
Abstract

In functional endoscopic sinus surgery (FESS) for chronic rhinosinusitis, it is often beneficial to create a surgically enlarged opening to the sphenoid sinus. The two standard endoscopic approaches in sphenoid sinus disease are transnasal, through the anterior wall of the sphenoid sinus, or transethmoid, through the posterior ethmoid sinus.
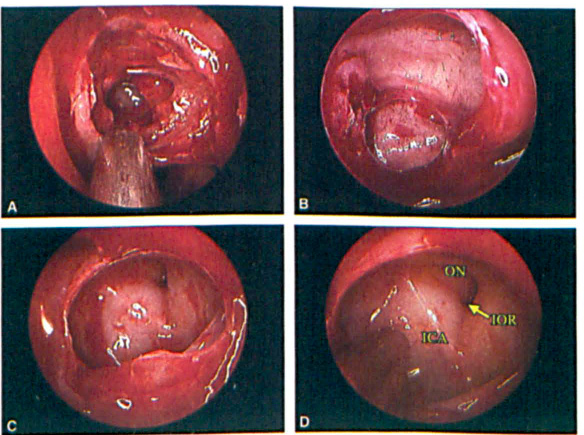
An approach to the sphenoid sinus through the ethmoid sinus requires dissection of the anterior and posterior ethmoid cells (figure, A). The important landmark in this technique is the posterior wall of the posterior ethmoid sinus (figure, B). The approach to the sphenoid sinus is men carried out through the inferior and medial portion of the posterior ethmoid sinus. This is important because approaching laterally and superiorly through the lateral portion of the ethmoid sinus could easily injure the optic nerve, or in the case of an Onodi cell, cause entry into the intracranial cavity. 1 The opening from the posterior ethmoid into the sphenoid sinus is shown in me figure, image C. Once mat opening has been enlarged, the lateral wall of the sphenoid sinus can be visualized, showing the internal carotid artery, optic nerve, and infraoptic recess (figure, D).
The transethmoid approach to the sphenoid sinus was described by Messerklinger. 2 In an anterior-to-posterior FESS dissection, the surgeon may choose this route as an extension of the posterior ethmoid dissection, to open the sphenoid sinus. As described above, care must be taken when entering the sphenoid sinus, to dissect inferiorly and medially to avoid injury to the vital structures of the lateral wall of the sphenoid sinus.