
Abstract
Among the many roles of the orientation and mobility (O&M) specialist is the responsibility for creating ongoing in-service education activities in O&M for teachers, other professionals, paraprofessionals (also referred to as paraeducators), administrators, parents, and individuals with visual impairments (Griffin-Shirley et al., 2000). It was further suggested that in-service activities should define the role of the O&M specialist and identify goals of the O&M program. In-service activities should also describe the roles of appropriate school personnel regarding concept and motor development, sensory skills instruction, and specific O&M techniques. Additionally, effective O&M instruction should be integrated into daily school activities, and supported and reinforced by all individuals who interact with the student (Griffin-Shirley et al., 2000). Although the use of paraprofessionals in O&M is not widespread, paraprofessionals are functioning in this role at a number of places and clarity on the appropriateness of their roles is needed (K. Zeider, personal communication, January 15, 2024).
Cmar et al. (2015) indicated that O&M specialists can incorporate “role-release” into their services by allowing other professionals to reinforce O&M skills and techniques. O&M specialists need to ensure that these individuals are prepared to serve in these roles and, as certified professionals, O&M specialists are still responsible for the management and
by answering questions on this article. For more information, visit:Earn CEs Online
A transdisciplinary team model fosters collaboration among professionals from various disciplines to assess, plan, and support a student's educational program (Fazzi et al., 2024). For O&M, transdisciplinary collaboration is often considered essential for addressing diverse needs, including those of students with additional disabilities (Fazzi et al., 2024). By integrating expertise across disciplines, team members can share roles and responsibilities, enhancing both student learning and professional growth (Bailey & Head, 1993). This role-release approach promotes a child-centered, collaborative framework in which O&M instruction is embedded in the school curriculum and reinforced by all individuals involved in the student's education (Griffin-Shirley et al., 2000; Silberman et al., 1998).
The essential purpose of professional development is to help school staff members expand their knowledge and skills, which, when applied to work, enhance job or organizational performance (Jacobs & Park, 2009). In the context of schools, enhanced job and organizational performance should result in increased student learning outcomes (Guskey, 2000; Joyce & Showers, 2002; Killian, 2002). Providing professional development for paraprofessionals is an important component of a school's improvement plan because improved student achievement is dependent on the effectiveness and contributions of all staff members (Fullan, 2005).
Professional preparation of O&M specialists began with the establishment of university programs at Boston College in 1960 and Western Michigan University in 1961. Although the following two decades saw the establishment of many additional university preparation programs in O&M, the need for services for children and adults outpaced the availability of O&M specialists (Wiener & Siffermann, 2024). Between the years 1988 and 2022, two attempts were made to develop programs to prepare O&M assistants who would work under the direction of certified professionals. The first attempt was assisted with a Rehabilitation Services Administration grant that utilized a “trainer of trainers” model (Wiener & Hill, 1993). Through this effort, educational materials were produced, and workshops were held nationwide to prepare supervisors who could then train and supervise O&M assistants. Although the program was comprehensive in nature, it failed to produce a significant number of assistants and was later abandoned. In 2004, a new attempt was made at preparing assistants by coupling academic preparation of assistants through universities with direct instruction in travel techniques provided by agencies and schools (Wiener & Siffermann, 2024). This program failed to materialize when the universities found that they did not have the resources necessary to establish courses for assistants.
A continuing shortage of O&M professionals has resulted in many children and adults receiving only intermittent instruction rather than more frequent sessions, which would better meet their needs. Most recently, the O&M Division of the Association for Education and Rehabilitation of the Blind and Visually Impaired (AER) established a Professional Issues Committee (PIC) to look again at the possibility of preparing paraprofessionals who could assist O&M specialists. By examining the previous models and a recent study administered by the Academy for Certification of Rehabilitation and Education Professionals (ACVREP), the PIC decided that preparing assistants solely dedicated to providing O&M services would be unlikely to succeed. They learned that there is a lack of funding for agencies and schools to hire such individuals. However, data from the ACVREP survey suggested that paraprofessionals who are already employed in educational settings could be trained to take on some of the responsibilities in O&M service (unpublished survey, ACVREP, 2024). The PIC therefore prepared a position paper that advocated for a program to provide O&M knowledge and skills to paraprofessionals and related personnel who are already embedded within the service delivery systems.
