
Abstract
Anxiety and depression are the two most prevalent mental health issues in general medical settings and important contribution to the worldwide disease burden (Vos et al., 2020). At least 2.2 billion people globally experience either near or distant vision impairment (World Health Organization, 2023). Projections indicate that by 2050, the global population will include approximately 61 million individuals who are blind and 474 million who will experience moderate to severe visual impairment (Bourne et al., 2021). Depression and anxiety are highly prevalent among adults with visual impairments, one-third of middle-aged and older adults with blindness or low vision have experienced depression or anxiety (Virgili et al., 2022). Studies have shown that if left untreated, mild depression can elevate the risk of progressing to major depressive disorder (Fogel et al., 2006), which can result in increasing disability, a lower quality of life, deteriorating health, and even death. However, previous research shows that people with visual impairments regularly pay more attention to physical symptoms than to their mental states. One-third of rehabilitation professionals and two-thirds of ophthalmic care providers do not focus on assessing their clients’ mental states (Nollett et al., 2019).
Both individuals with visual impairments and healthcare providers may overlook the effect of vision loss on mental health, leading to inadequate screening and treatment for anxiety and depression in this group (Van Munster et al., 2022). Consequently, depression and anxiety are frequently undetected (Holloway et al., 2015). Identifying and addressing depression and anxiety within the blind community can aid in early intervention and treatment, preventing exacerbation of the condition.
In early interventions for depression, nonpharmacological methods have been shown to be preferable, with limited negative effects (Salihu et al., 2021). Music therapy, for instance, has been demonstrated to alleviate psychological depression (Fancourt & Finn, 2019). Over the past decade, research on the health benefits of music has expanded rapidly (Chair et al., 2021; Croom, 2015; Moss, 2019). However, the integration of music therapy with traditional musical instruments remains a relatively small field of research. The African hand drum, a percussion instrument with deep roots in African history, is renowned for primal, passionate, and rhythmic melodies. Striking the drum with palms and fingertips creates unique rhythmic vibrations that evoke a sense of primal power and dynamic energy. These tactile rhythms and auditory stimuli significantly influence both physical and mental states (Durojaye, 2017). The integration of African hand drumming therapy represents a vibrant and engaging therapeutic approach within music therapy, stimulating individual creativity, releasing inner stress, and enhancing quality of life through drumming and subsequent verbal guidance (Flores, 2012).
Despite the variety of hand drums available, including Conga and Bougarabou, the research team chose the Djembe after doing a preliminary literature assessment and experimentation. The Djembe is a West African goblet drum that is known for its crisp, resonant sound and rich tonal range, making it ideal for solo and ensemble performances. Its unique rhythms, vibrations, and portability enhance emotional expression and aid in stress relief (Smith et al., 2014).
Cultural sensitivity was a key consideration in the project design. The research team included a music therapist and an assistant with professional training in African drumming, who have accumulated extensive experience in practice. Their expertise ensured that the implementation process fully respected the cultural and religious significance of the instrument. Through this approach, the project aimed to harness the therapeutic effects of the Djembe while avoiding any misappropriation of cultural elements.
Based on the premise of exploring additional music therapy approaches that integrate traditional instruments, researchers have proposed the therapeutic scheme incorporating African hand drums. This research involves a music therapy program utilizing an African hand drum, the Djembe, with members of the community at the Hamilton branch of Blind Low Vision New Zealand for a collective hand drumming therapy experiment.
A total of 18 people with visual impairments who exhibited depressive tendencies, all of whom volunteered, were recruited for the current study. The research team subsequently randomly assigned these 18 individuals into an intervention group and a waitlist control group, with nine participants in each group. The control group underwent Patient Health Questionnaire-9 (PHQ-9) assessments concurrently with the intervention group. The program spanned 6 months, with one session per month, and employed a mixed-methods approach to evaluate treatment outcomes. This research aimed to explore whether the rhythmic, repetitive drumming of the Djembe African hand drum can initially alleviate depressive symptoms among blind individuals. The goal was to provide people with visual impairments with a safe outlet for emotional expression and for managing stress, anxiety, and trauma, thereby promoting early intervention and treatment.
Methods
Participants
To participate in the research, individuals who are blind or have low vision needed to perceive themselves as having depressive tendencies, with symptoms such as high stress and anxiety levels. This study received approval from the The University of Waikato Human Research Ethics Committee HREC (Health) under protocol number 2022#02 and the participant consent form had been signed by Blind Low Vision New Zealand, Hamilton branch.
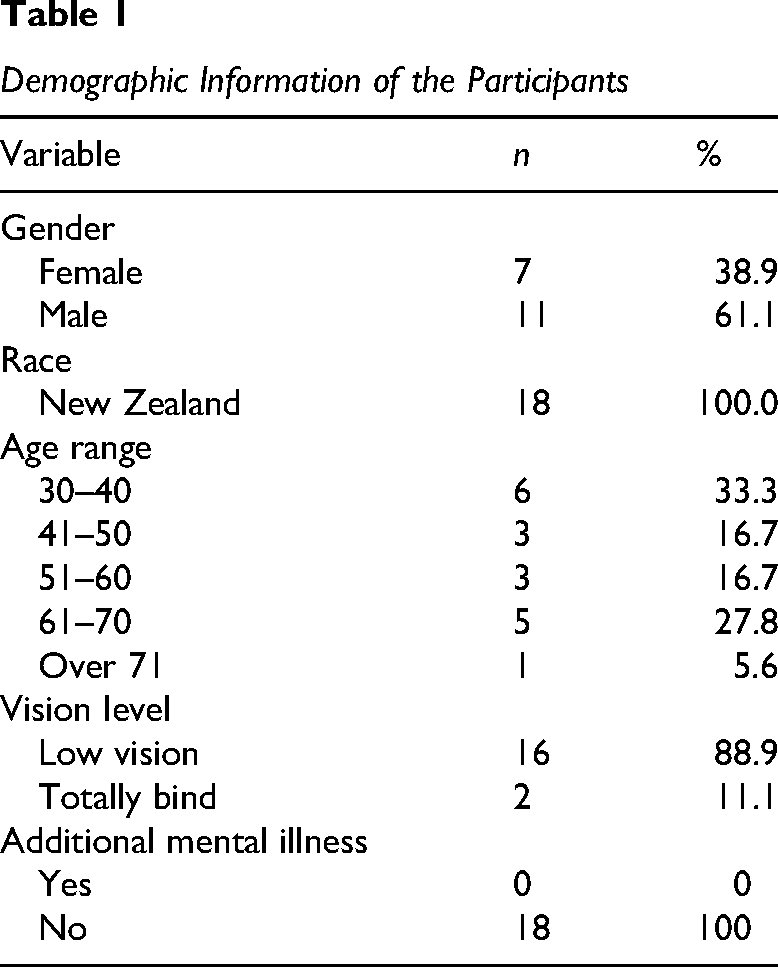
The sample consisted of 18 Blind Low Vision New Zealand members with visual impairments who were participating in African hand drum therapy. Among them, 16 had low vision and two were totally blind. The participants were between the ages of 31 and 72 years (M = 50.22, SD = 14.22). Table 1 shows the additional demographic information.
