
Abstract
A rare congenital nasopharyngeal hairy polyp was incidentally identified during an attempted adenoidectomy in a 15-month-old female. The patient presented with snoring and intermittent apnea concerning for upper airway obstruction. Magnetic resonance imaging (MRI) revealed a 2.5-cm partially enhancing nasopharyngeal mass along the soft palate, likely originating near the left nasopharyngeal wall or Eustachian tube orifice. The lesion was excised transorally without complications. Histopathological analysis confirmed a benign hairy polyp composed of mature adipose tissue, skeletal muscle, and cartilage, lined by keratinized squamous epithelium with underlying adnexa including pilosebaceous units. Postoperatively, the patient’s symptoms resolved. Interval postoperative MRI surveillance is planned for 6 months. This case highlights the importance of considering rare congenital lesions within the differential diagnosis of pediatric obstructive sleep symptoms. Early recognition and diagnosis can lead to appropriate surgical planning and better outcomes for these patients.
Introduction
Nasopharyngeal hairy polyps are extremely rare congenital lesions composed of mesodermal and ectodermal tissue. By 1989, approximately 120 cases had been reported, with a moderate increase in subsequent years. 1 The true prevalence and incidence remain unknown due to reliance on case reports. These lesions are believed to originate from the first or second pharyngeal arches and most commonly arise in the nasopharynx, oropharynx, or Eustachian tube.2,3 Diagnosis typically occurs in the neonatal period or early infancy, with reported ages ranging from 2 days to 26 months. 4 Symptoms generally present shortly after birth as upper airway obstruction, although cases in older children and adults have been documented.2,5 Prognosis is excellent following complete excision, and malignant transformation has not been reported. 4
Case Presentation
