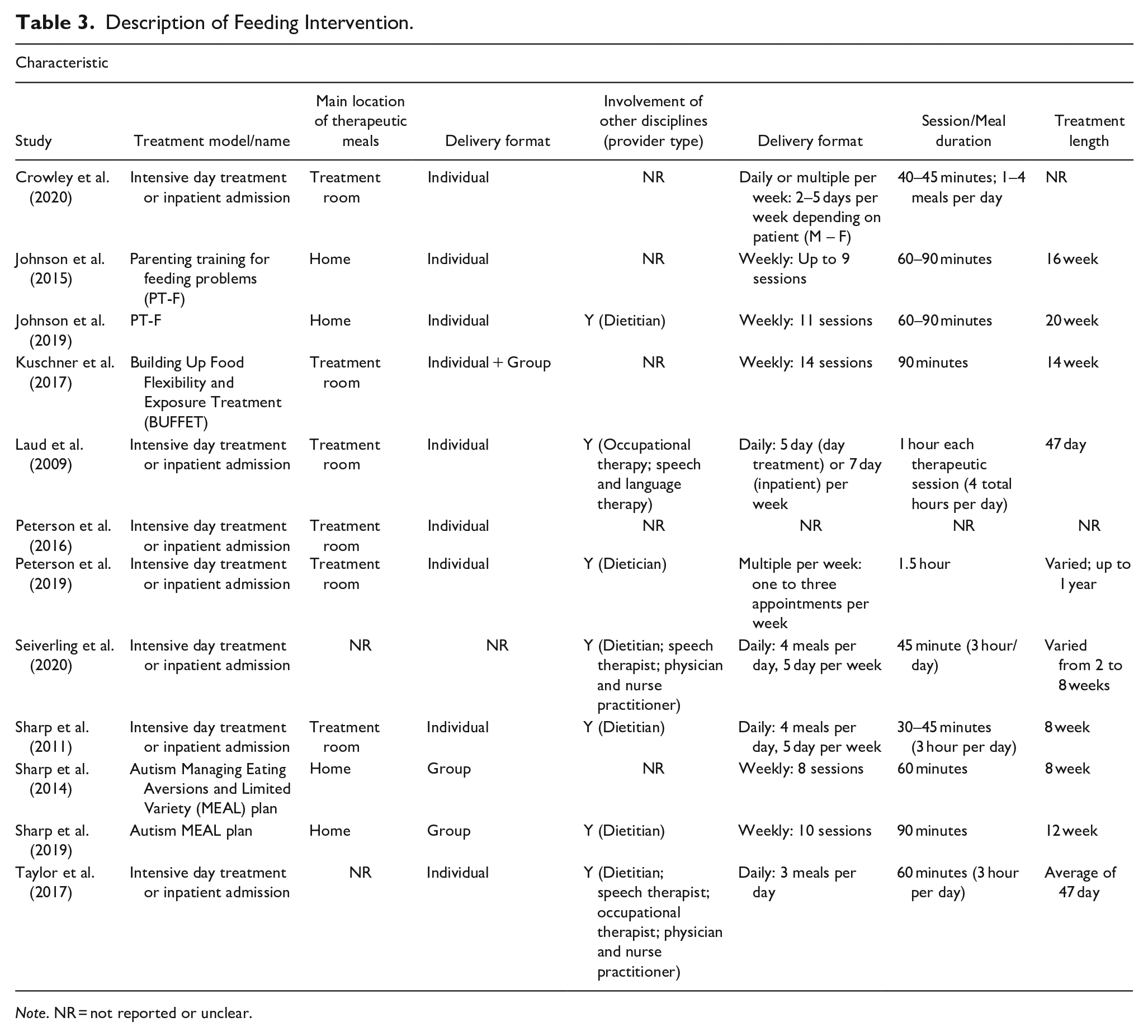
Note. NR = not reported or unclear.