Demographic Information of the Participants
Procedure
Since this research specifically targeted the population with visual impairments in New Zealand, the research team selected the Blind Low Vision New Zealand Hamilton branch as the target group. Blind Low Vision New Zealand operates as a member-led organization under the governance of the Royal New Zealand Foundation of the Blind, offering both practical assistance and emotional support to people with visual impairments. The members, ranging in age from early childhood to old age, have varying degrees of visual impairment, from low vision to total blindness (Blind Low Vision NZ, 2024). Before therapy, individuals with visual impairments who identified as having depressive tendencies provided electronic informed consent with researchers’ assistance and then completed a demographic survey. The hand drum therapy spanned approximately 6 months, commencing on June 27, 2024, and continuing until November 14, 2024, with group interventions conducted once a month. This article presents a detailed record of the intervention process along with an analysis of its therapeutic effects.
Considering that participants from the blind community may require additional time for adaptation and understanding, each session lasted 40 to 60 min. The location was in the Blind Low Vision New Zealand Hamilton branch community activity room. The specific schedule was as follows: In the first session, the facilitator gave a 10min briefing, welcoming participants and outlining the therapy, including the African drum's history and treatment procedures. In subsequent sessions, the initial 10 min were dedicated to a review of the intervention content, including an introduction to the hand drum and basic drumming techniques. Next, participants spent 10 min exploring the drum's texture and sound, familiarizing themselves with basic rhythms through auditory and tactile experiences. This exploration period was followed by a 15min group creative activity led by the facilitator, focusing on stress relief through music. Finally, the session concluded with 10 min of verbal guidance from the facilitators, followed by a 10min sharing session with the participants.
Each intervention session was divided into several standardized phases to ensure a consistent treatment experience while acknowledging individual differences. At the beginning of each session, the facilitator welcomed the participants and briefly introduced the session's objectives. In the first session, a brief introduction to the cultural and historical significance of the Djembe African hand drum was provided, along with an explanation of its traditional role in therapy. For subsequent sessions, the pre-intervention phase served as a review of previous experiences and a reinforcement of key drumming concepts.
The core phase of each session was dedicated to a standardized demonstration of drumming techniques and an experiential performance led by the facilitator. In every session, the facilitator played background music in various styles and combined different striking techniques and hand positioning, with particular emphasis on demonstrating how to produce bass and tone sounds. This demonstration was accompanied by verbal cues designed to maximize understanding among participants with visual impairments. Although the level of individual participation varied, the facilitators ensured that every participant received comprehensive and consistent guidance.
Regarding the implementation settings and process, the hand drumming therapy sessions were held in the activity room at Blind Low Vision New Zealand Hamilton branch. The space was arranged simply, providing side-by-side seating with participants sitting in a semicircle around the facilitator (see Figure 1). Each participant was equipped with a hand drum. Due to the flexibility of moving the hand drums, both the height and position of the drums were adjusted according to each participant's needs: The drums were either placed on the floor or positioned between the participant's legs. Prior to the practice, the facilitator provided technical guidance, explaining the basic drumming rules (drumhead and drum rim) and demonstrating the appropriate playing techniques. Throughout the process, the facilitator made adjustments based on participants’ responses and controls the tempo of the rhythms. In addition, because the participants were people with visual impairments, all forms were administered verbally by the research team.

Participants Sitting in a Semicircle Around the Facilitator
Measures
Feasibility
Feasibility measures include participants’ involvement in the intervention and the assessment of depressive symptoms. Two researchers monitored fidelity by observing the hand drumming therapy process, including the duration of activities, completion status, and any issues that arose during implementation. Both researchers were highly familiar with the intervention and played an important role in the adaptation process for the participants with visual impairments. One researcher led the African drum therapy practice, while the other observed each participant's engagement during the practice.
Following the demonstration of the facilitator, participants entered a guided practice phase, where they were encouraged to replicate the techniques. During this period, the facilitator circulated among the participants, providing feedback and corrections to ensure adherence to the standardized protocol. This period was followed by a collective performance activity aimed at promoting coordination and group participation. This final stage, which emphasizes improvisational drumming, represents the most crucial component of the session.
After the background music was played, participants were free to perform according to individual interpretations and interactions with others. Participants made choices regarding whether to incorporate bass or high tones and whether to strike the drumhead or the rim, all while remaining within the overall musical framework.
