
Abstract
This study examined the feasibility and acceptability of a culturally adapted, asynchronous online caregiver training program for Arabic-speaking families of children with developmental disabilities. The program addressed behaviors commonly described in the literature as challenging behavior,1 which may interfere with learning, participation, or social interactions. The training was culturally adapted using a structured checklist to enhance contextual and cultural relevance. Fourteen caregivers residing in Saudi Arabia participated. Pre- and post-training assessments showed statistically significant improvements in caregiver knowledge of behavioral strategies. Participants rated the training highly for clarity, cultural responsiveness, and perceived usefulness. Qualitative interviews underscored the program’s social validity and its relevance to caregivers’ lived experiences. These findings provide preliminary support for the potential of culturally grounded, online caregiver training programs to strengthen family capacity and expand access to evidence-based practices in underserved communities.
Keywords
Introduction
Challenging behaviors (CB) in young children refer to repeated behavior patterns that interfere with optimal learning or prosocial interactions with peers and adults (Powell et al., 2007). While CB is a traditional term in the field (Smith & Fox, 2003), modern literature and federal guidance emphasize that these actions are communicative responses to environmental, social, and cultural conditions rather than fixed child characteristics (Hendren & Widjaja, 2025; Moody & Stahel, 2025). Thus, the Center on Positive Behavioral Interventions and Supports (Center on PBIS, 2025) and the Office of Special Education Programs (OSEP, 2021) advocate for person-centered language, such as interfering behavior (IB), to focus on behavior’s impact on participation. We use CB when referring to the original training program (Lee, Hacker, Meadan, & Haidar, 2022) but adopt IB elsewhere to align with these inclusive perspectives. Regardless of terminology, these behaviors can predict long-term academic and social difficulties (Blair et al., 2010; Dunlap et al., 2006), and require early, culturally responsive intervention.
Children with disabilities, developmental delays, or emerging communication abilities may use CB to communicate needs or access support (Chan et al., 2023; Smith & Fox, 2003). When persistent, these behaviors can interfere with education, disrupt positive relationships, and hinder environmental integration (Frazier et al., 2022; Smith & Fox, 2003). Research also shows that persistent CB can shape long-term developmental outcomes and often restrict access to inclusive education or community engagement (Blair et al., 2010; Dunlap et al., 2006; Dunlap et al., 2010; Kulkarni et al., 2021; Matson et al., 2013; Mondi et al., 2022; Zaidman-Zait et al., 2020). Furthermore, CB can weaken connections with teachers, peers, and family, which can affect a child’s social and emotional well-being (Boyd et al., 2012; Mirenda et al., 2024; Simó-Pinatella et al., 2023).
IB impacts the entire family system. Family Systems Theory (FST) posits that family relationships are interdependent; thus, changes in one member affect all others (Cox & Paley, 1997). Within this framework, family characteristics, functions, and life cycles shape individual behaviors (Titelman, 2014). Families of children with autism or developmental disabilities often rely on external supports to maintain emotional balance (Musetti et al., 2024; Shepherd et al., 2024). However, intense demands can strain marital relationships, disrupt sibling interactions (Schuntermann, 2007; Watson et al., 2021), and increase social isolation (Macdonald et al., 2023; Meadan et al., 2010; Neilsen & McEvoy, 2004). Research reveals a bidirectional link: caregiver stress and health concerns increase the likelihood of CB, while the behavior itself further heightens caregiver distress (Cohrs & Leslie, 2017; Dykens, 2015; Hickey et al., 2020; Lloyd & Hastings, 2009; Yorke et al., 2018). This feedback loop disrupts daily routines and limits community participation (Doubet & Ostrosky, 2015; Musetti et al., 2024; Shepherd et al., 2024), particularly when caregivers feel unprepared (McIntyre, 2013).
Evidence-based practices (EBPs) can break this cycle. These interventions demonstrate effectiveness through rigorous empirical research and show consistent positive outcomes across multiple populations (Wong et al., 2015). In the field of developmental disabilities, EBPs rely on systematic assessment, explicit instruction, and ongoing evaluation to guide decision-making. These programs use clearly defined procedures and data-informed adjustments to promote skill development and address behaviors that interfere with learning. Notably, interventions grounded in EBPs effectively reduce interfering behavior and decrease the likelihood of persistent behavior patterns (Powell et al., 2007). Consequently, caregiver training based on these principles shows consistent success in reducing challenging behaviors in children with autism and other developmental disabilities (Burrell et al., 2020; Ferguson et al., 2019).
Caregiver Training Programs
Caregiver training programs have traditionally relied on in-person delivery; however, recent years have seen a growing shift toward online training to improve access and convenience (Adedipe & Walton, 2025; Akemoglu et al., 2019; Bearss et al., 2015). Research shows that online programs can improve caregiver knowledge of behavior management and positive parenting strategies (Adedipe & Walton, 2025; Tarver et al., 2014) while offering added benefits such as flexibility, privacy, and self-paced learning (Ingersoll et al., 2017). Although online formats may limit in-person interaction, delay feedback, and require access to technology (Vismara et al., 2018), many programs address these challenges through video demonstrations, embedded knowledge checks, resource libraries, and opportunities for real-time or asynchronous feedback (Bearss et al., 2018).
The Challenging Behavior Online Modules (CBOMs; Lee, Hacker, Meadan, & Haidar, 2022) represent one such asynchronous caregiver training program designed to increase caregiver knowledge of behavior support principles and positive parenting practices. The program includes six short instructional video modules (6–12 min each; M = 9 min), for a total instructional time of approximately one hour. Module content addresses reinforcement, functions of behavior, antecedent- and reinforcement-based strategies, functional communication training, and token economies, with a focus on positive reinforcement to support skill development. The CBOMs were delivered through a learning management system (Moodle), and caregivers progressed through the program sequentially, with completion of each video and corresponding knowledge check required to access the next module. Instruction relied on prerecorded videos paired with pre- and post-training assessments and embedded examples. Results from the original evaluation indicated increased caregiver knowledge from pre- to post-training (mean change = 24%) and high acceptability of both the content and delivery format (Lee, Hacker, Meadan, & Haidar, 2022).
Following initial development and feasibility testing with English-speaking caregivers in the United States, the CBOMs were translated and culturally adapted for caregivers in South Korea and Paraguay (Lee et al., 2023; Terol et al., 2023). These adaptations incorporated culturally relevant language, examples, and visuals while maintaining the core instructional structure. Findings from these studies also demonstrated increases in caregiver knowledge and high acceptability of the content and delivery format. Together, these efforts illustrate a key advantage of online caregiver training: the ability to adapt evidence-based content across cultural contexts through asynchronous access to translated and culturally modified materials (Vanegas et al., 2023).
This adaptability supports the dissemination of EBPs to caregivers in underserved contexts, particularly where in-person services remain limited or unavailable (Terol et al., 2023). In applied healthcare and education literature, researchers often describe such contexts as “low-resource settings,” sometimes alongside terms such as “low- or middle-income countries” or “developing countries” (Van Zyl et al., 2021). However, these classifications can obscure meaningful variation in service availability. National income level does not necessarily reflect access to developmental disability services for specific populations or regions (Van Zyl et al., 2021). For example, families in middle- or high-income countries may still face limited access to affordable, evidence-based developmental disability services (Lee & Meadan, 2021). In this paper, the term low-resource setting refers to any context in which access to developmental disability services remains limited, including reduced availability of evidence-based interventions delivered by trained professionals or caregivers.
Cultural Adaptation
Supporting caregivers of children with disabilities requires attention to their specific needs within the context of their daily lives. Most caregiver training studies have focused on White participants in high-income countries, which restricts understanding of families from underrepresented populations and low-resource settings (Dababnah & Magaña, 2023; DuBay et al., 2018). This reflects a broader trend where EBPs have emerged from Western, Educated, Industrialized, Rich, and Democratic countries and have excluded perspectives from the global majority (Henrich et al., 2010; Lee & Meadan, 2021). For example, Steinbrenner and Odom (2025) reported that most autism intervention studies did not include racial or ethnic demographic data, and among those that did, most participants were White. Without broader representation, it remains unclear whether existing interventions meet the needs of families who were not included in their original development.
