
Abstract

Approximately 2.87 million traumatic brain injuries (TBIs) occur in the United States each year (CDC, 2019). TBIs may occur on a spectrum, and concussions are typically categorized on that spectrum based on severity (Galetta et al., 2011; Kazl & Torres, 2019). The terms concussion and mild TBI are used interchangeably and are the most common form of TBIs (Galetta et al., 2011; Kazl & Torres, 2019). Concussions typically result with classic symptoms via “complex pathophysiological processes.” Examples of complex pathophysiological processes include neuronal depolarization; stretching and alteration of neural structures; alterations in cerebral blood flow; changes in glucose metabolism; and ionic shifts that manifest via cognitive, emotional, and sleep-related impairments (Esterov & Greenwald, 2017; Galetta et al., 2011; Kazl & Torres, 2019). Additionally, concussions have known effects on physical functions (Akhand et al., 2019; Aubry et al., 2002). For example, vestibular function and efficacy, gait, and neuromuscular control are all visually dependent functions and tasks needed for activities of daily living (Akhand et al., 2019; Galetta et al., 2011; Kazl & Torres, 2019; Ventura et al., 2015). Any impairments or deficits caused by a concussion typically resolve within 7–10 days. Persistent symptoms are often associated with autonomic nervous system dysfunction (Galetta et al., 2011; Kazl & Torres, 2019; Ventura et al., 2015).
Concussion is a complex injury that is often difficult to diagnose, assess, and manage due to its subjective nature (Aubry et al., 2002; Row et al., 2019; Ventura et al., 2015; Yengo-Kahn et al., 2016). As a result, concussions are diagnosed, assessed, managed, and treated using a variety of standardized concussion assessment tools such as: the Sport Concussion Assessment Tool (SCAT5), which includes a Post-Concussion Symptom Severity score (PCSS), cognitive testing, and balance testing (Bell et al., 2011; Echemendia et al., 2017; Murray et al., 2014; Powell & Myers, 1985; Row et al., 2019; Ventura et al., 2015; Yengo-Kahn et al., 2016). Other tools include neuropsychology tests such as the Immediate Post Concussion Assessment and Cognitive Testing (ImPACT), King-Devick Test, Sensory Organization Test, clinical reaction time, and others (Murray et al., 2014; Row et al., 2019).
The majority of concussion tests assess vision and visual-cognitive function post-concussion (Akhand et al., 2019), which poses a challenge for individuals who are visually impaired (i.e., those who are blind or have low vision). There are over 7.5 million people of all ages in the United States with visual impairments, and children account for at least 500,000 to 700,000 of this population (American Foundation for the Blind, 2019; National Federation of the Blind, 2019). By the year 2050, the incidence or prevalence of visual impairment numbers are projected to double to approximately 6.95 million persons with visual impairment (Varma et al., 2016).
Given that the prevalence of visual impairment is expected to rise in the next 30 years, and that assessing concussion via extant protocols requires vision, concussions may be under-recognized and under-reported in individuals with visual impairments. For example, within a review of literature, conducted by Fagher and Lexell (2014), regarding sports-related injuries in athletes with disabilities, including visual impairments, there were 25 studies yielding adequate quantitative results between 1985 and June 2013. The studies focused on Paralympic Games and other organized events for athletes with disabilities. Eight of the studies were based on Paralympic Games, including sports for athletes with visual impairment, six others included athletes with visual impairments at other venues. The review compiles an extensive list of reported injuries, but does not mention the diagnosis of concussion or TBI (Fagher & Lexell, 2014). One study included in the review (e.g., Silva et al., 2013) specifically looked at the Brazilian athletes with visual impairments participating in football 5-a-side at Paralympic Games and other international competitions between 2004 and 2008. Head injuries comprised 8.6% of the total injuries reported by body part; but, when tabulated by diagnosis, none of the reported injuries were diagnosed as concussion or TBI (Silva et al., 2013). Lack of assessment may be a significant reason for this paucity of data regarding concussion in athletes with visual impairments.
A reason for the limited amount of data on concussions and TBI in people with visual impairments may be partially due to head injury prevention adaptations that have been implemented to make sport and activities of daily living safer for individuals with visual impairments. For example, swimmer safety for an individual with a visual impairment is based on the effective use of a “tapper,” an individual who alerts the athlete as the swimmer approaches the end of the pool (Silva et al., 2013). However, a tapper alone cannot explain a lack of concussion reports in situations where there are no adaptations or other factors that reduce the risk of injury. A tapper also cannot account for situations in which head injury is reported, but there was no assessment for and diagnosis of concussion.