This study utilized the PHQ-9 to assess depressive symptoms (Kroenke et al., 2001). The PHQ-9 is a widely utilized depression screening tool that includes nine questions representing different symptoms and levels of depression. Measurement and comparison rely on symptom frequency before and after the therapy, such as “little interest or pleasure in doing things.” Participants respond to these questions using a 0 to 3 scale (0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day). The PHQ-9 demonstrates evidence of construct validity, external validity, and reliability (Kroenke et al., 2001), making it suitable for participants visual impairments. The PHQ-9 questionnaire used in this research was modified in wording to accommodate the people with visual impairments. Before each session, both the intervention and control groups completed the PHQ-9 to assess their emotional state and life status over the past 4 weeks, evaluating the intervention's sustained effects. Additionally, after each session, the intervention group completed a slightly modified version of the PHQ-9 to evaluate the immediate effects of the intervention. Supplemental Appendix 1 contains the depression assessments conducted on patients both before and after treatment.
Acceptability
The research team utilized both quantitative and qualitative methods to assess participants’ acceptance of the hand drumming therapy. To reduce the burden on participants (i.e., excessive form-filling), the research team conducted two quantitative evaluations throughout the intervention process. One was administered immediately after the first session, and the other immediately after the final session (see Supplemental Appendix 2). The quantitative assessment covered several aspects: engagement, participant behavior, the relevance of the activity, and overall satisfaction with the project. The User Engagement Scale's Engagement Subscale was used to assess engagement (O’Brien & Toms, 2010). Participants rated their level of engagement and experience in various aspects of the African drum therapy on a five-point scale (1 = strongly disagree and 5 = strongly agree).
The qualitative assessment in the project included five semistructured open-ended questions addressing: (1) the effect of the African drum therapy on alleviating depression and anxiety, (2) the effectiveness of the African drum therapy project in promoting relaxation and emotional expression, (3) the most helpful aspects of the project, (4) the least helpful aspects of the project, and (5) suggestions for improving the project.
Data Analysis
The research team calculated descriptive statistics for the African hand drum therapy program to examine participant characteristics, changes in depression levels before and after the therapy, and acceptance ratings. They computed the duration of each session, the overall intervention time and the number of items covered. The team documented all special issues that arose during the therapy. For the open-ended questions in the survey requesting participant feedback, two researchers categorized responses as positive, negative, neutral, or suggestions for improvement. The researchers then discussed and resolved any discrepancies or shortcomings, implementing adjustments for the next therapy project.
Changes in PHQ-9 scores were analyzed using a paired sample t-test. The total score was calculated by summing responses to all nine questions. A higher PHQ-9 score reflects greater depressive symptoms, with a scale ranging from 0 to 27. The analysis of PHQ-9 scores focuses on three aspects. First, the longitudinal changes before and after each intervention are examined to assess immediate effects. Second, cross-sectional comparisons between the six interventions are conducted to evaluate sustained effects. Finally, comparisons between the intervention group and the control group are performed to test intergroup differences. Together, these comparisons aim to assess both the immediate impact and the sustained effects of the therapy on participants’ depressive symptoms.
Results
Feasibility
Across the six sessions of African hand drum therapy, all nine participants with visual impairments were involved. Each session lasted between 45 and 60 min, yielding a total intervention time of approximately 315 min. Although minor deviations occurred during some sessions, for instance, the start time was slightly delayed due to a blind community meeting scheduled between morning tea and lunch, the intervention generally adhered to the planned schedule and virtually all intended content was covered.
During the implementation, no issues significantly affected the session's progress. Occasional interruptions from screen readers or environmental noise occurred but did not substantially affect the flow of the activities. Participants contributed by sharing techniques for drumming, playing a role in mutual assistance. This informal technical support was present throughout the project, though each instance was brief and appeared only in individual interactions. During the activity, other minor issues were noticeable, such as some difficulty with open-ended discussion topics post-therapy, which required verbal guidance from the facilitator.
Data Analysis
Firstly, to assess the immediate effect of each intervention, a paired-samples t-test showed a significant decrease in PHQ-9 scores from before to after the intervention. For instance, during the first intervention, the mean PHQ-9 score for the nine participants decreased from 5.67 ± 0.71 before the session to 3.78 ± 1.72 afterwards, with an average difference of −1.89 ± 1.17. Paired t-test results yielded t(8) = –4.85, p < .002, Cohen's d = –1.62, indicating that patients’ depressive symptoms improved significantly following the intervention, demonstrating a strong immediate effect (see Table 2). However, during the second intervention, the mean PHQ-9 score rebounded from 3.78 to 4.44 and then gradually decreased, suggesting that overall treatment efficacy improved cumulatively over time. This trend also indirectly underscores the significant effect of the first intervention on the participants (see Figure 2). Moreover, the immediate effects of the first three interventions were significant and relatively stable, with effect sizes ranging from 1.06 to 1.62. The effect of subsequent interventions gradually diminished. After the third intervention, from the fourth session onward, the effect size dropped below 1. Immediate improvements became stable and further diminished in magnitude. PHQ-9 scores continued to decrease in the last three sessions, but the differences did not reach statistical significance (see Table 2).
