
Abstract
Oral mucositis (OM) refers to erythematous and ulcerative lesions of the oral mucosa. This pathology can occur by various causes. Cancer therapy is one of the well-known causes of OM such as chemotherapy and/or with radiation therapy. It has been widely mentioned that oxidative stress parameters such as lipid peroxidation (LP) levels increase during cancer process. Glutathione (GSH) is one of the major intracellular enzymes to detoxify oxidant molecules. The aim of this study was to investigate and compare the effects of Triamcinolone Acetonide (TA), a synthetic steroid chlorhexidine (CHX), a chemical antiseptic, on 5- fluorouracil (5-FU), a chemotherapeutic agent and soft abrasion induced OM in buccal mucosa of rats.
OM was induced in rats through a combination of 5-FU treatment and mild abrasion of the cheek pouch with a wire brush. Buccal mucosa lipid peroxidation (LP) levels were higher (p< 0.05) in 5-FU group than in control although LP levels were lower (p<0.05) in TA group than in control group. The reduced glutathione levels were lower (p<0.05) in 5-FU group than in the control group although its level was higher (p<0.05) in TA and CHX groups than in the 5-FU group. Glutathione peroxidase activity was also higher (p<0.05) in TA group than the 5- FU group. In histopathological analyses, treatment with TA reduced 5-FU induced inflammatory cell infiltration and ulceration (p<0.001) but not with CHX.
In conclusion, we observed that TA and CHX treatment modulated chemotherapy induced oxidative injury in the rat OM. However, only TA histopathologically ameliorated the 5-FU induced OM of rats. These findings suggest that TA is a useful agent for management of experimental oxidative injury and OM caused by the chemotherapy.
Introduction
Oral problems such as mucosal ulcerations, xerostomia, and bacterial and fungal infections are frequent complications of cancer therapy. 1 Oral mucositis (OM) refers to erythematous and ulcerative lesions of the oral mucosa. This pathology can occur by various causes. Cancer therapy is one of the well-known causes of OM such as chemotherapy and/or with radiation therapy. 2 ,3 Severe OM can cause profound pain and oral functional incapability with clinical impairments which will affect the quality of life adversely. 4
Mechanisms for chemotherapy-induced mucositis are believed to include five-stage cascade model; 5,6 a) Initiation of tissue injury, b) Upregulation of inflammation via generation of messenger signals, c) Signaling and amplification, d) Ulceration and inflammation, e) Healing. It is strongly believed that in the first step of this cascade model, reactive oxygen species (ROS) exert an important role in the initiation of mucosal injury by chemotherapy induced cellular damage of the basal epithelial cells and cause subsequent clonogenic cell death in the epithelial layer via DNA damage. In addition to causing cell death, free radicals also activate second messengers that transmit signals from receptors on the cellular surface to the inside of the cell. This leads to up regulation of pro-inflammatory cytokines, tissue injury and consequently cell death. Antioxidants are thought to act as a scavenger for harmful reactive oxygen species which are known to potentiate mucositis. 5 , 7 Lipid peroxidation is a process generated by the effect of several reactive oxygen species (hydroxyl radical, hydrogen peroxide etc.) and also crucial step in the pathogenesis of several types of tissue damage in adult and infant patients. Moreover LP can also be generated by the action of several phagocytes. These reactive oxygen species readily attack the polyunsaturated fatty acids of the fatty acid membrane. The destruction of membrane lipids and the end-products of such lipid peroxidation reactions are especially dangerous for the viability of cells, even tissues. 8 , 9
Glutathione (GSH) plays an important role in a wide range of cellular processes, including cell differentiation, proliferation, and apoptosis, and disturbances in GSH homeostasis are involved in the etiology of many types of diseases. Elevated GSH levels increase the antioxidant capacity and the resistance to oxidative stress as observed in many cancer cells. Intracellular redox balance is regulated mainly by GSH 9 -11 that participates, not only in antioxidant defense systems, but also in many metabolic processes. 12 The molecular mechanism of how GSH modulates cell proliferation still remains speculative.
Several modalities have been suggested to reduce the severity of, or prevent OM such as oral care, cryotherapy, low-level laser therapy, amifostin, N-acetylcystein, palifermin, sucralfate, benzydamine, non-steroid anti-inflammatory drugs and growth factors. 13 Triamcinolone acetonide (TA) and Chlorhexidine (CHX) are chemicals which can be used in various oral mucosal diseases. Although, TA and CHX are widely used as clinically, the molecular mechanism of these agents are controversial in literature.
Although some studies pointed that ROS may play a pivot role in initiation phase of OM, to our knowledge, the ROS production in chemotherapy induced OM tissue in human or animal has not been reported so far in the literature. This is the first study with respect to investigate the ROS levels of chemotherapy induced OM tissue. In addition, the molecular pathway of possible effects of TA and CHX on ROS production and histopathological changes in OM tissue is not well identified yet. In the present study we aimed to investigate and compare probable positive effects of TA and CHX against 5-Fluorouracil (5-FU, a pyrimidine analogue anticancer drug) induced OM in rats.