Over the past decade, researchers have called for efforts to strengthen caregiver capacity in low-resource settings and to align interventions with the cultural and contextual realities of the families who use them (de Vries, 2016; Magaña et al., 2021; Rice & Lee, 2017). In response, multiple studies have developed or modified caregiver training programs to serve families of children with disabilities (Blake et al., 2017; Buzhardt et al., 2016; Chlebowsky et al., 2018; Kuhn et al., 2020; Lee et al., 2023; Sengupta et al., 2020). Cultural adaptation refers to the process of modifying an existing intervention to improve its contextual fit for a new population, including factors such as acceptability, effectiveness and sustainability (Cabassa & Baumann, 2013; Lee et al., 2023).
To guide systematic cultural adaptation, many researchers have drawn on the Ecological Validity Framework (EVF; Bernal et al., 1995), which outlines eight dimensions for evaluating the cultural fit of an intervention: language, persons, metaphors, content, concepts, goals, methods, and context. Lee et al. (2023) expanded this framework by developing the Cultural Adaptation Checklist (CAC), a structured quality appraisal tool designed to support culturally relevant and contextually appropriate intervention modification and documentation. The CAC reorganizes the original EVF dimensions into seven domains: language, persons, content, goals, methods, context, and process, and provides operationalized definitions and quality indicators for each. For example, the language domain includes considerations related to translation accuracy and dialectical appropriateness, and the persons domain addresses the cultural representation of those delivering or receiving the intervention. The content domain focuses on incorporating culturally relevant knowledge, values, and metaphors, while the goals domain considers alignment between intervention objectives and the priorities of the target community. The methods domain evaluates the cultural appropriateness of delivery formats and instructional strategies, and the context domain accounts for ecological and systemic variables such as access to services and sociopolitical environments. Importantly, Lee et al. added a new domain, process, which emphasizes iterative adaptation and stakeholder engagement. In total, the CAC includes 32 quality indicators that support the systematic evaluation and documentation of cultural adaptation efforts across diverse implementation settings (Lee et al., 2023).
Caregivers in Arab Countries
In a comparative study, Alkhateeb et al. (2019) examined caregivers’ perspectives on raising autistic children in the United States and several Arab countries. They found that families in both regions reported similar challenges, including mental health concerns, social stigma, and a negative impact on quality of life. As expected, caregivers in Arab countries reported greater concerns related to financial strain and limited access to services compared to their U.S. counterparts. A recent literature review by Alkhateeb et al. (2022) echoed these findings. Other researchers have examined the needs of caregivers in specific Arab countries. For example, mothers of autistic children in Saudi Arabia described significant barriers to navigating services and expressed a need for more intensive guidance in managing daily challenges (Alrajhi & Dimitriou, 2023). Similar concerns emerged among caregivers in Qatar and Morocco, where parents frequently reported difficulty addressing the CB of their autistic children (De Jonge et al., 2024; Ekas et al., 2024). These studies underscore the importance of providing accessible, culturally appropriate training for Arabic-speaking caregivers, particularly in the area of behavior support. Low-cost, caregiver-led interventions may offer a promising solution in low-resource contexts where professional services are limited (Lee & Meadan, 2021).
To address these needs, we culturally adapted an asynchronous online caregiver training program originally developed by Lee, Hacker, Meadan, and Haidar (2022), using the CAC (Lee et al., 2023) to better serve Arabic-speaking families. The program was pedagogical in nature, designed to build caregivers’ understanding of behavioral principles in everyday contexts, with a focus on identifying the purpose of behavior and using reinforcement strategies to reduce distress and support more adaptive alternatives. Our goal was to identify a feasible and meaningful training model for caregivers of children with disabilities in understudied, Arabic-speaking, and low-resource settings. We also examined how caregivers experienced the adapted program, including their understanding of behavioral concepts and their perceptions of its cultural relevance and social validity. This study was guided by the following research questions: (1) How does the culturally adapted program impact Arabic-speaking caregivers’ knowledge of behavioral principles? (2) How do Arabic-speaking caregivers perceive the cultural responsiveness and social validity of the program’s goals, procedures, and outcomes?
Method
Recruitment and Participants
Following approval from the university’s Institutional Review Board (IRB), participants were recruited using a purposive sampling strategy (Palinkas et al., 2015; Patton, 2015). Study information was shared on social media platforms and through direct contact with autism-related service providers and clinics. Inclusion criteria were: (1) Arabic-speaking caregivers, (2) a child under 12 years of age diagnosed with autism or another developmental disability who engages in behavior described in the literature as challenging behavior, (3) access to internet-enabled technology, and (4) residence in the United States, Saudi Arabia, Lebanon, Jordan, or Egypt. These locations were selected based on existing research networks and IRB-approved recruitment protocols.
Eligible participants completed an online consent form and demographic questionnaire prior to training. Of the 29 caregivers who accessed the modules, 14 completed all six training modules, assessments, and interviews and were included in the final analysis (see Table 1). Most participants resided in Saudi Arabia (n = 13, 93%), with one participant from Jordan (n = 1, 7%). The final sample included 11 mothers and 3 fathers. Educational backgrounds ranged from high school to doctoral degrees, with most participants holding at least a bachelor’s degree. All caregivers reported parenting a child under 13 years of age with a diagnosis of autism spectrum disorder (ASD), developmental delay (DD), intellectual disability (ID), or attention-deficit/hyperactivity disorder (ADHD). Caregivers described behaviors commonly identified as challenging in the literature, including vocal outbursts, physical aggression, sensory-related difficulties, task refusal, and restricted or repetitive behaviors occurring during daily routines such as mealtime, hygiene, play, and transitions.
Parent and Child Demographic Information.
