
Abstract
Complex motor stereotypies are rhythmic, repetitive, fixed, and non-goal directed movements (e.g., bilateral flapping/waving movements of the hands/arms). Movements typically begin in early childhood and can occur in otherwise normally developing (“primary”) or autistic (“secondary”) children. Stereotypies persist, occur multiple times a day, have prolonged durations, can be socially stigmatizing, and may lead to bullying and isolation. Prior behavioral treatment studies have focused on older children (ages 6–12) and report modest reductions in stereotypy (i.e., between 14% and 33%). The current study involves the functional assessment and treatment of five children with Primary Complex Motor Stereotypy using a modified awareness training procedure, differential reinforcement of other behavior, and schedule thinning in a nonconcurrent multiple baseline design. Results suggest a 99% reduction of motor stereotypy from baseline across all participants.
Keywords
Motor stereotypies are broadly defined as involuntary, rhythmic, repetitive movements that have a predictable, fixed pattern (form, fashion, amplitude, and location), appear purposeful, are prolonged in duration, and stop with distraction (Singer, 2009). Movements can assume multiple forms including bilateral arm flapping or rotating, hand waving/flapping, finger wiggling, leg shaking, body rocking, and head nodding (Singer, 2013). They may also contain other accompanying activities such as mouth opening or head posturing, occasionally making a sound, or the performing of the repetitive behavior while pacing or jumping. Motor stereotypies typically begin between ages 1 and 3 years, occur in bursts, last from seconds to minutes or longer, and occur multiple times a day. Each child typically has their own repertoire that may evolve gradually over time (Mahone et al., 2004).
Motor stereotypies are classified into two groups, “primary” or “secondary” based upon the presence or absence of additional developmental problems. For example, they are most often observed in children with autism spectrum disorder (ASD), intellectual disability, or sensory deprivation (labeled as “secondary”) or when present in typically developing children identified as “primary” (Singer, 2009). Primary motor stereotypies have been further differentiated into common (e.g., pencil tapping, nail biting, leg swinging), head nodding, and complex (involve bilateral, multiple movements such as hand and arm flapping and waving) (Péter et al., 2017; Singer, 2013). Movements typically occur when a child is engrossed in an activity, or experiencing periods of excitement, fatigue, stress, or boredom (Mahone et al., 2004; Singer, 2013). A subgroup has also been defined based on the presence of accompanying thoughts or visual imagery, labeled as intense imagery movements (IIM) (Robinson et al., 2014). The precise prevalence of primary complex motor stereotypies (pCMS) in children is unknown, with cited ranges between 2% and 10% (Kravitz, 1971; Péter et al., 2017; Salustro, 1978; Singer, 2009, 2013). Follow up studies have confirmed their persistence into adolescence (Castellanos, 1996; Niehaus, 2000; Oakley, 2015) and studies are currently assessing their presence in adulthood. Common comorbidities in pCMS include ADHD, tics, obsessive-compulsive disorder, and motor coordination problems (Harris et al., 2008; Mahone et al., 2014; Oakley, 2015). The precise etiology of pCMS is unknown with preliminary suggestions of Mendelian inheritance and de novo nonsense variants (Fernandez, 2022; Harris et al., 2008). The underlying pathophysiological mechanism for stereotypies is unknown with hypotheses ranging from psychological concerns to developmental alterations within cortico-striatal pathways (Augustine, 2021; Kates, 2005; Rapp, 2005).
PCMS is most often diagnosed by a pediatrician or neurologist following observation of the child and report by caregivers regarding symptom presentation (Barry et al., 2011). While capable of producing rich descriptive information, these assessment methods fail to conclusively identify the contextual variables which may influence the evocation and maintenance of complex motor stereotypy. The use of a systematic approach to assess environmental variables related to behaviors targeted for reduction (e.g., antecedent analysis; Smith & Iwata, 1997), common in the assessment and treatment of motor and vocal stereotypies in individuals with autism, provides important data for generating efficient and effective interventions (e.g., Heyvaert et al., 2014). Even for behaviors thought to be maintained in the absence of social stimuli (i.e., automatic reinforcement; Akers et al., 2020), the use of systematic and direct observation of antecedents may yield important considerations for treatment development. For instance, Barnea et al. (2016) evaluated the correspondence between indirect versus direct assessment procedures used to identify contexts where symptoms of movement disorders were likely to occur. They found significant inconsistencies between the self-report and direct observation measures; authors suggested that direct observation is a more sensitive approach to data gathering, as attending to variables related to internal events may be challenging for some learners.
Behavioral interventions are considered the front-line treatments for repetitive behaviors in both autistic (Boyd, 2012; Giles, 2012; Rapp, 2005) and pCMS (Bhatoa et al., 2022; Miller et al., 2006; Singer et al., 2013) neurotypical populations. In studies of children ages 6 to 12 years old with pCMS, the most commonly used approach has been a behavioral procedure combining awareness training and differential reinforcement of other behavior (DRO; e.g., Specht et al., 2016). In their approach, Specht et al. asked participants to mimic their own stereotypy after watching a video of themselves engaging in the behavior naturalistically (i.e., awareness training). Therapists then differentially reinforced participants’ suppression of stereotypy and gradually thinned the schedule of reinforcement. This awareness training plus DRO procedure has been shown to be beneficial in reducing complex motor stereotypies (Miller et al., 2006; Singer et al., 2013). Additional research on the combined use of a home-based, parent-administered DVD behavioral training program (Specht et al., 2016) plus telephone support provided by an experienced therapist showed promise in increasing the accessibility of previous procedures (Singer, 2018). Nevertheless, these preliminary studies raised noteworthy concerns and emphasized the need to identify and implement further alterations. For instance, despite over 80% of children developing PCMS before turning 3 years of age, research on behavioral intervention for PCMS reduction has focused primarily on older children in middle childhood through adolescence (e.g., Miller et al., 2006). The omission of younger children in previous studies is likely due to difficulty self-monitoring their behavior (including their own engagement in motor stereotypy), and complications when completing awareness training (Specht et al., 2012). In addition, although published studies were beneficial, efforts to further enhance their published 14% to 33% improvement on movement and impairment scales provide a meaningful next step for future research.
