
Abstract

Magill forceps can be found in every anesthesia cart. For anesthesiologists, they are the go-to instrument for nasotracheal intubation. They are also ideally suited for the removal of oropharyngeal foreign bodies—sometimes before the otolaryngology team has a chance to approach the patient. Less known are the contributions to the fields of anesthesiology and head and neck surgery of their inventor Sir Ivan Whiteside Magill. Born in Northern Ireland, Magill attended Queen’s University Medical School in Belfast and began training as a general surgeon. With the sudden outbreak of the First World War, Magill took a commission in the Royal Army Medical Corps. He served both as a Captain and medical officer to the Irish Guards through the Battle of Loos, then at a field hospital near Rouen, France. At the cessation of hostilities, he was posted to the Barnet War Hospital where he occasionally administered anesthetics for other surgeons. At demobilization, he was asked to state his current status. For a laugh, he listed “anesthetist.” This changed the course of his career. 1
In 1919 he was posted as an anesthetist at Queen’s Hospital for Facial and Jaw Injuries at Sidcup, Kent. It was at Sidcup that Sir Harold Gillies was at work revolutionizing reconstructive facial plastic surgery. Trench warfare, with its repeated battle charges into live fire, resulted in massive disfiguring injuries to the face and jaws of those who managed to survive. Reconstruction with grafts and local flaps required multiple surgeries. The existing anesthetic techniques, open-drop ether and transrectal ether-oil were wholly inadequate for patients with shattered faces. Chloroform insufflated through a narrow-gauge nasal “Silk” tube bubbled up in the surgeon’s face. Gillies commented to Magill: “Maggi—You seem to get this anesthetic into the patient alright, don’t you think you could devise some method of getting it out so that I am not anesthetized?” 2