Seven of the 12 studies (58%) involved intensive intervention delivered daily (M-F) (four studies; 33%) or through multiple meals per week (three studies; 25%) during a day or inpatient admission. In these studies, meals occurred for a fixed time period (e.g., 40 minutes; four meals per day). The remaining five studies (42%) evaluated three “branded” parent-training interventions (PT-F, MEAL plan, BUFFET) involving a standard curriculum. Branded interventions involved a set number of sessions delivered on a weekly basis over multiple weeks/months (e.g., nine sessions lasting 60–90 minutes per session delivered over a 20-week time period).
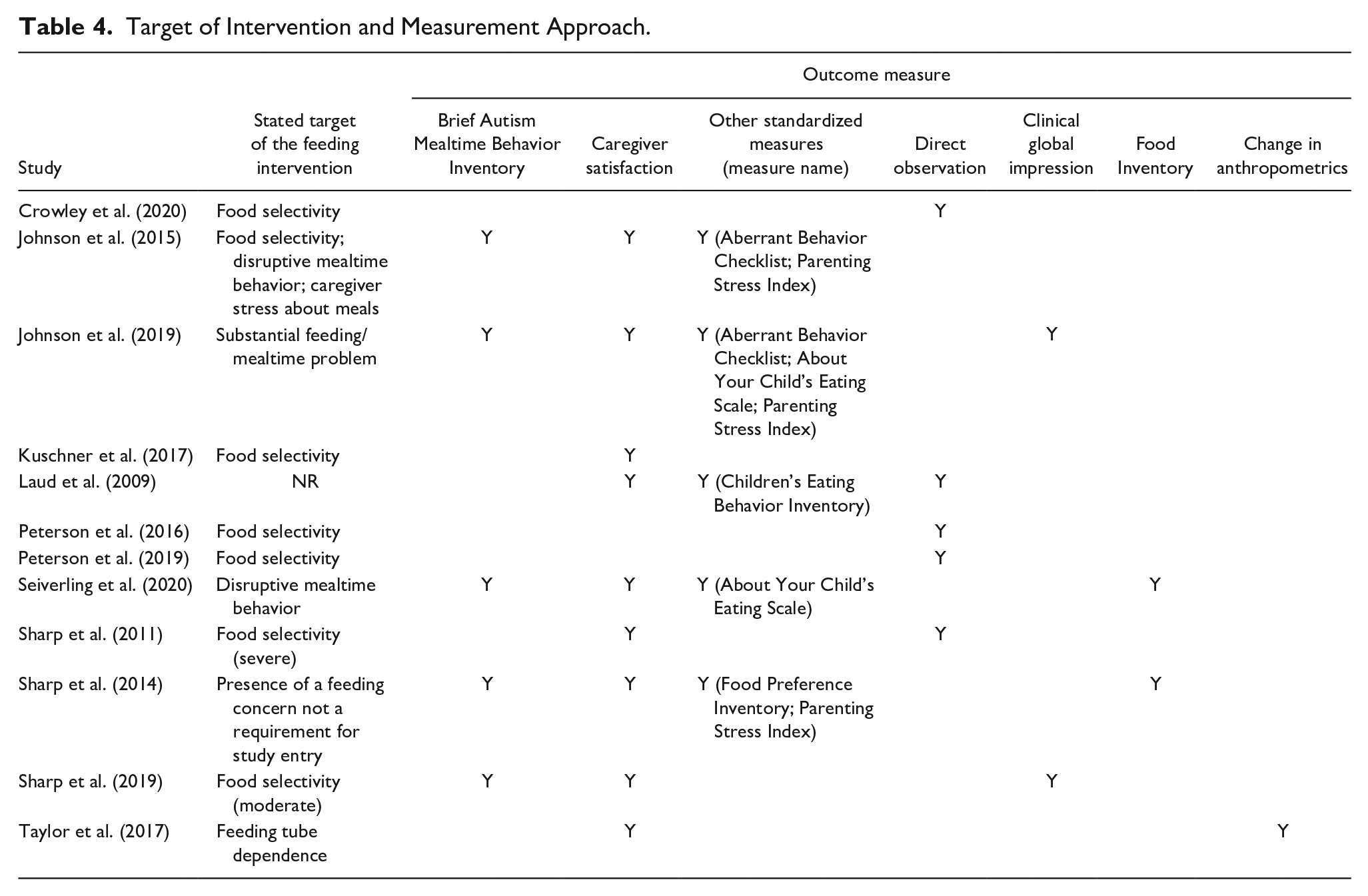
Target of Intervention and Measurement Approach
Seven studies (58%) involved specific reference to food selectivity as the target of intervention (Table 4), with two of these seven studies qualifying the severity of the food selectivity (i.e., moderate, severe). Caregiver satisfaction represented the most common outcome measure employed in the pool of studies (n = 9; 75%), followed by the Brief Autism Mealtime Behavior Inventory (BAMBI; n = 5; 42%) and direct observation of mealtime performance (n = 5; 42%). Five studies (42%) employed a variety of other parent-report questionnaires. Eight of the studies (67%) involved a multi-method battery of assessments.
