
Abstract
Depression, which is characterized by persistent low mood, diminished interest, and a loss of pleasure (World Health Organization, 2017), is recognized as a public health problem that can have a substantial impact on individuals, families, and society (Smith, Armour, Lee, Wang, & Hay, 2018). For example, research has documented the associations between depression and numerous other health-related outcomes, such as impaired health-related quality of life, higher rates of coronary heart disease, and increased mortality (Carney & Freedland, 2017; Shao et al., 2017). The study of depression among adults with visual impairments has been an area of particular interest (Brody, Roch-Levecq, Thomas, Kaplan, & Brown, 2005; Goldstein et al., 2012), since the presence of a visual impairment is known to increase the risk of depression (Margrain et al., 2012; Nollett et al., 2016). Reflecting these findings, estimates suggest that approximately 30% of adults with visual impairments in the United States experience depression (Brody et al., 2005; Margrain et al., 2012), a proportion that is considerably higher than the 8% of the general population with the condition (Brody, Pratt, & Hughes, 2018). Given the high prevalence of depression among adults with visual impairments, it is critical to identify modifiable factors related to depression among this population.
Lifestyle-related behaviors, during both sleep and awake time, can have important physical and mental health consequences (Rosenberger et al., 2019). Modifiable behaviors, including physical activity, sitting time, and sleep, have been linked to mental health outcomes among adults (Rosenberger et al., 2019; Zhai, Zhang, & Zhang, 2015) without disabilities. Because of the importance of each of these lifestyle-related behaviors in influencing physical and mental health outcomes, calls have been made to extend current research examining physical activity, sitting time, and sleep in independence, as well as to encourage researchers to consider the integrated nature of these behaviors (Rosenberger et al., 2019). This line of inquiry has largely focused on youth populations, where researchers have determined that youths meeting physical activity, screen-time, and sleep guidelines in concert are less likely to experience overweight or obesity or mental health concerns than those meeting none or some of these guidelines (Walsh et al., 2018; Zhu et al., 2019b).
Identifying the lifestyle-related behaviors that are associated with depression among adults with visual impairments can help inform the development of interventions to prevent or treat depression or depressive symptoms among this population. To date, however, research examining associations between modifiable behaviors, such as physical activity, sleep, and sitting time, and depression among adults with visual impairments is absent from the literature. Given the mental health benefits of these health-related behaviors among adults without disabilities (Rosenberger et al., 2019), it is logical to suggest that adults with visual impairments, a population at high risk for experiencing depression (Margrain et al., 2012; Nollett et al., 2016), may garner similar benefits. Thus, the first purpose of this study was to examine the associations between physical activity, sitting time, and sleep duration, as discrete behaviors, with depression. Moreover, given the integrative nature of the benefits of engaging in adequate amounts of physical activity, sitting, and sleep (Rosenberger et al., 2019), the second purpose of this study was to examine the effect of meeting none, one, two, or three of the guidelines for these behaviors on depression among adults with visual impairments. We adopted health-related guidelines for adults, which included standards outlined in the U.S. Department of Health and Human Services (HHS) publication, Physical Activity Guidelines for Americans, which recommends adults to engage in at least 150 minutes of moderate-to-vigorous physical activity per week (HHS, 2018); and the American Academy of Sleep Medicine (AASM) and Sleep Research Society’s (SRS) joint recommendation that adults to sleep at least seven hours per night. Given the sparsity of published sitting time guidelines for adults, we adopted recommendations for eight or less hours of sitting per day, which has been identified as a cut-off by several prior studies examining health outcomes associated with sitting time among adults (Gibson, Muggeridge, Hughes, Kelly, & Kirk, 2017; Koyanagi, Stubbs, & Vancampfort, 2018).