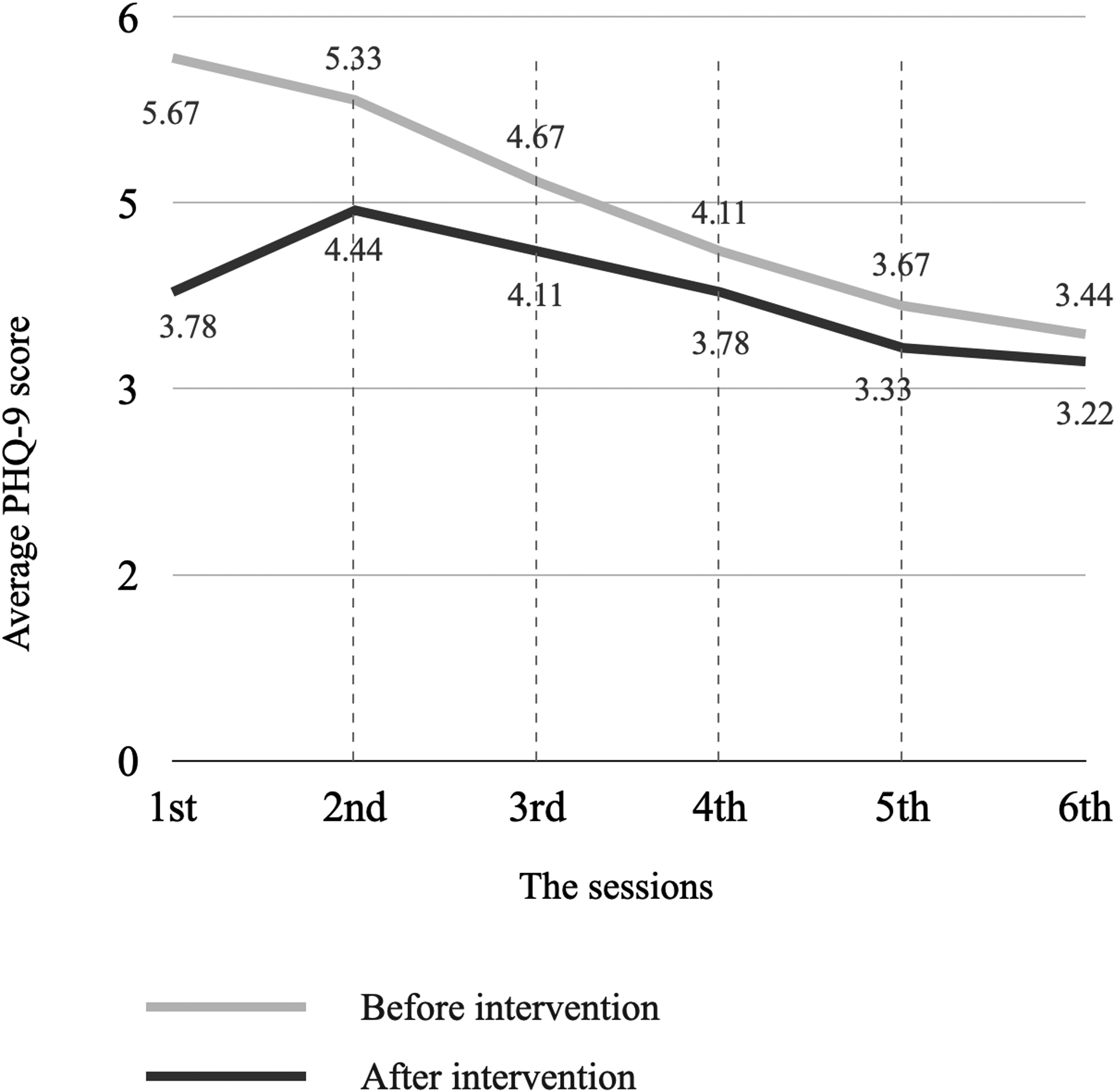
Changes in Average PHQ-9 Scores Before and After Intervention Over Six Sessions. PHQ-9= Patient Health Questionnaire-9
Summary of PHQ-9 Scores, Mean Differences, and Effect Sizes (Cohen's d) Across Six Intervention Sessions
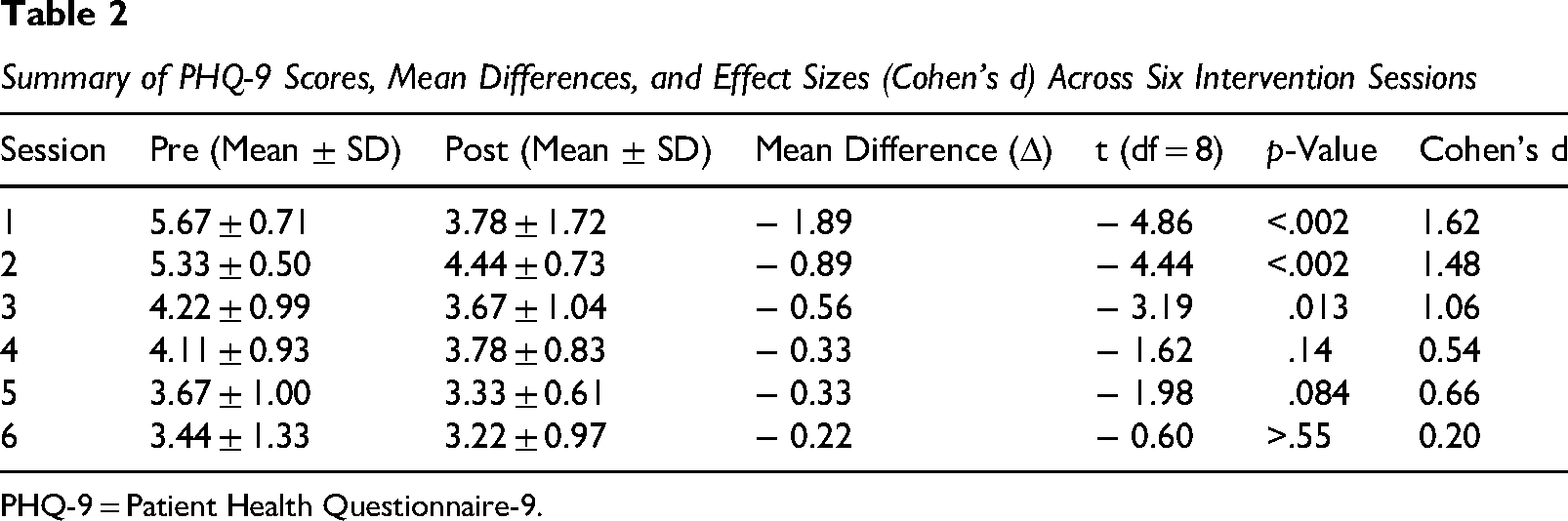
PHQ-9 = Patient Health Questionnaire-9.