Materials and methods
Animals
Thirty-six female, healthy, Wistar-albino rats, with 21–30 days of age, weighing 150-230 g were enrolled in this study. Rats were allowed 1 week to acclimatize to the surroundings before beginning any experimentation. All animals were housed in individual plastic cages with bedding. Standard rat food and tap water were available ad libitum for the duration of the experiments. The temperature was maintained at 22 ± 2 ºC. A 12/12 h light/dark cycle was maintained, with lights on at 07:00. Experimental protocol of the study was approved by the ethical committee of the Medical Faculty of Süleyman Demirel University (Protocol Number; 2009: 16-02). Animals were maintained and used in accordance with the Animal Welfare Act and the Guide for the Care and Use of Laboratory.
Chemicals
All chemicals used in this study were of analytical grade of high purity and were obtained from Sigma-Aldrich Chemical Inc. (St. Louis, MO) and all organic solvents came from Merck Chemical Inc. (Germany). All reagents except the phosphate buffers were prepared daily and stored at +4 ºC but were equilibrated at room temperature for 30 min before any analysis was initiated or reagent containers were refilled. Phosphate buffers were stable at +4 ºC for 1 month. 5-FU was purchased from Liba Lab. Inc. (İstanbul, Turkey). Triamcinolone acetonide was purchased from Bristol-Myers Squibb Inc. (İstanbul, Turkey). Chlorhexidine gluconat was gift from Drogsan Drug Inc. (Ankara-Turkey).
Study Groups
Except control group, oral mucosal injury was induced in rats through of 5-FU administration and mild abrasion of the cheek pouch performed with a wire brush in all groups. The 5-FU was applied i.p. in the all groups except control group at 1st and 3rd day of experiment. Mild abrasion applied on mucosa at 2nd and 3rd days in all animals of each groups. Saline, TA and clorhexidine were administered as intraoral topically for a period of 5 days (4th-8th day). All animals were anesthetized by ketamine 100 mg/kg at 9th day and sacrificed. The buccal mucosa samples were removed and divided into two parts including both of injured and healthy areas in each sample. Half of the samples fixed with 10% formalin during 24 h for histopathological examination. Remaining samples were stored at -33 ºC for LP and antioxidant analyses. The analyses were performed within one week.
Measurement of LP levels
LP levels in the buccal mucosa samples were measured with the thiobarbituric-acid reaction by the method of Placer et al. 14 Thiobarbituric acid-reactive substances were quantified by comparing the absorption to the standard curve of malondialdehyde (MDA) equivalents generated by acid-catalyzed hydrolysis of 1,1,3,3-tetramethoxypropane. LP values in the buccal mucosa were expressed as micromoles per gram of protein.
Reduced Glutathione (GSH), Glutathione Peroxidase (GSH-Px) and Protein Assay
The GSH content of the buccal mucosa samples was measured at 412 nm using the method of Sedlak and Lindsay. 15 The samples were precipitated with 50 % trichloracetic acid and then centrifuged at 1,000g for 5 min. The reaction mixture contained 0.5 ml of supernatant, 2.0 ml of Tris–EDTA buffer (0.2 M; pH 8.9) and 0.1 ml of 0.01 M 5,50-dithio- bis-2-nitrobenzoic acid. The solution was kept at room temperature for 5 min, and then read at 412 nm using a spectrophotometer (Shimadzu UV-1800, Kyoto,Japan). GSH-Px activities of the buccal mucosa samples were measured spectrophotometrically at 37 °C and 412 nm according to the method of Lawrence and Burk. 16 The protein content in the buccal mucosa samples was measured by the method of Lowry et al. with bovine serum albumin as the standard. 17
Histopathological Analyses
The samples removed from cheek pouches were fixed in 10% neutral-buffered formalin, dehydrated and embedded in paraffin. Tissue blocks (5 µm) were sectioned serially by a microtome, and stained with haematoxylin and eosin. Sections were blindly evaluated with light microscopy (x100 and x200) by the same pathologist. Scoring methods in rats were taken from Lima et al. 18 and Leitão et al. 19 The parameters of inflammatory cell infiltration, vascular dilatation and ingurgitation, presence of hemorrhagic areas, edema, ulceration and abscesses were determined in a single-blind manner and graded, on a score of 0–3, as follows, and described previously elsewhere. 20 0: Normal epithelium and connective tissue without vasodilatation; absence of, or discreet, cellular infiltration; absence of hemorrhagic areas, ulceration or abscesses. 1: Discreet vascular ingurgitation, areas of re-epithelialization; discreet inflammatory infiltration with mononuclear prevalence; absence of hemorrhagic areas, edema, ulceration or abscesses. 2: Moderate vascular ingurgitation, areas of hydropic epithelial degeneration, inflammatory infiltration with neutrophil prevalence, presence of hemorrhagic areas, edema and eventual ulceration, and absence of abscesses. 3: Severe vascular ingurgitation and dilatation, inflammatory infiltration with neutrophil prevalence, presence of hemorrhagic areas, edema and extensive ulceration and abscesses.