Target of Intervention and Measurement Approach.
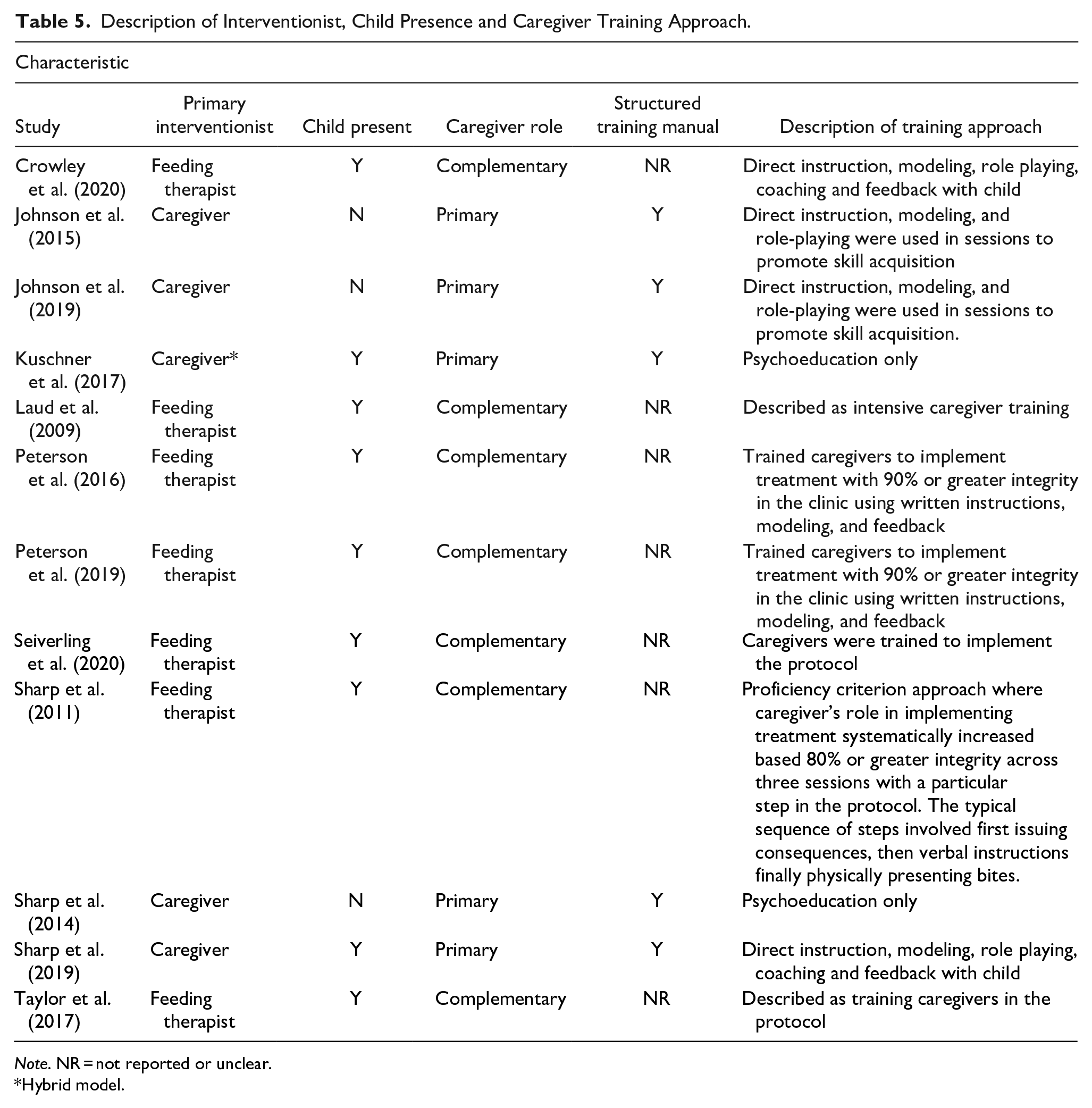
Interventionist, Child Involvement, and Caregiver Training
Seven studies (58%) involved a feeding therapist delivering treatment prior to generalizing treatment gains to a caregiver through caregiver training (i.e., a complementary caregiver role) (Table 5). These seven studies also coincided with treatment occurring during admission to a day or inpatient program. In this model, the feeding therapist established a treatment protocol, worked to stabilize the child’s behavior, and then generalized this protocol and progress to caregivers through activities that included direct instruction, modeling, and role playing. This process of treatment generalization was often guided by a proficiency or integrity target (e.g., 90% of greater caregiver integrity in the clinic) as part of the training process. In contrast, the five studies (42%) where the caregiver served as the primary interventionist at the onset of intervention represented the branded, structured training manuals (e.g., MEAL plan). The minimum level of training among these training manuals involved psychoeducation only (i.e., Kuschner et al., 2017; Sharp et al., 2014). PT-F developed by Johnson et al. (2015, 2019) and the most recent iteration of MEAL plan involved training activities similar to those employed during behavioral intervention occurring