These results indicate that the intervention group exhibited marked immediate improvements in the early sessions. As the intervention continued, baseline PHQ-9 scores gradually declined, and the magnitude of immediate improvement decreased. This pattern may reflect that participants’ depressive symptoms stabilized or approached a floor effect after early improvements (see Figure 3).
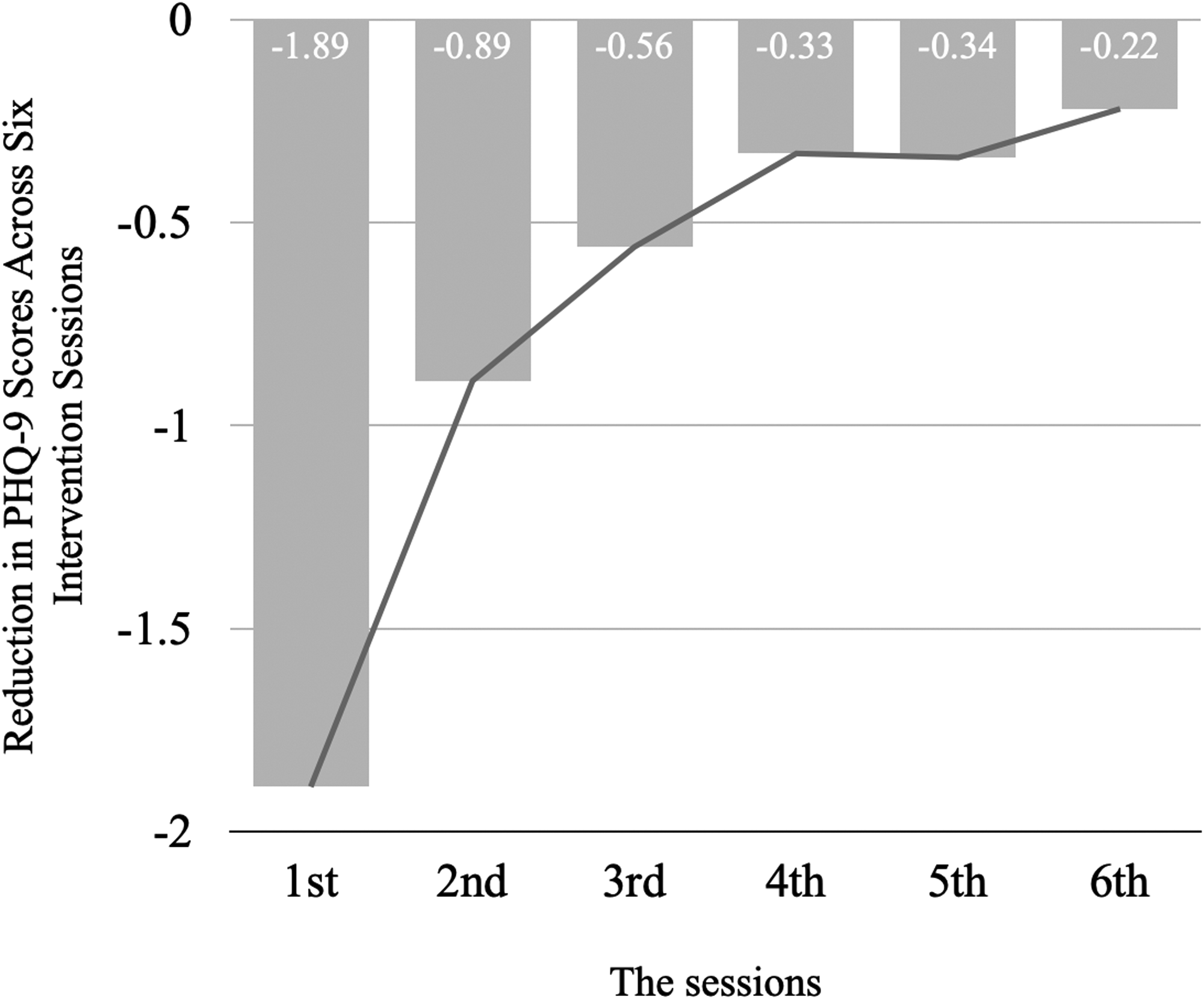
Reduction in PHQ-9 Scores Across Six Intervention Sessions. PHQ-9=Patient Health Questionnaire-9
Secondly, regarding the between-session comparison across the six interventions, a repeated measures analysis of variance (ANOVA) indicated a significant time effect on baseline PHQ-9 scores—F(5,40) = 12.37, p < .001, η2=0.61—indicating a cumulative improvement effect of the African hand drumming therapy. Further linear regression analysis showed that, on average, the baseline score decreased by 0.45 ± 0.07 points with each intervention (β = −0.45, SE = 0.07, t = –6.01, p < .001), which further supports this conclusion. These results demonstrate that, as the intervention progresses, the baseline PHQ-9 scores of the participants gradually decline, reflecting a cumulative improvement in depressive symptoms over the long term.
Furthermore, a comparison was conducted between the intervention and control groups. At the first measurement, the intervention group had a mean PHQ-9 score of 5.67, while the control group's mean score was 6.00, indicating that both groups were relatively well-balanced at baseline, thereby providing a reliable basis for subsequent comparisons. However, over the course of six interventions, the baseline PHQ-9 scores in the intervention group exhibited a clear downward trend, decreasing from 5.67 to 3.44, whereas the control group's scores remained relatively stable or even slightly increased from 6.00 to 6.89 (see Figure 4). This trend suggests a significant interaction between group and time. In other words, the intervention group showed a notable cumulative enhancement in treatment effectiveness, while the control group remained unchanged. Moreover, the average PHQ-9 score in the final session was 3.44 for the intervention group and 6.89 for the control group, showing a difference of approximately 3.45 points. This difference is clinically meaningful, indicating that the intervention group achieved a significant and substantial improvement in depressive symptoms.
