
Abstract

An 82-year-old man was referred for evaluation of nodular lesions on the tongue and left buccal mucosa. He had an 8-year medical history of chronic renal failure and had been treated with hemodialysis. Two months prior to presentation, the first nodular lesion appeared on the tip of his tongue. Seven days later, four new nodular lesions appeared in the oral cavity. The size of the lesions gradually increased.
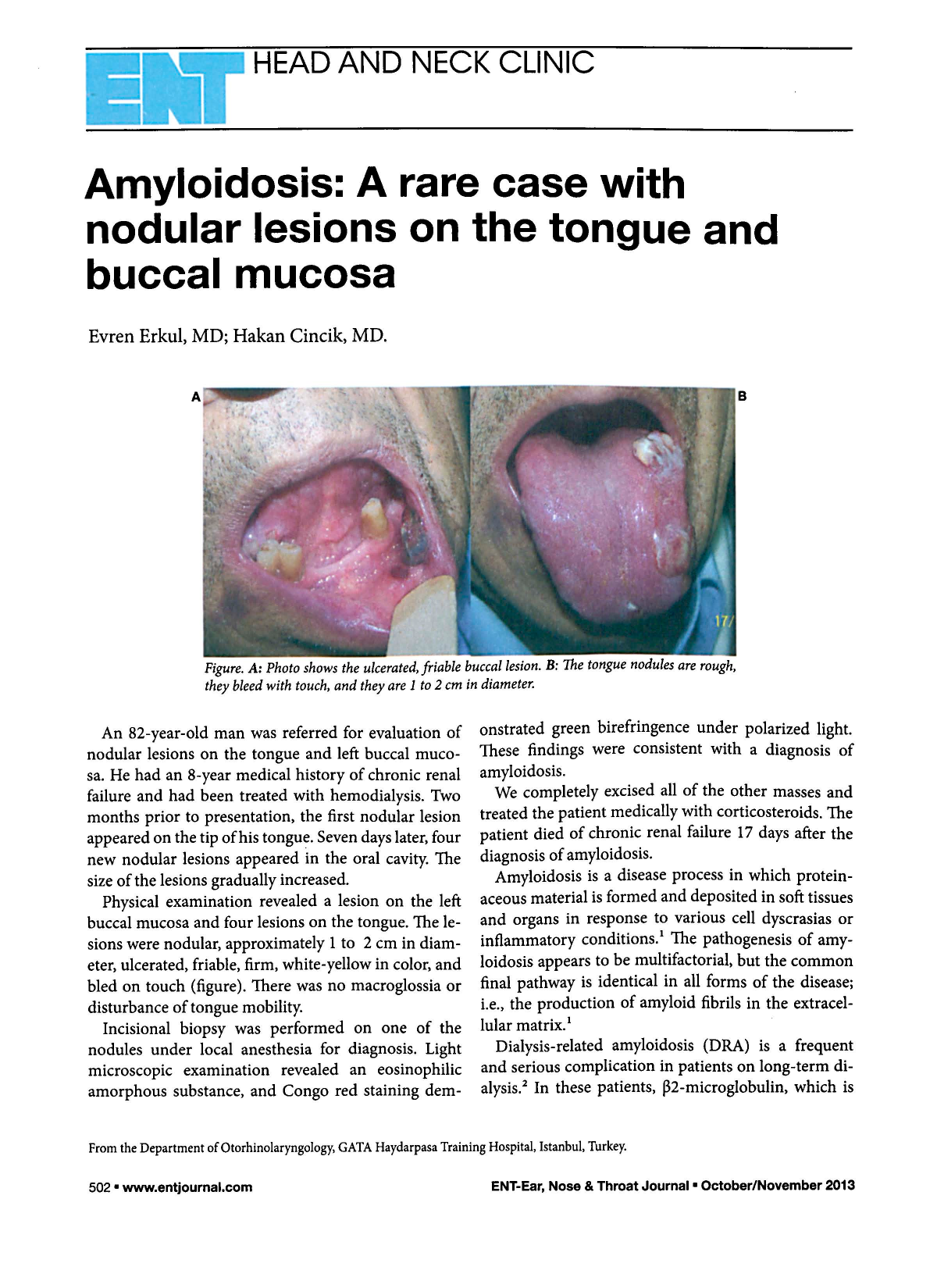
Physical examination revealed a lesion on the left buccal mucosa and four lesions on the tongue. The lesions were nodular, approximately 1 to 2 cm in diameter, ulcerated, friable, firm, white-yellow in color, and bled on touch (figure). There was no macroglossia or disturbance of tongue mobility.
Incisional biopsy was performed on one of the nodules under local anesthesia for diagnosis. Light microscopic examination revealed an eosinophilic amorphous substance, and Congo red staining demonstrated green birefringence under polarized light. These findings were consistent with a diagnosis of amyloidosis.
We completely excised all of the other masses and treated the patient medically with corticosteroids. The patient died of chronic renal failure 17 days after the diagnosis of amyloidosis.
Amyloidosis is a disease process in which proteinaceous material is formed and deposited in soft tissues and organs in response to various cell dyscrasias or inflammatory conditions. 1 The pathogenesis of amyloidosis appears to be multifactorial, but the common final pathway is identical in all forms of the disease; i.e., the production of amyloid fibrils in the extracellular matrix. 1
Dialysis-related amyloidosis (DRA) is a frequent and serious complication in patients on long-term dialysis. 2 In these patients, β2-microglobulin, which is part of the class I major histocompatibility complex antigen, is the major protein constituent of the amyloid fibrils. It fails to cross the dialysis membrane, resulting in the formation of amyloid fibrils. 2
Amyloid involvement of the oral tissues is rather rare; when it does occur, the tongue is the most frequent location, and amyloidosis in this area usually manifests as rubbery or firm macroglossia. 3 Amyloidosis of the tongue results in white-yellow nodules >1 mm in diameter and firmer than the other parts of the tongue. 4 Petechiae, ecchymoses, and hemorrhagic blisters may also be present.1,3 Zhou et al 5 reported 14 patients with oral amyloidosis, 12 of whom had macroglossia. Our patient did not show macroglossia, but hemorrhagic and ulcerated nodules were observed on the tongue and buccal mucosa.
In one study, 8 cases of DRA were found as tongue amyloid nodules among 103 long-term (>20 years) hemodialysis patients. 6 Our patient had been on hemodialysis for only 8 years. The definitive diagnosis is made by tissue biopsy. 7 Treatment of DRA has been limited to surgical removal of amyloid deposits. Clinical therapeutic strategies for DRA include dialysis, medical or surgical therapy, and renal transplantation to obtain normal serum levels of β2-microglobulin.4,8
New high-flux, biocompatible dialysis membranes are more permeable and are effective in treating amyloidosis. 4 More effective preventive therapy strategies will be helpful for patients with DRA. Benign epithelial and connective tissue neoformation—including fibrosarcoma, malignant fibrous histiocytoma, leiomyoma, papilloma, lipoma, lymphangioma, neuroma, hemangioma, and adenoma—must be considered in the differential diagnosis of oral masses. 3