One approach, used to mitigate both skills and motivational challenges when using procedures consistent with behavior modification is to offer children rewards for suppressing their own stereotypy (Miller et al., 2006). However, the literature on teaching individuals to self-monitor as the sole intervention for stereotypy suggests that these procedures may be difficult to implement and may not yield meaningful results (Fritz et al., 2012). However, it is possible that a self-monitoring component could bolster the effects of a differential reinforcement of other behavior (DRO) paradigm. The purpose of the current study is to extend the literature on the treatment of primary motor stereotypy in three ways: first, by using a functional assessment designed to identify contexts where stereotypy was most likely to occur, second, by using a modified game-based procedure for awareness training to increase its applicability for young children with PCMS, and third, by incorporating contexts identified in the assessment into treatment in order to increase the generality of the results.
Method
Participants and Setting
Five children (M = 5.4 years, range 4–6 years) and their caregivers participated in the current investigation. Each was referred for the behavioral treatment of motor stereotypies by their neurologist, who had confirmed the diagnosis of pCMS. Caregivers reported seeking services due to socially impairing rates of motor stereotypy occurring at school and community settings. None had received any previous behavioral intervention to address motor stereotypies. See Table 1 for participant demographics.
Participant Demographic Data.
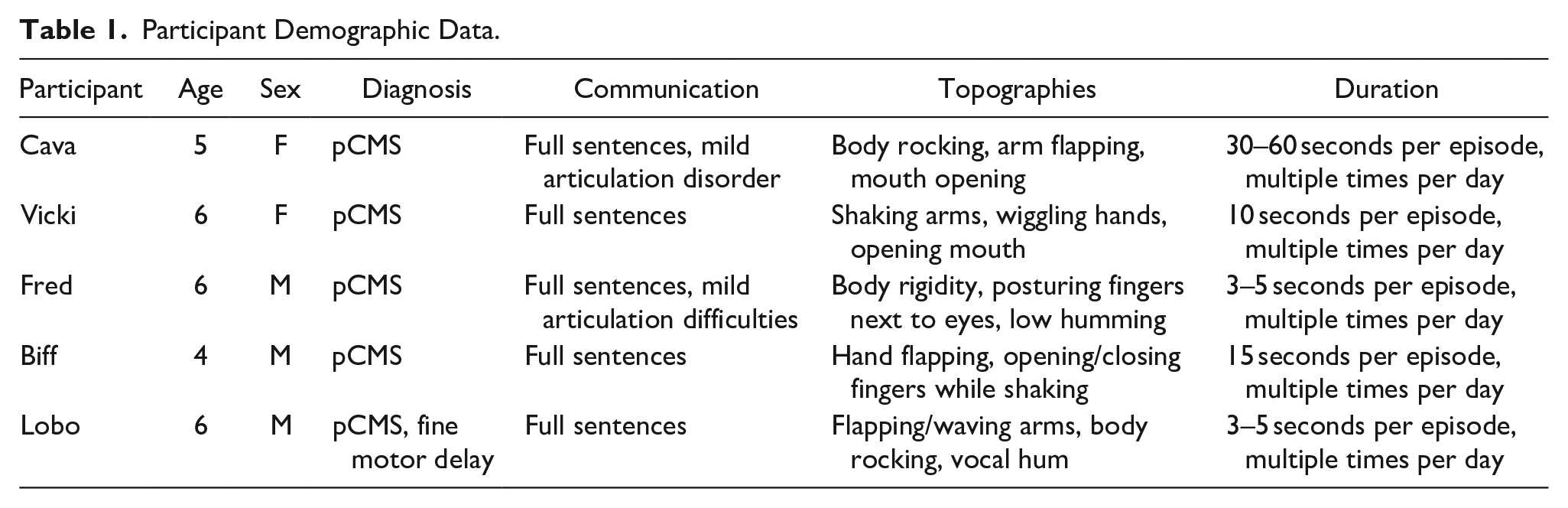
Sessions were conducted in a treatment room in a hospital-based outpatient behavior clinic in the mid-Atlantic region of the United States. Treatment courses averaged 7.6 hours, with a range of 6 to 10 hours arranged across 3 to 5 consecutive days. Each treatment room included tables, chairs, and was equipped with audio/video recording equipment that was used for later coding and interobserver agreement. Treatment teams included one clinician, the participant, and their caregiver(s). Clinicians trained caregivers to conduct all assessment and treatment sessions using a behavioral skills training paradigm (i.e., instructions, modeling, rehearsal, and feedback; Green, 1996). All participants assented to participate in their own treatment.