Statistical Analyses
Data are expressed as means ± SD of the numbers of determinations. Statistical significance was analyzed using the SPSS program (9.05; SPSS, Inc., Chicago, IL, USA). To compare the different treatments, statistical significance was calculated by the Mann–Whitney U test. p<0.05 was considered to indicate a statistically significant difference.
Results
This study was begun with 36 rats which were confirmed to healthy. Three rats died of unknown causes in 7th and 8th days in Group III and 3 rats died in 7th and 9th days in Group IV. Therefore, the samples of thirty animals were evaluated with respect to histopathologic and oxidative stress status.
LP results
Mean values of LP as μM/g protein in the control, 5-FU, 5-FU+TA and 5- FU+Chlorhexidin were 25.6, 30.1, 21.9 and 25.4, respectively. LP level was significantly (p<0.01) higher in 5-FU group than in others. LP levels were significantly lower in 5-FU+TA (p<0.001) and 5-FU+Chlorhexidin (p<0.05) groups than in 5-FU group. In addition, LP levels were significantly lower in 5-FU+TA group than 5-FU+Chlorhexidin (p<0.05) (Figure 1).
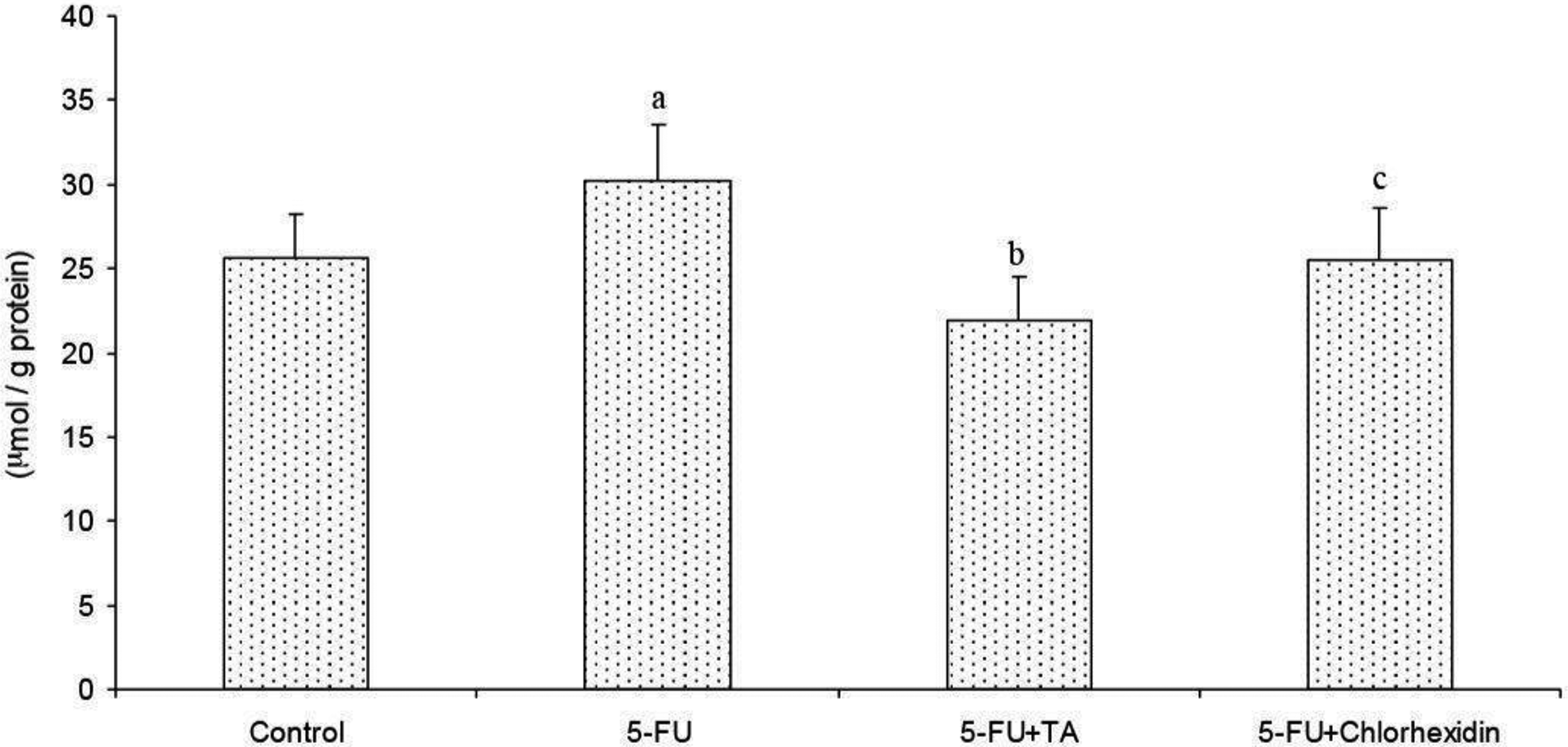
Effect of triamcinolone acetonide (TA) and chlorhexidin on 5-fluorouracil (5-FU)- induced lipid peroxidation levels in buccal mucosa of rats. (mean±SD and n=8). ap<0.01 versus control. bp<0.001 and cp<0.05 versus 5-FU group.