Methods
Data collection
This study employed an online survey methodology. Data collection for this study took place from June to September of 2019. Two visual impairment-related electronic discussion groups housed in the United States distributed study information to potential participants via email, with one discussion group allowing a second, reminder email. The invitation email explained the purpose, inclusion criteria, and the time commitment for the study, and it assured participants that participation was voluntary and that all responses would be kept anonymous and confidential. To be included in the study, a participant must have been 18 years of age or older, and self-reported having a visual impairment. Interested participants who followed the online survey link in the invitation email, and read and agreed to the terms of the consent form presented on the first page of the survey, advanced to the online questionnaire. The 27-item online questionnaire was hosted on the Google Drive Internet platform and was reviewed and deemed appropriate by an accessibility consultant with eye.t LLC (Baltimore, MD) prior to survey distribution. Data collection procedures were reviewed by the Human Subjects Review Committee at the first author’s intuition of employment and were determined to be exempt from institutional review board review according to federal regulations (exemption category 6.2). In total, 217 individuals accessed the distributed survey link. Of those, 182 individuals (83.8%) submitted complete surveys and were included in the analyses.
Measures
Physical activity and sitting time data were dichotomized to meeting or not meeting their respective guidelines. More specifically, physical activity guidelines were based on the HHS guidelines, and participants who reported engaging in at least 150 minutes of moderate-to-vigorous physical activity per week were considered “meeting physical activity guidelines,” whereas those below 150 minutes were considered “not meeting physical activity guidelines.” Sitting time recommendations were based on those used in prior research (Gibson et al., 2017; Koyanagi et al., 2018), where those who engaged in less than 8 hours of sitting time were categorized as “meeting sitting time guidelines,” whereas those who engaged in eight or more hours were categorized as “not meeting sitting time guidelines.” In addition to dichotomized variables, physical activity metabolic equivalent minutes-per-week (METmin/week) scores were derived using a standardized protocol (IPAQ, 2015) for correlational analyses.
Data analysis
The data analysis was conducted in three steps. First, descriptive analyses on mean and SD of the demographic variables, behavioral variables, and depressive symptoms were conducted. Additionally, a frequency analysis of participants’ sex; visual impairment level; and meeting none, one, two, or three health-related guidelines (i.e., physical activity, sitting time, and sleep) were conducted. Second, a Pearson product-moment correlation analysis was run on age, BMI, physical activity METmin/week, sitting time, hours of sleep, and depression scores. Finally, hierarchical regression analyses were conducted to estimate the association between behavioral and demographic variables and depression. Specifically, participants’ visual impairment level, sex, age, and education level were entered in the first block, body weight status as the second block, and number of movement guidelines met, first jointly then independently, as the last block of independent variables predicting depression. The residual P–P plot was examined for homoscedasticity, and variance inflation factor for multicollinearity diagnostics. The data analyses were conducted using the SPSS (ver. 25, IBM; Armonk, NY), with an overall p < .05 for statistical significance tests.
Results
Participants (Mage = 44.8 years, SD = 15.5) identified their race or ethnicity as Caucasian (n = 135, 74.2%), African American (n = 16, 8.8%), Hispanic or Latino (n = 9, 4.9%), and Asian (n = 8, 4.4%), and more than one racial or ethnic group (n = 14, 7.6%). Nearly half (47.8%) of the participants were self-identified in the B1 level of visual impairment (i.e., complete blindness). Most participants (n = 107, 58.8%) completed a bachelor’s degree or higher. A detailed description of the sample’s characteristics is shown in Table 1.
Frequency of participant demographic and behavioral characteristics (n = 182).