Magill developed considerable skill with blind nasotracheal intubation using larger diameter flexible tubes to reduce anesthetic leaks. His colleague, Stanley Rowbotham devised a laryngoscopic technique for nasotracheal intubation using a curved “guiding rod” (Figure 1). 3 Magill embraced the technique and improved the laryngeal insertion. He created double-curved serrated forceps that could grasp the endotracheal tube and guide insertion into the glottis (Figure 2). 4 Gauze packing was placed around the nasotracheal tube, and a second nasal expiratory tube was attached to suction assured a clear operative field. During intubation, Magill recommended the modern sniffing position as follows: The patient’s head for this maneuver should be as of a man “scenting the air” or (and more characteristic of Magill’s passions) “draining a pint of beer.”
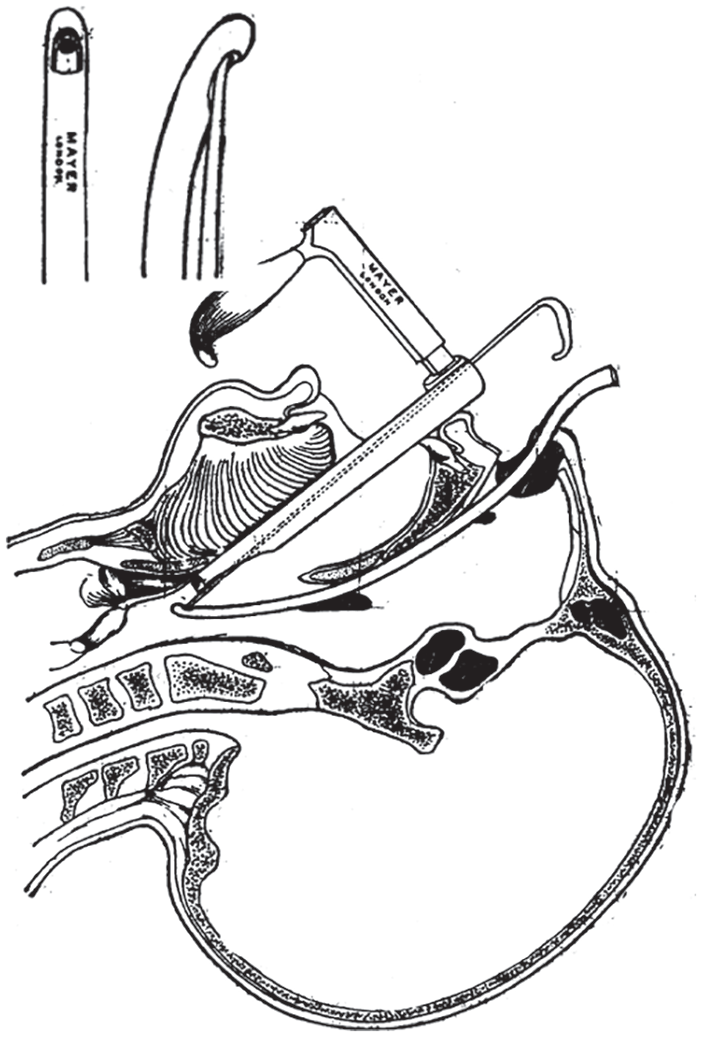
Laryngoscopic nasotracheal intubation with a “guiding rod” to advance the Silk tube into the glottis (insert). Modified after Rowbotham. 3
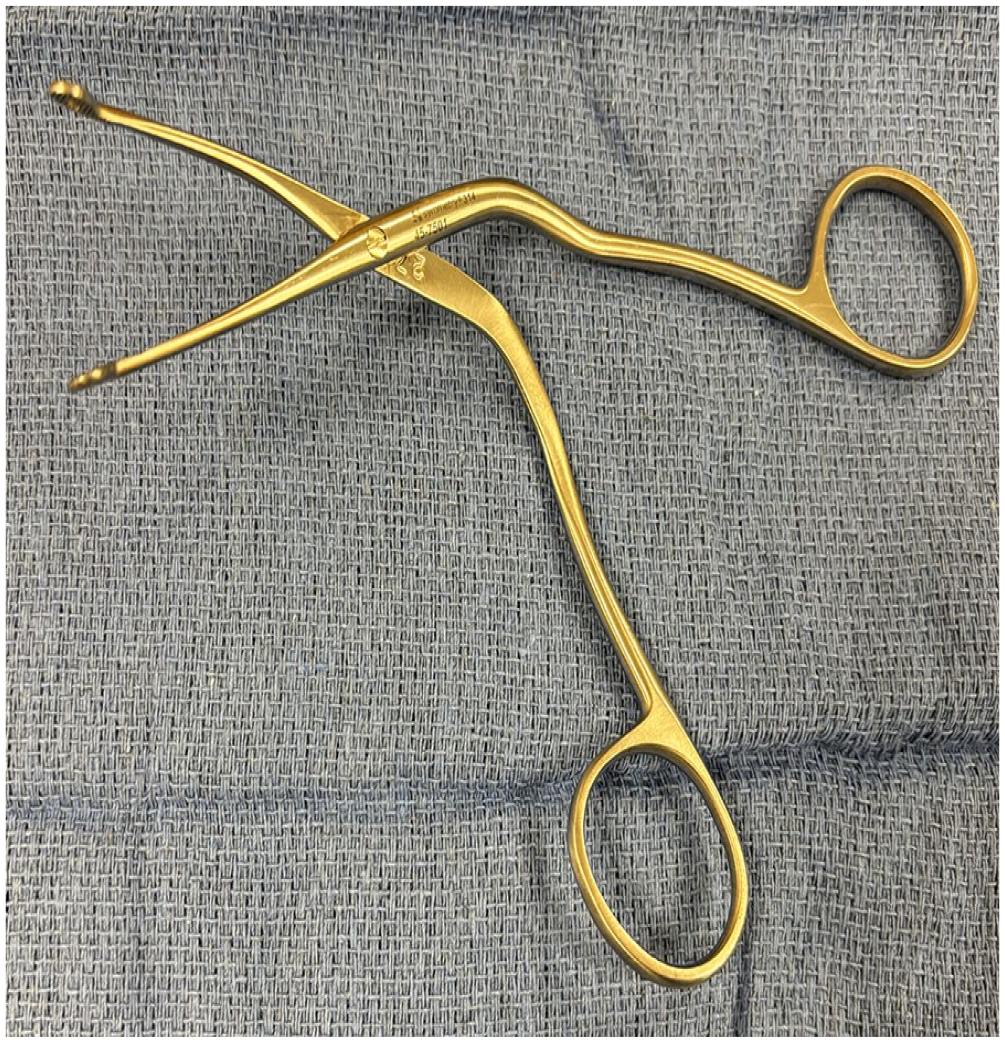
Magill forceps. The double curvature and serrated jaws facilitate endotracheal tube advancement and foreign body removal. Courtesy Elizabeth Drum, MD.
Magill’s forceps proved ideal for manipulation in the mouth and oropharynx. They have found use in advancing nasogastric tubes, 5 removing oropharyngeal coins 6 and occasionally swallowed dentures. In combination with a video-laryngoscope or fluoroscopy, Magills have been used to remove safety pins and marbles from the proximal esophagus. 7
Magill’s ingenuity led to an array of useful gadgets and techniques. He is credited with the first handheld laryngoscope with batteries in the handle, a portable nitrous oxide apparatus, and a bronchial blocker for single lung ventilation. He introduced the agent pentobarbital to the United Kingdom and was among the first to use curare as a paralytic agent in thoracic surgery. For his commitment and extraordinary contributions to the field of anesthesiology, Magill received honors including membership in the Royal Society of Medicine and knighthood in 1960.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Evidence
5—Expert opinion.