
Abstract
The Focus-Based Integrated Model (FBIM) tailors interventions based on a functional assessment of clients’ needs, integrating psychotherapy with pharmacological or rehabilitative support when necessary and emphasizing a strong Working Alliance (WA). This study evaluated therapeutic progress in clients treated with FBIM at four time points: baseline (T0), 3 months (T1), 12 months (T2), and follow-ups at 3 months post-therapy (T3). From April 2022 to July 2024, this longitudinal study was conducted at a community-based psychotherapy centre in Italy, enrolling 154 participants (Mage = 32.8 years; 54.3% female) who completed baseline assessments, with sociodemographic and clinical data collected on symptom severity, WA, and client motivation. Symptom severity declined significantly from T0 to T2. Within the integrated approach employed, that combined psychodynamic and Cognitive Behavioural Therapy (CBT) components, CBT showed stronger Task subscale scores at T2. Resistance to change impacted WA at T1 but decreased by T2. Contextual differences in WA at T1 diminished over time. Client motivation had no effect on WA. Structured approaches like CBT foster early collaboration, while changes in the WA over time reflect the therapist’s capacity to adapt to client needs and therapeutic challenges.
Keywords
Introduction
Integrated psychotherapy, now widely recognized for its clinical effectiveness, has evolved over decades, drawing from diverse therapeutic traditions, most notably the fusion of psychoanalytic and behavioural techniques (French, 1933). It was developed to combine the strengths of both approaches—symptom relief from cognitive-behavioural therapy (CBT) and the focus on relational dynamics from psychodynamic models—(Bordin, 1979; French, 1933; Freud, 1937, 1964; Greenson, 1965; Sterba, 1934), and evolved with the introduction of active therapist roles and techniques like homework and role-playing (Buchanan & Haslam, 2019; Cain, 2002; Markowitz & Weissman, 2004; Stolorow et al., 1987; Wachtel, 1977). This integration laid the groundwork for models that adopt a more holistic and personalized approach to treatment (Kozarić-Kovacić, 2008; Silberschatz, 2017).
One notable integrated model is the Focus-Based Integrated Model (FBIM), which combines psychodynamic and CBT strategies within a unified treatment trajectory, and may also include pharmacotherapy and rehabilitation programmes when indicated (Gislon, 2005; Kozarić-Kovacić, 2008). FBIM is characterized by a structured yet adaptable framework in which the therapist identifies a specific, evolving therapeutic focus based on rational, emotional, and behavioural assessment, often involving input from significant others (Gislon et al., 2010; Pagnini et al., 2013; Zapparoli, 1999). The plan is revised flexibly across phases, depending on the client’s developmental stage and complexity of the problem.
In the last decade, the FBIM has been developed by the Institute for the Study and Research on Mental Disorders (Istituto Per Lo Studio E La Ricerca Sui Disturbi Psichici, ISeRDiP) as a new psychotherapy model (Gislon, 2000, 2005; Zapparoli, 2009) that integrates psychodynamic psychotherapy of Freudian origin with Erikson’s life cycle model and cognitive-behavioural psychotherapy. This model, based mainly on focal interventions, it is classified as short-term psychotherapy with an average duration of fewer than 40 sessions. The model works on five fundamental pillars: (1) the specificity of the diagnosis (e.g. identifies the developmental dilemmas and conflicts); (2) the focus (e.g. the central conflict-what is the fear behind this conflict, and how dysfunctional mechanisms defends itself from this fear); (3) the integrated intervention (see below for further information); (4) the setting of self-therapy (e.g. awareness of new perspectives of functioning internalizing the tools to manage the symptoms), and (5) resistances to change (e.g. highlighting overly rigid defences, a lack of flexibility to change, and difficulty in relating and receiving help). A functional diagnosis is established during the initial sessions, in which the patient’s evolutionary conflict—referred to as the focus—is identified. This conflict arises between the individual’s evolving needs over the course of life and the fears that may emerge in response to these changes. To manage these fears, the person may adopt dysfunctional reactions, known as defences, which hinder the natural development of their life, leading to psychological distress and symptoms.
The therapist, trained in the FBIM model, offers the patient this functional interpretation of their problem and proposes the most suitable therapeutic intervention to address the specific fears and defences involved. To foster a strong therapeutic alliance and ensure brevity of treatment, the therapist decides whether to initially adopt a CBT-predominant therapeutic emphasis or to use a psychodynamic-oriented focus, depending on the patient’s needs. This approach, known as the choice of rein, constitutes an integrated therapy in which each phase is characterised by a prevailing therapeutic orientation (e.g. CBT or psychodynamic), rather than distinct or separate treatments.
For example, in the FBIM model, cognitive-behavioural modality interventions typically focus on psychoeducation, identification of automatic thoughts, cognitive restructuring or process-based interventions, gradual exposure, behavioural activation, problem-solving training, and relapse prevention. In contrast, intensive short-term dynamic psychotherapy interventions may include clarification, challenging defences, emotional engagement, confronting resistance, emotional breakthroughs, linking emotions to past relationships, reintegration, and reflection.
FBIM therapists also act as intermediaries between the patient’s dysfunctional patterns and their internal resources, helping them resolve internal conflicts and move toward a more constructive and adaptive perspective. The ultimate goal for patients is to develop new tools to manage their symptoms and gain insight into the intrapsychic motivations that have interfered with their lives and the fulfilment of their needs.
A central concept in this evolution has been the Therapeutic Alliance (TA), initially discussed by Freud (1937, 1964) and later formalized by Sterba (1934), Greenson (1965), and Bordin (1979), who defined the Working Alliance (WA) as a combination of emotional bond, agreement on goals, and consensus on tasks—factors consistently linked to therapy success (Flückiger et al., 2018). In this study, the WA is conceptualized in line with Bordin’s (1979) tripartite model, which defines the alliance through three interrelated components: the emotional bond between client and therapist (Bond), agreement on therapeutic objectives (Goals), and consensus on the tasks needed to achieve those objectives (Tasks). This framework guided both the theoretical orientation of the study and the choice of measurement (Working Alliance Inventory—Short Form, WAI-SF). Inside the flexible structure of FBIM, a strong WA is considered crucial, especially in brief or time-limited formats (Gislon & Zapparoli, 2000).
While research on integrated psychotherapy is growing, most studies have emphasized overall efficacy rather than the mechanisms through which it works, including the role of a specific factors and their evolution over time (Zapparoli, 1999). Although the general efficacy of the FBIM has been supported by prior studies, less attention has been paid to the longitudinal dynamics of the WA within this integrated framework. In particular, it remains unclear how the WA evolves over time and how it interacts with clients’ baseline characteristics—such as motivation, resistance, and diagnostic profile—to shape therapeutic outcomes. While some research has explored these aspects in FBIM (Beutler et al., 2012; Feldman & Feldman, 2005; Gislon et al., 2023; Miscioscia et al., 2018), the interplay between WA, symptom reduction, and patient engagement across different treatment phases remains largely unexplored. Moreover, despite robust and consistent findings showing that WA is a strong predictor of outcomes across therapeutic modalities (Baldwin et al., 2007; Crits-Christoph et al., 2011; Zuroff & Blatt, 2006), it is still important to examine how this relationship manifests in specific therapeutic contexts. FBIM introduces structural and procedural elements—such as phase specific therapeutic orientation and intentional shifts in therapeutic strategy—that may pose unique challenges to the development and maintenance of WA. These transitions, while clinically valuable, could moderate the alliance-outcome relationship, especially for clients with complex or ambivalent presentations.
Investigating WA within the FBIM framework therefore offers a valuable opportunity to move beyond general associations and toward a more nuanced understanding of process-outcome dynamics. This study aims to fill that gap by examining how WA develops over time, how it interacts with client characteristics, and how it contributes to long-term outcomes. These insights are essential not only for advancing clinical theory but also for optimizing the implementation of integrated models like FBIM in real-world practice.
Objectives
The aims of the study were as follows:
1. To longitudinally assess the influence of the Working Alliance (WA) on therapeutic outcomes: Conducted in a community-based psychotherapy centre, the study investigated how changes in the quality of the WA, measured at multiple critical time points—before the initial consultation (T0), after 3 months (T1), at the end of therapy (approximately 12 months, T2), and during follow-up at 3 months (T3)—relate to therapeutic progress, symptom improvement, and sustained clinical outcomes over time. “Long-term outcomes” in this context refer to symptom levels and alliance quality assessed at post-treatment follow-up. The explicit focus was on understanding the role and dynamics of WA throughout therapy, rather than confirming the general effectiveness of FBIM, which has already been established in prior literature (Gislon et al., 2023).
2. To examine interactions between client baseline characteristics, Working Alliance, and clinical outcomes: The study explored how clients’ initial characteristics (e.g. diagnosis, motivation, resilience, resistance to change, and therapeutic focus) interact longitudinally with variations in WA and influence the trajectory of therapeutic outcomes. The aim was to clarify whether and how the initial clinical profiles of clients moderate the strength and therapeutic role of the WA over time. Since FBIM flexibly integrates both CBT and psychodynamic techniques, the analysis also considered how the predominant therapeutic orientation (CBT or psychodynamic oriented) within the integrated treatment may moderate these associations.