at day treatment or inpatient programs, such as direct instruction and role playing. PT-F and MEAL plan, however, differed regarding child involvement in this training process. PT-F did not involve the child during the training process, while MEAL plan involved parent-child dyads.
Description of Interventionist, Child Presence and Caregiver Training Approach.
Note. NR = not reported or unclear.
Hybrid model.
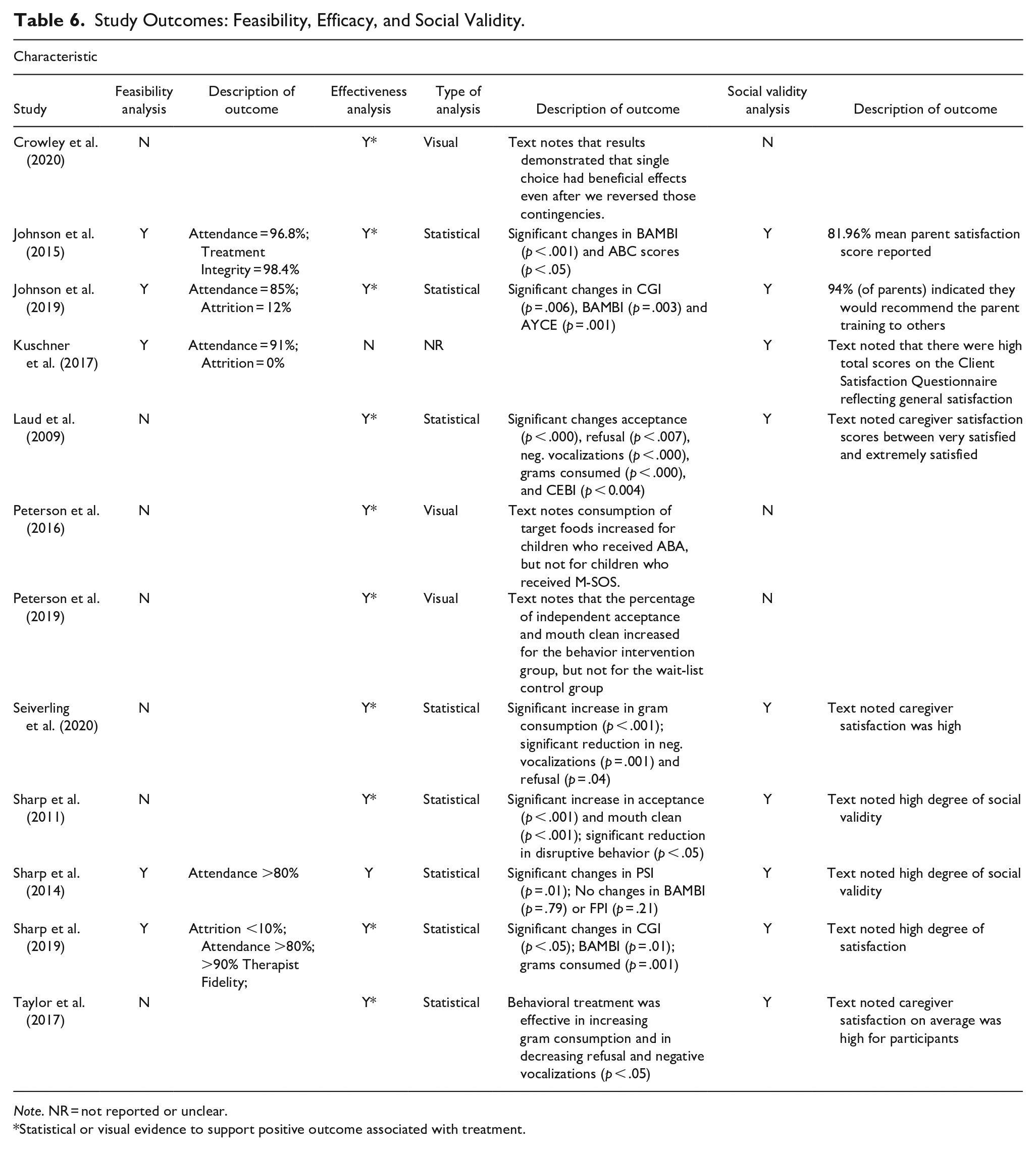
Study Outcomes
Table 6 provides a description of study outcomes including feasibility, efficacy, and social validity. Five studies (33%) presented data on feasibility metrics; all five involved manual-based treatments (i.e., PT-F; MEAL plan; BUFFET) and presented data supporting feasibility. Eleven of the 12 studies (92%) involved either statistical or visual data analysis to determine the potential impact of intervention. When analyzed, 10 of 11 studies demonstrated some evidence (i.e., statistical or visual evidence of treatment efficacy on primary outcome measures) supporting the efficacy of intervention in improving feeding outcomes. All nine studies assessing social validity via caregiver satisfaction questionnaire reported high levels of satisfaction associated with intervention.
Study Outcomes: Feasibility, Efficacy, and Social Validity.
Note. NR = not reported or unclear.
Statistical or visual evidence to support positive outcome associated with treatment.
Discussion
This systematic review identified 12 studies evaluating the benefits of behavioral intervention to target feeding problems in children with ASD that also described the involvement of parent training in the treatment process. This review compliments prior reviews evaluating behavioral intervention to address feeding problems in children with ASD - which primarily summarized single-case research studies (e.g., Aponte et al., 2019; Ledford et al., 2018)—to show a similar pattern of benefit when evaluated using a group design. The consensus outcome across the pool of studies suggests likely benefit associated with intervention, with evidence of a positive change on one or more outcome measures in 10 of the 11 studies evaluating effectiveness. Eight of these studies evaluated outcomes using statistical analysis, with seven of the eight noting a statistically significant change associated with treatment. The remaining three studies evaluated treatment outcomes through visual analysis of mealtime data; all three describe positive changes in performance following intervention. When reported, the pool of studies also provides evidence of high social validity associated with treatment as measured by post-intervention satisfaction questionnaires. This evidence most often involved a narrative description of caregiver satisfaction (i.e., there was a high degree of satisfaction).
