
Abstract

Significance Statement
This case illustrates a rare presentation of Eagle syndrome presenting with facial nerve palsy and highlights the successful management through a transmastoid decompression approach, sparing complete styloid resection. The patient’s functional recovery emphasizes the potential utility of targeted decompression in cases with facial nerve compression at the stylomastoid foramen.
Case Report
A 63-year-old man known for hypertension presented with sudden, complete left facial nerve paresis, with no improvement after an initial course of high-dose oral steroids prescribed in the emergency department. On further questioning, he reported mild pain and discomfort in the ipsilateral jaw for many years. He denied any history of trauma.
Upon assessment in the otolaryngology clinic 4 months post-symptom onset, examination showed no recovery of facial movement, and a suspected prominent styloid process palpable transcervically. Computed tomography and magnetic resonance imaging of the head and neck were thus obtained, showing marked thickening and elongation of the left styloid process impinging on the stylomastoid foramen and causing foraminal stenosis (Figure 1). A transmastoid facial nerve decompression was offered, with extensive preoperative counseling on the lack of clear evidence that radiologic findings necessarily correlated with his symptomatology. He underwent a lower lid ectropion repair by our ophthalmology colleagues.
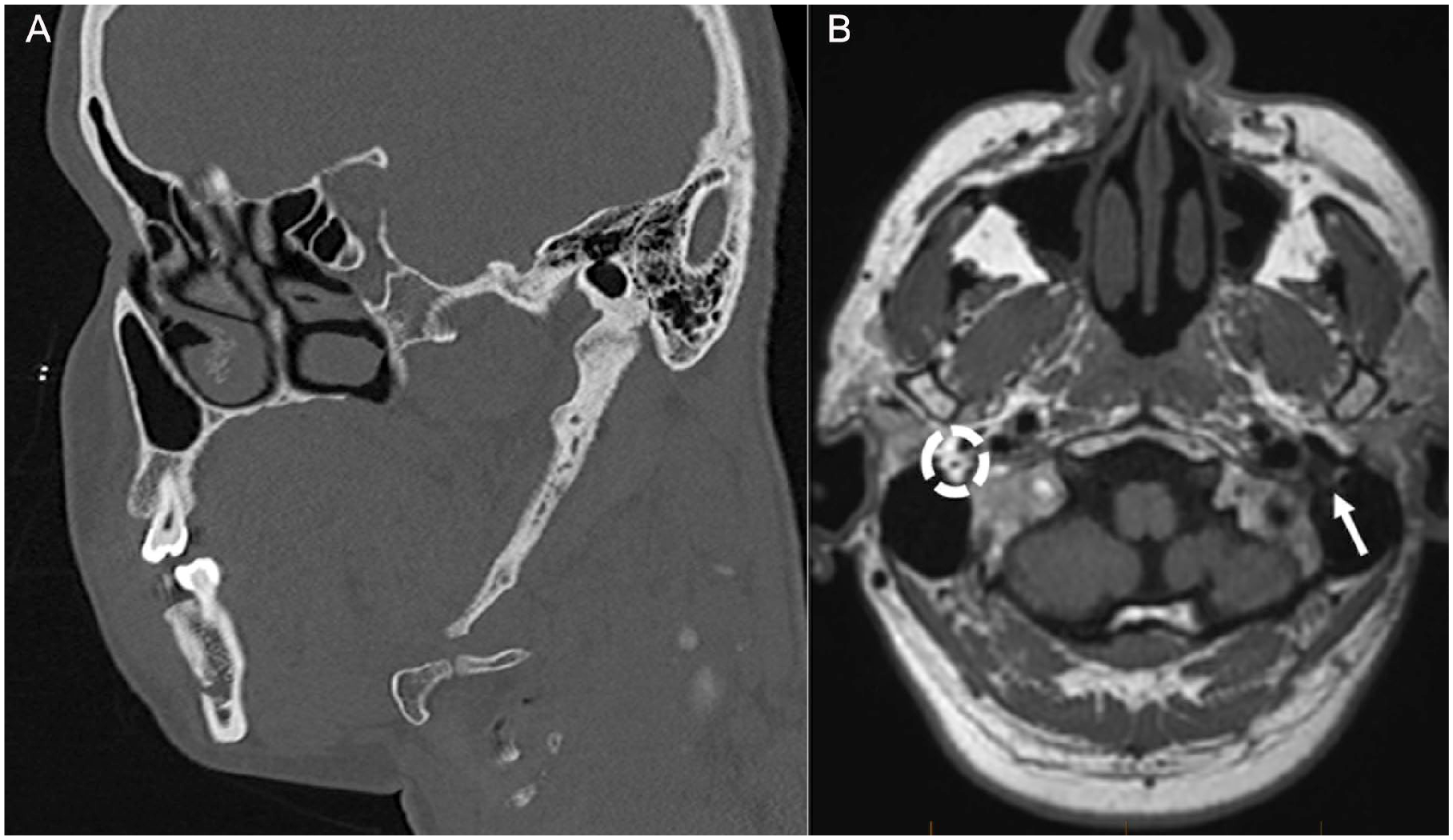
Oblique computed tomography reformat along the axis of the markedly elongated styloid process (A) and axial non-enhanced T1 magnetic resonance imaging showing loss of the normal fat signal surrounding the facial nerve at the left stylomastoid foramen (arrow), normal signal circled on contralateral side for comparison (B).