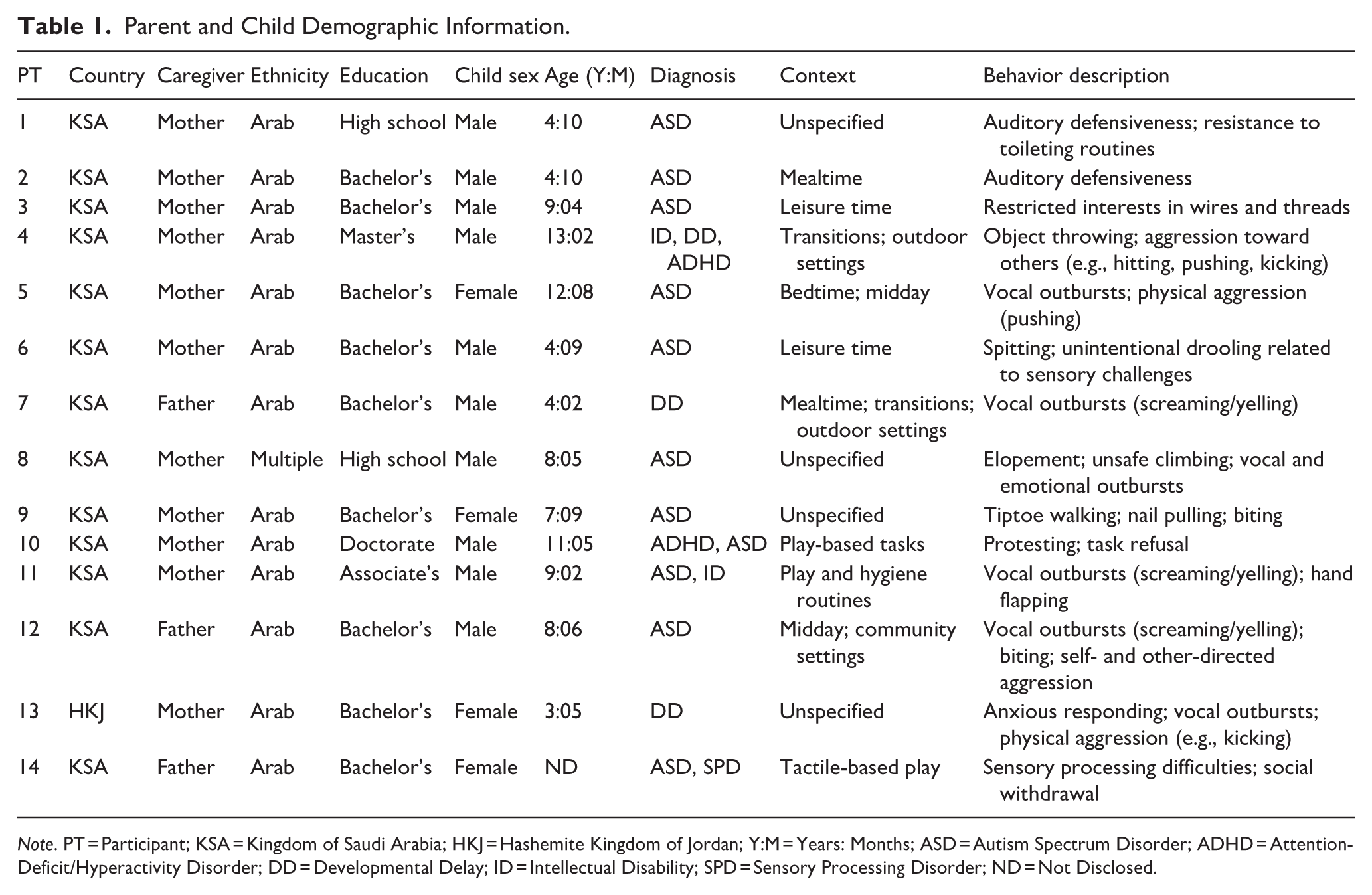
Note. PT = Participant; KSA = Kingdom of Saudi Arabia; HKJ = Hashemite Kingdom of Jordan; Y:M = Years: Months; ASD = Autism Spectrum Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; DD = Developmental Delay; ID = Intellectual Disability; SPD = Sensory Processing Disorder; ND = Not Disclosed.
Design
This study used a descriptive multiple methods design to evaluate program feasibility and cultural responsiveness (Kazdin, 2017). The research did not aim to establish causal effects but focused on preliminary caregiver outcomes. The quantitative strand utilized a one-group pretest-posttest approach to measure changes in behavioral knowledge. In parallel, the qualitative strand used semi-structured interviews to explore caregiver perceptions of relevance, clarity, and cultural appropriateness (Patton, 2015). These two components addressed distinct research aims and remained separate throughout the process. Consistent with multiple methods, rather than mixed methods, design, the analysis did not integrate the two data sets (Creswell & Plano Clark, 2018). This dual-track approach allowed for a comprehensive assessment of the program’s feasibility for Arabic-speaking families.
Participants and Recruitment
Following approval from the university’s Institutional Review Board (IRB), the researchers recruited participants using a purposive sampling strategy (Palinkas et al., 2015; Patton, 2015). Study information was shared on social media platforms and through direct contact with autism-related service providers and clinics. Inclusion criteria were: (1) Arabic-speaking caregivers, (2) a child under 13 years of age with a developmental disability and challenging behavior, (3) access to internet-enabled technology, and (4) residence in the United States, Saudi Arabia, Lebanon, Jordan, or Egypt.
Of the 29 caregivers who accessed the modules, 14 completed all training requirements and were included in the final analysis (see Table 1). Most participants resided in Saudi Arabia (n = 13), with one in Jordan (n = 1). The sample included 11 mothers and 3 fathers with educational backgrounds ranging from high school to doctoral degrees. All caregivers reported parenting a child with a diagnosis of ASD, DD, ID, or ADHD.
Researcher Positionality Statement
An Arabic-speaking Saudi national conducted recruitment and interviews. His linguistic and regional alignment supported rapport and culturally appropriate communication. To respect privacy and gender-related norms, all interviews utilized audio-only WhatsApp messaging. The broader research team consisted primarily of female researchers, including bilingual and bicultural doctoral students and a faculty member. Most members were Board Certified Behavior Analysts. The first authors led the cultural adaptation, while the qualitative analysis occurred exclusively among Arabic-speaking members to preserve linguistic nuance. The lead analyst did not participate in recruitment or interviews to reduce the influence of prior assumptions (Berger, 2015).
Measures
Caregiver Demographic Questionnaire
Participants completed an online questionnaire prior to training. The tool collected information on caregiver age, gender, education, income, and preferred communication. Caregivers also provided data regarding their child’s age, diagnosis, and the perceived impact of behaviors on the family.
Parent Knowledge Assessment (PKA)
The PKA (Lee, Hacker, Meadan, & Haidar, 2022) addressed the first research question: How does the culturally adapted program impact Arabic-speaking caregivers’ knowledge of behavioral principles? The PKA aligns with the instructional content and measures caregiver knowledge of core behavioral concepts, such as functions of behavior, reinforcement, and antecedent- and consequence-based strategies. The assessment consists of 30 items, with 5 questions mapped to each of the 6 instructional modules. Each item utilizes a multiple-choice or true/false format with four to five possible responses, including a “do not know” option to reduce guessing.
To ensure linguistic and conceptual equivalence, the research team translated the PKA into Modern Standard Arabic. The adaptation refined item scenarios to reflect culturally relevant caregiver-child interactions. For example, the assessment for the final module (Module 6) requires caregivers to identify the most effective timing for praise following a desired child behavior and to distinguish appropriate examples of descriptive verbal praise. Other items evaluate knowledge of reinforcement systems, such as token economies and the correct application of symbolic rewards.
To provide a precise measure of knowledge gain, participants completed the PKA as a pretest and posttest for each section of the training, with one attempt per assessment and unlimited time. This repeated-measure structure resulted in 12 total assessment points per participant. The researchers scored each correct response as one point and each incorrect or “do not know” response as zero. The team summed these scores for a maximum possible score of 30. Lee, Hacker, Meadan, and Haidar (2022) reported acceptable internal consistency for the PKA, with Cronbach’s alpha coefficients of .63 at pretest and .82 at posttest. In the present study, the PKA served as an index of caregiver knowledge change associated with participation in the asynchronous training program, without the implication of causal effects.
Social Validity Semi-Structured Interviews
Semi-structured interviews served as the primary qualitative data source to address the second research question: How do Arabic-speaking caregivers perceive the cultural responsiveness and social validity of the program’s goals, procedures, and outcomes? Guided by the social validity framework (Wolf, 1978), the researchers investigated perceptions of the training’s acceptability, feasibility, and relevance to their daily lives (Baer et al., 1968; Kazdin, 2021; Lane & Beebe-Frankenberger, 2004; Schwartz, 1996). Arabic-speaking research team members developed the initial interview protocol, which the full team refined and piloted with two external native Arabic-speaking caregivers to ensure clarity and cultural relevance.
The final protocol consisted of 13 open-ended questions. To assist in the interpretation of these findings, the team organized the questions into four primary domains (see Supplemental Information SI-1): (1) Procedures and Usability, which addressed experiences with the online modules, difficult components, and the delivery method; (2) Goals and Relevance, which addressed the helpfulness of module components, content quality, and recommendations for improvement; (3) Cultural Responsiveness, which addressed the presentation of information and the alignment of the training with the caregivers’ daily lives and child interactions; and (4) Outcomes and Impact, which addressed the implementation of strategies, changes in parent and child behavior, impact on the family, and the likelihood of recommendation to others.