Our findings are consistent with the framework presented by Bearss et al. (2015), with parent training either involving a primary or complimentary approach to empower caregivers to deliver intervention. Approached using this framework, a few themes emerged. First, the approach to caregiver involvement appears context dependent. Complementary training occurred exclusively during admission to day treatment or inpatient programs; primary training involved branded treatments designed for delivery in an outpatient setting. Second, the frequency of contact and main location of therapeutic meals coincides with this dichotomy. Treatment occurring at day treatment or inpatient programs involved delivery of intervention in a treatment room at a feeding clinic. In this model, treatment most often involved daily therapeutic activities. In contrast, branded treatments involved caregivers implementing intervention in the home setting between training sessions and clinical contact occurred on a less frequent (weekly) basis. Finally, there appears to be some similarities in training activities (e.g., direct instruction, modeling, role playing) across both primary and complimentary models; however, branded treatments specifically reference the use of a structured training manual/curriculum for teaching behavioral principles.
Our findings are less clear regarding factors driving this dichotomy in parent involvement. One possibility is that treatment setting serves as a proxy for symptom severity. That is, children requiring daily therapeutic support may necessitate a therapist-driven intervention at the onset of treatment due to the intensity of the feeding problem. Intuitively, it also makes sense that children with less severe feeding problems would more likely benefit from a parent-mediated (i.e., primary) model of care. Manual-base interventions (e.g., PT-F; MEAL Plan) were specifically designed for caregivers to serve as primary interventionist; the MEAL Plan also explicitly references targeting a moderate level of food selectivity. Few studies in this review, however, provided specificity regarding symptom severity to fully elucidate whether certain patient characteristics are associated with use of a primary or complimentary model of parent training.
The studies captured in this review suggest there may be increased interest in describing and evaluating parent training within the context of feeding intervention. Although the search spanned a 50-year period, the earliest article identified in this review was published in 2009; nine of the 12 studies (75%) were published since 2015. While the field currently lacks specific guidelines for selecting a parent training approach (i.e., primary, complimentary) during a feeding focused treatment, this uptick in publications permits some general recommendations regarding best practice based on the extant literature. First, training should involve multiple modalities (e.g., role playing, psychoeducation, modeling) to promote skill acquisition. Second, live practice with the parent-child dyad conducting meals should be included as one of the modalities, when possible, to permit direct feedback and treatment adjustments as needed. Third, training should also include a method for tracking caregiver proficiency implementing treatment recommendations; a consideration particularly important when intervention involves more complicated and/or challenging mealtime modifications. Finally, the training process should include programing for client-specific considerations (e.g., meals with siblings; frequent meals outside the home) to promote optimal generalization and maintenance of treatment gains in the home environment.
This review is limited by the data available in the identified articles. Although data extraction followed a standardized process, we may not have fully captured what occurred during feeding intervention, including parent training, due to lack of sufficient detail in the text. The extant literature is also unclear whether training with different techniques/components promote generalization to other settings (e.g., restaurants, social events, etc.) and/or whether caregivers continue to implement intervention with high treatment integrity in the absence of direct clinical support. Although some studies reported information on caregiver satisfaction with training methods, further clarity is needed on the social validity of training approaches and/or preference for different methods for empowering caregivers to deliver treatment. Future research is also encouraged to present data on parent characteristics (e.g., age, sex) that might inform adaptations or modifications to training to enhance adoption. This reflects a broader need to develop best practice standards for caregiver involvement in feeding intervention. Future research should continue to explore efficient and effective avenues to involve caregivers during the treatment process and report on these processes following established guidelines to permit replication and/or independent evaluation of different training approaches (e.g., Strengthening of Reporting of Observational Studies in Epidemiology [STROBE]; von Elm et al., 2007).
In sum, this review corroborates prior support for behavioral intervention leading to improved feeding outcomes for children with ASD while also documenting caregiver participation in the treatment process. In doing so, the review also identified the need for enhanced descriptions of the training process. Small improvements in research rigor and a more thorough description of procedures could enhance efforts to involve caregivers in feeding interventions. It would also expand our understanding of whether certain patient or parent characteristics are associated with the use of a primary versus complimentary models of parent training. This includes important questions about the treatment setting, training approach, severity of the feeding problem and/or maintenance of outcomes outside of the clinic setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Marcus Foundation.