GSH results
Mean values of GSH as μM/g protein in the control, 5-FU, 5-FU+TA and 5- FU+Chlorhexidin were 16.5, 15.5, 29.6 and 30.3, respectively. GSH values were significantly higher in 5-FU+TA (p<0.01 and p<0.001) and 5-FU+Chlorhexidin (p<0.01) groups than in 5- FU and control groups. There was no significant difference between 5-FU and control groups and between 5-FU+TA and 5-FU+Chlorhexidin groups (Figure 2).
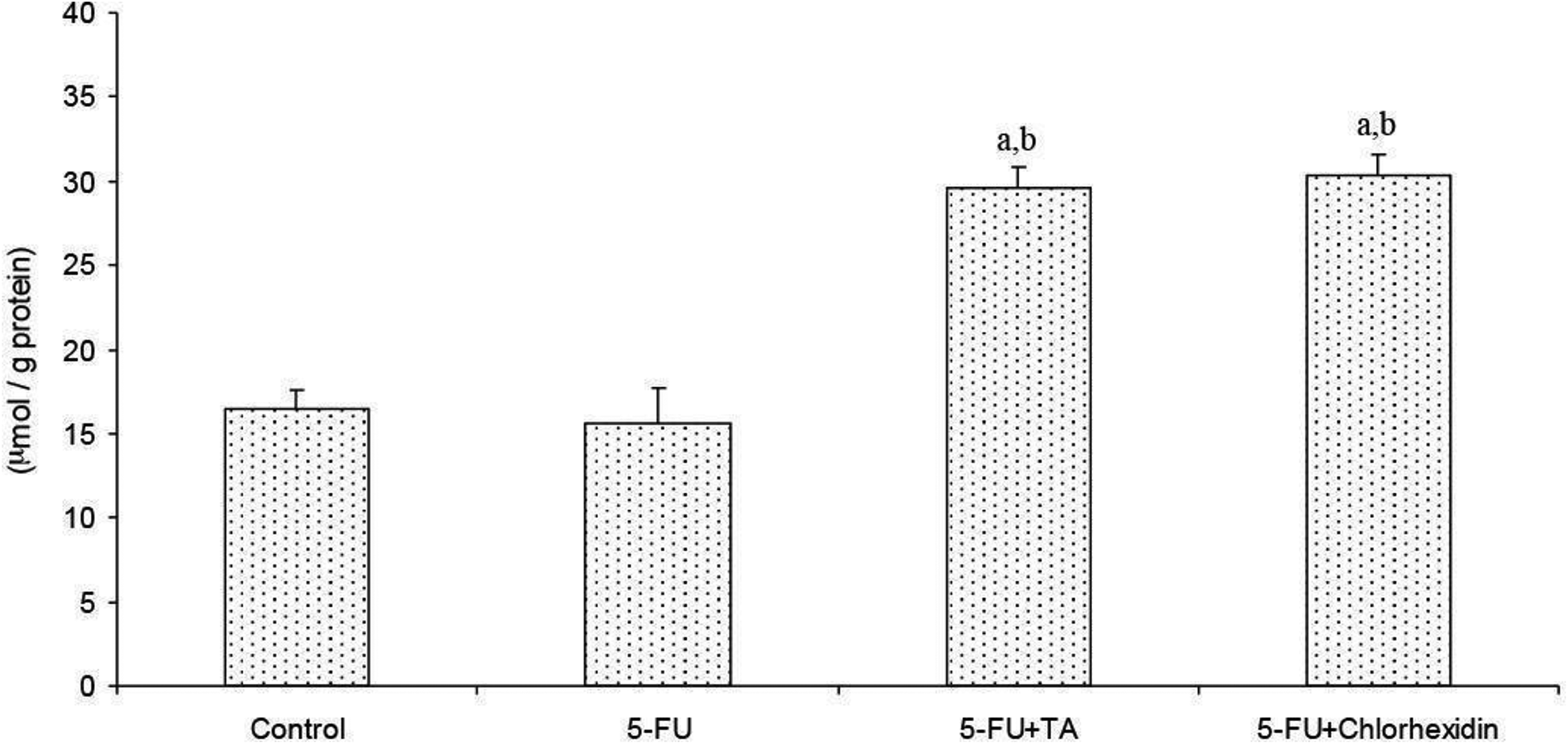
Effect of triamcinolone acetonide (TA) and chlorhexidin on 5-fluorouracil (5-FU)- induced reduced glutathione (GSH) changes in buccal mucosa of rats. (mean±SD and n=8). ap<0.001 versus control. bp<0.001 versus 5-FU group.