Response Measurement, Interobserver Agreement, and Treatment Integrity
For both the antecedent analysis and treatment evaluation sessions, motor stereotypy data were collected via pencil and paper along with a digital timer to record duration of motor stereotypy in seconds, using a two-second onset and offset criterion. That is, the therapist recorded the duration of stereotypy by starting a timer once it began and stopping the timer upon its cessation. This criterion was used in order to capture relative percentages of stereotypy, and allowed the therapist to make data-based decisions in-vivo during the appointments. As this data collection procedure had the potential for increased human error, all sessions were recorded using a HIPAA compliant video and cloud-based storage system that allowed for later review and coding. All appointments were re-coded after they occurred in order to calculate exact percentages of stereotypy that occurred during sessions. The percentage of motor stereotypy during the session was calculated by dividing the total duration of stereotypy that occurred by the total duration of the session. Motor stereotypy for all participants was broadly defined as rhythmic and repetitive flapping, waving, and body rocking; see Table 2 for individual definitions. Although it did not occur during the assessment or treatment sessions, any instances of disruptive behavior would also have been recorded.
Participant Interobserver Data.
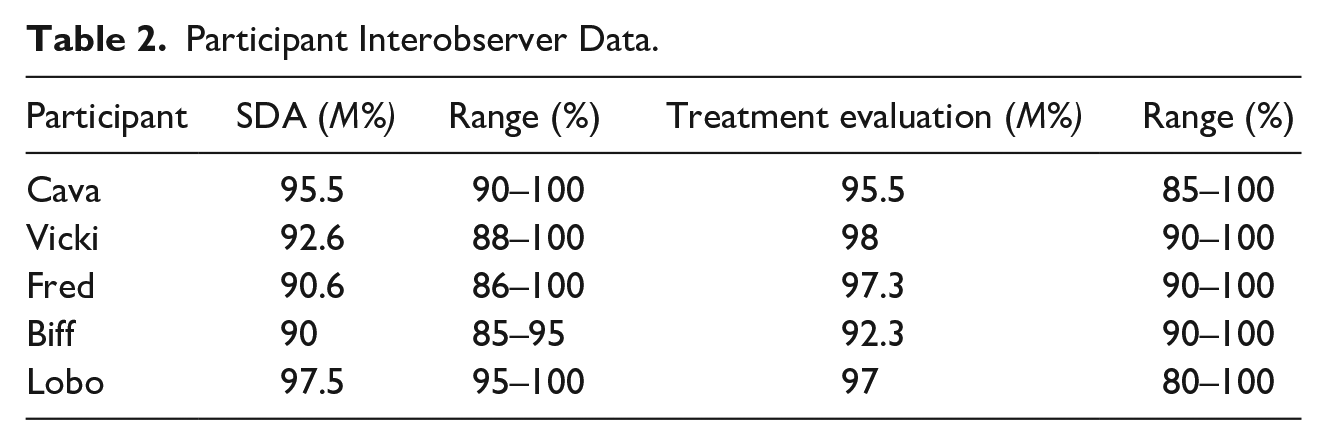
To determine interobserver agreement (IOA), a partial agreement within intervals method was used. Specifically, we divided all sessions into 10-second intervals; during these intervals, the smaller number of seconds of stereotypy was divided by the larger number and converted to a percentage. Agreement on the nonoccurrence of the behavior was scored as 100%. The percentage of all intervals were then averaged across the session. IOA was calculated on an average of 71% of all antecedent analysis sessions (range, 50–100%) and 55% of all treatment sessions (range, 50–60%). See Table 2 for IOA calculations for all participants.
Procedural integrity of therapists and/or caregivers was also evaluated in 30% of antecedent analysis and treatment evaluation sessions via the video recording system. To calculate the percentage of correct procedural implementation, we divided the correct therapist responses by total opportunities and multiplied by 100%. Procedural integrity averaged 90% for Cava (range, 80–100%), 96% for Lobo (range, 80–100%), 99% for Vicki (range, 90–100%), 95% for Biff (range, 90–100%), and 90% for Fred (range, 80–100%).
Procedures
Indirect assessment
Prior to conducting the antecedent analysis, participants and their caregivers were interviewed using a semi-structured assessment tool to develop a preliminary list of hypothesized setting events that were correlated with motor stereotypy, as well as to identify participant preferences around specific items and activities (see Appendix A for complete assessment, with specific prompts to solicit responses included in quotations). Specific questions involved asking caregivers their observations related to what their children were engaged with during periods of stereotypy. During discussion around frequency and topography of stereotypic movements (i.e., steps 1–5) between therapists and caregivers, participants were free to engage in preferred activities that were made available noncontingently. This free play time was used to maximize comfort during this initial appointment and provided opportunities for rapport building. During discussion around high stimulation items (i.e., step 6), therapists included participants to the extent possible (e.g., asked participants about preferences, then confirmed with caregivers regarding their retrospective observations about relationships between engagement and stereotypy). Participant responding varied during the indirect assessment; however, all were able to comment on their preferences with minimal prompting. Information gathered from this indirect assessment informed hypotheses related to high and low stimulation contexts that would later be tested in the functional assessment.