The next step was to determine what roles these individuals might assume in assisting O&M specialists. Previous attempts at establishing roles for paraprofessionals were made by the authors of position papers that were authorized by the AER O&M Division. These had been created by consensus of the PIC, which only consisted of 5‒7 members. To truly represent the thinking of the field of O&M, it was decided that a more representative method was needed to develop a list of role responsibilities and, thus, the idea of a Delphi study was born.
A Delphi study is a research method that uses questionnaires through multiple rounds to gain consensus on a topic with varied perspectives. Experts are asked to provide ratings and explanations over multiple rounds allowing differing views to be shared and discussed (Hsu & Sandford, 2007). These additional rounds allow participants to reevaluate their ratings based on the feedback provided by other participants. A set level for consensus should be established and any statements reaching this threshold would be removed from additional rounds. For items that do not reach this level of consensus, the amount of change (minimum of 20%) in the ratings would be used to determine if it should be included in further rounds. If no further change is expected, then there may not be a need for additional rounds.
In many Delphi studies, a predefined threshold percentage is not specified (Foth et al., 2016). When explicitly defined, the appropriate percentage for consensus in a Delphi study still varies across different research fields and individual studies. In systematic reviews of Delphi studies, which identified percent agreement as the most common method for defining consensus, the median threshold was 75% (Diamond et al., 2014; Foth et al., 2016). However, the acceptable percentage can differ based on the study's context and objectives, with reported thresholds ranging from 50% to 97% (Diamond et al., 2014). Researchers should establish the consensus threshold in advance, considering the specific goals and requirements of their study.
The current study used a modified Delphi approach while maintaining the key indicators for quality Delphi research including: specific criteria for consensus, pre-planned for a set number of rounds of responses with the degree of change in participant responses determining if further rounds were needed, and clear selection criteria for participants (Diamond et al., 2014; Jandhyala, 2020). This study used a modified Delphi approach that differed from a traditional Delphi study since items to be evaluated were provided to the participants in the first round and were not generated by the participants themselves. This study also differed from a traditional Delphi by using multiple panels of experts instead of a single group. Delphi studies may use multiple panels of experts allowing results to be compared based on expert background with at least 10 members per panel or group (Okoli & Pawlowski, 2004). Non-iterative, parallel surveys for multiple groups were also used in established Delphi research on functional vision assessments (Kaiser et al., 2020) and describing competence in literary braille (Lewis et al., 2012) consistent with this modified Delphi approach.
Methods
Instrument
The authors developed two parallel questionnaires for a modified Delphi study using an online survey tool. A separate survey was created for each group of participants. One group consisted of university instructors who will be referred to as “instructors” for the rest of this paper. The other group consisted of O&M professionals who are direct service practitioners and will be referred to as “practitioners” for the remainder of this article. There is a range of perspectives on this topic, and the authors wanted to better understand the specific points of view of the university instructors and experienced practitioners. Using separate groups allowed the authors to compare the sources of the comments and results when consensus was and was not reached. By incorporating separate groups, the authors were able to include all of the participants’ comments in the next round of the survey while also keeping it a manageable length to reduce attrition.
An initial assessment questionnaire was developed based on a list of competencies from the Atlantic Provinces Special Education Authority (APSEA, 2019) O&M Delivery Guidelines. These guidelines were originally created as a resource for teachers of students with visual impairments within the APSEA regarding the provision of O&M services in a team capacity. As these guidelines were only used internally, they were not based on research or peer review. The authors reviewed the competencies and expanded the list where necessary. This list was compared against established resources and textbooks (Fazzi & Barlow, 2017; LaGrow & Long, 2011). Two additional professionals with over 40 years of total combined experience were asked to review the competencies and provided additional feedback. The survey asked the participants to rate the appropriate role of a paraprofessional regarding 32 basic indoor skills, 23 advanced indoor skills, and 25 outdoor skills. Participants were asked to rate and provide comments on each skill for the appropriate role that a paraprofessional could serve using the following definitions:
teaching = teaching the technique or procedure independently; reinforcing = reinforcing after instruction is provided by an O&M specialist; and not appropriate = not appropriate for a paraprofessional.
