
Abstract

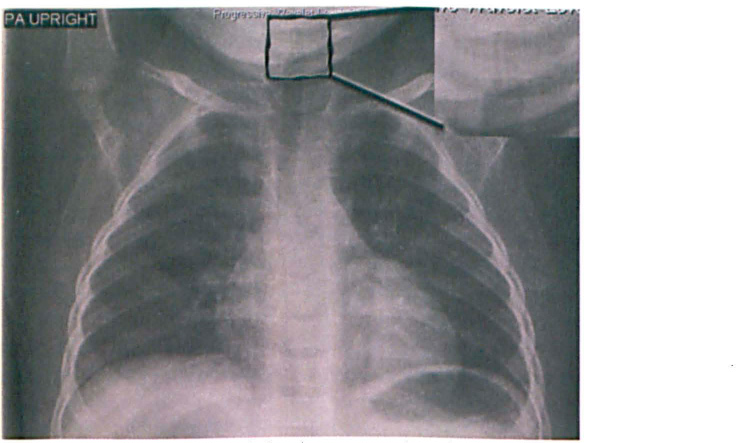
The steeple sign (magnified in the inset image) can be seen on our patient's posterior-anterior upright chest x-ray. The steeple sign is highly suggestive of subglottic narrowing and is often seen in laryngotracheitis. Additionally, the foreign body can be visualized in the subglottic space.
Laryngotracheobronchitis (i.e., croup) accounts for 90% of infectious airway obstructions in children. 1 The peak incidence in children is 18 to 24 months of age; the duration of illness is typically 3 to 5 days. 2 The most critical factor in those with viral croup is the amount of edema in the subglottis, which is the narrowest portion of the upper respiratory tract in children. The diagnosis is based mostly on the history and physical examination, but it may be aided by imaging or endoscopic visualization. Management strategies for viral croup may include glucocorticoids, epinephrine, heliox, and cool mist oxygen therapy.
Croup may be considered atypical if it occurs in infants younger than 6 months of age, lasts more than 7 days, or does not respond to appropriate treatment. 1 Other etiologies besides acute viral laryngotracheitis—such as supraglottitis, retropharyngeal abscess, bacterial tracheitis, or foreign body—should be considered in these atypical cases.
A 12-month-old boy presented with new-onset biphasic stridor at an outside hospital. He was diagnosed with and treated for croup. The child was otherwise healthy and was developmentally within normal limits. He was given racemic epinephrine, cool mist oxygen therapy, and glucocorticoids while hospitalized. His overall condition improved, but he continued to have mild, although improved, stridor. He was subsequently discharged on oral steroids.
One week later the patient presented to our emergency department with worsening biphasic stridor. No history of possible foreign body aspiration was elicited. The chest radiograph at presentation is shown in figure 1. While a subglottic foreign body can be visualized retrospectively, it is easy to see how the presentation of this child biased the initial interpretation of the radiograph to that of subglottic narrowing alone. Given the prolonged and atypical course of his croup-like presentation, however, we elected to perform rigid laryngobronchoscopy.
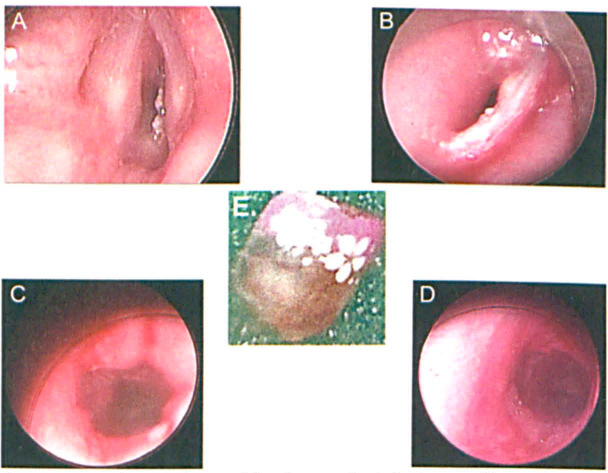
A Miller laryngoscope was brought into the field, and the larynx was visualized. An abnormality was noted in the inferior aspect of the right posterior vocal fold; therefore, a rigid bronchoscope was introduced to the field. Slight retraction on the vocal fold and passage of the bronchoscope into the subglottis made the presence of a foreign body apparent. An acrylic fingernail was found in the subglottis. It was removed via optical bronchoscopic forceps (figure 2).
Bronchoscopy 2 weeks later revealed residual grade I subglottic stenosis from prolonged retention of the foreign body. The patient was treated conservatively with a proton pump inhibitor and oral steroids for several weeks, and subsequent follow-up revealed no residual subglottic stenosis.
The presence of foreign bodies in the subglottic airway has a low prevalence (3 to 12%) when compared to other airway sites; however, the presence of a foreign body at this site may cause significant edema, resulting in airway distress or even death.3,4 While cases of large, completely obstructing foreign bodies in the subglottis would lead to sudden respiratory distress, the initial presentation of smaller foreign bodies in the subglottis can be quite similar to croup, presenting with biphasic stridor, cough, and/or the steeple sign. A transient response to steroids and other symptomatic therapy used to treat croup may occur secondary to the temporary decrease in edema surrounding the foreign body.
While approximately 5% of children with croup will have recurrent episodes, it is important to rule out other etiologies in patients with “atypical” presentations, especially the presence of a foreign body. 1 Referring physicians are often keen to recognize symptoms of lower respiratory tract foreign bodies, but symptoms suggestive of laryngeal or subglottic foreign bodies do not often raise the same clinical suspicion. 5
Although only limited published reports describe the misdiagnosis of an airway foreign body as croup, the inclusion of this diagnosis in the differential of patients presenting with atypical croup is important and may be life saving.6,7 Even though the differential diagnosis of croup is vast, foreign body aspiration should always be considered in any child not showing progressive clinical improvement. Failure to expeditiously diagnose a subglottic foreign body may result in complications such as subglottic stenosis and even death.