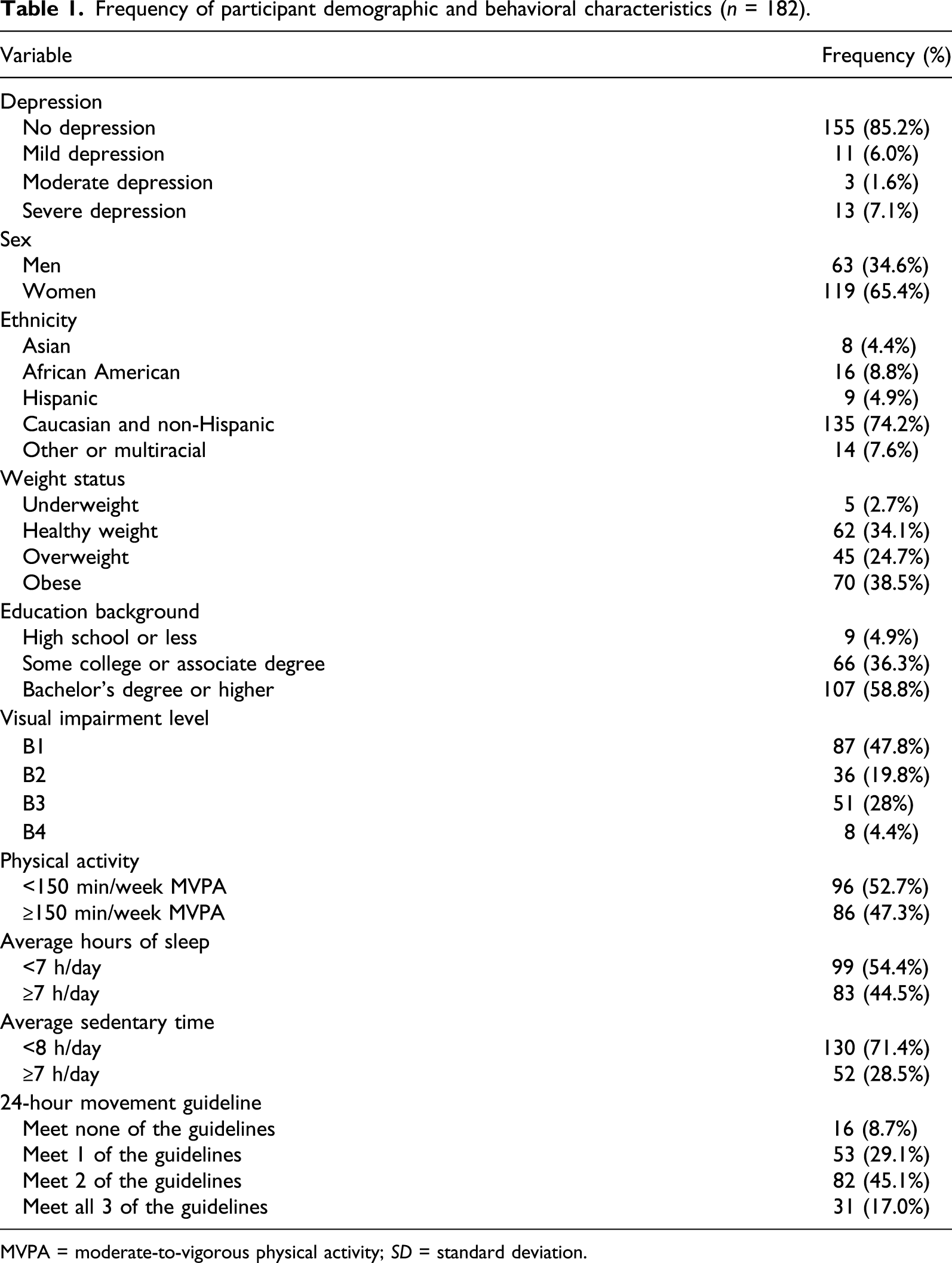
MVPA = moderate-to-vigorous physical activity; SD = standard deviation.
About one third of the participants (33.1%) were of a healthy weight, a quarter (24.7%) had overweight, and 38.5% had obesity. As seen in Table 1, less than half of the participants (47.3%) met the physical activity guideline, about 44.5% met the sleep guideline, and about 71.4% met the sitting time guideline. Taken together, only 17% of the adults with visual impairments concurrently met all three of the guidelines, 45.1% concurrently met two, 29.1% met one, and 8.7% met none of the guidelines.
Correlation coefficients between behavioral variables, demographic variables, and depression.