GSH-Px results
Mean values of GSH-Px as IU/ g protein in the control, 5-FU, 5-FU+TA and 5- FU+Chlorhexidin were 14.3, 11.9, 20.8 and 19.8, respectively. GSH-Px activity was significantly (p<0.05) lower in 5-FU group than in others. GSH-Px values of 5-FU+TA group were significantly higher than the values of 5-FU+Chlorhexidin and 5-FU groups (p<0.01 and p<0.001, respectively). In addition, GSH-Px values of 5-FU+Chlorhexidin were significantly higher than the values of 5-FU groups (p<0.01). On the other word, there were significant differences among all groups (Figure 3).
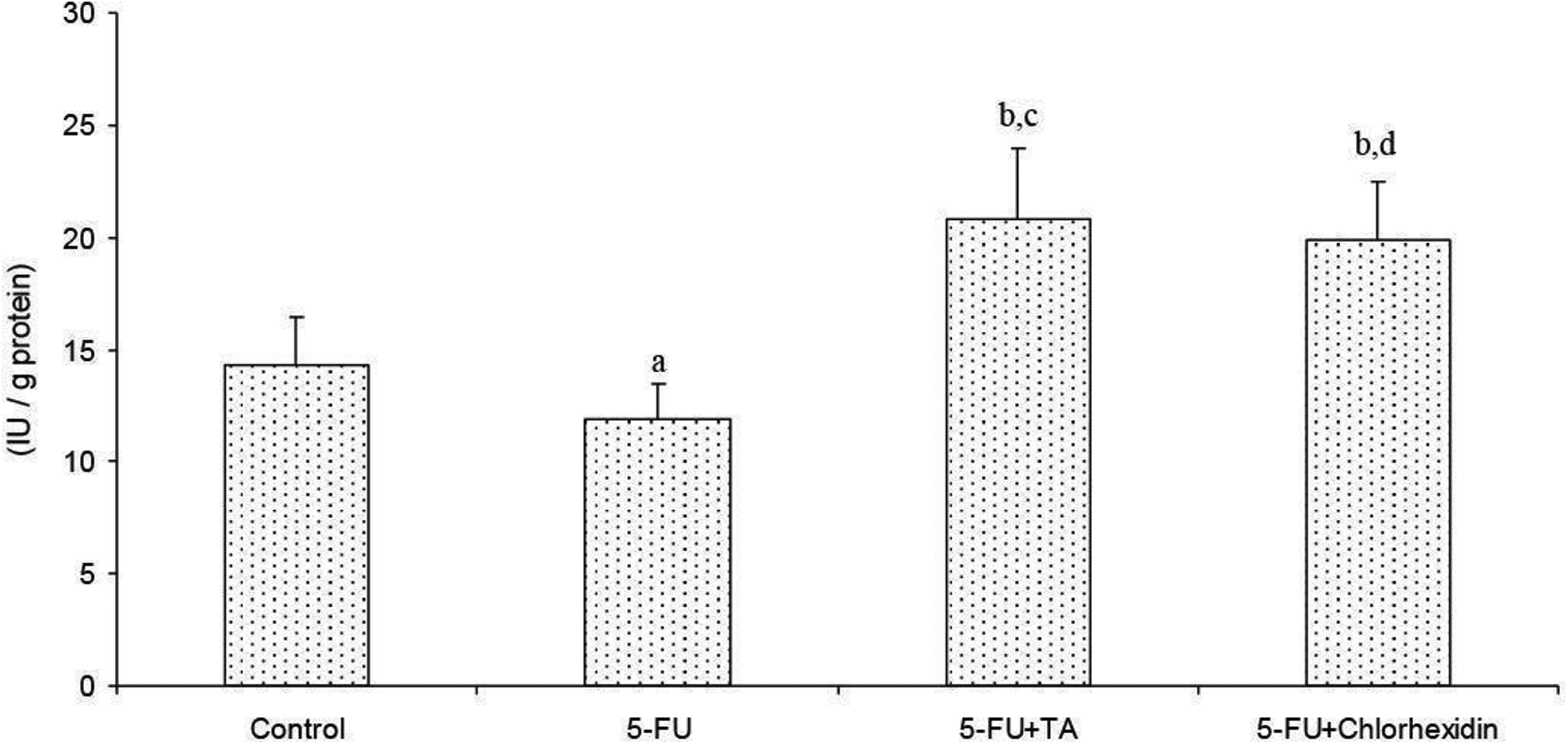
Effect of triamcinolone acetonide (TA) and chlorhexidin on 5-fluorouracil (5-FU)- induced reduced glutathione peroxidase (GSH-Px) activity changes in buccal mucosa of rats. (mean±SD and n=8). ap<0.05 and bp<0.01 versus control. cp<0.001 and dp<0.01 versus 5-FU group.