Procedures
Cultural Adaptation Process
The researchers culturally adapted the Challenging Behavior Online Modules (CBOMs) using the Cultural Adaptation Checklist (CAC; Lee et al., 2023), which provides a structured framework across seven domains: language, persons, content, goals, methods, context, and process (see Table 2). For a comprehensive documentation of the 32 quality indicators used in this study, refer to Supplemental Information SI-2.
Cultural Adaptation of the CBOM Using the CAC.
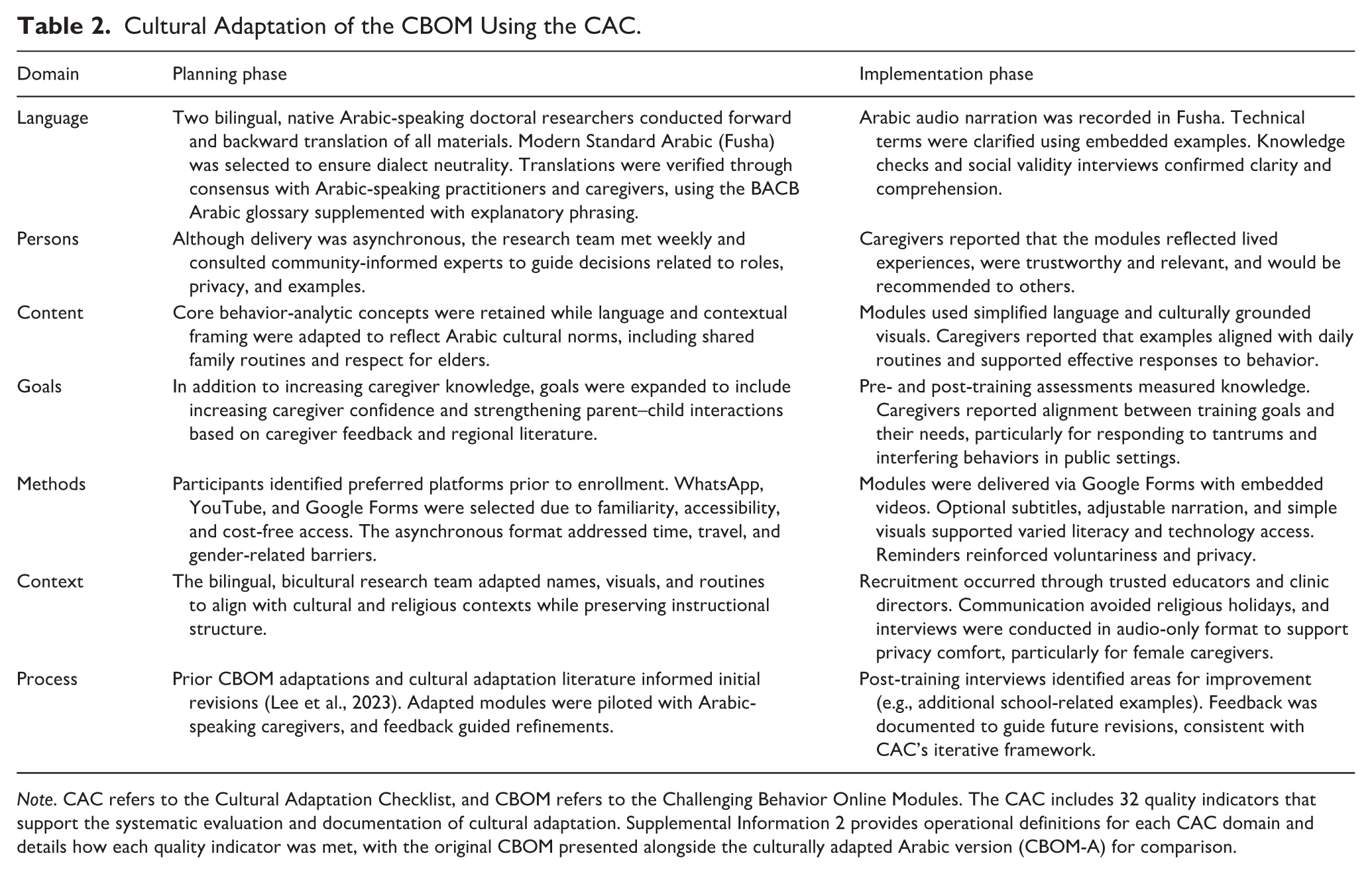
Note. CAC refers to the Cultural Adaptation Checklist, and CBOM refers to the Challenging Behavior Online Modules. The CAC includes 32 quality indicators that support the systematic evaluation and documentation of cultural adaptation. Supplemental Information 2 provides operational definitions for each CAC domain and details how each quality indicator was met, with the original CBOM presented alongside the culturally adapted Arabic version (CBOM-A) for comparison.
Two native Arabic-speaking doctoral researchers led the adaptation. They conducted forward and backward translation, coordinated iterative team review, and incorporated feedback from community-informed experts throughout the process. The research team consulted two Arabic-speaking experts with direct experience supporting caregivers: (a) a Lebanese American Board-Certified Behavior Analyst (BCBA) who was also a caregiver of a young child with developmental delays and (b) a Lebanese national special education teacher. Following internal revisions, an external Arabic-speaking special education expert from Saudi Arabia reviewed the full set of modules to evaluate clarity, coherence, and cultural appropriateness. The team finalized all materials through consensus to ensure consistency across module content and delivery procedures.
Online Training Program
Caregivers completed a self-directed, asynchronous online training adapted from the Challenging Behavior Online Modules (CBOMs; Lee, Hacker, Meadan, & Haidar, 2022). The Arabic adaptation, Challenging Behavior Online Modules–Arabic (CBOM-A), retained the original six-module structure and instructional sequence, with all content delivered in Modern Standard Arabic. Modules addressed core applied behavior analysis concepts relevant to caregiver practice, including behavioral function, reinforcement, antecedent-based strategies, and skill development (see Table 3).
Summary of Content in Each Online Training Module.
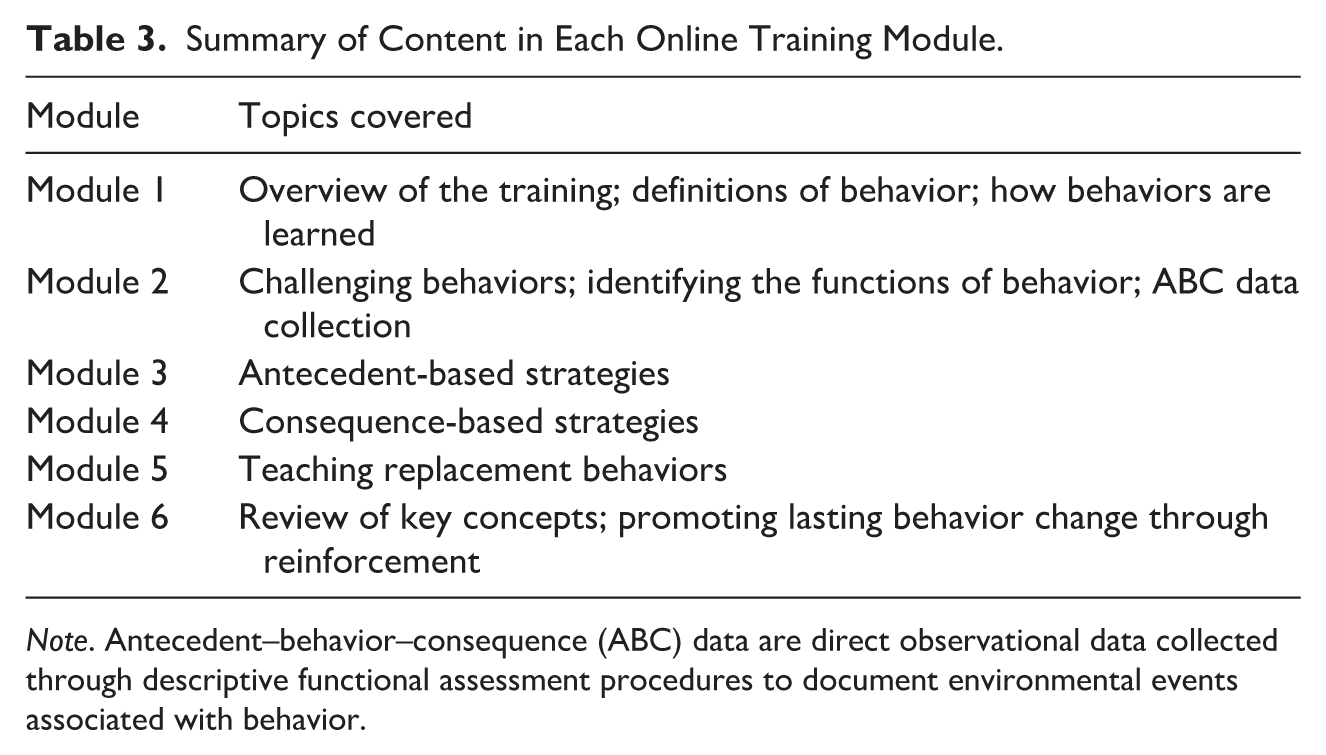
Note. Antecedent–behavior–consequence (ABC) data are direct observational data collected through descriptive functional assessment procedures to document environmental events associated with behavior.