Methods
Ethical Issues
The research involving human participants was reviewed and approved by the Ethics Committee for Research in Psychology (Commissione Etica per la Ricerca in Psicologia, CERPS) at Università Cattolica del Sacro Cuore in Milan, Italy, on October 14, 2022 (protocol number: 47-22). All participants provided written informed consent to participate in the study.
Study Design
The present study utilized a longitudinal observational design with three primary data collection points: baseline (T0), 3 months (T1), and 12 months (T2), along with a follow-up assessment scheduled for 3 months (T3) post-therapy. The study was conducted from April 2022 to July 2024 at the CRF Zapparoli Centre of the Istituto per lo studio e la Ricerca sui Disturbi Psichici (ISeRDiP). The checklist for Strengthening The Reporting of OBservational studies in Epidemiology (STROBE) (von Elm et al., 2008) was completed (Appendix S1).
Participants
Recruitment
For each new admission of a potential participant to the CRF Zapparoli Centre of the Istituto per lo studio e la Ricerca sui Disturbi Psichici (ISeRDiP), the researcher was informed by the referring psychotherapist so that he could proceed with the invitation to participate in the study. In addition, to facilitate the recruitment process, meetings were organised with the psychotherapists involved in the clients’ treatment pathways to outline the characteristics and objectives of the project and to emphasise the importance of long-term participation in follow-up activities.
Inclusion and Exclusion Criteria
Children aged 13 years or older and whose parents gave Informed Consent and adults who were able to provide Informed Consent and who were referred by psychotherapists for an FBIM pathway at the CRF Zapparoli Centre of the Institute for the Study and Research on Mental Disorders (ISeRDiP) were eligible to participate in the study. Clients who accessed the Centre for other reasons such as, for example, Specific Learning Disorders (SLD) assessments; parenting support; participants with severe cognitive impairment or oppositional behaviour were not considered eligible.
Study Size
Based on the sample size analysis, the study required between 123 participants (statistical power = 0.80; non-centrality parameter = 18.45; α = .05; 1−β = .80; F(111) = 1.87) and 178 participants (statistical power = 0.95; non-centrality parameter = 26.70; α = .05; 1−β = .95; F(166) = 1.84) to detect a two-tailed difference. The ISeRDiP Centre admitted an average of 100 new clients annually, and we aimed to recruit from a minimum of 125 up to 180 participants. To ensure the feasibility of reaching this sample size, we involved an additional 10–20 external collaborators who had previously trained at ISeRDiP and used the integrated brief focal psychotherapy model. Each collaborator was able to refer at least 5–10 clients.
Procedures
Following presentation of the information sheet and signing of the Informed Consent Form, participants who agreed to take part in the study completed a sociodemographic questionnaire and two self-report measures either on paper or online using Qualtrics software (Qualtrics®, Provo, UT, USA; https://www.qualtrics.com), depending on their preference, and two questionnaires. Participants under 18 years of age completed the measures independently, after obtaining informed consent from their parent or legal guardian; parents did not participate in the assessment process.
Data collection was structured across four timepoints: baseline (T0), 3 months after therapy start (T1), end of therapy (~12 months; T2), and 3-month follow-up post-therapy (T3). Symptom measures were collected at T0, T1, T2, and T3, while the Working Alliance Inventory—Short Form (WAI-SF) was collected at T1 and T2. Both clients and therapists completed the WAI separately and independently.
At T1 and T2, therapists also completed a clinical form including data on the client’s diagnosis (ICD-10), therapeutic focus, developmental potential, underlying fears, resistance to change, resilience, use of medication, and other relevant variables. These therapist-reported variables were later included in the analyses exploring the interaction between client characteristics and alliance development.
Due to natural variations in therapy duration, some participants had not yet reached later timepoints (T2 or T3) by the end of data collection. Others completed therapy but did not return for the follow-up assessment (T3).
Measures
– Sociodemographic data: This information included gender, date of birth, level of education, type of employment/occupation, marital status, presence of children (if any, how many and their ages), and cohabitation status. Participants were also asked about the reasons for their current consultation and whether they had previously received any other psychological, psychotherapeutic or psychiatric treatment, including the type of approach used if possible, and any medication they were taking. The estimated time to complete these questions was approximately 5 min.
– Symptom checklist-90-R (SCL-90-R) (Prunas et al., 2012), designed to assess various psychological characteristics, including Somatization (SOM), Obsessive-Compulsive (O-C), Interpersonal Sensitivity (I-S), Depression (DEP), Anxiety (ANX), Hostility (HOS), Phobic Anxiety (PHOB), Paranoid Ideation (PAR), and Psychoticism (PSY). It also includes three global indices: Global Severity Index (GSI), which serves as a comprehensive indicator of the current intensity of psychological distress perceived by the individual; Positive Symptom Total (PST), reflecting the number of symptoms reported; and Positive Symptom Distress Index (PSDI), which measures the individual’s response style. The questionnaire comprises 90 items and typically requires approximately 12 min to complete.
– Working Alliance Inventory—Short form revised (WAI-SF): The current study employed a revised 12-item version (Hatcher & Gillaspy, 2006), derived from the Working Alliance Inventory (WAI) (Busseri & Tyler, 2003; Hatcher & Gillaspy, 2006; Lo Coco et al., 2011). Items are rated on a 7-point Likert scale, yielding a total score from 12 to 84, with higher scores indicating a stronger alliance. It was translated into Italian for clients (WAI-P) and staff (WAI-T) (Lingiardi, 2002). Both clients and therapists completed the WAI. Analyses were conducted separately on the two perspectives.
In addition to client self-report measures, therapists completed a clinical rating form at T1 and T2, including data on diagnosis (ICD-10), therapeutic focus, developmental potential, underlying fears, motivation, resilience, security system, and resistance to change. These variables were collected for research purposes and included in the analyses examining predictors of alliance and outcome trajectories.
Time
The SCL-90-R (crf. par. 2.4.1) was administered to participants before the first consultation (T0), during psychotherapy (T1), at the end of the therapy process (T2), and during follow-up (T3), totalling four assessments, while the WAI was completed at T1 and T2. At the same time, the psychotherapist was asked to complete the WAI either online or on paper, according to his or her preference, during psychotherapy (T1) and at the end of the therapy process (T2).
Setting
Data were collected at the CRF Zapparoli Centre, part of ISeRDiP, a community-based outpatient psychotherapy centre located in Milan, Italy. The centre provides short- and medium-term integrated psychotherapy services based on the FBIM, combining psychodynamic and cognitive-behavioural approaches. Clients are referred for a range of psychological and psychiatric issues, including emotional distress, anxiety, depression, relational difficulties, and adjustment problems. Services are provided by licensed psychotherapists trained in the FBIM approach, and are tailored to both adolescents and adults, depending on clinical need. The centre also engages in clinical research, training, and supervision. The assessment was administered in a suitable setting, free from distractions. If the participant preferred an online format, a dedicated computer and/or tablet was made available at the centre to ensure they could still ask questions about unclear content and provide reliable responses. It is important to note that the client and psychotherapist were not informed of each other’s participation in the project.
Treatment
The FBIM framework integrates three theoretical perspectives: developmental, psychodynamic, and cognitive models. Each contributes to functional diagnosis, treatment design, and implementation, either individually or in combination, depending on client needs. These models provide unique insights into human behaviour, including the origins of adaptive and maladaptive patterns, their persistence, and mechanisms for change (Gislon, 2005).
All participants received treatment under the same protocol: the Focus-Based Integrated Model (FBIM). This is not a comparative trial between CBT and psychodynamic therapy, but an integrative approach where different techniques are employed flexibly across treatment phases depending on client needs. For analytical purposes, the predominant therapeutic orientation employed in each phase was labelled as CBT or psychodynamic, reflecting the emphasis rather than distinct treatment conditions. This designation was determined retrospectively by the treating therapist, who coded the prevailing orientation applied during each participant’s treatment within the FBIM framework. Therapy setting (in-person vs. online modality) was also recorded for each participant as part of the baseline assessment. In therapy, “focus” (Box 1, Supplementary Material 1) refers to identifying the primary psychological issue underlying distress, serving as the entry point for change. Establishing this focus helps prioritize interventions to break dysfunctional cycles and restore the client’s strengths. While motivated clients may desire change, they often struggle to implement it effectively (Gislon, 2005; Gislon & Zapparoli, 2000). The Security System, encompassing internal and external mechanisms for addressing needs while managing fear and frustration (Figure 1), provides diagnostic insights into resistance to change, present from the first session (Figure 2).