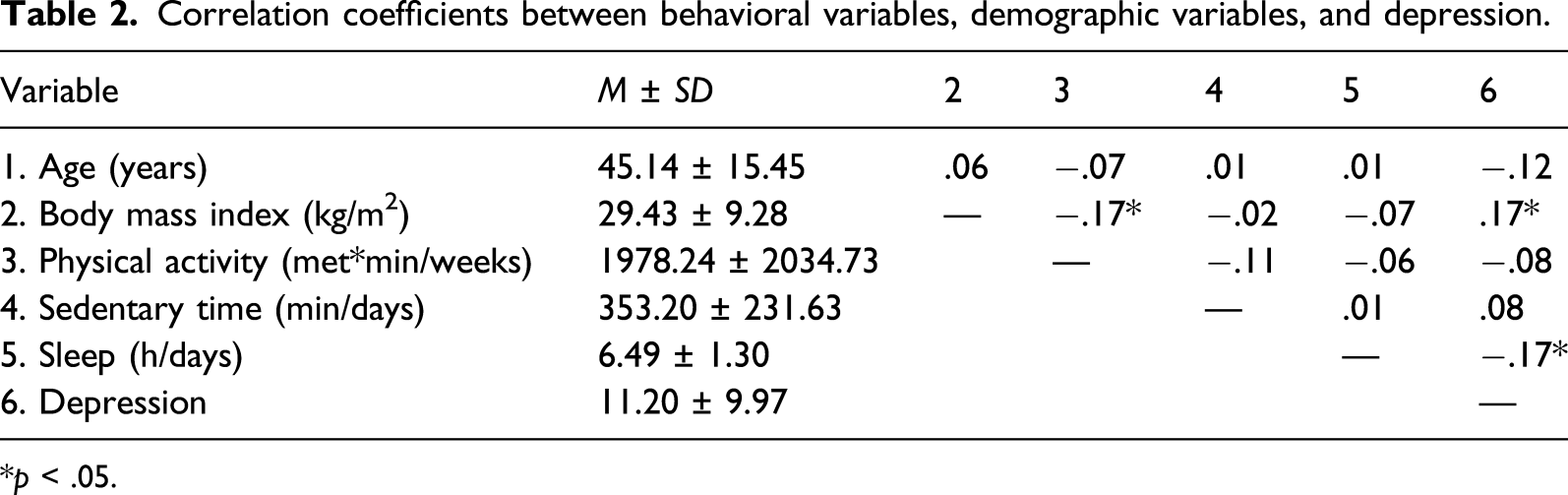
*p < .05.
Hierarchical multiple regression analysis results predicting depression.
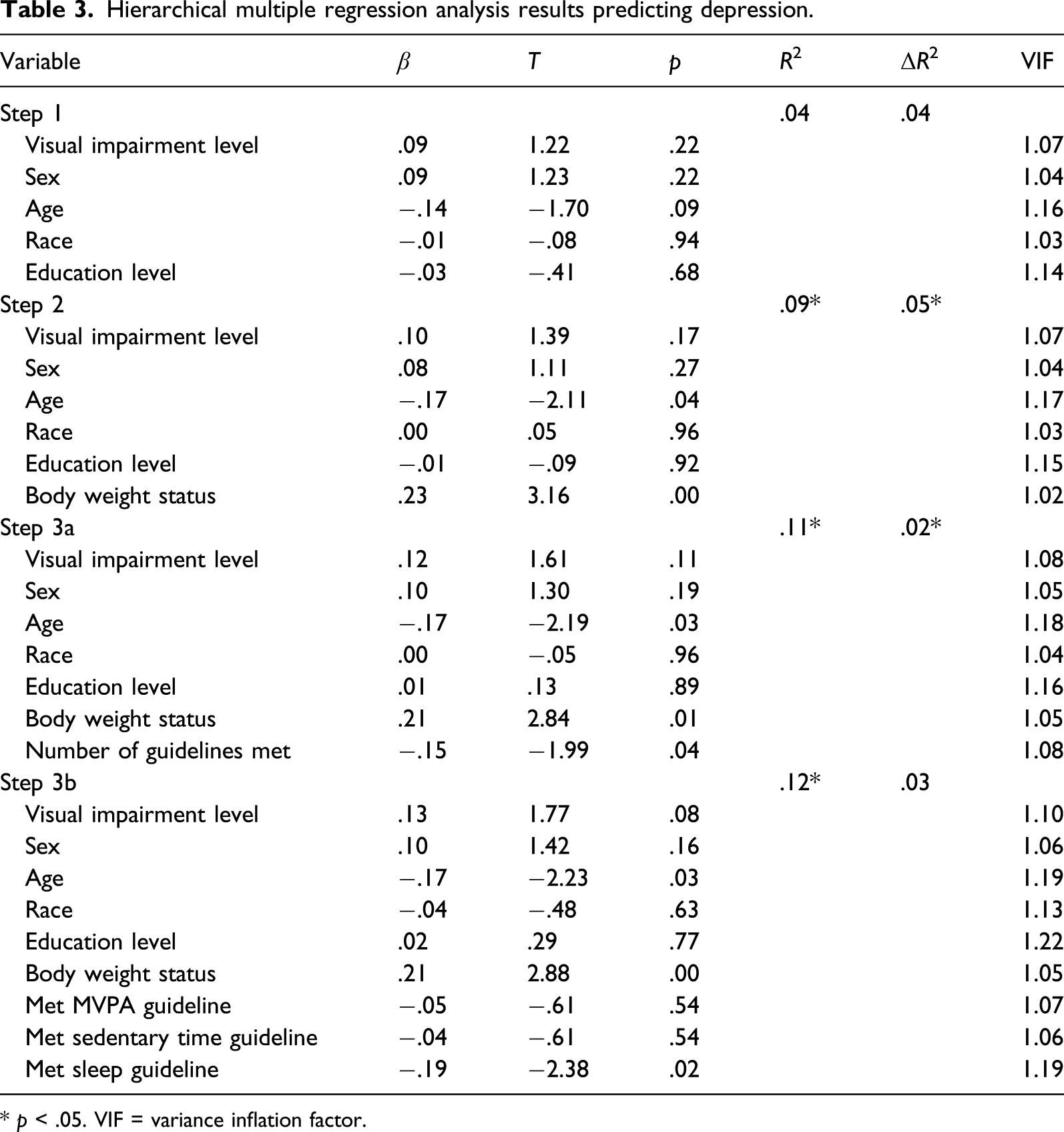
* p < .05. VIF = variance inflation factor.
Discussion
Brody and colleagues (2018), utilizing a population-based sample of adults aged 20 years and over in the United States, estimated that 8% of the U.S. population experienced depression in 2016. In the current sample, nearly double that many adults with visual impairments (14.7%) reported experiencing some degree of depression, according to the Major Depression Inventory. Although this figure is lower than recent estimates of depression prevalence of nearly 30% of adults with visual impairments in the United States (Goldstein et al., 2012; Margrain et al., 2012), it still represents as substantial percentage of the population. Thus, understanding how modifiable lifestyle-related behaviors are associated with depression is of the utmost importance.
When examining associations between physical activity, sitting time, and sleep duration, as discrete behaviors, with depression, sleep emerged as the most important lifestyle-related behavior. More specifically, meeting the sleep guideline was a significant negative predictor of depression scores in the hierarchical regression analyses. The importance of sleep health for depression is not surprising as inadequately short, as well as overly long, sleep duration is associated with an increased risk of depression among adults without disabilities (Zhai et al., 2015). The current study extends these findings to a population at a high risk of experiencing depression, adults with visual impairments (Brody et al., 2005; Margrain et al., 2012). It is important to note, however, that mechanisms underlying this relationship are not well understood among populations with or without visual impairments. That is, according to Zhai and colleagues (2015), although some arguments have been made connecting short sleep duration with increased psychological fatigue and depression (van Noorden, van Fenema, van der Wee, Zitman, & Giltay, 2012), more research is necessary to support and understand these connections.