Histopathological results
The specimens were graded with scoring system as written above. Histopathological changes were shown in Table 1 and Figure 4. Presence of the oral mucositis observed with intense cellular infiltration, including neutrophil and extensive ulcers in the cheek pouch of animals exposed to 5-FU (Figure 4). Treatment with TA significantly reduced 5-FU induced inflammatory cell infiltration and ulceration (p<0,001). Furthermore we also observed re- epithelization in TA group. However we did not observe any re-epithelization in Chlorhexidin treatment group. In addition we observed ulceration and intense inflammatory cell infiltration consist of neutrophils. TA group also had significant difference between Chlorhexidin group (p<0,001).
Oral Mucositis Findings of Buccal Mucosa After Histopathological Examination.
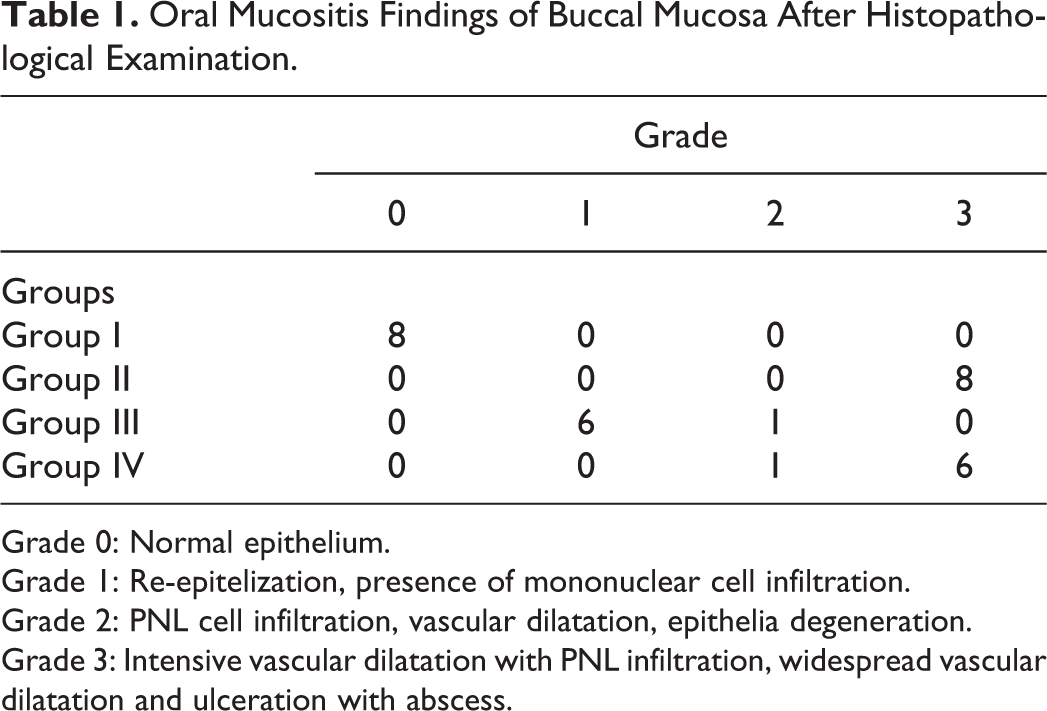
Grade 0: Normal epithelium.
Grade 1: Re-epitelization, presence of mononuclear cell infiltration.
Grade 2: PNL cell infiltration, vascular dilatation, epithelia degeneration.
Grade 3: Intensive vascular dilatation with PNL infiltration, widespread vascular dilatation and ulceration with abscess.
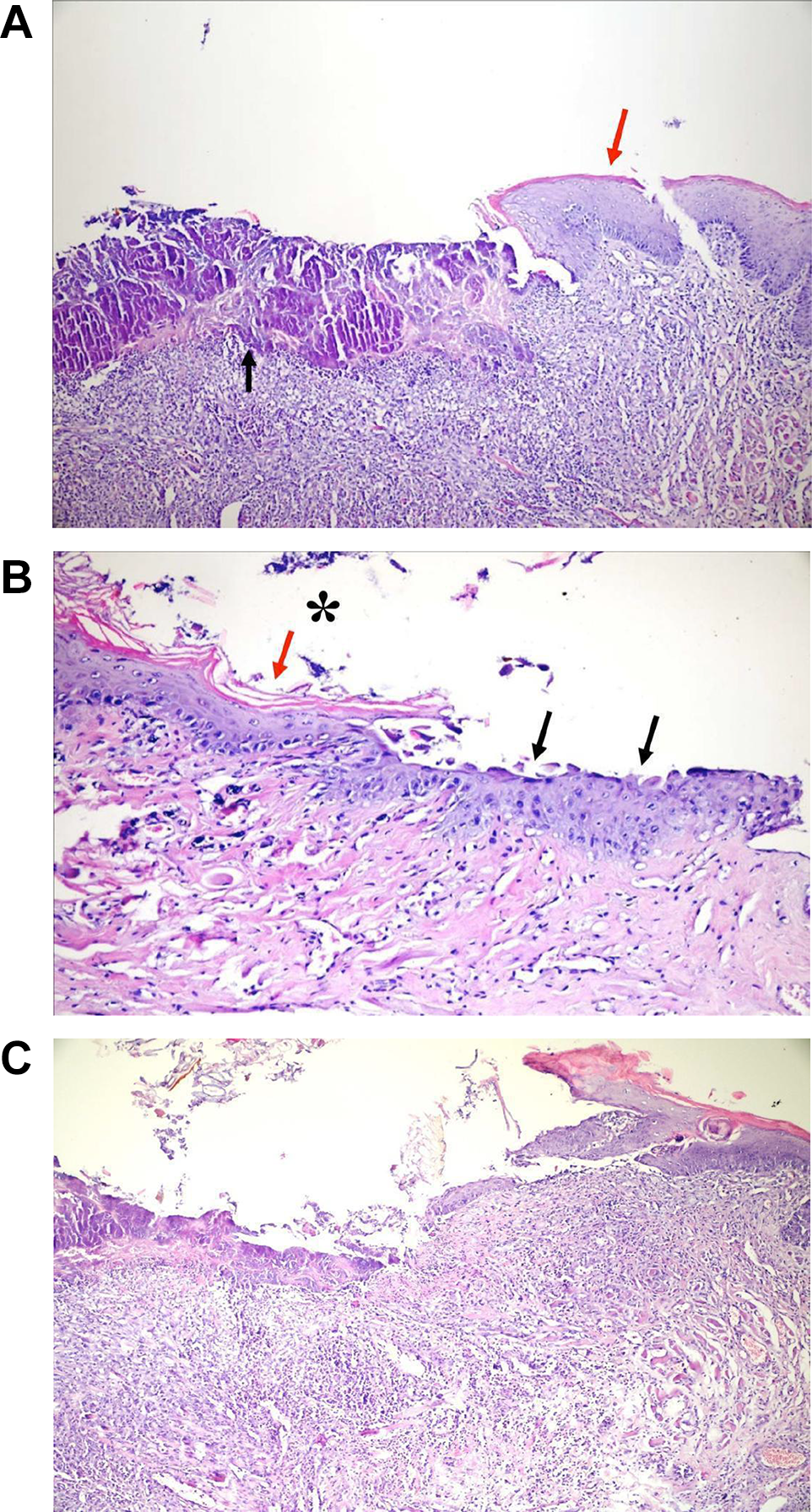
Histopathological aspects of oral mucositis of rats’ cheek pouches; (A) from 5-FU induced OM group: stratified squamous epithelium (red arrow) and generalize necrotic and ulcerative areas with inflamed cell infiltration (black arrow), (H&Ex100). (B) from TA group: stratified squamous epithelium (red arrow) and re-epithelialization areas (black arrows), (H&Ex200). (C) presence of extensive ulceration, necrosis and severe inflammatory infiltration with neutrophil prevalence. (H&Ex100).
Discussion
Mucositis is a complex process which is initiated by injury of cells in the basal epithelium and its underlying tissue. The probable mechanisms of oral mucositis induced by chemotherapy involve complex biological events mediated by a number of inflammatory cytokines such as tumor necrosis factor-α (TNF-α), IL-1 and IL-6; the direct effect of chemotherapeutic drugs or radiation on the basal epithelium and connective tissue; and the oral microbial environment. However, ulcerative mucositis results in the destruction of the oral mucosa as an anatomical barrier. The mouth thus becomes a portal of entry for enteric bacteria, viruses and fungi. These kinds of ulceration of the oral mucosa results in an increased risk of infection, especially when there will be immunosuppression. 21,22