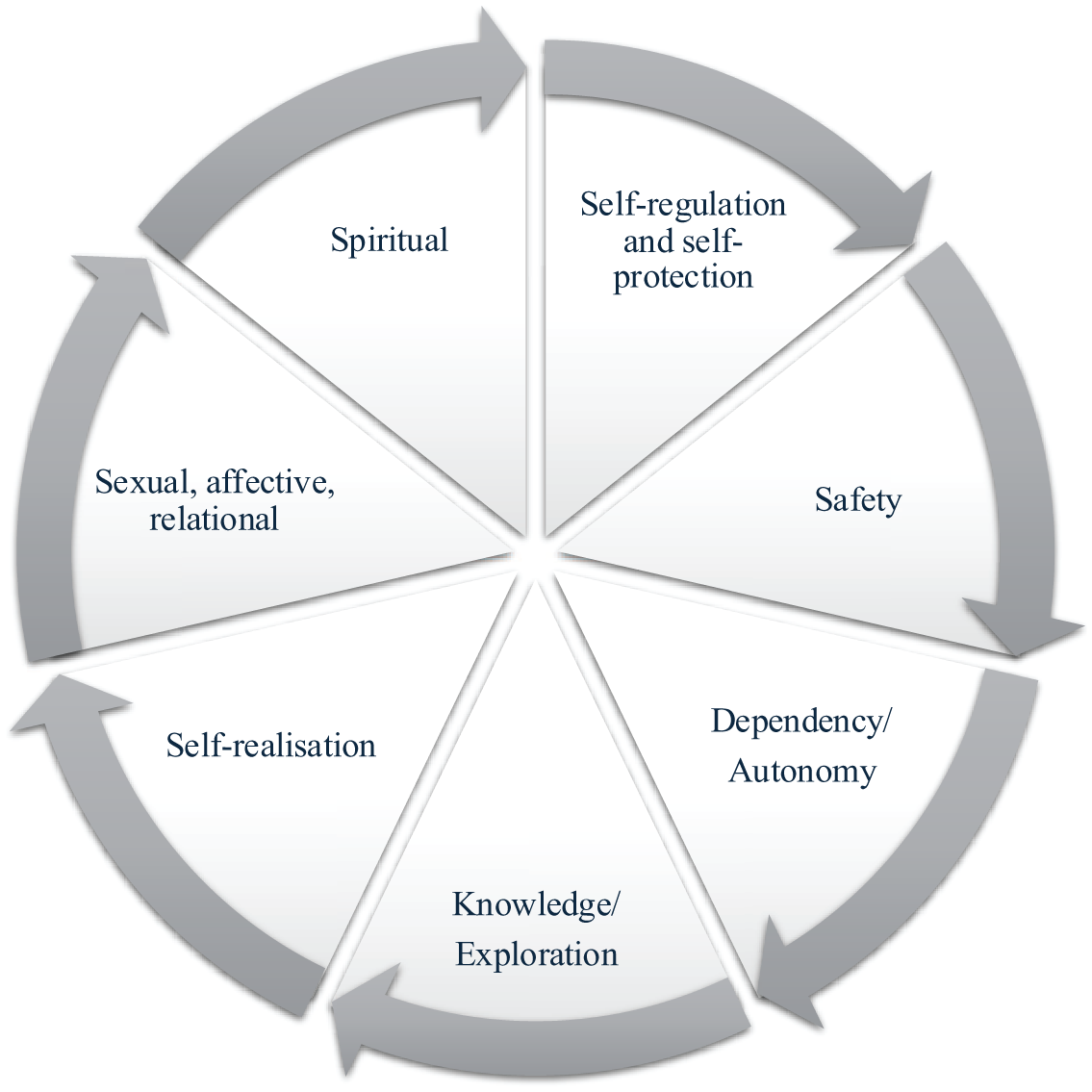
Main areas of specific needs as conceptualized in the Focus-Based Integrated Model (FBIM).
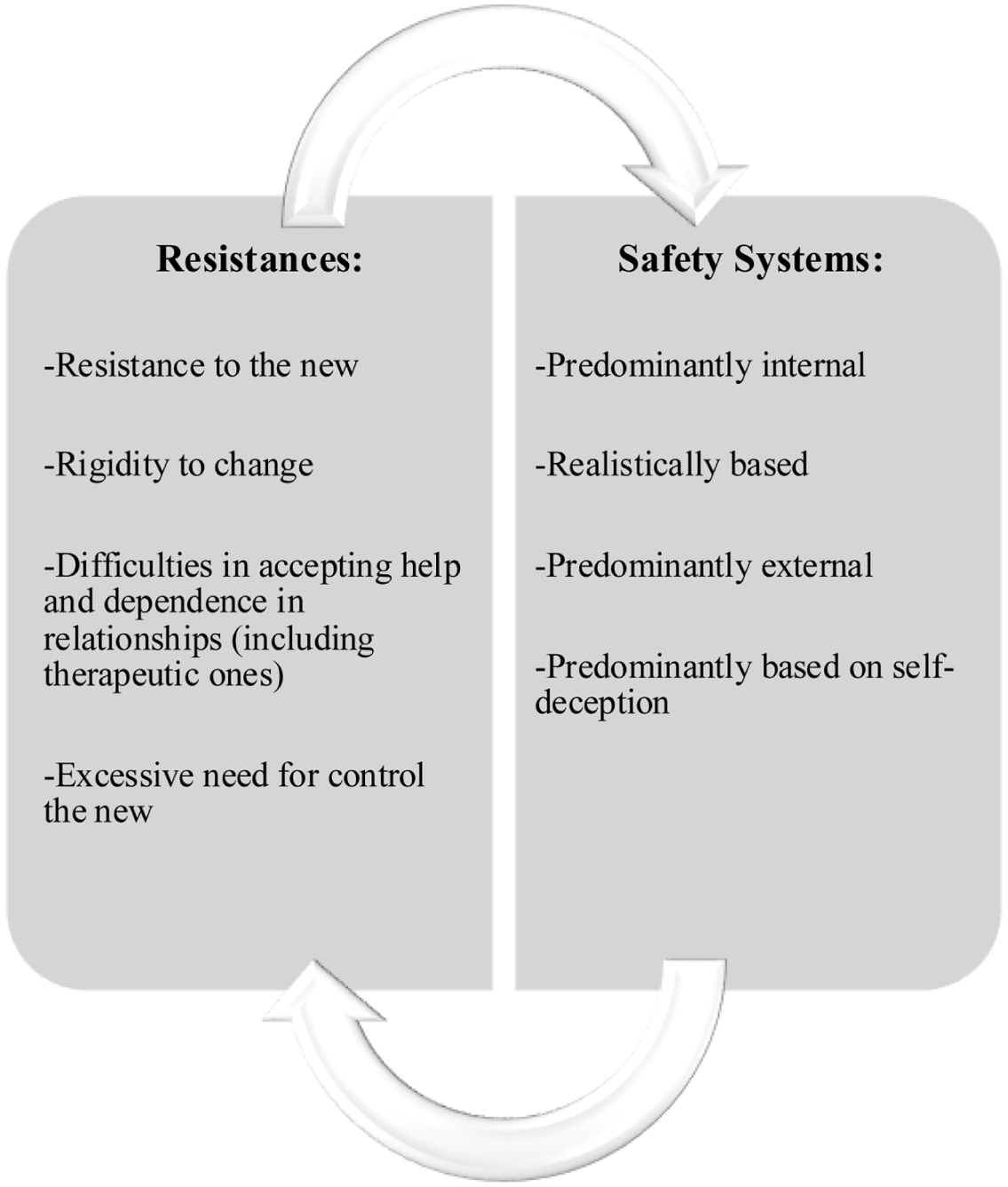
Resistance to change and the security system according to the Focus-Based Integrated Model (FBIM).
“Brief” therapy emphasizes balancing time and effectiveness. Modern life often hinders self-care, and the model leverages clients’ internal resources to regain balance. Brevity is not a limitation but a strategic approach enabling clients to confront distress and overcome obstacles (Gislon, 2005; Gislon & Zapparoli, 2000; Zapparoli, 1999). This approach views clients within ongoing development, addressing past barriers to resume growth. When conditions allow, therapy identifies and removes obstacles, empowering clients to become self-reliant. The primary goal is fostering continuous growth, equipping clients to handle both current and future challenges effectively.
All participants received treatment according to the Focus-Based Integrated Model (FBIM), which integrates cognitive-behavioural and psychodynamic techniques. The relative emphasis on each modality varied across clients and treatment phases, depending on the evolving therapeutic focus. Thus, any reference to “CBT” or “psychodynamic” in the results reflects the phase-specific therapeutic orientation within the integrated treatment, not distinct treatment conditions.
Statistical Analysis
Initial data analysis was descriptive in nature. For continuous variables, means and standard deviations (SDs) were provided; for categorical variables, data were expressed as integers and percentages. Both clients and therapists completed the WAI. Analyses were conducted separately on the two perspectives. Both clients and therapists completed the WAI. Analyses were conducted separately on the two perspectives.
The selection of variables and analyses was directly informed by the two main aims of the study. To address the first aim, repeated-measures ANOVAs were performed to assess changes in symptom severity and WAI-SF scores across the five time points: T0, T1, T2, and T3. These analyses aimed to identify significant trends in therapeutic progress and long-term outcomes. Post hoc pairwise comparisons with Bonferroni correction were applied to explore specific differences between time points.
For the second aim of the study, we investigated whether baseline characteristics (e.g. diagnosis, motivation for change, resilience, resistance, and therapeutic focus) were associated with variations in WA and symptom profiles. To this end, MANOVAs were conducted separately at T1 and T2 to examine the cross-sectional associations between these baseline variables and the WAI-SF subscales (bond, goal, and task), from both client and therapist perspectives. Although the results are presented across multiple time points to illustrate change, the MANOVAs themselves were not repeated-measures analyses. Repeated-measures ANOVAs, instead, were used exclusively to assess within-subject changes in symptom severity (SCL-90-R) and WAI-SF scores across time points (T0, T1, T2, and T3), with post hoc Bonferroni-corrected comparisons applied as needed.