Several open-ended questions were included asking for additional feedback and input on the survey. Participants provided comments and feedback throughout the survey allowing opportunities for them to include any skills or competencies that were not addressed. There were no additional items that were consistently identified. These paraprofessionals might be school paraprofessionals, rehabilitation service providers, related service providers, residential staff, and others. The individual would have undergone specific preparation related to appropriate O&M knowledge and skills and would be under the guidance of a certified or licensed O&M specialist. For the purposes of this survey, we were considering these O&M skills for individuals of all ages.
Participation and Recruitment
The study was approved by the institutional review board at the University of Kentucky and informed consent was received from all participants. Individual email requests were sent to the coordinators of 20 university O&M programs in the United States and Canada asking for faculty members to participate and to recommend three O&M practitioners to serve in an expert role.
Instructors
University instructors were required to (a) teach or have taught multiple O&M courses at a university within the last 3 years; (b) understand the program enough to accurately represent the O&M coursework (techniques, methods, and collaboration content); (c) and hold certification in O&M, such as Certified Orientation and Mobility Specialist (COMS) through ACVREP or National Orientation and Mobility Certification (NOMC) through the National Blindness Professional Certification Board (NBPCB).
Practitioners
Professionals participating in the survey were required to (a) have worked as an O&M specialist for at least 5 years; and (b) have current certification in O&M (e.g., from ACVREP or NBPCB).
Data Collection
Participants completed two rounds of questionnaires from January to April 2024. In round 1, participants were asked to identify the appropriate role of a paraprofessional regarding each of the specified skills while also providing a rationale for their rating. In round 2, participants were provided information on the skills where 70% consensus was reached, but they were not asked to rate these skills again. Then participants were asked to again rate each of the skills where 70% consensus was not established while reviewing the additional explanations provided by the other participants for their rating from round 1. For skills that did not reach consensus after the second round, there were minimal changes from round 1 to 2. The authors determined that a third round was unnecessary and unlikely to provide further agreement.
Following round 1 of the survey, responses in support of a teaching role for paraprofessionals were minimal, except for a few select skills. The authors evaluated these results in preparing for round 2, since a teaching role in O&M for paraprofessionals seemed nearly impossible. It was determined that the ratings for a “teaching role” could also apply to a “reinforcing role,” since there is less responsibility and risk in a reinforcement role. Therefore, round 1 ratings for “teaching” were counted in addition to the ratings for “reinforcing” to simplify the number of skills that still needed to be evaluated in round 2. Additionally, in round 1, participants were asked to rate the appropriate role of a paraprofessional for “bus travel.” Although this item did not reach consensus, participants had different interpretations of this skill—whether the bus in question was a public bus or a school bus and whether the travel involved was to familiarize the student with the location of the parked school bus or if it was to actively use a public bus traveling along a designated route. The authors clarified the roles related to “bus travel” in round 2 by including the skills “using public bus transportation” and “familiarization to a parked bus, thus increasing the total number of outdoor skills by one.
Results
Fifteen instructors from 13 university O&M programs participated and completed round 1 of the survey. Of the instructors (N = 15), 40% (n = 6) had been teaching at the university level for at least 15 years, and 20% (n = 3) respectively from each range of 1‒5 years of experience, 6‒10 years of experience, and 11‒15 years of experience. There were 14 university instructors who completed the survey in round 2. Participant numbers decreased from round 1 to round 2 due to a lack of response from instructors and practitioners who had completed round 1.
Twenty-one practitioners, who graduated from 11 different O&M programs, participated and completed round 1 of the survey. In round 2, there were 17 O&M practitioners who completed the survey. Of the practitioners, 4 had worked with an O&M assistant previously. When asked about the population that they primarily serve, 16 practitioners worked more with children and 5 worked more with adults. Of the practitioners group, 25% (n = 5) had between 6 and 10 years of experience, 20% (n = 4) had from 11 to 15 years of experience, and 55% (n = 11) had 15 or more years of experience.