Training Delivery and Participant Flow
Participants received a single email with links to the six training modules. The modules utilized Google Forms with embedded private YouTube videos to support a consistent sequence and automated data collection. These platforms required no specialized software, were accessible across devices, and reduced barriers to participation for caregivers across diverse geographic contexts. A screenshot of the training interface appears in Supplemental Information 4 (Supplemental Information SI-4).
Each module followed a fixed sequence: (1) a pre-training knowledge assessment, (2) an instructional video in Arabic, and (3) a post-training knowledge assessment (e.g., Pre-PKA 1, Module 1 Video, Post-PKA 1).
The researchers required completion of the pre-test before video access and the post-test to finish the module. Most individuals finished the program within 10 days. The team monitored progress through form submissions and sent weekly reminders via WhatsApp. After the conclusion of all modules and associated assessments, one author conducted individual, audio-only semi-structured interviews via WhatsApp. The researcher recorded and transcribed all sessions verbatim in Arabic. Interviews lasted an average of 46 min (range = 18–125 min). Participation remained voluntary without incentives.
Data Analysis
Quantitative Analysis
Prior to hypothesis testing, we examined the distribution of pre–post difference scores to assess the normality assumption for the paired-samples t test. Visual inspection of a histogram and Q–Q plot indicated approximate normality with no extreme deviations. We then conducted a paired-samples t test to evaluate within-participant changes in caregiver knowledge from pre- to post-training. Given the study’s feasibility focus and small sample size (n = 14), the analysis was intended to provide a preliminary estimate of knowledge change rather than to support causal inference or population-level generalization. Paired-samples designs are commonly used in feasibility and pilot research and remain robust to modest departures from normality when within-participant change is the primary outcome. All analyses were conducted using R version 4.3.2 (R Core Team, 2023).
Qualitative Analysis
Braun and Clarke (2006): familiarization, initial code development, theme identification, review, definition, and final report construction. Because the interview protocol followed predefined social validity domains (see Supplemental Information SI-1), a priori codes informed the initial process while allowing for iterative refinement across analytic phases. To strengthen analytic independence, the researcher who did not recruit or interview participants led the analysis.
Arabic-speaking research team members, fluent in the native language and cultural context, conducted the initial coding exclusively in the original Arabic. This step ensured the preservation of linguistic nuance and cultural meaning before any linguistic transfer. Following this primary phase, the team translated the transcripts and developed themes into English to achieve conceptual equivalence. To protect the integrity of the data, bilingual team members cross-referenced the English versions with the original Arabic recordings and text. The team resolved linguistic discrepancies through repeated review and consensus-based discussion until the final English themes accurately reflected the caregivers’ original intent and cultural expressions.
The team used a priori domains from social validity theory (Wolf, 1978) and the Cultural Adaptation Checklist (CAC; Lee et al., 2023; Lee et al., 2025) for the initial code structure. During the second phase, the coding team reviewed data excerpts, refined code definitions, and resolved disagreements through discussion and re-examination of the text until consensus was reached. This process resulted in a thematic codebook applied consistently across all transcripts (see Supplemental Information SI-3).
Results
Quantitative Results
Descriptive statistics indicated an increase in caregiver knowledge following the intervention. The mean pretest score across all modules was 18.43 out of 30 (61.4%), which increased to 21.43 out of 30 (71.4%) on the posttest. This improvement was observed across all modules (see Figure 1). At the module level, mean pretest percentages ranged from 38.6% (Module 1) to 84.3% (Module 6), while posttest percentages ranged from 52.9% (Module 1) to 95.7% (Module 6). Each module showed an increase in mean scores, with the largest gains observed in Module 4 (from 67.1% to 81.4%) and Module 1 (from 38.6% to 52.9%; see Figure 2). At the individual level, participants demonstrated variability across pre- and posttest conditions (see Figure 3). Most participants showed increases in the percentage of correct responses, with gains ranging up to approximately 38 percentage points. A small number of participants showed decreases in performance, with the largest decline observed from 53% to 47%. Results from the paired-samples t test indicated that posttest scores (M = 21.43, SD = 6.10) were significantly higher than pretest scores (M = 18.43, SD = 4.55), t(13) = 3.12, p = .008, with a medium effect size (Cohen’s d = 0.56) and a 95% confidence interval for the mean difference of [3.08, 16.92]. On average, participants demonstrated a 3-point (10%) increase in knowledge from pre- to post-training. These findings provide a preliminary estimate of within-participant knowledge change consistent with the study’s feasibility focus.
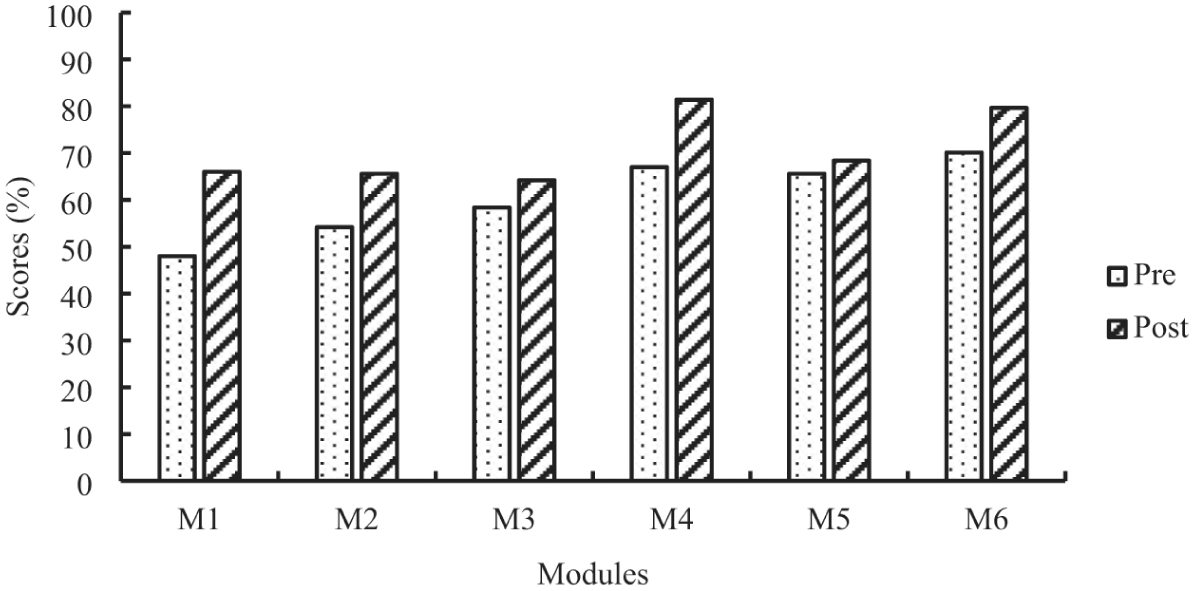
Average percentage of pre- and post-PKA correct responses by module.