Caregivers also shared videos of participants’ stereotypy with therapists to assist with creating operational definitions. In addition to obtaining their assent for treatment, therapists also discussed motor stereotypies with participants themselves to better understand their expectations for treatment. Most caregivers reported that they had not previously discussed stereotypy with their child for fear of creating undue anxiety. Interestingly, when participants were asked, they were all aware that these behaviors were occurring. Some shared that their stereotypy only bothered them when they engaged in the behavior unknowingly in public; however they also expressed that they enjoyed their stereotypy during periods of boredom or when they were engaged with high preferred activities. Therapists worked with participants and their caregivers to identify environments where stereotypy caused child distress; these contexts were the only ones where the intervention would be implemented (i.e., children would be free to engage in motor stereotypy during times of their choosing).
Structured descriptive assessment
The functional assessment was conducted using a multielement design in order to identify discriminative conditions under which complex motor stereotypy may be more likely to occur (Durand & Carr, 1992). Conditions were informed from the indirect assessment and included attention, control, alone (Fred, Lobo, Biff), ignore (Vicki), a high stimulation condition (Vicki, Fred), and a low stimulation condition (Fred, Vicki, Cava, Biff, Lobo). There were no programmed consequences for motor stereotypy in any of the conditions, as all caregivers noted that stereotypy was likely to abate following interruption (e.g., when participants were vocally redirected to another activity). During the attention condition, participants had continuous, noncontingent access to caregiver attention without any other stimuli in the room. During the control conditions, participants were provided with preferred items and caregivers were instructed to play with their child as they typically would. During alone conditions, participants were instructed to remain in the treatment room while caregivers stepped out to complete paperwork. The ignore condition, which was used for Vicki after she expressed concern about being left alone in the treatment room, involved both caregivers being unavailable to provide attention or access to preferred items and was signaled by parents’ diverted attention to a work laptop. High stimulation conditions involved noncontingent access to music (Vicki) or videos (Fred) via an iPad© or tablet that were identified as being high preferred activities by participants. Low stimulation conditions involved access to activities (e.g., books, toys, and drawing) that were identified by participants as being low preferred. All assessment sessions were 5 minutes in duration.
Treatment evaluation
Following stable, differentiated responding in the functional assessment, a treatment evaluation was conducted using a nonconcurrent multiple baseline across participants (e.g., Ledford, 2022; Slocum et al., 2022). Caregivers of all participants implemented the treatment procedure which included two phases: first, involved a game-based awareness training (i.e., GBAT) procedure designed to promote participant awareness of stereotypic movements. Next, a differential reinforcement of other behavior (DRO) with schedule thinning procedure was used to motivate participants to suppress stereotypy for a fixed interval of time. Importantly, treatment evaluation sessions occurred in the evocative contexts identified by the antecedent analysis. During both phases, caregivers were trained to implement treatment procedures using a behavioral skills training paradigm (i.e., instructions, modeling, rehearsal, and feedback; Green, 1996). Specifically, therapists modeled the use of the procedure for caregivers, then gradually faded themselves out of the treatment room while providing directive feedback. Criteria for mastery involved independent implementation of all procedures at 100% fidelity, and therapists provided immediate corrective feedback upon the occurrence of procedural errors.
Game-Based Awareness Training involved an adapted awareness training procedure designed to increase acceptability and feasibility with a very young clinical population. Prior to the start of the procedure, the clinician provided instructions for how to play the game, which involved both participant and their caregiver(s) competing to quickly identify the occurrence of motor stereotypy. Specifically, caregivers were instructed to mimic the topography of stereotypy that they have observed from their child in order to increase the salience of the behavior for the child. Participants were taught to tact their observation of their caregivers’ demonstration of stereotypy using a preferred word or phrase (e.g., “Bazinga!”). Simultaneously, caregivers were instructed to use the same phrase to identify instances where their child engaged in operationally defined motor stereotypy. Correct identification of mimicked stereotypy earned either participants or their caregiver a point toward winning the game, depending on who engaged in stereotypy first. Thus, participants were motivated to both suppress their own stereotypy while recognizing the occurrence of approximations by their caregivers in order to win the game. Game duration varied, and ended after a “winner” reached 5 points, who was then permitted to select a 5-minute leisure activity. Caregivers were instructed both to have high discrimination of each occurrence of their child’s stereotypy and to engage in stereotypy approximations to improve their child’s discrimination skills.
Resetting Differential Reinforcement of Other Behavior (DRO) with Schedule Thinning occurred after participants successfully and accurately identified the presence of caregivers’ approximations of their stereotypy while minimizing their own (i.e., winning the “game” for three consecutive rounds). The DRO procedure involved teaching participants to suppress stereotypic behaviors for a fixed interval of time in order to earn access to tangible reinforcement (e.g., access to screen time, access to a preferred snack) that was identified by the participant. Specific suppression strategies were not explicitly taught, as previous research suggested that this was not a necessary component (e.g., Specht et al., 2016). The interval was set to 5 minutes as that was generally the length of a single game-based habit reversal session. A visual and/or physical discriminative stimulus (e.g., a bracelet worn exclusively during the DRO interval) was used to signal that the intervention was in place and facilitate generalization programming. Contingent on the presence of stereotypy during the DRO interval, the interval was reset and the caregiver provided a reminder to the participant about the expectations for earning their preferred activity. After the DRO interval ended, participants were permitted to take off the bracelet and could engage in stereotypy freely. The duration of the interval was determined by calculating the average session duration of the last three GBAT sessions. If the participants engaged in PCMS during the DRO interval, the interval time was reset and the caregiver provided a reminder to the participant regarding what they must do to earn the prize.