TA is a synthetic corticosteroid and a powerful anti-inflammatory compound due to their ability to inhibit all stages of the inflammatory response, from redness to wound healing to cell proliferation. 23 TA possesses anti-inflammatory, anti-pruritic, and anti-allergic action which may provide prompt relief of oral tenderness, pain, inflammation and ulceration. TA maintains a protective covering which augments the effects of the steroid. 24 Although some studies have reported TA-induced cytotoxicity, 25 present study remains controversial, due to its anti-inflammatory effects. The most important result of this study is TA act as antioxidant / protective molecule in OM model in the buccal mucosa tissue. The redox status of the cells is of significance to determine the cellular anti-oxidant defense. It is generally determined by reduced glutathione (GSH), which is a major nonprotein cellular thiol in mammalian cells. GSH accounts in high amount of intracellular total glutathione in healthy cells. 26 GSH and its precursors have been reported to protect many cell types from oxidant-induced apoptosis. 27 The ratio of reduced glutathione to oxidized glutathione (GSSG) has been widely used as an indicator of cellular redox status. 28 GSH is used as a substrate to synthesis the GSH-Px. 29 The preservation of cellular GSH/GSSG ratio means less oxidative damage in the cell. 30 Thus, for the pathogenesis and treatment of buccal mucosa, this redox status is one of the important factors which may play crucial roles. GSH- Px, one of the major intracellular antioxidant enzymes, detoxifies hydrogen peroxide to water and also scavenge other peroxides. 31 In the current study we determined that GSH levels in TA groups are significantly higher (p<0.05) than other groups. ROS directly damage cells, tissues and blood vessels, and stimulate transcription factors such as nuclear factor (NF)-κB. Once activated, NF-κB leads to the upregulation of many genes, including those that result in the production of proinflammatory cytokines IL-1β, IL-6 and TNF-α. 32 , 33 It has been previously reported that TA in one of the strongest anti-inflammatory agent widely use in different inflammation models.