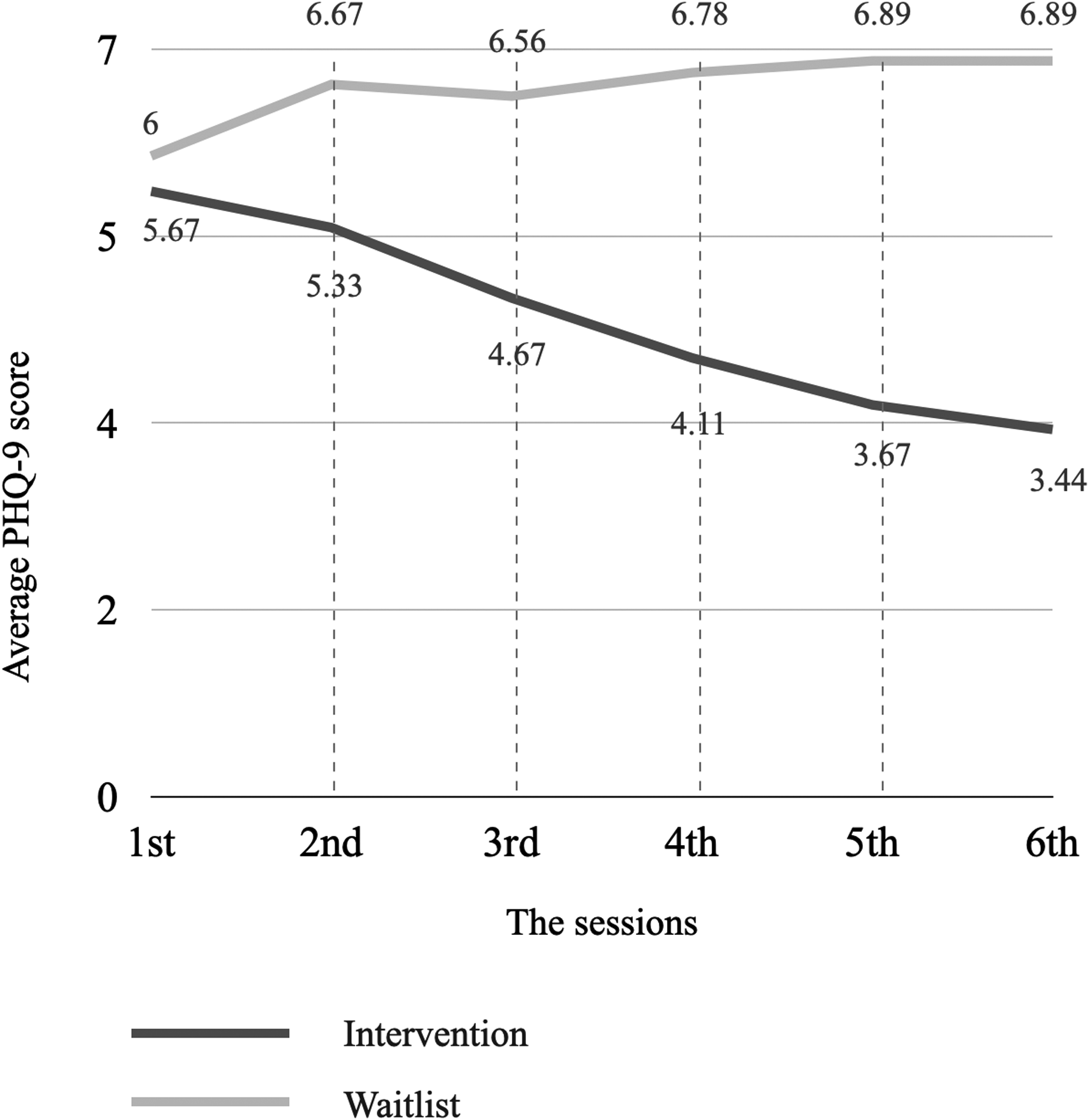
Comparison of Average PHQ-9 Scores Between Intervention and Waitlist Groups Across Six Sessions. PHQ-9= Patient Health Questionnaire-9
In addition, based on an item-level analysis of the PHQ-9 responses, the immediate effects of the African hand drumming therapy were particularly pronounced in several key symptom domains. Specifically, scores for “feeling down, depressed, or hopeless” (item 1) were significantly reduced postintervention, indicating alleviation of negative mood. Similarly, improvements in “loss of interest or pleasure in doing things” (item 2) suggest that participants experienced a notable restoration of engagement and enjoyment in daily activities. In addition, the decrease in scores for “feeling tired or having little energy” (item 4) reflects an effective enhancement of overall energy levels. Moreover, lower scores on “feeling bad about yourself, feeling like a failure, or that you have let yourself or your family down” (item 6) indicate that negative self-evaluation and self-blame were also mitigated. Collectively, these symptom-specific improvements demonstrate that the hand drumming therapy not only alleviates overall depressive symptoms but also targets critical aspects of mood, motivation, and self-worth, thereby supporting its potential as an effective intervention.
Acceptability
After the first and final intervention sessions, the research team conducted a satisfaction survey with the participants. It is noteworthy that during the first intervention session, one participant with autism experienced sensory overload. This significantly affected his overall experience, and his PHQ-9 score deviated considerably from those of the other participants. Moreover, he indicated that he was unable to continue with subsequent interventions. After consultation, the research team decided to replace him with another participant with visual impairment, resulting in data from a new sample of nine participants.