As can be inferred from the introduction to this report, there are currently no objective measures or biomarkers for diagnosing a concussion. Thus, identification of concussion for any person is solely based on symptom severity and performance on clinically vetted tools. Experts in concussion assessment suggest that evaluators use more than one diagnostic tool to reduce the likelihood for false negatives and false positives (Broglio et al., 2015). Using scales and checklists with tests of balance and neurocognition may indeed increase the sensitivity and specificity of concussion evaluation (Broglio et al., 2015). However, there are no current recommendations for evaluating the presence of a concussion specifically designed for an individual with a visual impairment. Given that extant protocols require visual input, the purpose of this report is to explore and describe the current literature on concussion management, analyze current practices in managing concussions in the visually impaired, and offer alternative assessments to be inclusive of individuals with visual impairments.
Methods
The databases utilized for this report included: PubMed, Web of Science, and EBSCO-CINAHL. Search terms used both singularly and combined were concussion, assessment, management, diagnosis, treatment, blind, visually impaired, and epidemiology. Available articles and concussion assessments were then analyzed to determine relevance and applicability.
Discussion of the Assessments
Summary of Concussion Tests and Information Regarding Items That Require Vision.
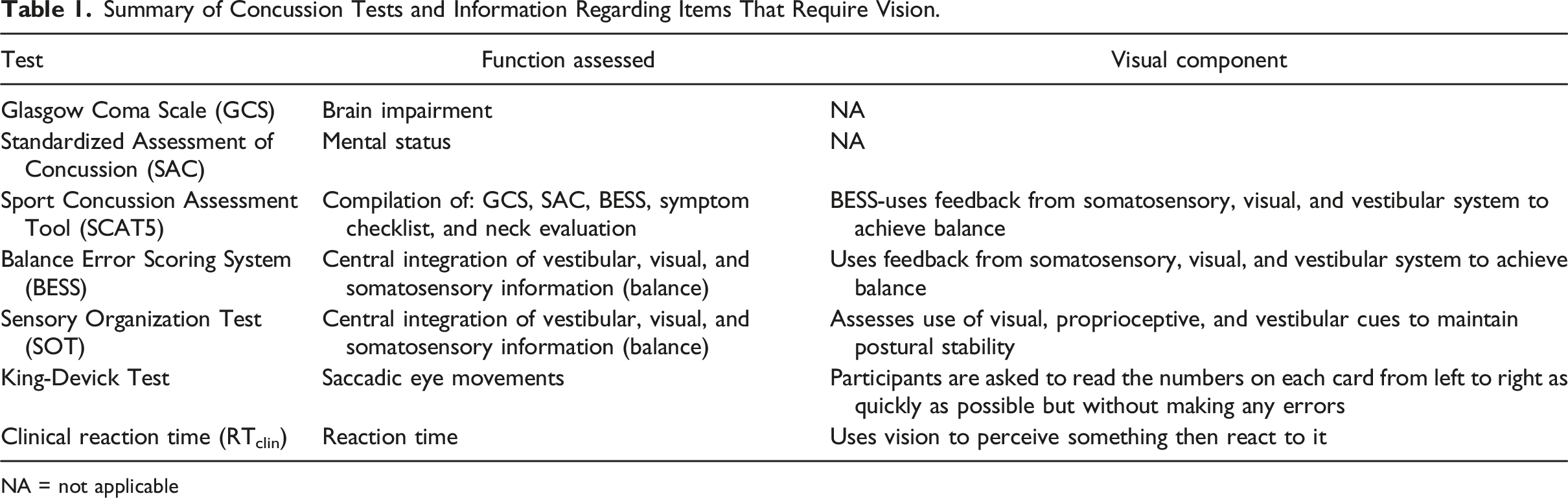
NA = not applicable
The Standard Assessment of Concussion (SAC) provides clinicians with an objective measure of mental and cognitive status, and the Balance Error Scoring System (BESS) assesses balance and coordination. Immediate Post-Concussion Assessment and Cognitive Testing (imPACT) is an objective tool used to guide return to activity decisions post-concussion. The computerized neurocognitive assessment measures memory, attention span, visual, and verbal problem solving. The King-Devick test is a rapid number naming assessment that quickly identifies impairments in eye tracking capabilities, attention, and language post-concussion. Tests of reaction time can also be used to identify and track recovery post-concussion as studies have shown a decrease in reaction time immediately following a concussive incident (see Table 1).
Many of the previously mentioned assessments described in Table 1 are visually dependent, meaning individuals with visual impairments may have difficulty completing them. Parts of the SCAT5 are able to be verbally communicated to an individual, which may be beneficial to this population. For example, Horvat et al. (2003) found that people with visual impairments use different strategies to maintain balance to trade efficiency for safety. Therefore, it may be an effective tool for concussion diagnosis in those individuals, as long as there is a baseline and normative data for comparison. Future research is needed to draw such a conclusion.