After three consecutive sessions in which the participant earned the prize without resetting the DRO interval, the interval was systematically increased by 50%. If the participant was unable to suppress PCMS at a given criterion, the DRO the interval was systematically decreased by 20%. At the end of the treatment course, therapists instructed caregivers to implement practice of the DRO procedure at the interval that was mastered during the in-person therapy. Recommendations included daily practice both in the presence of evocative stimuli identified in the assessment as well as across multiple contexts in the home.
Follow-up appointments were conducted with participants and their caregivers and occurred approximately 1 month on average after the completion of treatment (range, 3–6 weeks). Appointments occurred remotely in the family’s homes via a secure videoconferencing platform, and lasted 60 minutes. Each family used a smart device, which included both audio and video capabilities. During follow-up appointments, the therapist conducted live observations of the implementation of the DRO procedure, and data were collected on the percentage of stereotypy that occurred in each session as well as caregivers’ procedural fidelity. In addition, the therapists reviewed data collected by caregivers regarding the frequency and success of skills practice to determine the generality and overall feasibility of the treatment procedures.
Results
For Cava, motor stereotypy occurred a high rates in the control condition, where she was allowed to watch a favorite video (i.e., Peppa Pig) with her parents (Figure 1). A significant decrease was associated with the introduction of game-based awareness training (GBAT; 94% reduction from baseline), with further reductions occurring following implementation of the resetting DRO procedure (i.e., 97% reduction from baseline, Figure 3). Overall, there was low variability in her responding across phases once the awareness training component (i.e., GBAT) was implemented.
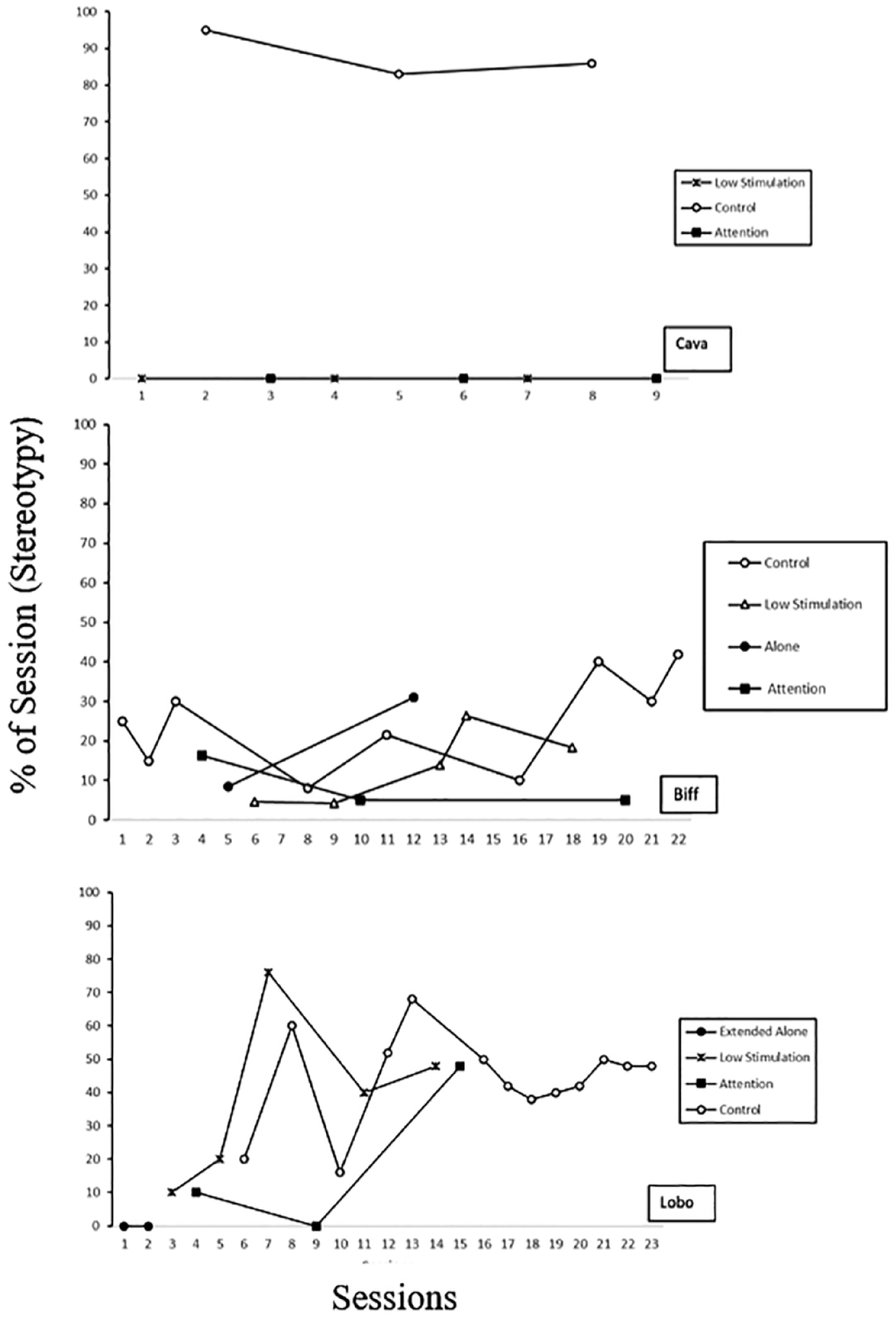
Structured descriptive assessment results for Cava, Biff, and Lobo.