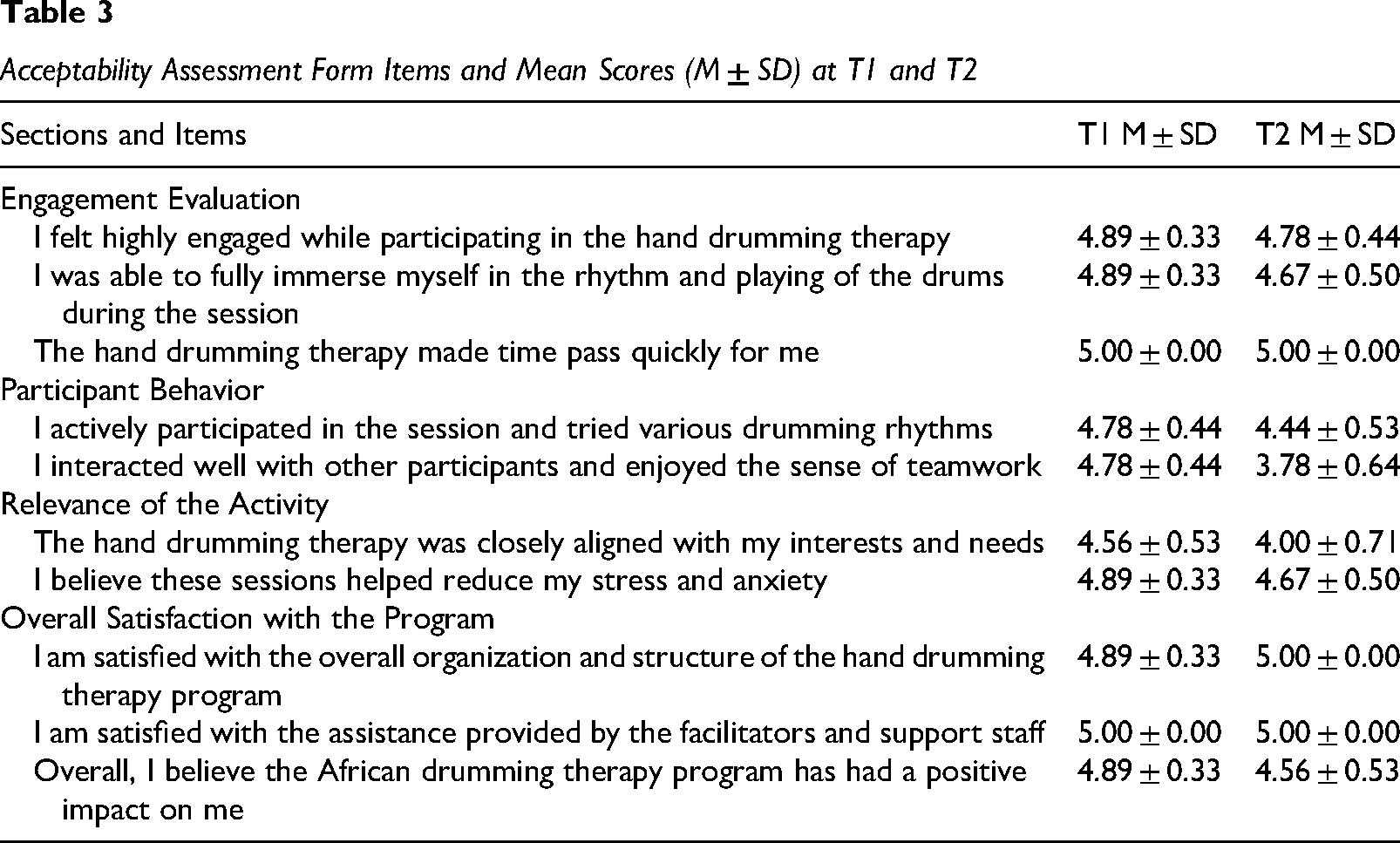
As shown in Table 3, most items (e.g., “immersion” and “sense of time passing”) received high scores in both assessments, indicating that the African hand drum therapy was effective in enhancing interest and concentration. Although some indicators (such as items 1 and 2) experienced slight declines, the overall scores remained positive. In terms of interpersonal interaction, the score for “interaction with other participants” dropped from 4.78 to 3.78, which is a relatively notable decrease. Regarding overall satisfaction, despite slight decreases in some items, scores for “project organization” and “staff assistance” remained at or increased to the highest level, demonstrating the stability of the program's management and support system. Most participants continued to acknowledge the positive impact of the therapy (with the average score for item 10, although slightly reduced, still above 4.5). In summary, overall satisfaction and acceptance of the hand drum therapy remained high in both assessments, particularly in terms of organization and support, although some indicators showed a slight decline in the final assessment.
Acceptability Assessment Form Items and Mean Scores (M ± SD) at T1 and T2
Responses to open-ended questions were mostly positive, addressing the impact of hand drumming therapy on emotions and its overall effects. Some participants mentioned the benefits of group participation in the community setting, noting opportunities for interaction with community members during the experience. For example, one participant commented, “I enjoyed the activity; it made me feel free and relaxed. Everyone sat together, and not only was I drumming, but I also felt like there were others providing accompaniment around me.”
All comments regarding stress and depression relief were positive. One participant noted, “I found that while drumming along with the facilitator, I had a strong urge to release my emotions. After doing so, I felt very comfortable.” Another remarked, I enjoy playing the piano, so I have good control over rhythm and beats. While drumming, I imagined the rhythms I use when playing the piano. Although the content was simple, it felt very rich. I liked it and found a new instrument to help me relax.
Reactions to the hand drumming therapy were predominantly positive. However, some negative feedback was noted. For instance, one participant felt that more than 40 min of repetitive drumming could become tedious. Some participants suggested that the experience might be better suited to small groups of three to four individuals. Therefore, in future projects, recommendations for improving the African drum therapy include reducing the group size to fewer than five participants, incorporating different drumming patterns, balancing the time allocated for the experience and interaction, and appropriately controlling the duration of the activity.
Discussion
This study aimed to assess the feasibility and acceptability of the hand drumming therapy intervention for depression and stress among the adults with visual impairments. The researchers evaluated the effectiveness of implementing this intervention in a group setting within the visually impaired community. The study found that the majority of participants engaged fully in the planned session, the two researchers adhered strictly to the established protocol, and participants did not exhibit significant cognitive burdens. Although there were minor issues with adaptation in specific cases, which did not substantially impact the overall implementation of the project.