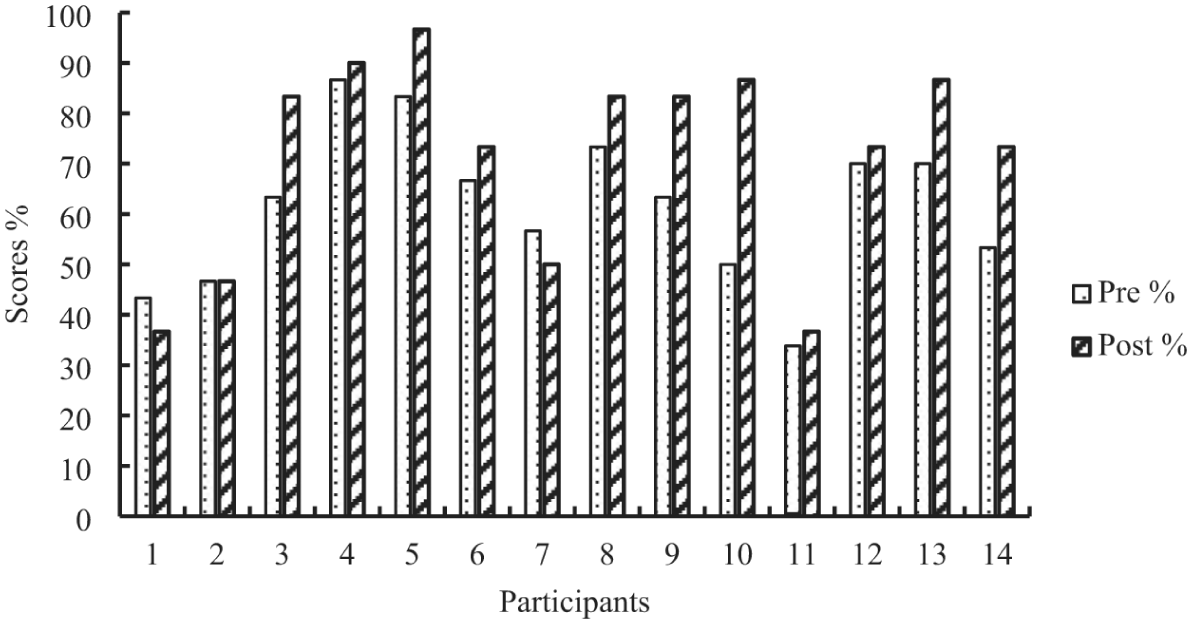
Percentage change of pre- and post-PKA scores by participant.
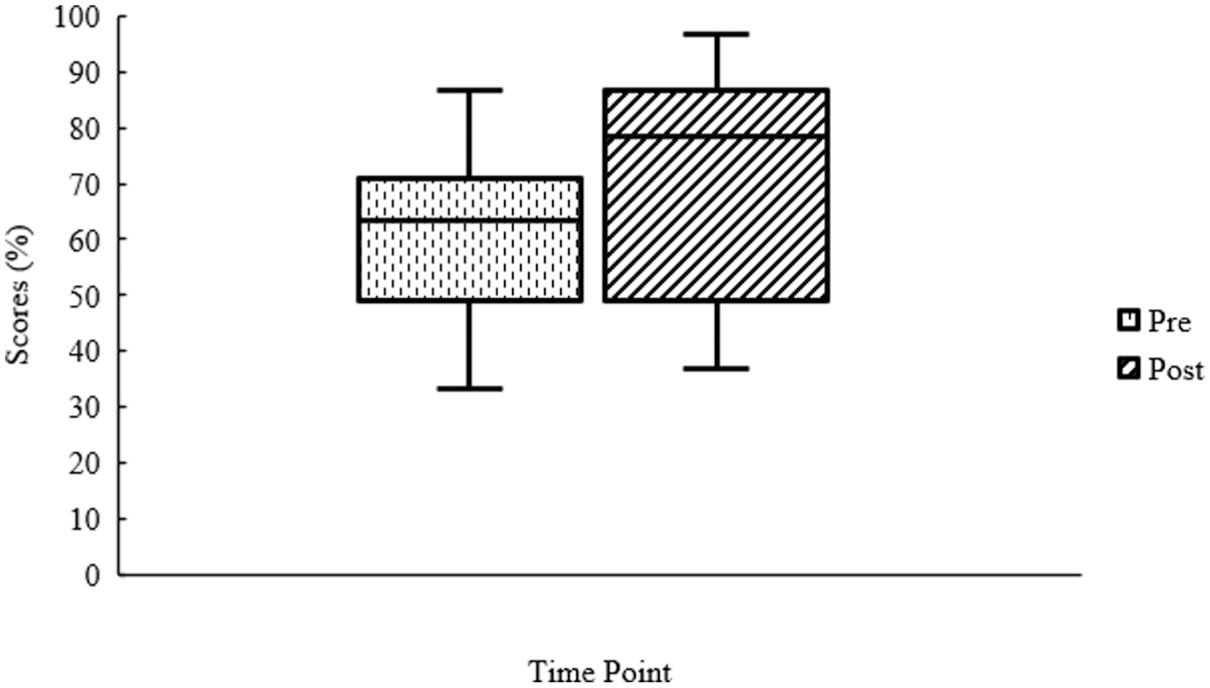
Distribution of pre- and post-training knowledge assessment scores.
Qualitative Findings
To examine caregivers’ perceptions of the social validity, feasibility, and cultural responsiveness of the culturally adapted caregiver training, we conducted semi-structured interviews with participating caregivers. Thematic analysis identified four overarching themes with eight associated codes (i.e., analytic building blocks), which are summarized in the thematic map (see Figure 4). Results are organized by theme to clarify how caregivers described the acceptability and feasibility of the training, the perceived practical significance of the content, the cultural and linguistic fit of the adaptation, and recommendations for improvement. This structure aligns with the study’s focus on feasibility and social validity rather than treatment efficacy. Detailed code definitions and representative excerpts are provided in Supplemental Information-4.
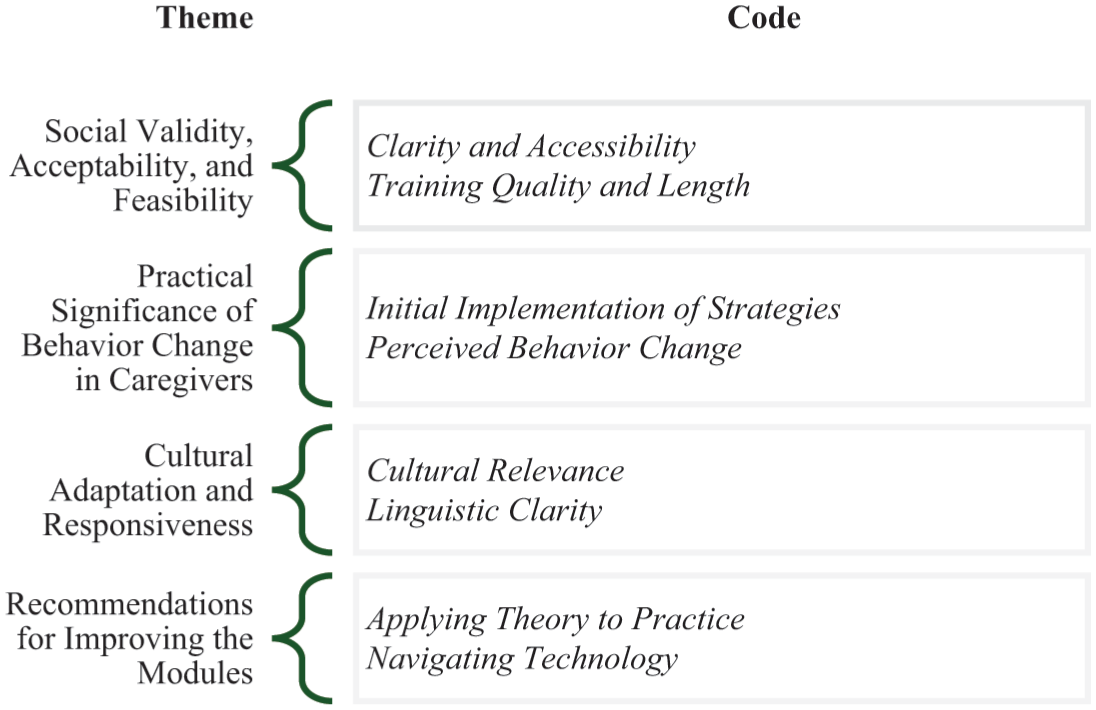
Thematic map for social validity interviews.
