
Abstract

Significance statement
Meningiomas are extremely rare tumors in the nasal cavity. They can often be confused with nasal polyps on clinical examination and radiologic imaging. Definitive diagnosis is made histopathologically and malignant types can be seen although rarely. Therefore, the diagnosis of nasal meningioma should be kept in mind in patients with nasal masses.
A 44-year-old female patient was admitted to our center with right-sided nasal obstruction and intermittent epistaxis which had increased in the last 6 months. The patient's medical history was unremarkable. General examination and routine laboratory test results were normal. Examination of the nasal cavity revealed a dark red, smoothly circumscribed mass in the right nasal cavity that bled easily to the touch. Non-contrast paranasal computed tomography (CT) images revealed a smoothly circumscribed hypodense lesion in the right nasal cavity indistinguishable from the turbinates. Contrast-enhanced paranasal magnetic resonance imaging (MRI) demonstrated an approximately 3.5 × 2 cm mass completely filling the right nasal cavity. The lesion containing the cystic opening was hypointense on T1-weighted images and isointense on T2-weighted images. Peripheral mild contrast enhancement was observed in postcontrast sections in the diffusion-unrestricted mass (Figure 1). The patient was diagnosed as nasal polyp. She was operated on by an otolaryngologist and the mass was removed. The lesion was diagnosed as meningioma on pathologic examination. The patient was discharged without any postoperative complications. The patient was followed up for 6 years with imaging and examination and no recurrence was observed. T2-weighted axial (A) and sagittal (B), T1-weighted axial (C) slices show a smoothly circumscribed mass lesion (asterisk) with a cystic opening (arrowhead) in the right nasal cavity. Minimal right deviation of the septum due to the lesion is noted (red arrow). In the postcontrast section (D), the lesion is minimally peripherally contrasted.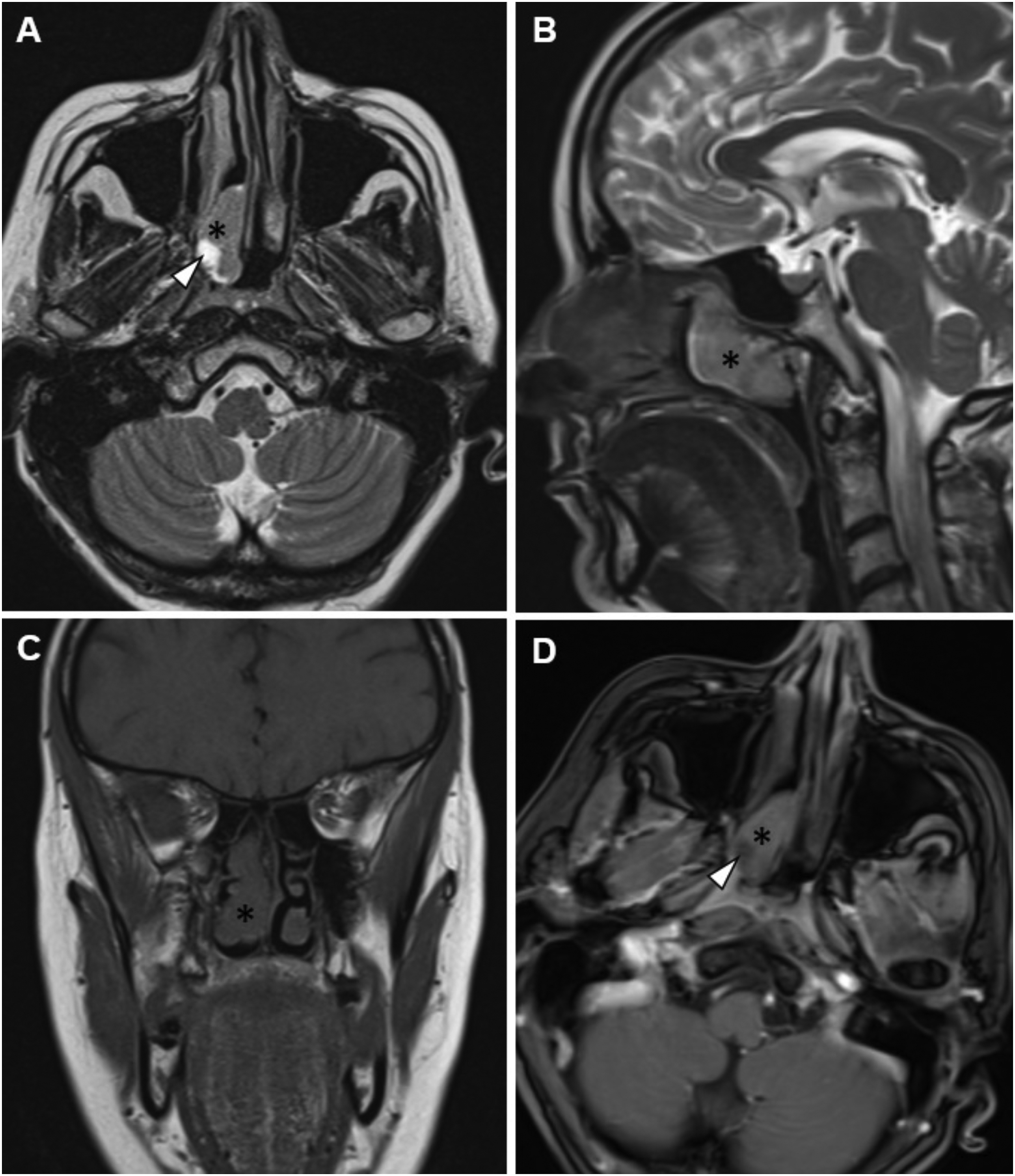
Meningiomas arise from arachnoid cap cells and account for approximately 25% of central nervous system tumors. However, extracranial meningiomas are rare. (1–2% of meningiomas). 1 It can be seen in the sinonasal canal, middle ear, scalp, soft tissues of the face and neck, skull bones, and salivary glands. 2 Primary extracranial meningiomas of the nasal cavity not associated with an intracranial lesion are extremely rare and have been reported as case reports in the literature. Symptoms are nonspecific and may include nasal congestion, anosmia, nasal discharge, epistaxis and head and face pain. On physical examination, they are observed as pink-red, non-infiltrative, globular-lobular contoured masses. Although they are usually benign, local invasion and metastasis can be seen in malignant types. 3 Differential diagnosis with nasal polyps is difficult with imaging methods. It is observed as a smoothly circumscribed hypodense lesion on CT. On MRI, cranial meningiomas are isointense with gray matter on T1- and T2-weighted images and show homogeneous contrast enhancement on postcontrast slices. 4 However, atypically located meningiomas may have polyp-like peripheral contrast as in our case. Currently, surgical excision of non-malignant types is the treatment of choice and adjuvant treatment is not required. 5
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the patient for this study.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.