It would be valuable to develop new tools or adaptations of existing tools for concussion recognition and subsequent concussion management that are applicable to individuals with visual impairments. Evaluation of the autonomic nervous system may be one way to recognize concussion without relying on visual system signs, symptoms, and neurocognitive function. The autonomic nervous system controls heart rate, digestion, and respiratory rate. The autonomic nervous system also contributes to blood flow and supply to the brain, which increases the efficiency of the brain. Alterations in cerebral blood flow is a neurometabolic change associated with concussions.
Autonomic nervous system function can be measured using tools such as exercise intolerance tests like the Buffalo Concussion Treadmill Test (BCTT) and the Buffalo Concussion Bike Test (BCBT). The efficacy of the autonomic nervous system can be assessed with heart rate variability, the Valsalva maneuver, and head upright tilt table testing. These assessments may be a potential way to diagnose, treat, and manage concussions in athletes with visual impairments.
The Buffalo Concussion Treadmill Test has been shown to safely identify exercise intolerance as a marker of autonomic nervous system dysfunction associated with sport-related concussion without adversely affecting recovery. A study conducted by Leddy et al. (2018) concluded that exercise intolerance during the BCTT is an important indicator for predicting time to recovery from concussion and return to play. The test consists of a progressive treadmill work out where speed and incline are continuously increased. Heart rate, rating of perceived exertion (RPE), and symptoms are assessed every minute and compared to the athlete’s baseline. Testing is stopped only if the athlete reports an increase in symptoms (> 3 points from baseline symptom score) or voluntary exhaustion (RPE > 17). Although modifications of treadmill testing might be needed for athletes who are visually impaired, it is feasible, since a treadmill with additional tactile modifications can be used effectively as a tool for exercise by individuals who are visually impaired (Lieberman et al., 2019). The Buffalo Concussion Bike Test is another graded exertion test for assessing exercise tolerance after concussion. Heart rate at symptom exacerbation using the BCBT has been shown to be statistically equivalent to heart rate at symptom exacerbation using the BCTT. The BCBT may be useful for assessment of persons unable to complete the BCTT because of balance problems, orthopedic injury, or other limitations (Haider et al., 2019).
Recently, Custer et al. (2019) noted the utility of the BCTT in conjunction with other concussion assessment tools in the evaluation of a swimmer with visual impairment who had protracted symptoms after being kicked in the head during practice. Initial assessment revealed an elevated post-concussion symptom scale (PCSS) score, elevated Dizziness Handicap Inventory (DHI) which measures the impact of dizziness by measuring self-perceived handicap, and an elevated Activities-Specific Balance Confidence Scale (ABC), a self-reported measure of balance competency and confidence. The swimmer was cleared to return to play after completing the BCTT with no exacerbation of symptoms. Concurrent improvement in the PCSS and modified Balance Error Scoring System (mBESS) were also noted and considered in the return-to-play (RTP) decision (Custer et al., 2019).
To accommodate athletes with visual impairments on balance assessments, modifications may need to be made to ensure a valid assessment of their condition. The use of tactile modeling where the assessor has the athlete feel what they are doing can indicate to the athlete what the assessor wants them to do to assess their balance. Another technique called physical guidance can also be used where the assessor moves the athlete’s body through the motion can be executed to assess their balance. These two techniques along with verbal instructions have been shown to help tremendously with novel tasks (Cieslak et al., 2015).
Conclusion
In summary, the diagnosis of concussion has increased drastically in the United States; concurrent with media attention focusing on high-profile athletes and the passage of laws and policies requiring medical clearance of athletes suspected of sustaining a concussion. Although there is evidence to suggest that individuals who are visually impaired are at risk of sustaining head injuries while participating in sports and other mobility-related activities, the diagnosis of concussion may be under-recognized and under-reported in this group. Underreporting may be due to the fact that assessment of visual and visual-cognitive function is part of commonly used standardized concussion assessment tools after the injury. Thus, current assessment tools for concussion may exclude the diagnosis of concussion in individuals with visual impairments. As a result, specific accommodations are needed to effectively diagnose and manage concussions in individuals with a visual impairment. Assessments such as the DHI or ABC may be useful to assess balance and impairments of the vestibular system post-concussion. Utilizing tactile techniques to assess physical skills such as balance must also be incorporated for accurate assessment of concussions. Finally, testing for autonomic nervous system dysfunction may be useful in guiding return to sport or activities of daily living decisions in persons with blindness or visual impairment. Much research is warranted, however, to determine the effectiveness of using specific assessments and techniques on diagnosis and treatment of concussions in individuals with visual impairments. Furthermore, we suggest the creation of a concussion diagnostic specifically tailored for individuals with visual impairments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.