Whereas participants who met sleep guidelines were more likely to have lower depression scores than those that did not, similar associations were unfounded with regard to the other two lifestyle-related behaviors: physical activity and sitting time. This finding might be considered surprising, particularly given the physical- and mental health–enhancing benefits that are commonly associated with engagement in these behaviors (Zhu et al., 2019a). For example, in a recent study by Haegele and Zhu (2019), a significant relationship emerged between minutes engaged in moderate-to-vigorous physical activity and psychological health among a cohort of 159 adults with visual impairments. Similarly, a study examining health-related quality of life, physical activity, and sedentary behavior among adults with visual impairments found that adults who engaged in less sitting demonstrated more positive health-related quality of life scores (Haegele, Famelia, & Lee, 2017). Although these prior studies have examined psychological health constructs, they are conceptually distinct from depression, and therefore differences in findings may be expected. Perhaps an additional explanation of the nonsignificant association could be related to inflated figures of those meeting guidelines in this study. More specifically, the number of participants meeting guidelines, particularly physical activity guidelines, in this analysis appears quite high. That is, nearly 50% of adults in this study reported figures that meet physical activity guidelines, which is substantially higher than recent figures that suggest that just 18.7% of youths with visual impairments meet physical activity recommendations (Zhu et al., 2019b). A noted limitation of this study is the utilization of self-report instruments (Adams et al., 2005), which may have contributed to an overreporting of desirable measures (i.e., minutes of physical activity), thus inflating percentages of individuals meeting guidelines in this study.