All university instructors and O&M practitioners held COMS certifications from ACVREP. No NOMC professionals or university instructors participated in the study. This study was intended to represent perspectives and practices for the United States and Canada. Two university faculty members participated from the two respective universities in Canada that have O&M programs. No Canadian practitioners participated in the study.
Consensus was reached identifying a reinforcing role for a paraprofessional could be appropriate for 48 of the 55 indoor skills and only 4 of the 25 outdoor skills. Table 1 shows all of the 52 skills where 70% agreement was reached for a reinforcement role in either round from both university instructors and practitioners. In round 1, 46 out of 55 indoor skills and only 6 out of the 24 outdoor skills were able to reach 70% consensus regardless of the rating and role. Both groups reached consensus on 11 of the remaining 28 skills in round 2.
Skills for Which Both Instructors and Practitioners Reached Consensus on Reinforcement Role
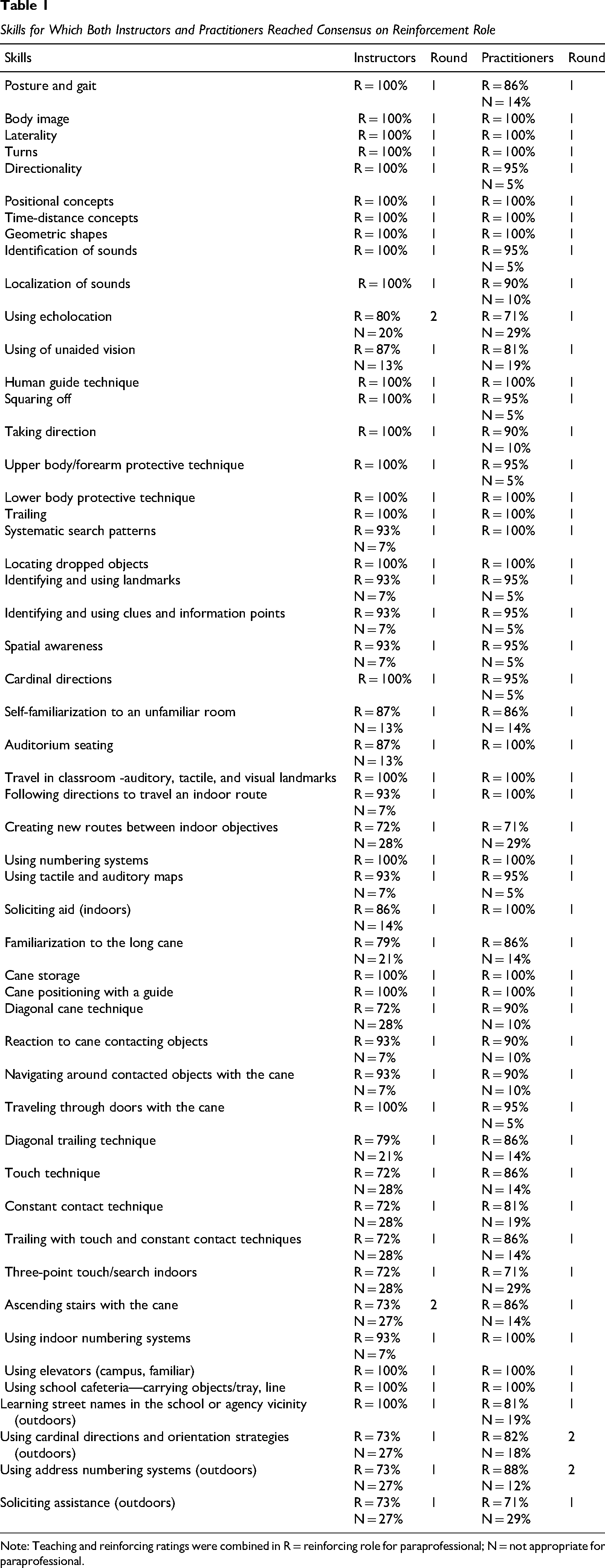
Note: Teaching and reinforcing ratings were combined in R = reinforcing role for paraprofessional; N = not appropriate for paraprofessional.