Effect sizes (e.g. partial eta squared) were reported to quantify the magnitude of observed effects. Assumptions of normality, sphericity, and homogeneity of variances were tested, with Greenhouse-Geisser corrections applied when sphericity was violated. Statistical significance was set at p < .05. All analyses were conducted using Jamovi software (version 2.8.38).
Results
The Sample
Out of an initial pool of 245 potential participants, 154 participants took part to the study and completed the questionnaires at baseline (T0), 129 participants (83.8%) completed the first follow-up (T1). At this point, 22 participants had dropped out, and 3 were still in therapy but had not yet reached the 3-month mark by the time data collection ended. At the final follow-up (T3), data were available for eight participants. Although only one participant dropped out between T2 and T3, the majority (52) completed therapy but did not return for the 3-month post-treatment follow-up, and 32 were still engaged in ongoing therapy (Figure 3).
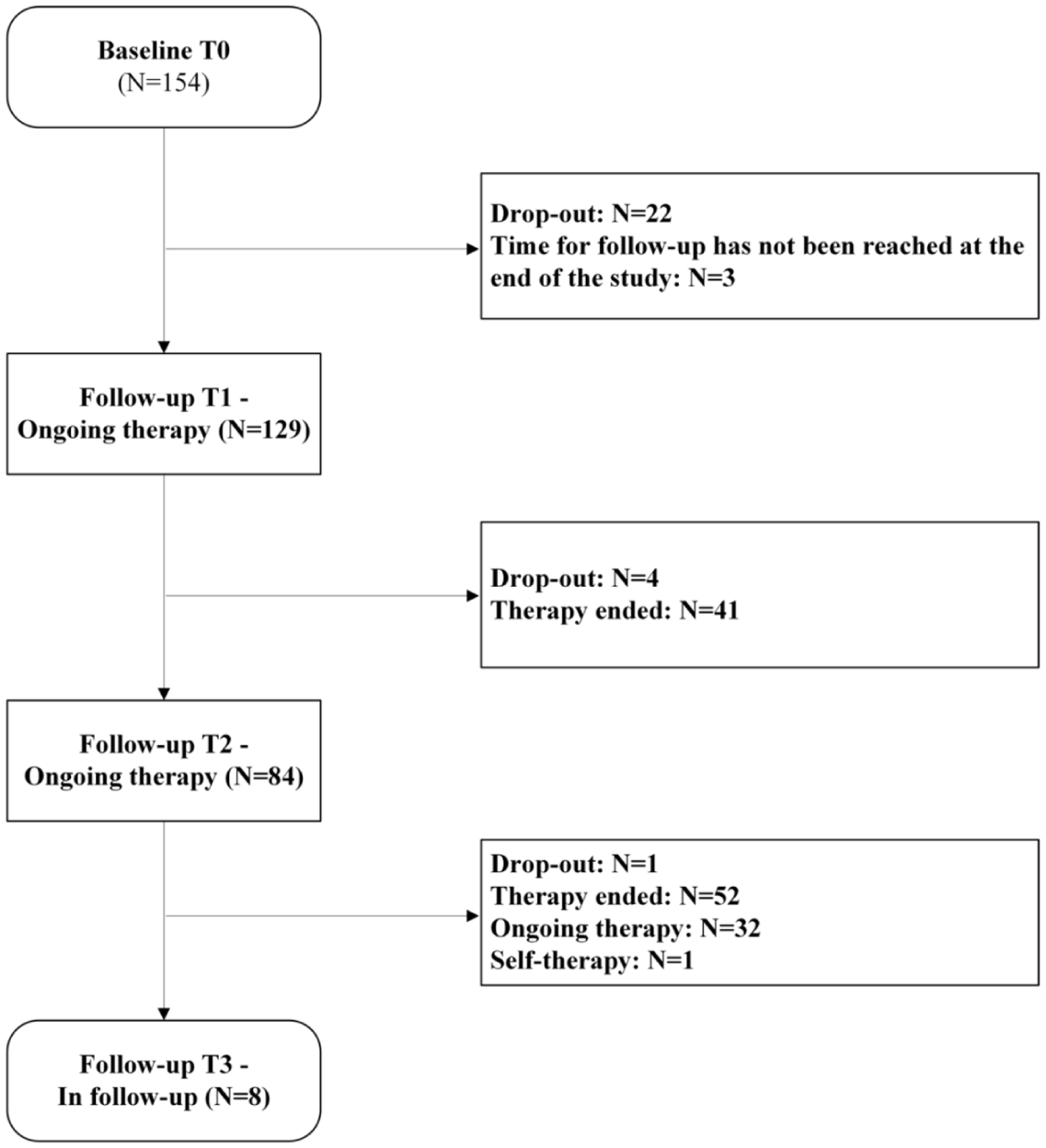
Flowchart of the client inclusion and participation process.
The participants, all Italian, had an average age of 32.8 years (SD = 10.9; range 14–69), with the majority being female (N = 82; 54.3%). Only 4 participants (2.59%; 3 attending high school and 1 at the end of junior high school) were under the age of 18. A comprehensive overview of the sample’s socio-demographic characteristics is provided in Table 1.
Socio-Demographic Characteristics of the Sample.
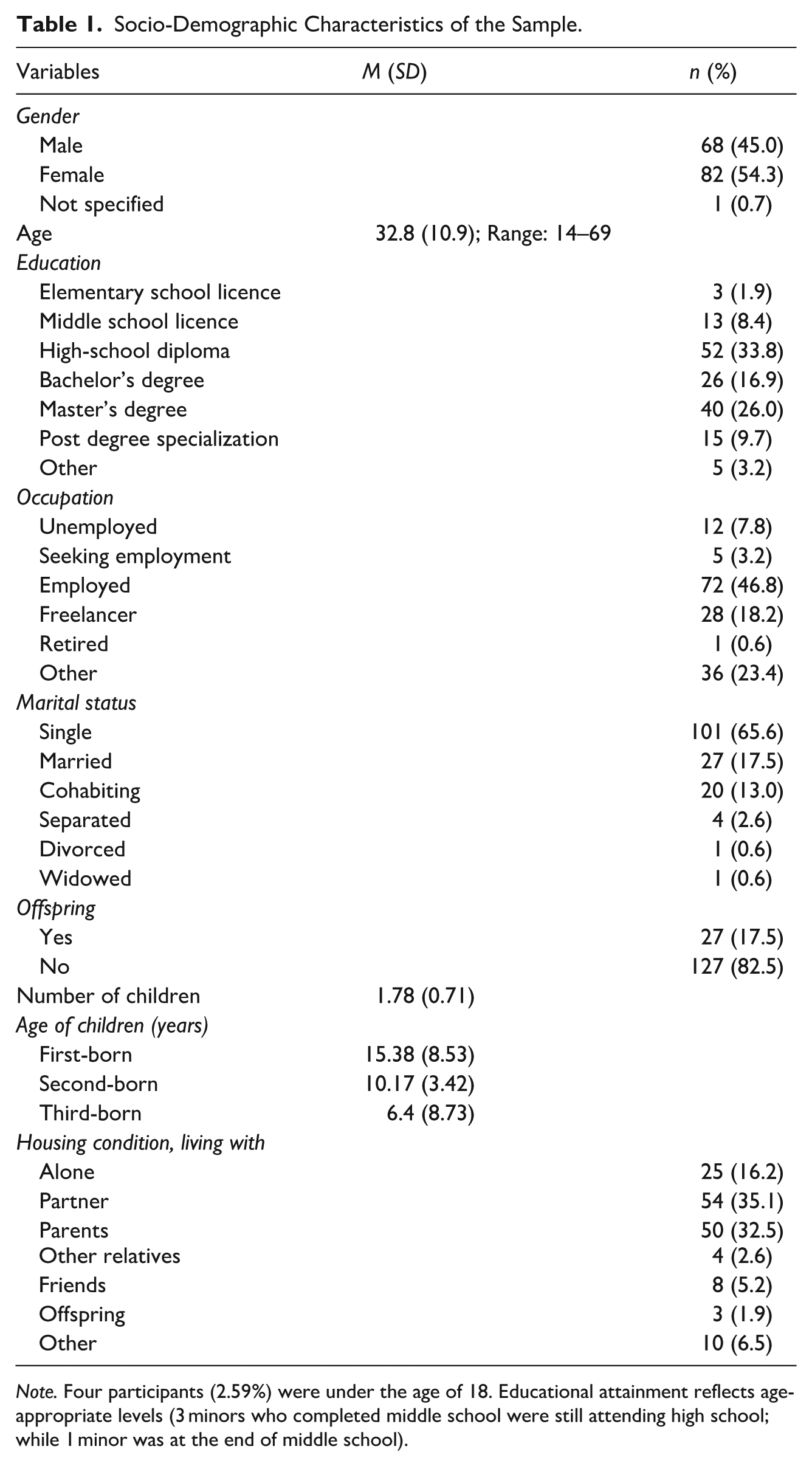
Note. Four participants (2.59%) were under the age of 18. Educational attainment reflects age-appropriate levels (3 minors who completed middle school were still attending high school; while 1 minor was at the end of middle school).