The second purpose of this study was to examine the impacts of meeting none, one, two, or three of the guidelines for physical activity, sitting time, and sleep on depression among adults with visual impairments. Consistent with assertions from Rosenberger and colleagues (2019) citing the integrative benefits of concurrently meeting these behavior guidelines, the number of guidelines met emerged as a significant negative predictor of depression scores among participants (i.e., adults who met more guidelines concurrently were less likely to report experiences of depression). This finding extends the extant literature examining the health benefits of meeting multiple health-behavior guidelines beyond youth without disabilities (Zhu et al., 2019a) to a population of adults with visual impairments who are particularly vulnerable to depression (Margrain et al., 2012; Nollett et al., 2016). Of concern, just 17.0% of the sample in this study reported to concurrently meet the three guidelines. Failing to meet each of these guidelines, which was the case for 83% of the sample in this study, may deprive this population from the psychological benefits associated with collectively meeting these guidelines, such as the reducing the likelihood of depression. Of particular concern among adults with visual impairments may be low levels of adherence to physical activity (47.3%) and sleep (44.5%) guidelines. These figures are not surprising, given prior research demonstrating that youths and adults with visual impairments appear to experience challenges with engagement in physical activities (Haegele, Aigner, & Healy, 2019; Marmeleira, Laranjo, Marques, & Pereira, 2014). As such, multi-behavioral interventions focused on promoting physical activity and enhancing sleep duration may be of particular relevance for this particular population.
Limitations are evident in this study. First, self-report instruments to measure physical activity, sitting time, and sleep may be viewed as a limitation as physical activity and sleep may be overreported, and sitting time underreported, due to social desirability (Adams et al., 2005). Although self-report instruments have historically been the main source of information on how individuals spend time, and they may be advantageous when attempting to gain access to, in an economically efficient manner, groups of individuals who are generally geographically dispersed, Rosenberger and colleagues (2019) suggest diverting away from self-report measures, since it is challenging for individuals to achieve the level of detail in data needed to examine movement across a 24-hour period. Second, while excellent reliability, and acceptable concurrent, criterion, discriminant and structural validity for the Major Depression Survey has been reported (Bech et al., 2015), this instrument has not been validated specifically for people with visual impairments. Third, the sample included in this study—which was skewed toward women, Caucasians, those with a bachelor’s degree or higher, and individuals who identified as having a B1 visual impairment level—may also be viewed as a limitation. Certain demographic groups may experience different lifestyle-related behaviors in different ways or may be more or less willing to disclose symptoms of depression. For example, non-24-hour sleep-wake disorder is a circadian rhythm disorder that is experienced by approximately 55–70% of totally blind individuals (Emens & Eastman, 2017), which may affect the ability of a large percentage of this particular sample in meeting sleep guideline rates. In addition, according to Call and Shafer (2018), women appear to be more likely to endorse symptoms of depression than men, which could influence self-reported results. As such, readers must take the participant characteristics of our sample into consideration when attempting to generalize these results to broader populations of people with visual impairments. Finally, data were limited in regard to the identification of specific visual impairment diagnoses and potential additional disabilities or health conditions among participants. However, since these variables were not collected in this study, it is unknown how specific visual impairment diagnoses or additional disabilities, or health conditions influenced the association between lifestyle-related behaviors and depression.
Conclusions
The current study provides evidence that the majority of the adults with visual impairments (82.9%, n=151) do not concurrently meet all three behavior guidelines. Controlling for the demographic variables, the number of behavior guidelines jointly met was negatively associated with experiencing depression. The current study’s results should prompt the continued examination of health-behaviors among adults with visual impairment using a more holistic 24-hour activity cycle framework. The results demonstrate the value of extending this framework to better understand the disparities related to depression among adults with visual impairment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.