Social Validity, Acceptability, and Feasibility
This theme reflects caregivers’ perceptions of the program’s feasibility and acceptability and includes two codes: clarity and accessibility, and training quality and length. Caregivers described the goals of the training as meaningful and relevant to their needs. Many commented on the professional presentation and clear organization of the content. Several noted that the material suited caregivers with varied educational backgrounds. Many also reported greater understanding of evidence-based strategies and increased confidence when responding to their children’s behavior. One caregiver stated, “Your program is very impressive, clear, and professional. It stands out and is easy to understand for people of all backgrounds, whether they are beginners or experts.”
Caregivers also discussed the acceptability of the training procedures. They described the structure as straightforward and the content as thorough yet easy to follow. One caregiver shared, “the topic is very straightforward. May God reward you for explaining the principle and clarifying the terminology, which is somewhat technical for us. We are not specialists, but it was explained very clearly.”
In addition to content clarity, the caregivers commented on training quality and delivery. They described the videos as organized and supportive of learning through visuals and examples. One caregiver noted, “you’re reaching out to people with diverse knowledge and expertise. . . I understood the concepts better because you provided situations, visual scenarios, videos, and interactive experiences. . . It was comprehensive.”
Several caregivers commented on training length and pacing, with specific reference to the concise video format. As one caregiver stated, “these videos were short and focused on the key points. . . There was no boredom, and the content was entirely understandable. Honestly, I truly enjoyed watching them; they’re great.”
Taken together, these features shaped caregivers’ overall impressions of the program. Many expressed interest in continued access to the materials and reported recommending the training to others, as noted by one participant:
The entire content is fantastic. I even recommended it to some of my friends. It’s all consolidated unit by unit or in one great training course. I hope you keep it available for anyone, not just for your study, and share it online so anyone can access this intensive content, a summary of everything we’ve discussed.
Practical Significance of Behavior Change in Caregivers
This theme captures caregiver reports of early strategy use and perceived changes in daily interactions and includes two codes: initial implementation of strategies and perceived behavior change. Several caregivers voluntarily described early efforts to apply training strategies and reflected on how the content aligned with their daily caregiving routines. Although implementation of fidelity was not evaluated, these self-reports suggest perceived value and potential influence on child behavior. For instance, one mother mentioned, “I’ve started incorporating some of these strategies, particularly reinforcement and extinction. . . I’m seeing some results, although I’m still in the early stages of implementation.” Another caregiver described a decrease in her child’s screaming after informally applying differential reinforcement and extinction strategies learned during the training and explained:
I tried my best not to show any reaction, meaning I attempted to ignore this behavior. Whenever he saw that, for instance, I turned to the other side, didn’t look at him, occupied myself with something else, or engaged him with another activity, he eventually stopped. [screaming]
Caregivers also described increased confidence when managing daily routines and setting boundaries, noting perceived shifts in their parent–child interactions. As one caregiver shared, “I felt like I regained control. I realized that I had been lenient with him for a while, and maybe because he has improved a lot. . . I am actually happy with the results.”
Overall, participants described the training content as directly applicable to their daily lives and highlighted the practical use of applied behavior analysis principles presented in the online training. These testimonials illustrate caregivers’ perceptions of the program’s relevance and applicability to their parenting experiences.
Cultural Adaptation and Responsiveness
This theme reflects caregiver perceptions of the cultural and linguistic features of the training and includes two codes: cultural relevance and linguistic clarity. The participants described the examples as culturally relevant and aligned with their community context. One caregiver shared, “it’s clear that you really conveyed the topic to our community. I felt that the examples were very relevant to us. Thank you for the effort you put into this topic because it’s not easy.”
The caregivers also described the modules as clear, accessible, and appropriate for an Arabic-speaking audience. Several commented on the use of straightforward language and professional translation. One participant stated, “I’m an English language teacher, and I noticed that you used simple and very clear terms. It means the information wasn’t complicated to the point where it needed extensive translation.”
Participant Recommendations for Improving the Modules
This theme summarizes caregiver suggestions for strengthening the training and includes two codes: applying theory to practice and technology navigation. Although caregivers viewed the modules positively, many identified specific areas where additional support could improve usability and application.
With respect to applying theory to practice, several caregivers described challenges when transferring knowledge from the modules into daily interactions with their children. While caregivers reported that the concepts were clear, they noted difficulty recalling and using strategies consistently in real-life situations. One caregiver explained that the challenge did not stem from the content itself but from applying it during everyday caregiving demands:
Well, it’s like I don’t think there’s anything difficult, but the practical application is a bit challenging, that’s what it needs. I’ve read it and then when I try to implement it, I struggle to recall the information . . . . Sometimes, I find more challenges in the actual application.
In addition to challenges with application, caregivers offered recommendations related to assessment features and instructional clarity. Several participants expressed interest in clearer feedback on learning checks to better evaluate their understanding of the material. One caregiver described this need directly, stating, “you gave me the questions before the video, correct? Then, you gave me the questions after the video. You should, at the end, give me the results to compare and see if my answers were correct or not.”
The participants also discussed challenges associated with technology navigation, particularly when moving between platforms during the training. Some described uncertainty when accessing links or returning to the training interface. One caregiver explained, “I’m somewhat weak in technology. So, when I entered WhatsApp through the link, I would get two options: open in the same app or exit the app.” Another caregiver described losing responses after switching between applications.
Despite these challenges, caregivers shared their feedback constructively and demonstrated continued engagement with the training. Many framed their suggestions as ways to strengthen an already helpful program. Across interviews, caregivers continued to describe the training as relevant and supportive of their parenting practices. Several reported that the knowledge they gained applied to daily routines and decision making. Taken together, these findings provide preliminary qualitative support for the feasibility and social validity of the CBOM-A and suggest that culturally adapted caregiver training may offer meaningful support for families in low-resource contexts.
Discussion
This study evaluated the feasibility, cultural responsiveness, and preliminary knowledge outcomes of an asynchronous caregiver training program (CBOM-A) for Arabic-speaking families. Findings provide early support for the program’s potential to improve caregiver knowledge while it also addresses cultural and linguistic needs. However, consistent with feasibility research, these knowledge gains are preliminary and do not establish causal impact.
From a behavior analytic perspective, several mechanisms may account for these outcomes. The modules incorporated visuals and culturally relevant scenarios that functioned as discriminative stimuli for appropriate caregiver responses, thereby promoting stimulus control over targeted concepts (Cooper et al., 2020). In addition, the combination of narrated instructional modules and repeated pre- and post-assessments reflects key features of structured, computer-based instruction, in which sequenced content and opportunities to respond support the acquisition of conceptual repertoires (Higbee & Sellers, 2020). The asynchronous format also aligns with research that demonstrates that self-directed training can effectively teach behavior analytic procedures and expand access to intervention (Higbee & Sellers, 2020). Finally, the observed increase in caregiver understanding is consistent with prior implementations of these modules in Paraguay and South Korea (Lee et al., 2023; Lee, Meadan, & Xia, 2022; Terol et al., 2023).