He was taken to the operating room 6 months post-onset of the facial paralysis. A mastoidectomy was performed, and the mastoid segment of the facial nerve was carefully uncovered up until the stylomastoid foramen. A transcervical or transoral approach for complete resection of the styloid was deemed unnecessary, as the transmastoid approach provided sufficient access to the narrowed stylomastoid foramen. The bony protuberance at the base of the styloid process was carefully drilled, and the styloid process thinned and fully disconnected from the mastoid fully liberating the nerve. The epineurium was incised along the length of the mastoid segment, with immediate expansion of the nerve noted intra-operatively (Figure 2).
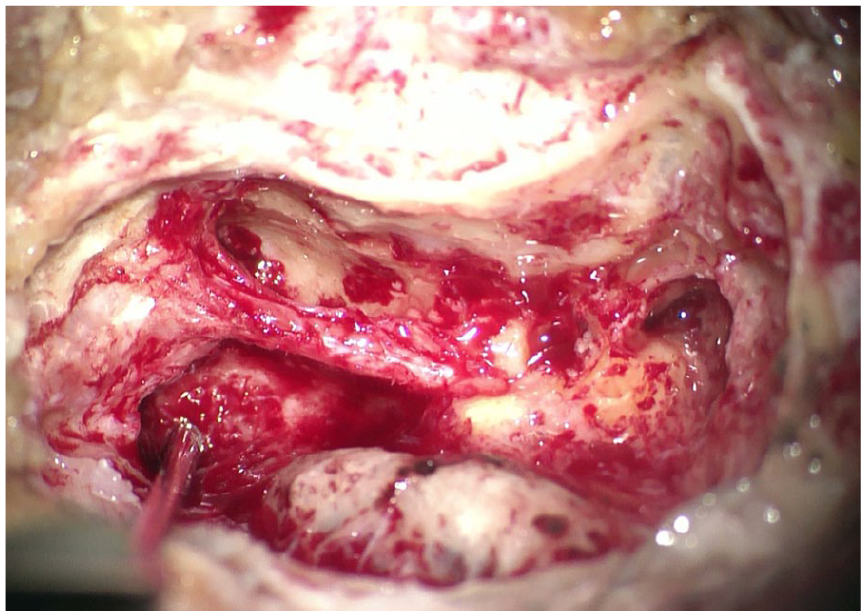
Intra-operative photo showing the exposed facial nerve, decompressed in its mastoid segment and at the stylomastoid foramen, with incised epineurium.
The patient recovered very well from the surgery, with no postoperative vertigo, hearing loss, or other complications. He was referred for facial retraining therapy with an experienced speech-language pathologist. At 3-month follow-up, he already noticed more facial tone and early volitional movement of the oral commissure and periocular complex. At 1-year follow-up, he improved further with complete eye closure with effort. While he did have residual asymmetry and some periocular synkinesis with a smile, he had excellent resting tone, no functional deficits, and was very satisfied with his outcome (Figure 3).

Postoperative facial movement at 1-year post-decompression shows good resting tone, full eye closure, and a volitional smile despite residual asymmetry.
Discussion
First described by Watt W. Eagle in 1937, Eagle syndrome (ES) is a rare condition including a constellation of symptoms explained by an elongated styloid process or mineralization of the stylohyoid ligament, including neck and orofacial pain. 1 Symptoms may result from either direct cranial nerve impingement or through impingement of the carotid vessels and surrounding sympathetic plexus (termed styloid-carotid artery syndrome). 2 While radiographic evidence of an elongated styloid (classically greater than 3 cm) may be apparent in 4% of the population, only 4% of those with radiologic findings are clinically symptomatic. 1 Thus, radiologic evidence of an elongated styloid is solely supportive of the diagnosis in the appropriate clinical context.
The pathogenesis of ES is debated, with various theories including congenital etiologies, reactive ossifying hyperplasia from chronic irritation, post-traumatic osseous metaplasia, or endocrinopathies. 1 In a histological and immunohistochemical study of osteogenetic changes of the styloid process in ES patients, Kim et al identified a potential for both axial growth secondary to callus-induced endochondral ossification and apical growth due to intramembranous ossification when subject to tensile strength. 3 Axial enlargement at the styloid foramen may lead to compression of the facial nerve as it exits the skull base. 2
Facial nerve palsy secondary to ES is exceedingly rare, with fewer than 10 cases documented in the literature (Table 1).2,4-9 While most patients presented with acute facial nerve paralysis, cases of progressively worsening or intermittent weakness have also been described.7,8 Most patients had associated symptoms, interestingly often reporting a subacute or chronic history of radiating neck or jaw pain suggestive of an underlying slowly evolving process prior to eventual facial nerve compression, as was the case in our patient.4,6,9 While initial conservative management with oral steroids and possibly facial neuromuscular training therapy may be beneficial, most patients ultimately underwent surgical intervention.