Of the study participants, 37.9% (N = 58) had never sought contact with psychologists, psychotherapists, or psychiatrists before attending the Centre. This was followed by 33.3% (N = 51) who had accessed psychological services more than 12 months prior to this new contact. Most participants were not taking any medication at the time of entry (N = 118; 76.6%). As shown in Table 2 (Supplementary Material 2), the primary reasons for seeking services were predominantly related to managing emotional experiences (N = 74; 48.4%).
Summary of the Results of the Repeated Measures ANOVA for Key Variables Over Time and in Interaction with the WAI-SF Scale.
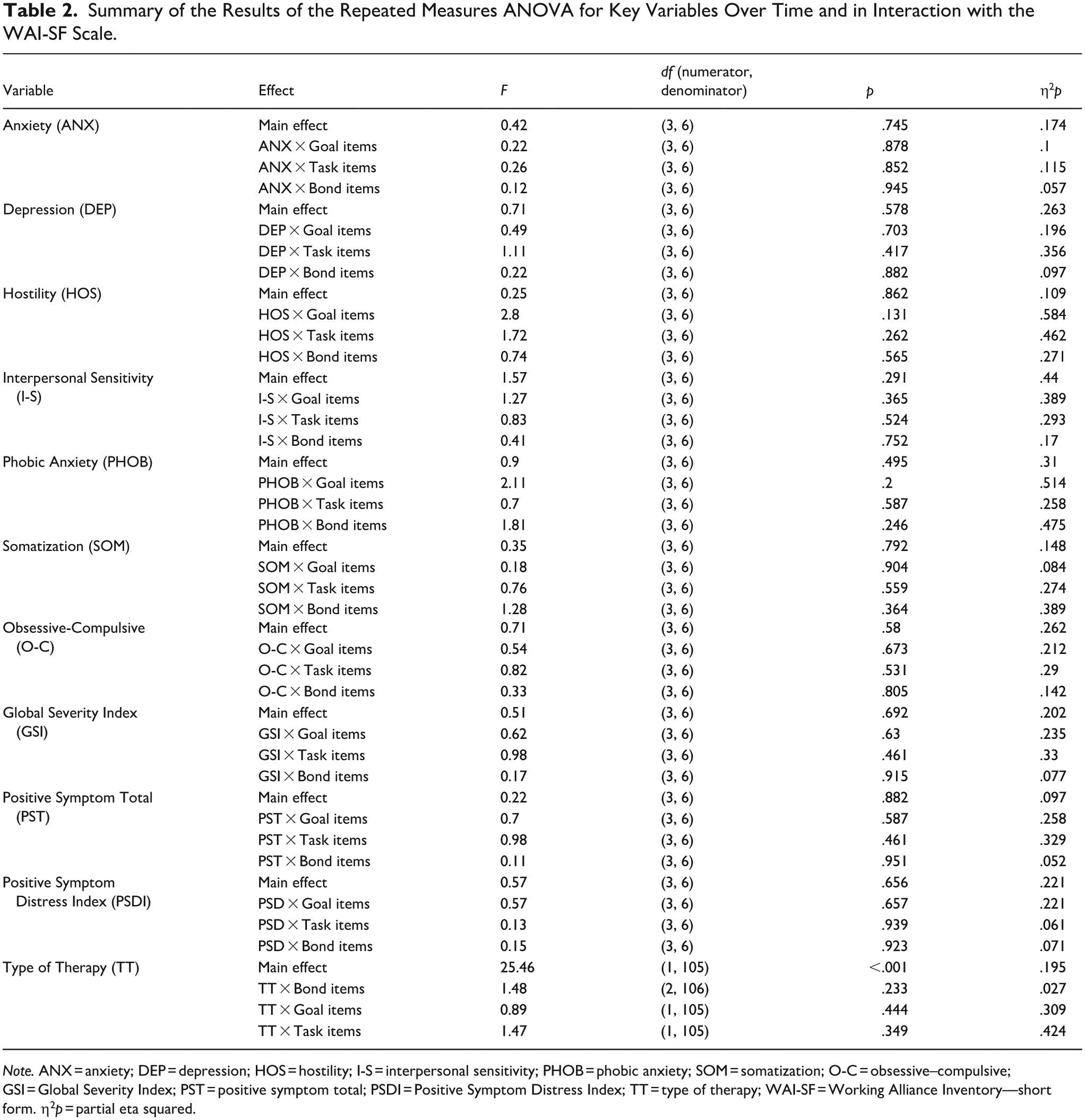
Note. ANX = anxiety; DEP = depression; HOS = hostility; I-S = interpersonal sensitivity; PHOB = phobic anxiety; SOM = somatization; O-C = obsessive–compulsive; GSI = Global Severity Index; PST = positive symptom total; PSDI = Positive Symptom Distress Index; TT = type of therapy; WAI-SF = Working Alliance Inventory—short form. η2p = partial eta squared.
Table 3 (Supplementary Material 3) presents the clinical characteristics of the sample at T1, T2, and T3, highlighting any significant changes over time, while Table 4 (Supplementary Material 4) summarizes the key characteristics of the sample at the end of therapy, providing a snapshot of the clinical status following treatment completion. The most frequent diagnostic categories included depressive episodes (F32), anxiety-related disorders (F41), and adjustment disorders (F43), although several other diagnoses were represented at lower frequencies (Table 3, Supplementary Material 3). Full ICD-10 codes are reported for transparency. Due to the limited sample size at T3 (N = 8), these results are reported for descriptive purposes only and should be interpreted with caution.
Main Results of MANOVAs Performed Considering the Impact of Client Characteristics on Clients’ Development of WA.
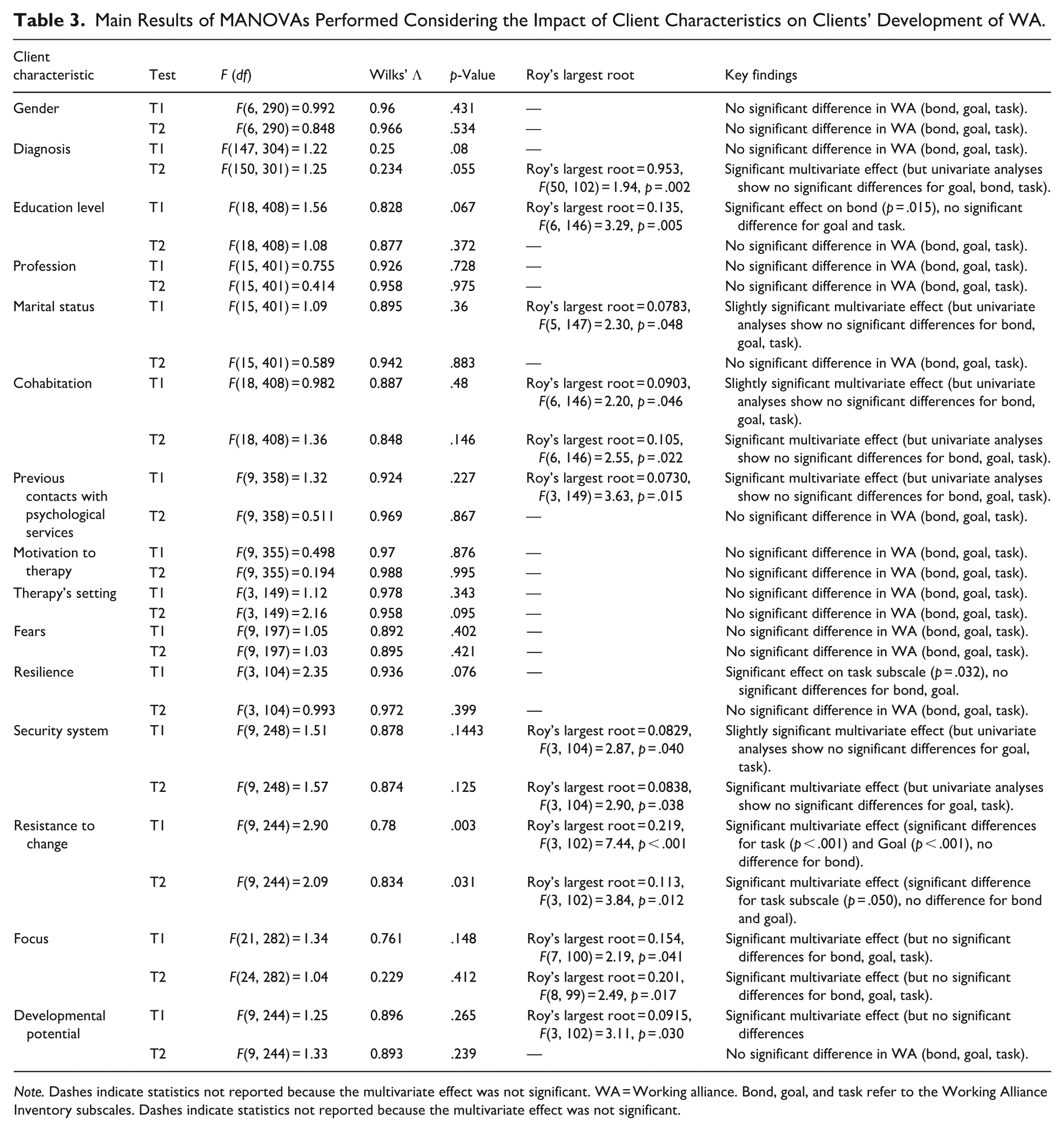
Note. Dashes indicate statistics not reported because the multivariate effect was not significant. WA = Working alliance. Bond, goal, and task refer to the Working Alliance Inventory subscales. Dashes indicate statistics not reported because the multivariate effect was not significant.