For Biff and Lobo, motor stereotypy was largely undifferentiated across test and control conditions (Figure 1). However, as moderate levels of stereotypy were observed during the control conditions, and as functional impairment was reported to occur primarily in social settings with peers, the decision was made to extend the assessment in the control context to achieve stable baselines ahead of treatment. For both participants, implementation of the GBAT procedure for both participants resulted in reductions of motor stereotypy of 78% and 80%, respectively (Figure 3). Lobo engaged in variable responding immediately following the introduction of the resetting DRO procedure, which was suggested by his caregivers to be a reaction to the social demand of the DRO. However, levels of stereotypy reduced and stabilized by session 43 of the treatment evaluation. Both participants required multiple, consecutive resets to the DRO; Biff’s responding remained low, reflecting only a few short bouts of stereotypy that quickly came under stimulus control. Lobo required multiple resets of the DRO timer (e.g., sessions 33, 36, 39, 40) during the initial phase prior to successfully accessing the earned activity. Despite the need for multiple interval resets, Lobo’s responding stabilized and maintained at low levels once schedule thinning occurred.
Fred and Vicki (Figure 2) both engaged in motor stereotypy primarily in the high stimulation contexts, which involved noncontingent access to cartoon videos (Fred) or high preferred music (Vicki). Following the introduction of the independent variable (i.e., the GBAT), levels of stereotypy decreased to near-zero, reflecting a 98% reduction from baseline for both participants (Figure 3). Levels of stereotypy remained low following the implementation of the DRO procedure.
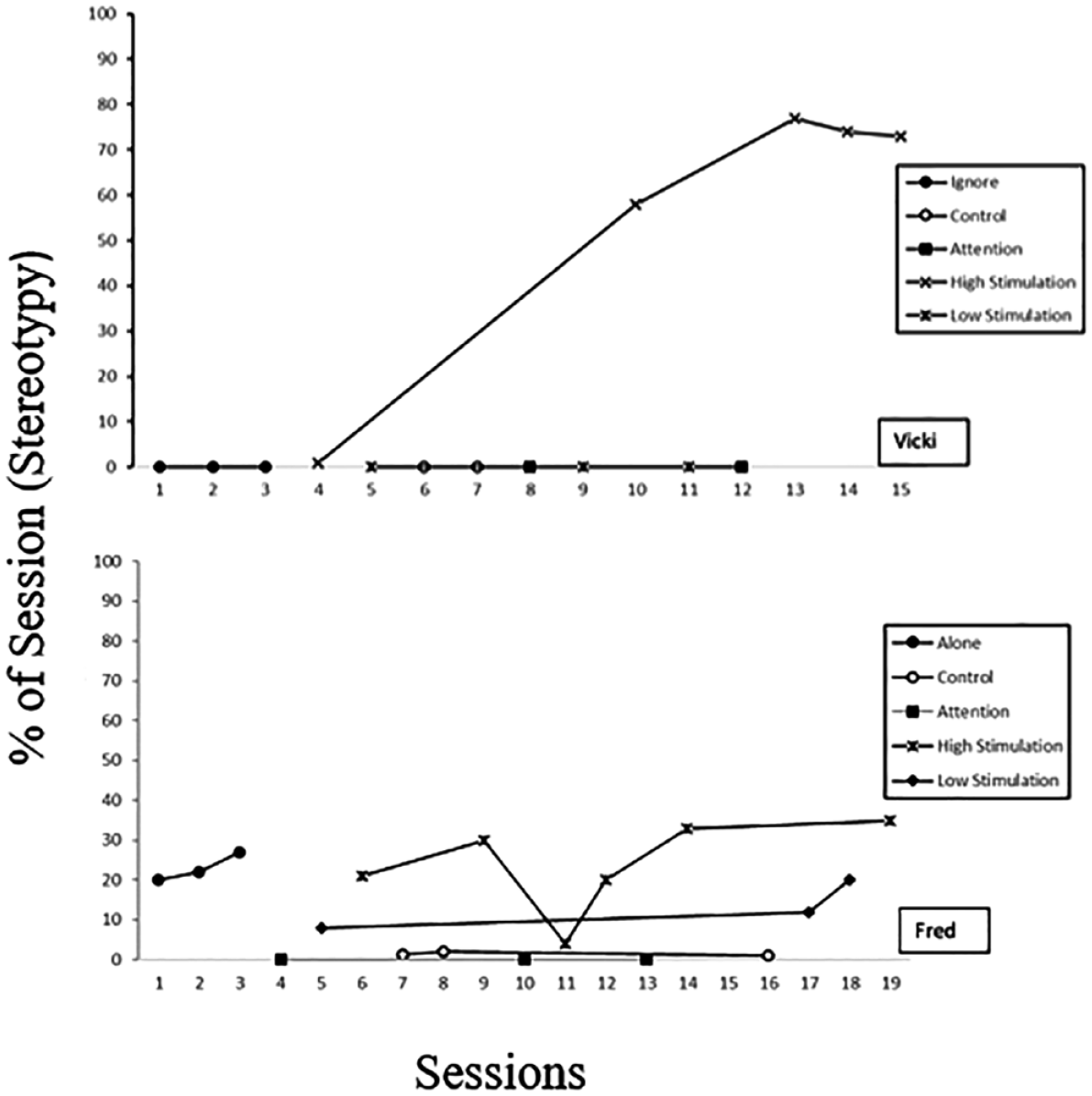
Structured descriptive assessment results for Vicki and Fred.