Participants gave high ratings to the program's format, facilitator interactions, content engagement, and group performance suitability. Despite some challenges related to timing and drumming techniques, feedback from participants reflected their interest in and the effectiveness of the program. These findings support the feasibility and acceptability of the intervention method, indicating that it can be effectively implemented through collective drumming and is suitable for the adult population with visual impairments.
The intervention approach in this research aligns with experiential strategies (King, 2009). The core of experiential strategies lies in leveraging the facilitator's practical experience. The research team found that this approach is particularly well-suited to the highly experiential nature of African hand drumming therapy. The facilitators were able to flexibly adjust their guidance based on their experience, providing more intuitive and appropriate instruction for the participants with visual impairments. During the treatment process, individualized cases may emerge, such as the presence of additional physiological or psychological pathological features, which require a case-specific analysis. In instances where a participant exhibits extreme sensitivity to sound, the intervention should be immediately terminated and consultation with the appropriate pathology department should be sought. Furthermore, in the postperformance interaction segment, sharing personal experiences and insights allowed facilitators to establish deeper emotional connections with participants, enhancing the therapeutic effect. These factors, combined with a controlled research environment, likely contributed to the high level of participant engagement observed in this research.
Some participants encountered adaptation challenges at the beginning of the project, such as difficulty grasping the rhythm of drumming or keeping up with the musical beats. Although these issues affected individual therapeutic sessions, they did not significantly diminish participants’ overall acceptance of the intervention.
Results and observational records indicate that participants’ feedback was generally positive, with particular appreciation for the personalized guidance and extensive experience shared by the facilitators. Most participants reported that the approach helped them gain a deeper understanding and appreciation of hand drum playing, achieving noticeable effects in stress relief and depression alleviation. The result supports the advantages of experiential strategies in creating immersive experiences. Additionally, some participants sought further communication with facilitators about other family members’ mental health issues after the sessions.
Notably, participants exhibited great enthusiasm for the improvisation segment of the intervention. During drumming, different rhythms emerged, such as combinations of striking the drum surface and the drum rim, which were improvised. Most participants showed interest in this improvisation, believing that improvisational playing provided a freer and more relaxing experience.
Limitations and Future Research Directions
One limitation of this study is the potential self-selection bias among participants. Due to the limited size of the blind community, recruitment may have involved some degree of self-selection. However, when assigning participants to the intervention and control groups, the research team adhered strictly to random allocation. Future studies should employ more robust random recruitment methods.
Another limitation is the relatively small sample size. Future studies should incorporate larger samples and adopt a longitudinal approach to assess the intervention's long-term effects. Moreover, although the PHQ-9 in this study was modified in terms of wording to better reflect the perspectives of people with visual impairments and underwent multiple rounds of investigation, it should be acknowledged that every measure has inherent limitations. Future research should explore alternative or supplementary assessment tools to further validate and refine the measurement of depressive symptoms in this population. Additionally, exploring how to enhance the replicability of the intervention while maintaining the experiential characteristics is a valuable area for further investigation.
Implications for Practice
Our research findings indicate that group-based African hand drumming interventions for individuals with visual impairments experiencing depression and stress offer significant insights when conducted in a safe environment. Several considerations can enhance the effectiveness of the experience for the participants with visual impairments.
Firstly, proper equipment preparation and space arrangement are essential. Drums should be selected based on participants’ needs, considering size, weight, and other preferences. Facilitators should assist in choosing suitable drums before the intervention, with African djembe drums recommended for their clear sound and accessible height. The space should be safe, obstacle-free, and equipped with tactile markers to aid navigation for participants with visual impairments.
Secondly, training facilitators is vital to ensure the effectiveness of the therapy. Facilitators need to receive ample practice opportunities to become proficient in various verbal guidance techniques and strategies for handling different situations. This ample practice includes describing the structure and playing techniques of the African hand drum verbally (since people with visual impairments cannot visually identify the drum's structure), addressing issues that arise during practice, such as reactions to coexisting conditions, and providing postsession guidance. An experience-sharing mechanism among facilitators is important for promoting the exchange and dissemination of successful therapeutic methods through regular discussions and sharing sessions.
Furthermore, personalized adjustments tailored to each participant's needs and progress are essential. Facilitators need to adapt their guidance methods flexibly according to the individual needs, particularly concerning different conditions, levels of depression, and stress. Personalized guidance can enhance the therapeutic outcomes for participants.
Finally, establishing an effective feedback mechanism is critical as well. Continuously updating the therapeutic process based on feedback can be achieved by creating regular feedback channels to gather participants’ opinions on each session's content, rhythm, and guidance methods. Through these feedbacks, facilitators can understand participants’ emotional responses, needs, and expectations regarding potential therapeutic outcomes.
Supplemental Material
sj-docx-1-jvb-10.1177_0145482X261454344 - Supplemental material for Exploring the Potential for African Hand Drumming in Alleviating Stress and Depression Among the Blind Community
Supplemental material, sj-docx-1-jvb-10.1177_0145482X261454344 for Exploring the Potential for African Hand Drumming in Alleviating Stress and Depression Among the Blind Community by Yuan Ma and Kudakwashe Chininga in Journal of Visual Impairment & Blindness
Supplemental Material
sj-docx-2-jvb-10.1177_0145482X261454344 - Supplemental material for Exploring the Potential for African Hand Drumming in Alleviating Stress and Depression Among the Blind Community
Supplemental material, sj-docx-2-jvb-10.1177_0145482X261454344 for Exploring the Potential for African Hand Drumming in Alleviating Stress and Depression Among the Blind Community by Yuan Ma and Kudakwashe Chininga in Journal of Visual Impairment & Blindness
Footnotes
Acknowledgments
The authors would like to thank the patients, members, volunteers, and staff in Blind Low Vision, Hamilton, New Zealand.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Materials
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.