Moreover, TA treatment also decreased the ulcer area, ulceration, formation of abscesses and inflammatory cell infiltration in the buccal mucosa. Re-epithelization areas were also observed. Steroids may be additional mechanism against the buccal mucosa by which they exert their anti-inflammatory effects. For example, steroids destabilize the mRNA of the proinflammatory enzyme Cyclooxygenase-2 (COX2) by inhibiting the activity of p38. 34
Furthermore, the steroid signaling interacts with other signaling pathways activated by various cytokines, thus regulating diverse biological processes through modulating the expression of target genes. Steroids are powerful anti-inflammatory drugs. They modulate the expression of genes involved in inflammation through both transrepression and transactivation mechanisms. 35 , 36 While transcriptional repression of pro-inflammatory cytokines is widely accepted as the primary anti-inflammatory mechanisms, 37 such a mechanism occurs slowly, usually taking days or weeks to reach their maximal anti-inflammatory effects. OM is associated with high levels of interleukin synthesis. Additionally; steroids have also been shown to rapidly (within hours) inhibit the production of proinflammatory cytokines, associated with the inhibition of both p38 and JNK activities. 38 , 39 Interestingly, several laboratories have shown that steroids enhance the expression of MKP-1 in a variety of cell types, including epithelial cells, mast cells, and macrophages. 40 , 41 Moreover, the anti-inflammatory potencies of steroids are found to be proportional to their ability to induce MKP-1. 42
While inflammation is an important physiological response for the immune defense against pathogens or tissue injury, chronic or excessive inflammation can lead to inflammatory diseases, organ damage, and in severe cases, mortality, such as in patients with severe sepsis. 43 Inflammatory cytokines, such as TNF-α and interleukins play a pivotal role in the inflammatory response and contribute to the induction of enzymes responsible for the physiology of the inflammatory cascade. 44 Therefore, identification of small molecules that inhibit inflammation pathway in OM and undesirable side effects of current anti-inflammatory agents represents a major focus in the development of new anti-inflammatory drugs.
CHX, as a mouthwash, with concentrations of at least 0.2%, is a useful activity in oral diseases. Qutob et al. 45 reported that in their recent sistematically review, the evidence on the use of chlorhexidine mouthwash, to prevent oral mucositis needs further investigation. In addition, they suggested that it should not be considered in the management of OM because of conflicting with some articles in favor of their use and others against their use in current evidence. Although the studies are conflicting, CHX is one of the most widely used mouthwashes chemotherapy induced OM. In present study, although, CHX reduce oxidative stress level, it was not enough to clinical and histological improvement. Comparing with TA, histopathologic inefficiency of CHX may be due to other useful anti-inflammatory mechanisms which triggered by TA such as COX2.
The antioxidant enzyme system inherent in the cellular defense system is the most important defense mechanism against ROS. GSH acts as an antioxidants, and has preventive effect against extensive production of ROS by TA and chlorhexidin. Effects of TA and chlorhexidin on GSH-Px activities and GSH in human and animal studies are conflicting. 46 -48 Smillarly, Miura et al. 48 reported that GSH depletion increased the permeability of retinal pigment epithelium although TA had no effect on BSO-induced GSH depletion. Citirik et al. 47 demonstrated that commonly used steroids including dexamethasone and triamcinolone did not affect GSH levels on retinas in adult pigmented rats. The GSH values did not change between TA and chlorhexidin groups although GSH-Px values were increased by chlorhexidin treatment. Adaptative antioxidant responses of GSH were accompanied by GSH-Px enzymatic activity upregulation.
In conclusion, results of the current study suggest that TA increases GSH synthesis to preserve the redox balance, thus will maintain adequate cellular antioxidant defenses. The protective effects of TA and CHX, however, have not yet been reported in the buccal mucosa tissues, even though they are being widely used in many clinical practices. The results provide further important information in understanding the therapeutic effects of TA and CHX. However, results of the study are not relevant yet for clinical relevance. Future studies should therefore be aimed at identifying the specific intracellular pathways chemotherapy induced changes in oxidative stress of exposed oral mucosa of animal and human.
Footnotes
Acknowledgements
MN and SG formulated the present hypothesis. ACU and MN were responsible for writing the report. SG, GA and ACU were responsible for analysis of the data. GA and MY made critical revision in the manuscript. This work was partially supported by the Unit of Scientific Research Project, Süleyman Demirel University (No: 1953-TU-09).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.