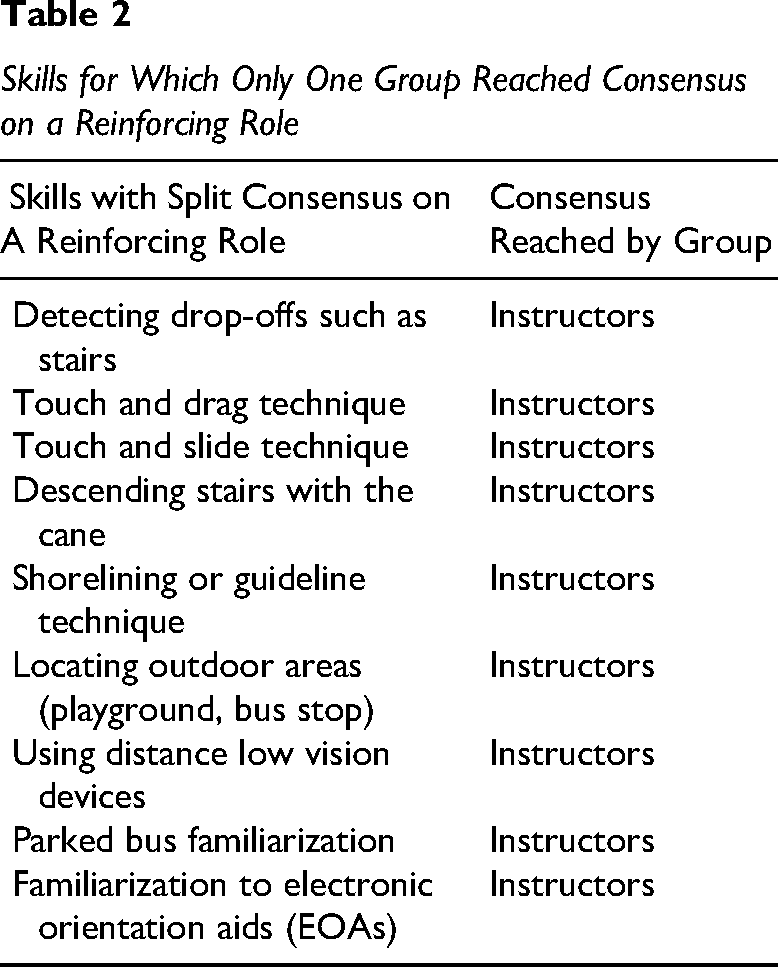
Table 2 shows the skills for which consensus was reached for one of the groups only. For all nine of these skills, consensus was reached in the practitioner group but not the university instructor group.
Skills for Which Only One Group Reached Consensus on a Reinforcing Role
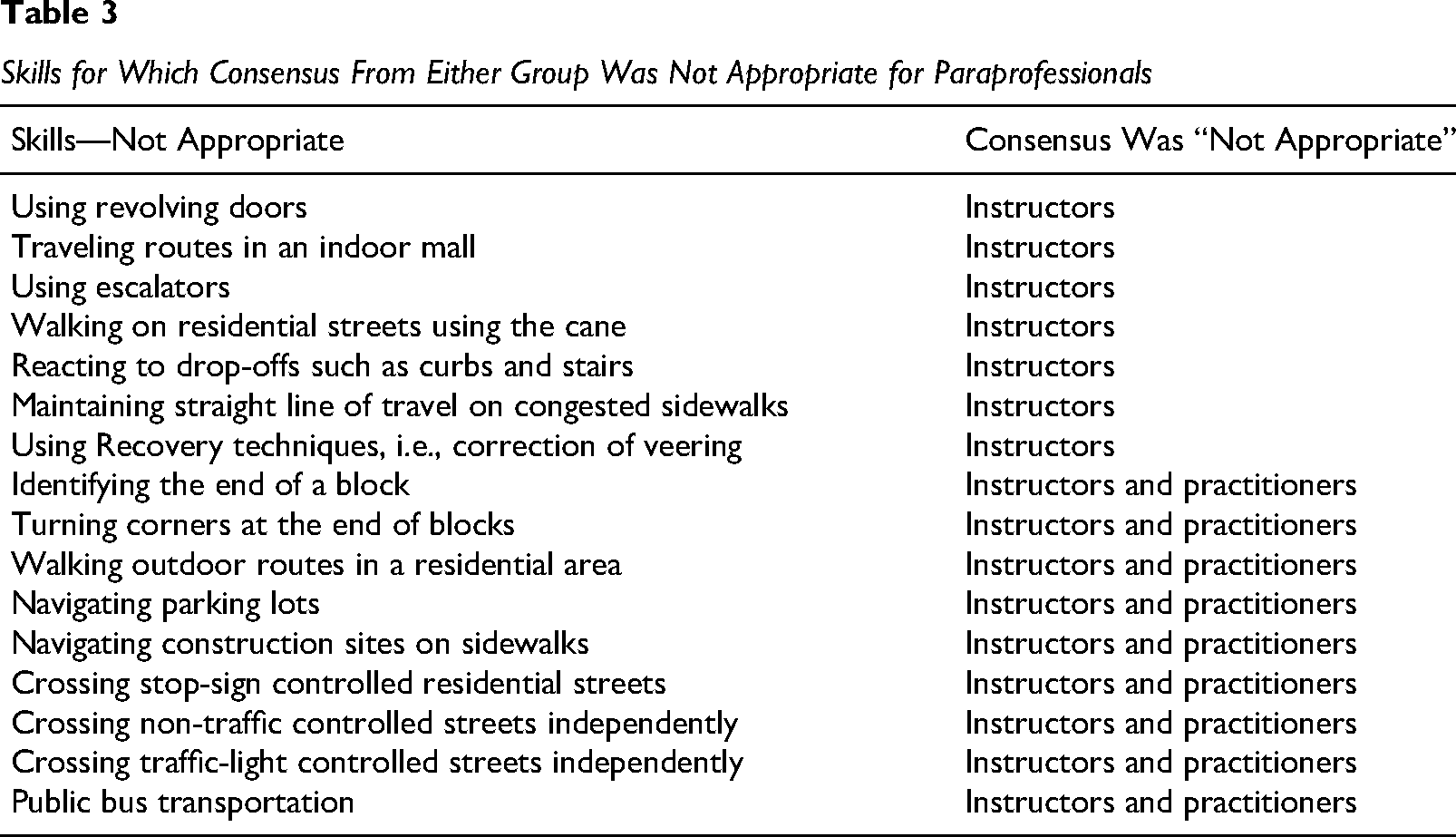
The authors grouped all the single-group and both-group consensus ratings of “not appropriate for a paraprofessional” together, since this was enough of an area of concern that it should be discussed separately (see Table 3). There were 16 skills for which at least one group reached 70% consensus, 9 of which included both groups, that it was “not appropriate for a paraprofessional” to have the role.
Skills for Which Consensus From Either Group Was Not Appropriate for Paraprofessionals
Discussion
This discussion is based on the results of this study and the authors’ experiences. The use of paraprofessionals in O&M will allow children and adult consumers to gain additional practice in between lessons provided by O&M specialists. Reinforcement of the various concepts and skills specified in this document would provide an enhanced experience for the learner. Such reinforcement would help them maintain their skill level, rather than having to relearn the material after being away from it for a period of time. Initially, the O&M specialist would have to invest time in the preparation of the paraprofessional. However, eventually, the advantage for the professional would be to execute a more efficient means of delivering services.
The response from university instructors and O&M professionals was clear in the reserved and limited reinforcement role they supported for paraprofessionals regarding O&M services. Although the university instructors were more conservative in their ratings than the practitioners, it was good to see that the groups were mostly aligned in their responses. Participant comments highlighted many of the factors contributing to this conservative approach. It has been assumed that the O&M specialist would provide in-service instruction to the paraprofessional. Given the current shortage of professionals and overflowing caseloads, it is an appropriate question to consider whether the O&M specialist has time to provide in-service instruction and whether the need to add this activity would actually help reduce their workload.