Main Results of MANOVAs Performed Considering the Impact of Client Characteristics on Therapists’ Perception of WA.
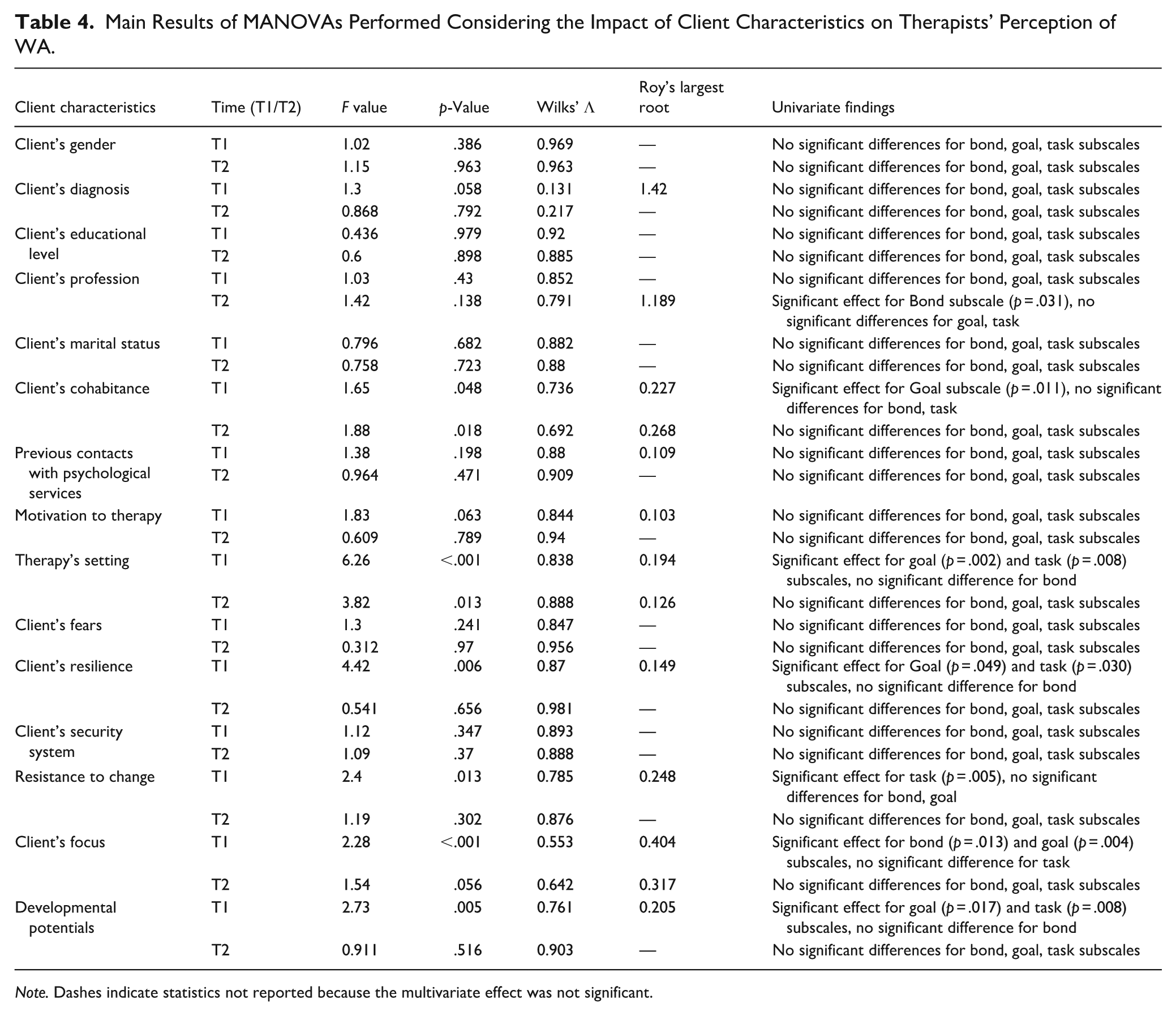
Note. Dashes indicate statistics not reported because the multivariate effect was not significant.
In line with the study aims, the Results are presented in two sections: first, the longitudinal analyses of changes in WA and symptom severity across therapy and follow-up (Aim 1); and second, the associations between baseline client characteristics, predominant therapeutic orientation, and WA dimensions at different time points (Aim 2).
Stability of Symptoms and Alliance Across Time
Overall, repeated-measures ANOVAs revealed that most symptom dimensions (e.g. ANX, DEP, HOS, PSDI) remained stable across the examined time points, and their interactions with WA dimensions were non-significant, with consistently small effect sizes (partial η2p). This indicates that, in the short-to-medium term, symptom reduction and alliance processes tended to evolve relatively independently.
By contrast, a robust main effect emerged for the predominant therapeutic orientation, F(1, 105) = 25.46, p < .001, η2p = .195, showing that CBT-oriented treatments were associated with higher alliance ratings across time compared to psychodynamic-oriented treatments. This represents one of the strongest and most consistent findings of the study, underscoring that the therapeutic focus substantially shaped the development of the alliance over time (Table 2). Importantly, this main effect was not moderated by the specific WA dimensions (bond, task, goal), suggesting that CBT emphasis exerted a general advantage on alliance ratings rather than selectively enhancing a single subcomponent. To further disentangle this general effect, post hoc comparisons were conducted, which revealed specific differences on the Task subscale at T2.
Specifically, Task items at T2 for the FBIM were significantly higher than for the Cognitive Behavioural Therapy (CBT)-predominantly oriented (Mean Difference = 6.904, SE = 1.590, t(104) = 4.343, p < .001) and the Psychodynamic Therapy-predominantly oriented (Mean difference = 6.428, SE = 1.553, t(104) = 4.140, p < .001). Similarly, Task items at T2 for the Psychodynamic Therapy-predominant therapeutic emphasis were significantly lower than those for the CBT-predominant therapeutic emphasis (Mean difference = 7.643, SE = 2.004, t(104) = 3.814, p = .003). In contrast, no significant differences were found between therapy types for Task items at T1 or other pairwise comparisons involving Task items at T2 after correction for multiple comparisons (Bonferroni-adjusted p > .05).
Taken together, these results highlight the relative stability of symptoms across therapy, alongside a clear and time-sensitive impact of therapeutic orientation on the Task component of alliance, with CBT emphasis showing the most consistent benefit by the end of treatment.
Influence of Clients’ and Therapists’ Characteristics on Alliance Development
How Client Characteristics Shape Their Own Perception of WA
Based on the longitudinal analyses, several client characteristics were examined in relation to their influence on the WA subscales—bond, goal, and task—at T1 and T2. None of the variables tested—gender, profession, marital status, cohabitation, therapy modality, fears, motivation to therapy, and previous psychological service contacts—showed significant effects on WA subscales at either T1 or T2.
Diagnosis showed an overall significant multivariate effect on WA (Roy’s largest root = 0.953, p = .002); however, univariate analyses indicated no significant differences for Bond, Goal, or Task subscales. Similarly, educational level had a significant multivariate effect at T1 (Roy’s largest root = 0.135, p = .005), primarily driven by differences in Bond (p = .015), but this effect did not persist at T2.
Resilience demonstrated a marginally significant effect on the Task subscale at T1 (p = .032) but no significant differences at T2. Client resistance to change yielded the most notable results, with significant multivariate effects at both T1 (Roy’s largest root = 0.219, p < .001) and T2 (Roy’s largest root = 0.113, p = .012). Univariate analyses revealed that this effect was primarily driven by significant differences in the Task and Goal subscales at T1 (p < .001) and the Task subscale at T2 (p = .050).
Other factors, including security system variables, showed a significant omnibus effect in the MANOVA, but the follow-up univariate analyses on the individual WAI subscales did not consistently reach significance (Table 3).
The Interplay Between Client’s Characteristics and the Therapist’s Perception of WA
MANOVA analyses were conducted to examine therapists’ perceptions of the WAI subscales (bond, goal, task) at T1 and T2 in relation to client characteristics. No significant differences emerged in WAI-SF subscale ratings based on gender [T1: F(3, 96) = 1.02, p = .386; Wilk’s Λ = 0.969; T2: F(3, 90) = 1.15, p = .963; Wilk’s Λ = 0.963], marital status [T1: F(15, 257) = 0.796, p = .682; Wilk’s Λ = 0.882, T2: F(15, 241) = 0.758, p = .723; Wilk’s Λ = 0.880], educational level [T1: F(18, 261) = 0.436, p = .979; Wilk’s Λ = 0.920; T2: F(18, 244) = 0.600, p = .898; Wilk’s Λ = 0.885], or previous psychological service use at either time point [T1: F(9, 231) = 1.38, p = .198; Wilk’s Λ = 0.880; T2: F(9, 217) = 0.964, p = .471; Wilk’s Λ = 0.909]. Similarly, client diagnosis didn’t show a significant multivariate effect at T1 and T2 [T1: F(126, 169) = 1.30, p = .058; Wilk’s Λ = 0.131; T2: F(120, 157) = 0.868, p = .792; Wilk’s Λ = 0.217]. Cohabitance showed a significant omnibus effect in the MANOVA at both T1 and T2; however, the follow-up univariate analyses indicated that this effect was not consistently significant across the WAI-SF subscales. Client profession significantly influenced perceptions of the bond subscale at T2 [F(5, 681) = 2.59, p = .031].