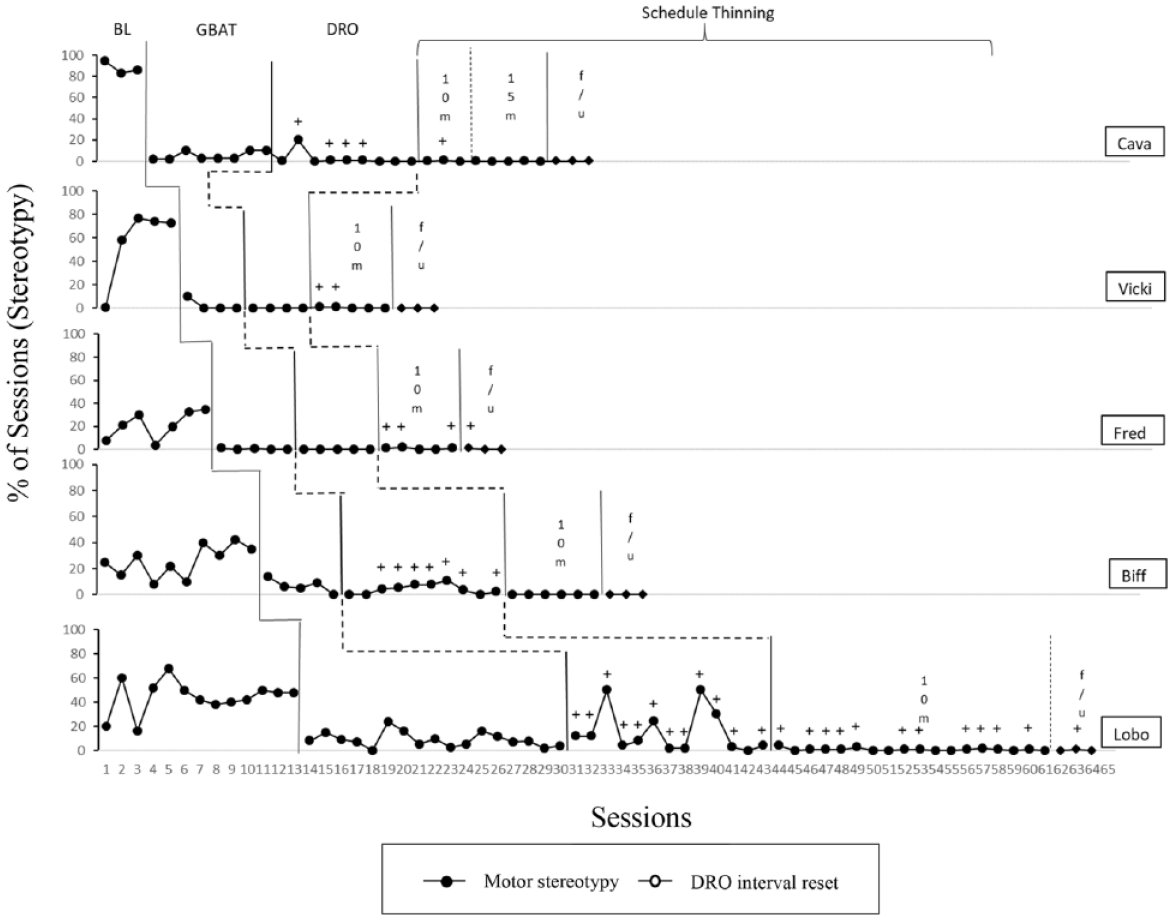
Nonconcurrent multiple baseline across participants.
Follow up data gathered during the telehealth appointments are reflected in the last phase of the treatment graphs. Therapists observed participants and their caregivers practice the DRO procedure in the context of evocative stimuli first identified in baseline. All participants were observed to have low and stable levels of stereotypy, with only two (Lobo and Fred) requiring a single trial where the DRO needed to be reset. Caregivers demonstrated 100% procedural fidelity during these structured observations. In addition, caregivers reported that the DRO procedure was effective in reducing stereotypy to near zero levels during generalization practice at home, with an average of 96% of practice trials occurring without the need to reset the DRO interval (range, 90–100%).
Discussion
The first objective of the current study was to leverage functional assessment procedures commonly used with autistic stereotypy to identify evocative contexts where participants’ complex motor stereotypies would reliably occur. To do so, we used a combination of indirect assessment (i.e., caregiver interview), videos taken of participants’ motor stereotypy occurring at home, and a systematic manipulation of antecedent variables. While it is likely that participants’ motor stereotypy was maintained via the sensory consequences produced by the emission of the behavior, these consequences were not specifically examined here. Caregiver report of the setting events of their child’s stereotypy was generally useful in creating broad hypotheses related to relevant antecedent test conditions. The inclusion of the antecedent analysis allowed for additional collaboration between caregivers and their therapist as to which types of contexts would produce the highest rates of stereotypy. Specifically, therapists solicited feedback from caregivers following each antecedent condition regarding whether rates observed were comparable to those seen at home. This dialogue allowed the assessment to be iterative in nature. The results suggest that, at least for these neurotypical learners, the specific setting events in the environment may mediate whether or not stereotypy occurs, and for what duration of time.