Reported Cases of Eagle Syndrome Causing Facial Nerve Weakness in the English Literature
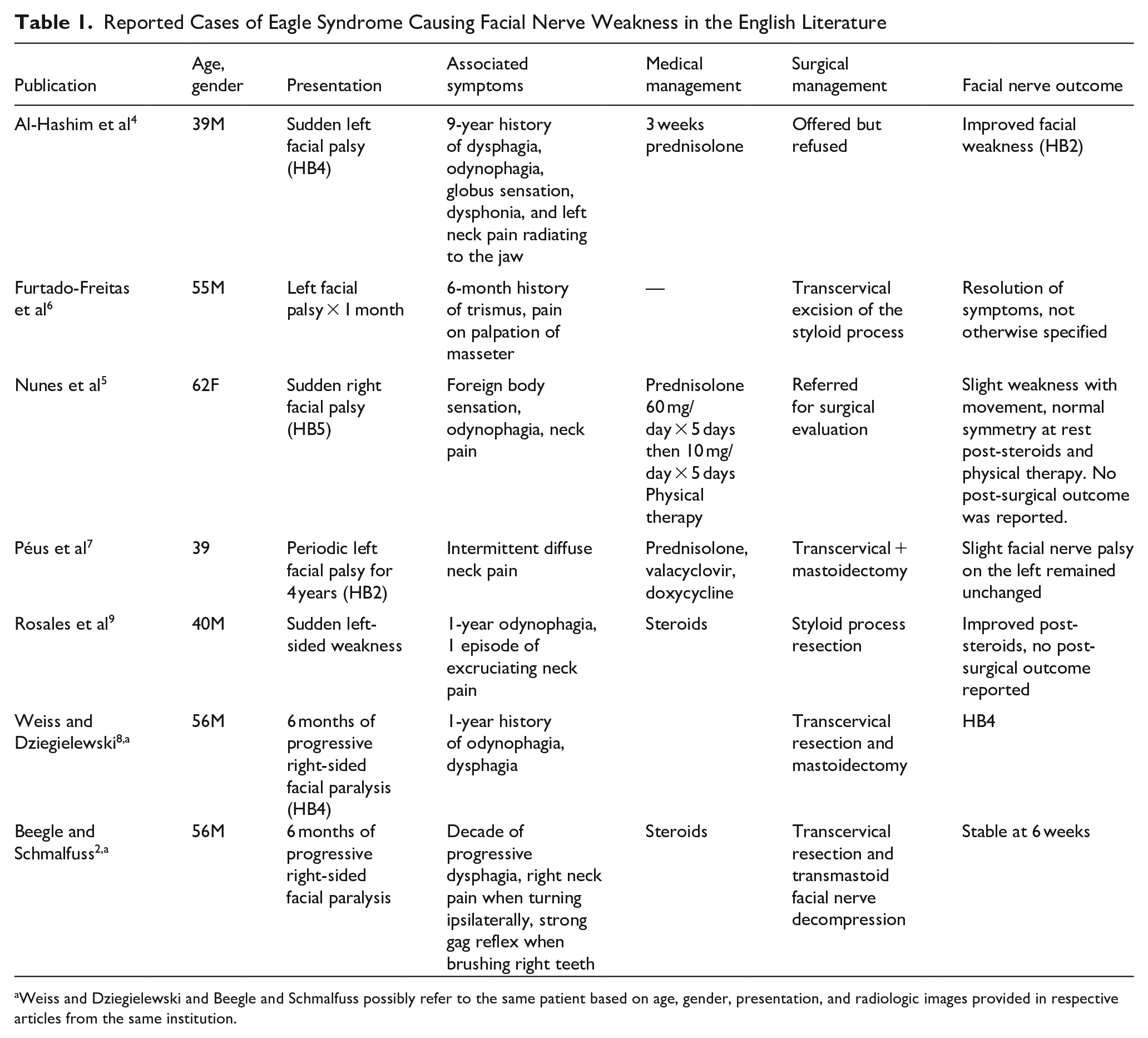
Weiss and Dziegielewski and Beegle and Schmalfuss possibly refer to the same patient based on age, gender, presentation, and radiologic images provided in respective articles from the same institution.
Most authors describe performing an entirely transcervical, transoral, or combined transmastoid/transcervical styloidectomy, with varying outcomes.2,6-9 We are the first to report transmastoid decompression allowing nerve expansion at the compressed stylomastoid foramen without full styloid resection. This approach provided excellent visualization and minimal morbidity, yielding favorable results with excellent facial nerve recovery despite delayed decompression at 6 months post-onset. This rare case of ES with facial paralysis expands the limited literature and highlights that avoiding full styloidectomy may reduce morbidity while achieving effective symptom resolution and recovery.