At T1, no statistically significant differences were observed in therapists’ WAI subscale ratings—bond, goal, and task—based on clients’ motivation to therapy, F(9, 229) = 1.83, p = .063; Wilk’s Λ = 0.844. However, the overall multivariate effect of “motivation to therapy” was supported by Roy’s largest root, suggesting a significant influence on the combined dependent variables, [Roy’s largest root = 0.103, F(3, 96) = 3.29, p = .024]. Despite this multivariate effect, univariate analyses revealed nonsignificant differences for the individual WAI subscales (bond, goal, and task), indicating that the overall effect was not driven by specific alliance dimensions. At T2, no statistically significant differences were found in WAI subscale ratings based on client motivation, F(9, 214) = 0.609, p = .789; Wilk’s Λ = 0.940, indicating no sustained effect over time.
Therapists’ WA ratings at T1—comprising bond, goal, and task—varied significantly based on clients’ resistance to change, F(9, 207) = 2.40, p = .013; Wilk’s Λ = 0.785. This multivariate effect was further supported by Roy’s largest root, indicating a significant influence on the combined alliance dimensions [Roy’s largest root = 0.248, F(3, 87) = 7.19, p < .001]. Univariate analyses showed that the effect was primarily driven by significant differences in the Task subscale, F(3, 59) = 4.66, p = .005, with no significant differences observed for the Bond or Goal subscales. At T2, no statistically significant differences in WA ratings were found based on resistance to change, F(9, 192) = 1.19, p = .302; Wilk’s Λ = 0.876. At T1, therapists’ WAI ratings—bond, goal, and task—differed significantly based on the therapy modality (online modality vs. in-person modality), F(3, 97) = 6.26, p < .001; Wilk’s Λ = 0.838. The overall multivariate effect of “therapy modality” was further supported by Roy’s largest root, indicating a significant influence on the combined dependent variables, [Roy’s largest root = 0.194, F(3, 97) = 6.26, p < .001]. Univariate analyses demonstrated that this effect was driven by significant differences in the Goal subscale, F(35, 35) = 10.56, p = .002, and the Task subscale, F(31.08, 31.08) = 7.26, p = .008, while no significant differences were observed for the Bond subscale.
At T2, a statistically significant difference in WAI-SF ratings was also identified based on the therapy modality, F(3, 91) = 3.82, p = .013; Wilk’s Λ = 0.888. The multivariate effect of “therapy modality” was supported by Roy’s largest root, indicating a significant impact on the combined dependent variables, [Roy’s largest root = 0.126, F(3, 91) = 3.82, p = .013]. However, univariate analyses revealed no significant differences across the Bond, Goal, or Task subscales, suggesting that the effect was not attributable to specific alliance dimensions at T2. Together, these findings indicate that therapists’ perceptions of the alliance are sensitive to specific client factors (resistance to change, therapy modality), while other characteristics show little or no consistent impact. This underscores the importance of contextual and motivational elements in shaping therapist–client alliance dynamics (Table 4).
Discussion
The alliance’s potential for therapeutic benefit is a contentious theory. While many researchers and theorists regard the alliance to be therapeutic in and of itself, others see it as a by-product of successful therapy or as a general feature that makes the genuinely effective components of treatment function (Zilcha-Mano, 2017). This study represents one of the few in the existing literature that investigates the implementation of FBIM, with a particular focus on assessing symptom changes at key time points. This longitudinal design allows for a comprehensive understanding of both the therapeutic progress and the long-term outcomes of the intervention.
A central aspect of this study was the examination of the WA, tracking improvements in alliance quality and initial symptom severity over time. Additionally, the study aimed to explore how symptom profiles evolved in relation to the development of the therapeutic alliance throughout the therapeutic process. Within the FBIM framework, the WA is considered a central mechanism of change, but the present findings also show that its effectiveness is shaped by the therapeutic orientation and by contextual factors such as therapy modality. This underscores the flexibility of FBIM as a model that integrates different approaches to meet clients’ needs, while also highlighting possible limits of specific orientations when assessed over short-to-medium time frames.
In particular, no significant changes in symptomatology were detected through the administration of the SCL-90-R in relation to the WA, suggesting that alliance-related processes may evolve somewhat independently of symptom reduction in the short-to-medium term. However, the prevailing therapeutic focus within the FBIM (CBT- or psychodynamic-oriented) seems to play a critical role in shaping the development of the alliance. The repeated-measures ANOVA revealed that, within the FBIM framework, therapies with a predominant CBT orientation showed significantly higher scores on the Task subscale of the WAI at T2 compared to those with a predominant psychodynamic orientation. This suggests that CBT-predominant therapeutic emphasis may have had a more immediate or stronger impact on task performance at the second time point. This difference could be attributed to the structured nature of CBT, which focuses on modifying thoughts and behaviours, potentially leading to more rapid improvements in task-related performance. Another possible explanation for this better performance concerns a specific variable of the FBIM model: the choice of the rein. In the approach to therapy, the choice of the cognitive rein is not random but is made because of the best indication for that specific patient. The choice of to prioritize a CBT-predominant therapeutic emphasis rather than a psychodynamic-oriented one, based on the patient’s characteristics and clinical needs, arises precisely from the need to favour alliance and brevity and this could be the reason for a better performance on the Task subscale of the WAI-SF. In contrast, psychodynamic-predominant emphasis did not show measurable improvements within the study timeframe, suggesting either that its effects may require longer treatment durations to emerge, or that they are less readily captured by WA subscales focusing on tasks and goals. However, the absence of significant differences between the Psychodynamic approach and the other predominant orientations at Task subscale of WA at T2 could imply that the effects of Psychodynamic-oriented therapy on task performance were more subtle or that its therapeutic mechanisms did not translate as clearly into the task performance outcomes within the study period. Moreover, while CBT-predominant therapeutic emphasis appeared to show a more marked impact, further research may be needed to explore the underlying mechanisms and longer-term effects of each therapy type on WA. Moreover, although the interactions between the rein and the specific WA dimensions were not significant, the presence of a main effect of therapy predominant rein suggests that these orientations may shape outcomes independently of these subcomponents. This pattern points to a relative stability of psychological symptoms and alliance factors across time, while underscoring the importance of considering the overall therapeutic approach when evaluating treatment progress.
The statistically significant influence of clients’ resistance to change on WA at T1, particularly the Task subscale, highlights that early in therapy, resistance may primarily affect the collaborative and goal-oriented aspects of the therapeutic process. This finding aligns with theoretical frameworks suggesting that resistance to change can hinder mutual agreement on tasks and active participation in therapy. On the contrary, the absence of significant effects at T2 may suggest that, over time, resistance diminishes as the therapeutic relationship strengthens or as clients become more engaged in the process. This could indicate that therapists are effective in addressing resistance during therapy, underscoring the importance of therapeutic skills in managing resistance early on. These results appear to be consistent with research on alternative psychotherapy modalities that highlight how alliance strengthening was predicted by gradual reinforcement and repaired rupture patterns at the start of treatment, while alliance stability was predicted by the unrepaired rupture pattern at the start of treatment (Zilcha-Mano & Errázuriz, 2017). Overall, while client characteristics such as diagnosis, educational level, and resistance to change demonstrated some influence on WA, these effects were often limited to specific subscales or time points.
Moreover, the statistically significant differences in WA (both at T1 and T2) based on therapy modalities suggest that contextual factors significantly influence WA. This finding supports existing evidence that therapy modality (e.g. in-person vs. online) can impact the collaborative and goal-oriented dynamics of therapy (Hanley et al., 2017; Saxler et al., 2024). However, at T2, the lack of significant differences in the subscales suggests that as therapy progresses, the setting becomes less critical, potentially due to client and therapist adaptation to the environment. From a clinical perspective, this suggests that FBIM may be flexibly and effectively delivered in hybrid formats, with initial contextual differences diminishing once the alliance is consolidated.
The absence of significant differences in WA based on client motivation at both T1 and T2 was unexpected. These findings suggest that motivation, often viewed as a predictor of therapy engagement, operationalized as retention in treatment and follow-up (Franco, 2012; Ryan, 2012), may have a more complex or indirect relationship with WA. It is possible that motivation impacts WA only when combined with other variables, such as client-therapist matching or therapy modality. Alternatively, the lack of significance may indicate that therapists were skilled at engaging less motivated clients and fostering a strong alliance regardless of initial attitudes.