Although using a paraprofessional for O&M services might enhance the service, it will not solve the issue of shortages of O&M services. In addition, although collaboration with related service providers is covered in university programs, concerns were expressed by participants that many individuals who work with people who are blind or have low vision are not currently equipped to take on the task of providing O&M instruction. Most university programs teach aspects of collaboration and managing risk or liability, but supervising paraprofessionals in a continual reinforcement role is more than can be covered within the current O&M coursework in addition to the other necessary content. It should be noted that supervision of O&M interns is much different from supervising paraprofessionals in an O&M context, since interns have already completed an established set of academic standards and content.
There are many areas that require further research and investigation to determine the most appropriate and effective way to implement a program for paraprofessionals supporting O&M services. Research should establish whether a clear and measurable connection exists between additional practice, reinforcement, and specific outcomes for students or clients. Additional research should determine the appropriate details necessary for a comprehensive program for preparing paraprofessionals to support O&M services.
Supervision, Risk, and Liability
Liability and risk are primary concerns when considering O&M instruction and assigning the reinforcement of O&M skills to paraprofessionals. The O&M specialist would need specific supervisory abilities to appropriately prepare and oversee an O&M paraprofessional's reinforcement of O&M skills. According to the ACVREP code of ethics for COMSs (3.7; 2024): When planning or using alternative or new methods for instruction (e.g., remote supervision, role release, group instruction), the COMS will consider the safety and the best interest of the client, impact on team members, ethical implications of the method based on ACVREP standards, consultation with relevant professionals and jurisdiction regulations. (p. 14)
To afford the O&M specialist those needed skills, additional in-service instruction opportunities should be made available to them. Administrators will need to understand and support the O&M specialist and the paraprofessional within a reinforcement role and not an instructional role. The field of O&M needs to evaluate whether there could be standardized preparation of paraprofessionals. In the future, the field may want to consider writing guidelines for utilization of O&M paraprofessionals. The materials from the first study on O&M assistants would be useful in such a publication (Wiener & Hill, 1993).
Certified O&M specialists are the best individuals to be able to judge a paraprofessional's suitability to reinforce O&M principles, which specific O&M skills they could cover, and with which specific students they could appropriately work. This practice cannot be rigidly managed or defined for all circumstances. Within the established guidelines, it may be appropriate for a paraprofessional to have a larger or smaller role, depending on the situation, to increase effectiveness, encourage student independence, and minimize risk. As one participant explained: Almost every answer to this survey is dependent on the type, scope, and quality of the proposed paraprofessional training. A requirement to approve the paraprofessional's role on a student-by-student and skill-by-skill basis may be necessary, as our diverse population makes it impossible to provide blank statements, and what may be very appropriate for one student may be out of the question for another, even for the same skill (e.g., when additional impairments add complexity to the situation).
This model for an O&M paraprofessional places significant responsibility on the O&M professional. It would be ideal for a contract to be established between the O&M specialist and paraprofessional to reduce liability and clearly identify what skills and what a reinforcing role should look like. A clearly defined job description would need to be part of this agreement. The O&M specialist should evaluate, introduce, teach to an accepted level of practice of the O&M skills before assigning a paraprofessional the task of reinforcing the O&M skill. The paraprofessional would reinforce O&M skills under the direction, guidance, and ongoing monitoring by the O&M specialist. The O&M specialist would provide in-service instruction on the individualized application of O&M skills. The paraprofessional would observe the O&M specialist during the O&M lesson to ensure consistency.
Limitations
The O&M skill ratings did not consider the age, physical or mental abilities, or disabilities of the student or client. O&M skills are used within different environments and have various levels of difficulty depending on the application. The current study did not rate all the O&M skills within the application of indoor or outdoor environments; familiar or unfamiliar environments; nor did it identify when the student or client had mastered the learning of the skill. The results should only be applied to practices involving COMS and services in the United States and Canada.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.