The second objective was to incorporate a modified procedure for awareness training that would be age-appropriate for early learners with pCMS. Previous studies targeting behavior change in this population have used a self-monitoring procedure involving practice in front of a full-length mirror (Miller et al., 2006). While these strategies have been effective for older populations, anecdotal reports have suggested that young children were unwilling or unable to benefit from these strategies due to inattention or poor motivation. The game-based awareness training procedure (i.e., GBAT) described in the current study involved teaching children to discriminate between the occurrence and nonoccurrence of stereotypy in an age-appropriate format. Referred to as “gamification” in the behavioral science literature (e.g., Sailer et al., 2017), the use of game-based elements in real-world contexts increases motivation, and thus, performance, in a specific activity. In our approach, the caregiver served as a model of their child’s own behavior, thereby prompting the child to monitor instances of similar behavior. The child was implicitly incentivized to engage in fewer instances of stereotypy and detect instances of their caregiver’s modeled stereotypy in order to win the game and earn access to a preferred activity.
The final objective of the study was to incorporate relevant contexts identified by the functional assessment procedure into the intervention to increase generality. Participants’ ability to suppress their stereotypy in previously evocative contexts suggests that the resetting DRO procedure may generalize beyond the treatment context. While the GBAT procedure did produce significant reductions in stereotypy for all participants, we felt the addition of the DRO provided a necessary external validity component to the intervention. Ultimately, treatment for pCMS is only useful to children if they can engage in daily activities while simultaneously suppressing their stereotypy at the times of their choosing.
These results are consistent with previous findings in the tics literature regarding tic suppression and the use of contingent reinforcement procedures (e.g., Woods et al., 2008). It is most likely that the effect of the intervention on motor stereotypy were the result of punishment (e.g., Specht et al., 2012) rather than reinforcement of other behavior. However, anecdotally, both caregivers and participants themselves reported high levels of acceptability with the procedure both during treatment and in subsequent follow up appointments.
Despite having promising preliminary results, there are a number of limitations to the current study. The first limitation is the experimental rigor of the study, which involved a nonconcurrent multiple baseline (MBL) across participants. Specifically, the use of nonconcurrent MBL designs have been criticized due to threats to internal validity (e.g., Cooper et al., 2020). Consistent with recommendations from Slocum et al. (2022), we attempted to arrange tiers with sufficient lag time between phase changes. In addition, the use of a nonconcurrent MBL across five participants design minimized the likelihood that coincidental events were impacting the experimental control of the intervention.
The order of phases (i.e., GBAT always preceding the DRO procedure) is another methodological limitation to the current study. As participants’ rates of stereotypy were reduced significantly during the GBAT phase, we were unable to experimentally demonstrate the utility for both awareness training and the DRO procedures. That is, the GBAT phase may do little to improve the reductions in stereotypy that would occur with a DRO phase alone. Future extensions of this research should alternate the order of the conditions to identify whether there is a beneficial impact of both phases of treatment. Inclusion of caregiver treatment acceptability measures would provide added benefit, as there may improvement in families’ subjective experience of stereotypic behavior during the gamification procedure.
Another potential limitation of the study is generality of the procedure given the small sample size and programmed length of the DRO interval itself. With regard to the former, given the relative scarcity of patients and families receiving this diagnosis and presenting for behavior therapy, we felt that reporting on these first five participants would be a sufficient first step in disseminating a promising variation of a traditional habit reversal procedure. Future research should replicate and extend the use of a game-based awareness training procedure for participants in a wider age range. Regarding the DRO length as a limitation, while we did seek to programmatically increase the interval in the course of our brief intervention, the goal of our pilot study was to examine the feasibility of the assessment and treatment procedures rather than to evaluate the limits of stretching the DRO interval. However, in school and community settings, participants would likely be required to suppress their motor stereotypy for periods considerably longer than ten minutes. While research on tic behaviors suggests that participants are able to engage in suppression for up to 40 minutes (Specht et al., 2012) without rebound effects, additional data are needed in order to test the durability of the suppressive effect of the DRO on motor stereotypies as interval length is extended.
Future research should seek to evaluate the effects of consequent manipulation on the maintenance of primary complex motor stereotypy. While such a procedure was outside the scope of our current investigation, a thorough evaluation of the reinforcing properties of motor stereotypy may lend additional insight into treatment options (e.g., use of sensory extinction) for this group. In addition, it may be useful to replicate the findings in the current study using other service modalities (i.e., telehealth) in an effort to increase the potential reach of the intervention.
Despite the limitations noted, the current study offers preliminary evidence for the efficient assessment and treatment of a socially stigmatizing behavior in a neurotypical pediatric population. An essential component of the treatment process was to help children develop discriminative control over their own behavior. As more is learned about the pathophysiological mechanisms for primary stereotypies, the procedures described in the current study may provide insight related to the interplay between environmental and biological processes.
Footnotes
Appendix A. Functional Interview of Tics and Stereotypies (FITS)
Indicate whether any of the following unwanted movements have been present in the last month
Indicate whether any of the following unwanted vocalizations have been present in the last month
_______________________________________________________________________________________________________________
____________________________________________________________________________
___________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
____________________________________________________________________________
_______________________________________________________________________________________________________________
“Many children with PCMS engage in stereotypy during periods of high stimulation. These next questions will try to help us identify activities that may be related to episodes of stereotypy.”
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
____________________________________________________________________________
_______________________________________________________________________________________________________________
____________________________________________________________________________
_________________________________________________________________________________________________________
_________________________________________________________________________________________________________
_________________________________________________________________________________________________________
Acknowledgements
We would like to thank Kissel Goldman, Steve Lindauer, and Kim Sloman for their feedback on previous versions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.