Social Validity, Acceptability, and Feasibility
Caregivers endorsed the program’s clarity and accessibility. They noted that the professional organization suited varied educational backgrounds and that the Modern Standard Arabic (MSA) enhanced comprehension across regions (Holes, 2004). This high acceptability aligns with prior research which demonstrated that asynchronous, culturally responsive training supports caregiver engagement (Ingersoll et al., 2017; Meadan et al., 2016). To further structure the interpretation of these results, the team applied the eight domains of the Bowen et al. (2009) feasibility framework: acceptability, demand, implementation, practicality, adaptation, integration, expansion, and limited efficacy testing.
Evidence supported the domains of acceptability and practicality as primary strengths; most participants completed the training independently with personal technology and reported that the goals were meaningful. The adaptation domain also showed strength, as participants emphasized the value of visuals and scenarios grounded in their own cultural context. However, the 51% attrition rate (14 of 29 participants) highlights significant challenges in the demand and implementation domains. This dropout rate reflects broader digital health trends often influenced by time constraints, content overload, or a lack of immediate support (Dai et al., 2021).
While recruitment yielded strong initial interest within Saudi Arabia, outreach to Arabic-speaking diaspora communities in the United States resulted in no enrollment. This indicates that the expansion domain requires more tailored engagement strategies to reach families outside of the Middle East. Furthermore, integration appeared only partial; while caregivers applied strategies at home, they noted difficulties with consistency and a lack of broader institutional support from schools or clinics.
Community engagement proved vital to the adaptation process, as Arabic-speaking community members supported referrals and ensured the content remained relevant. Finally, the study met the criteria for limited efficacy testing through the observed 10% increase in knowledge scores, though the lack of a control group prevents a full assessment of impact. Future iterations should incorporate platform analytics and exit feedback to guide refinements to content structure, pacing, and long-term sustainability across these eight domains.
Practical Significance and Behavior Change
Caregivers reported early efforts to use reinforcement and extinction strategies. These experiences reflect FST (Cox & Paley, 1997; Titelman, 2014), where shifts in caregiver behavior create ripple effects in family dynamics. These outcomes link to improved caregiver self-efficacy and resilience (Bekhet et al., 2012; Manning et al., 2011). However, caregivers identified a “theory-to-practice” gap. This result mirrors findings that asynchronous content often requires a pair with real-time coaching to yield high-fidelity implementation (Chung et al., 2022; Rispoli et al., 2025). Future studies must evaluate blended delivery models that combine asynchronous modules with synchronous coaching or peer mentorship to enhance strategy implementation (Snodgrass et al., 2018). Furthermore, to move beyond self-reports, researchers should incorporate direct observation, parent-recorded videos, and third-party coding to differentiate between knowledge acquisition and real-world behavior change (Frost et al., 2020; Sone et al., 2021).
Cultural Adaptation and Responsiveness
The adaptation process followed the CAC (Lee et al., 2023), which ensured alignment with the values of Arabic-speaking families. This systematic approach produced content that participants described as “emotionally validating” and “deeply relevant” to their lived experiences. The use of Modern Standard Arabic (MSA) supported comprehension across a geographically diverse sample; however, caregiver recommendations for dialectal variation suggest that further linguistic tailoring may enhance emotional salience and reduce the perceived distance of technical instruction (Holes, 2004). These findings address broader critiques of Eurocentric intervention models that often overlook collectivist and spiritual values within non-Western communities (Dababnah & Magaña, 2023; Magaña et al., 2021).
Caregivers also identified linguistic nuance as a key feature in the presentation of behavioral concepts. Ongoing refinement should prioritize strength-based terminology to avoid the pathologization of child behavior. For example, the replacement of terms such as “challenging behavior” with more neutral or context-sensitive descriptors may reduce stigma associated with developmental disabilities and increase the acceptability of intervention practices (Banks et al., 2023). These adjustments may improve contextual fit and support the uptake and sustained use of intervention strategies. Through the incorporation of caregiver feedback throughout the adaptation process, the program extended beyond translation and moved toward a culturally responsive model that reflects the values and communication practices of the target community.
Limitations and Future Directions
Several methodological limitations warrant explicit acknowledgment. First, the study relied on caregiver self-reports, which introduces the potential for social desirability bias. Participants may have felt inclined to report positive experiences to researchers who share their cultural or linguistic background (Rosenman et al., 2011). Second, although knowledge scores increased, a significant theory-to-practice gap remains. The current data measure conceptual understanding rather than the fidelity of implementation or direct child outcomes; therefore, the team cannot confirm if caregivers successfully translated this knowledge into functional behavior change (Frost et al., 2020). Third, while MSA supported broad comprehension, the use of a formal register may have created an emotional distance. The absence of dialectal variations represents a linguistic limitation that could impact the personal resonance of the instruction (Holes, 2004). Finally, Arabic-speaking families are not a monolith. This sample primarily consisted of college-educated mothers in Saudi Arabia, which limits the generalizability of the findings across the regional, socioeconomic, and cultural diversity of the Arab world.
These limitations provide a roadmap for future research. To address the gap between knowledge and action, future studies should evaluate blended delivery models that pair asynchronous content with synchronous coaching (Chung et al., 2022). Researchers must also move beyond knowledge checks to include child-focused outcomes, such as direct behavioral observations or quality-of-life ratings. Such data would clarify the link between cultural responsiveness and clinical efficacy. To improve social validity, ongoing refinement must focus on dialectal adaptation to enhance emotional salience. Furthermore, future efforts should utilize Community-Based Participatory Research (CBPR) to reach a more diverse range of Arabic-speaking subgroups (Banks et al., 2018). Ultimately, the integration of cultural resonance, strength-based terminology, and real-time support is essential to promote the sustained use and maintenance of intervention strategies in underserved contexts.
Conclusion
The CBOM-A offers a culturally responsive and linguistically accessible tool to bridge service gaps for Arabic-speaking families. This study demonstrates that the systematic adaptation of asynchronous training, guided by the CAC yields meaningful increases in caregiver knowledge and high social validity. Through the prioritization of strength-based terminology and culturally grounded scenarios, the program moves beyond mere translation toward a model that reflects the values and practices of the target community.
While high attrition and the absence of implementation metrics indicate a need for further refinement, these findings reflect a successful step toward equitable service delivery. Grounded in behavior analytic principles and community priorities, this program provides a scalable foundation for developmental disability services in underserved contexts. Future caregiver interventions should continue to prioritize terminology and delivery models that reduce stigma and support sustained impact across diverse global populations.
Supplemental Material
sj-docx-1-bmo-10.1177_01454455261444277 – Supplemental material for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity
Supplemental material, sj-docx-1-bmo-10.1177_01454455261444277 for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity by Ban Haidar, Rayan Alqunaysi, Hedda Meadan, Melanie R Martin Loya and Menaka De Alwis in Behavior Modification
Supplemental Material
sj-docx-2-bmo-10.1177_01454455261444277 – Supplemental material for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity
Supplemental material, sj-docx-2-bmo-10.1177_01454455261444277 for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity by Ban Haidar, Rayan Alqunaysi, Hedda Meadan, Melanie R Martin Loya and Menaka De Alwis in Behavior Modification
Supplemental Material
sj-pdf-3-bmo-10.1177_01454455261444277 – Supplemental material for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity
Supplemental material, sj-pdf-3-bmo-10.1177_01454455261444277 for Cultural Adaptation of a Caregiver Training Program for Arabic-Speaking Families: Feasibility and Social Validity by Ban Haidar, Rayan Alqunaysi, Hedda Meadan, Melanie R Martin Loya and Menaka De Alwis in Behavior Modification
Footnotes
Acknowledgements
We thank the caregivers for their time and insights, and the Society of Autism Families in Saudi Arabia for sharing study information and supporting family recruitment.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.