These results align in part with findings from other therapeutic orientations. For instance, in CBT-predominant therapeutic emphasis, the structured and transparent nature of treatment has been repeatedly associated with higher early ratings of the task dimension of the WA (Flückiger et al., 2018; Horvath & Symonds, 1991). This pattern was also observed in our study, where CBT-predominant therapeutic emphasis was associated with stronger task-related scores at the end of therapy. In contrast, psychodynamic-predominant therapeutics emphasis often emphasize the bond dimension and deeper relational processes, which may take longer to develop and are sometimes underrepresented in task-oriented metrics (Safran & Muran, 2006). Moreover, previous meta-analyses (Flückiger et al., 2018) have found that although alliance is a consistent predictor of outcome across modalities, the timing and weight of specific alliance components (bond, goal, task) may vary depending on the therapeutic model and phase. Our findings support this view by showing that alliance dimensions are not equally sensitive to all client or therapy variables, and their relevance may shift across treatment stages. Additionally, resistance to change—central in psychodynamic theory—has been linked to early alliance ruptures in several studies, and its resolution is considered a key mechanism for improving outcomes (Halfon, 2021; Zilcha-Mano & Errázuriz, 2017). The temporary influence of resistance observed in our study echoes this literature, suggesting that therapists may have actively worked through resistance during the early sessions, leading to more stable alliance ratings by the end of treatment.
Collectively, these findings highlight that WA is a dynamic construct influenced by client- and therapy-related factors differently across therapy stages. Resistance to change and therapy setting appear to impact WA early on, while client motivation does not show a direct influence in this study. By situating these dynamics within the FBIM framework, our findings suggest that while CBT-predominant emphasis may foster faster improvements on task-oriented dimensions, psychodynamic-predominant emphasis might require longer timeframes to reveal its strengths, particularly in relational aspects of the alliance. This underscores the need for a multidimensional approach to understanding WA, where specific variables may exert influence at different stages or in specific contexts (Table 8, Supplementary Material 5).
Strengths and Limitations
The study’s strengths include its longitudinal design, allowing for the observation of changes over time and capturing both immediate and long-term effects of integrated psychotherapy. The diverse participant recruitment enhances generalizability, while established psychometric assessments ensure reliable measurements of therapeutic alliance and symptom change. Additionally, the involvement of psychotherapists fosters practical understanding, and the emphasis on follow-up assessments provides insights into the sustainability of therapeutic outcomes. The study has also several limitations, including its reliance on self-reported measures, which may introduce biases such as social desirability or response distortion. Additionally, the relatively small sample size may affect the generalizability of the findings, limiting their applicability to broader populations. The study’s focus on a specific therapeutic approach might also restrict the understanding of integrated psychotherapy’s effectiveness across different modalities. Furthermore, the lack of control groups may hinder the ability to draw definitive causal conclusions regarding the observed changes in symptoms and therapeutic alliance. Finally, although the follow-up sample was small, the descriptive data at T3 may offer preliminary insights into the stability of clinical improvements after therapy conclusion. Future research with larger follow-up samples is needed to confirm these trends.
Clinical Implications
The clinical implications of this study are multifaceted and hold significant promise for enhancing therapeutic practice. Firstly, this study acknowledges the contemporary pressures faced by clients, promoting the development of therapeutic models that leverage existing resources and encourage self-care. Such adaptations make therapy more accessible and relevant, particularly for individuals confronting economic and social challenges. The findings also underscore the importance of empowering clients to take an active role in their therapeutic journey, fostering greater autonomy and resilience, which are critical for long-term success. The significant impact of resistance to change on the Task subscale highlights the need for therapists to focus on managing resistance explicitly during the initial stages of therapy. Early identification and intervention strategies aimed at addressing resistance—such as motivational interviewing or resistance-specific techniques—may enhance therapeutic outcomes. Additionally, the study supports the efficacy of brief therapy approaches, demonstrating that effective interventions can be delivered in shorter time frames without compromising therapeutic outcomes. This insight may lead to a broader acceptance of short-term therapies within clinical settings, thereby improving access to mental health care for diverse populations.
Research Implications and Future Directions
The study’s findings underscore the potential of the FBIM to enhance therapeutic outcomes through a robust WA, while also emphasizing the necessity for future research on therapist-specific factors and personalized interventions. Differentiating between the alliance’s trait-like and state-like elements that define each patient will be important in the FBIM in the future. When these two components are separated, it becomes clear that the patients’ trait-like alliance component—their overall capacity to build fulfilling relationships with others, their internal representations of themselves and others, and their expectations in interpersonal relationships—is responsible for some aspects of the alliance-outcome association. This capacity can affect both the patient’s capacity to gain from therapy and the therapist’s capacity to build a fulfilling connection with the patient, which shows up as a solid alliance.
Furthermore, insights from this study may inform investigations into the dynamics of the TA, examining how various therapeutic models interact to affect client outcomes. Additionally, by pinpointing specific obstacles and client strengths, clinicians can develop tailored follow-up strategies that provide ongoing support and facilitate sustained progress beyond the initial therapy phase.
Conclusion
This study underscores the dynamic nature of the WA in FBIM and its role in therapeutic outcomes. Resistance to change and therapy modalities significantly influenced WA early in therapy, while client motivation showed no direct impact. CBT-predominant therapeutic emphasis demonstrated faster task-focused collaboration, highlighting the benefits of structured approaches, though further research on long-term effects is needed. The findings emphasize the value of tailored, client-cantered strategies and brief therapy models in fostering robust alliances and accessible care. Future research should explore therapist-specific factors and the interplay of trait-like and state-like components of the alliance to optimize outcomes.
Supplemental Material
sj-docx-1-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-1-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Supplemental Material
sj-docx-2-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-2-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Supplemental Material
sj-docx-3-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-3-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Supplemental Material
sj-docx-4-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-4-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Supplemental Material
sj-docx-5-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-5-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Supplemental Material
sj-docx-6-bmo-10.1177_01454455261416501 – Supplemental material for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study
Supplemental material, sj-docx-6-bmo-10.1177_01454455261416501 for Working Alliance and Therapeutic Change in Integrated Psychotherapy: A Longitudinal Study by Eleonora Volpato, Susanna Bergamaschi, Mattia Cis, Davide Sattin, Milena Ruffino, Giacomo Tognasso, Maria Clotilde Gislon and Francesco Pagnini in Behavior Modification
Footnotes
Acknowledgements
We would like to thank all the clients at the CRF Zapparoli Centre of the Istituto per lo studio e la Ricerca sui Disturbi Psichici (ISeRDiP) very much for their availability and participation. A special thank also to the psychotherapists of the CRF Zapparoli Centre of the Istituto per lo studio e la Ricerca sui Disturbi Psichici (ISeRDiP): Laura Boniardi, Fiore Bottazzi, Valeria Brazzoduro, Silvia Cavedoni, Michele Clemente, Barbara Colombassi, Francesca Ditta, Valentina Franchi, Marta Iungo, Giuliana Maggio, Federico Manzionna, Daniela Mazzitelli, Alessandra Messa, Sonia Molteni, Ottavia Musini, Valentina Moro, Dania Osualdella, Raffaella Pace, Angela Panetta, Vivian Pellegrinelli, Tobia Porta, Anna Roncoroni, Beatrice Rota, Elena Sartorio, Anna Sirtori, Giacomo Tognasso, Anna Luisa Eleonora Tutino, Simona Verrastro, Nicoletta Vurro. We would like to thank also Cristina Piazzolla and Tania Stievano for their support over the study period.
Abbreviations
Focus-Based Integrated Model (FBIM); Therapeutic Alliance (TA); Commissione Etica per la Ricerca in Psicologia (CERPS); Istituto per lo Studio e la Ricerca sui Disturbi Psichici (ISeRDiP); Strengthening The Reporting of OBservational studies in Epidemiology (STROBE); Symptom Checklist-90-R (SCL-90-R); Somatization (SOM); Obsessive-Compulsive (O-C); Interpersonal Sensitivity (I-S); Depression (DEP); Anxiety (ANX); Hostility (HOS); Phobic Anxiety (PHOB); Paranoid Ideation (PAR); Psychoticism (PSY); Global Severity Index (GSI); Positive Symptom Total (PST); Positive Symptom Distress Index (PSDI); Working Alliance Inventory—Short form revised (WAI-SF); Working Alliance (WA); Working Alliance Inventory for Clients (WAI-P); Working Alliance Inventory for Therapists (WAI-T); Cognitive Behavioural Therapy (CBT); Standard Deviations (SDs); Specific Learning Disorders (SLD).
Ethical Considerations
The studies involving human participants were reviewed and approved by Commissione Etica per la Ricerca in Psicologia (CERPS) of Università Cattolica del Sacro Cuore, Milan (Italy) on 14th October 2022 (protocol number: 47-22). The participants provided written informed consent to take part to this study.
Author Contributions
Eleonora Volpato: Conceptualization; methodology; writing—original draft; writing—review and editing; project administration; investigation; resources; formal analysis; software. Susanna Bergamaschi: Conceptualization; writing—original draft; writing—review and editing; methodology. Mattia Cis: Conceptualization; writing—review and editing; methodology. Davide Sattin: Conceptualization; writing—review and editing; methodology. Milena Ruffino: Conceptualization; writing—review and editing; methodology. Giacomo Tognasso: Conceptualization; writing—review and editing. Maria Clotilde Gislon: Conceptualization; supervision; Francesco Pagnini: Methodology; conceptualization; supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Istituto per lo Studio e la Ricerca sui Disturbi Psichici (ISeRDiP) is the funding body of the submitted study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eleonora Volpato and Francesco Pagnini were supported by Istituto per lo studio e la Ricerca sui Disturbi Psichici (ISeRDiP) for conducting the study. Eleonora Volpato declares the winning of an ERS Long-Term Research Fellowship 2024 grant (ID Number: LTRF202404-01155), which is unrelated to this study. The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
![]()
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.