A 15-month-old female was referred for persistent snoring, nasal congestion, and occasional apnea associated with a nasopharyngeal mass. Her medical history included tympanostomy tube placement and a prior adenoidectomy attempt at an outside facility at 15 months of age that was discontinued upon discovery of the mass. Physical examination revealed a well-appearing child with a visible nasopharyngeal lesion. MRI demonstrated a 2.5-cm T1-hyperintense, partially enhancing mass along the soft palate, possibly attached to the left nasopharyngeal wall or Eustachian tube orifice (Figure 1). Given the absence of suspected bony involvement and the desire to avoid unnecessary radiation exposure, CT imaging was not pursued. One month later, at 16 months of age, the patient underwent transoral endoscopic removal under general anesthesia. The pediatric anesthesia department did not require pre-operative labs in this otherwise healthy child. The soft palate was suspended transnasally, and endoscopic visualization facilitated excision at the base. Hemostasis was achieved without complications, and critical structures, including the torus tubarius, were preserved. The excised specimen was well-circumscribed and contained multiple tissue types, including soft tissue, cartilage, and hair (Figure 2A-B). (A and B) Magnetic Resonance Imaging of the orbits showing the coronal (Image A) and axial (Image B) views. Note the partially enhancing mass in the nasopharynx along the soft palate (Medial arrow in image B). The mass has a questionable stalk-like appearance to the left nasopharyngeal wall or possibly the opening of the Eustachian tube (Lateral arrow in Image B) (A–D) Nasopharyngeal mass after excision (A), and endoscopic view of the mass adhering to the left nasopharyngeal wall or possibly the opening of the Eustachian tube (B). Histopathological demonstration of lobules of mature adipose tissue, admixed with skeletal muscle and cartilage, covered by keratinized squamous epithelium with hair follicles and associated sebaceous and seromucinous glands (C and D)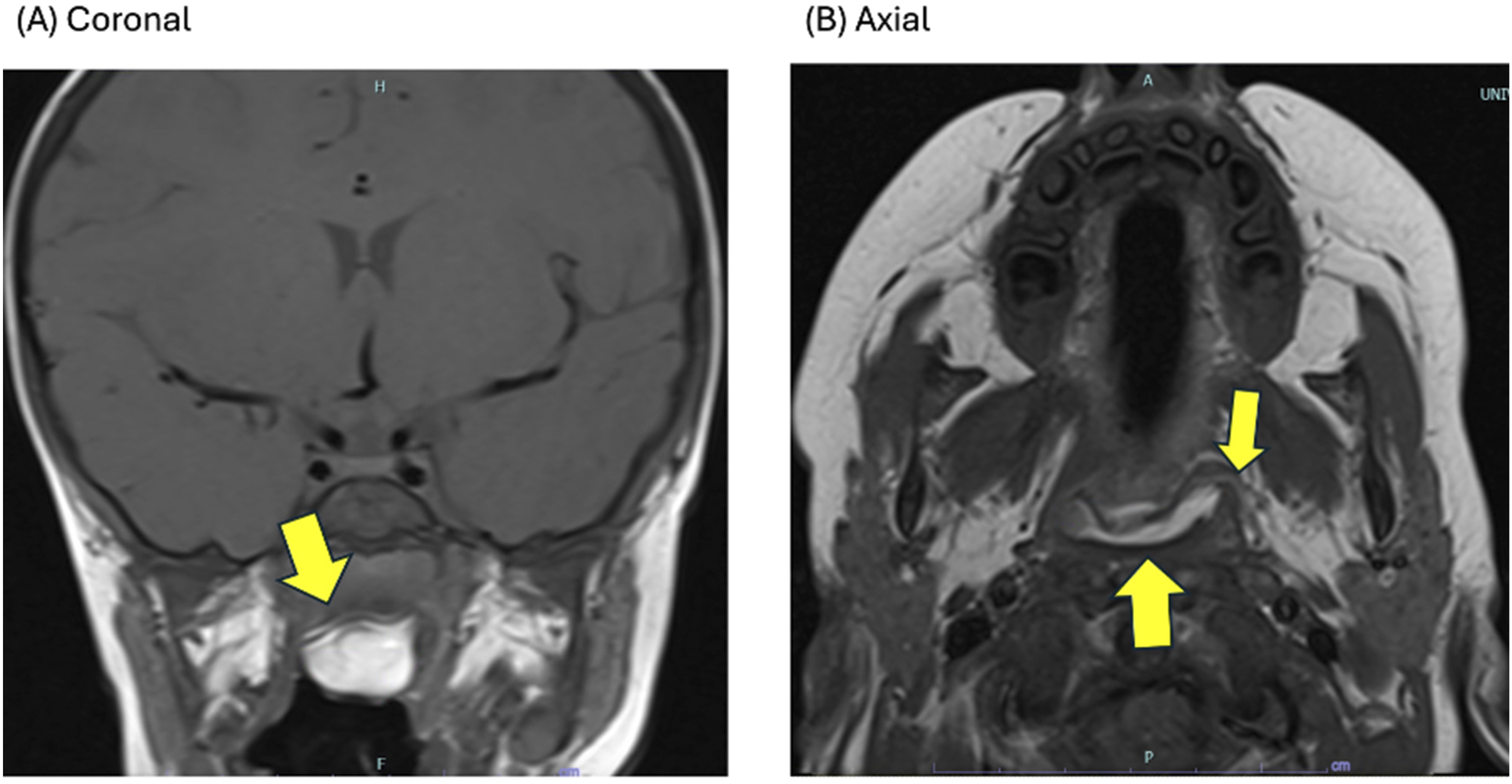
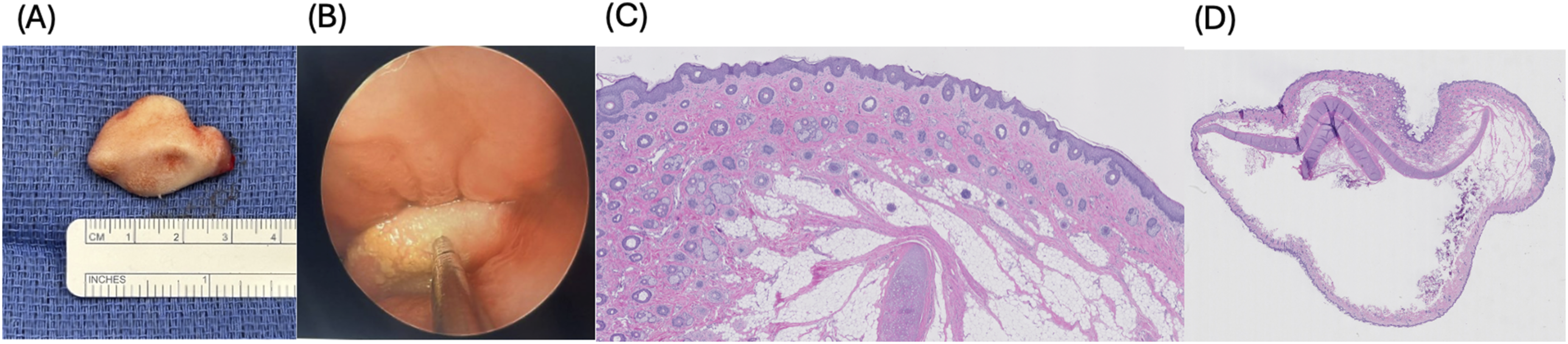
Histopathological evaluation revealed a polypoid mass composed of ectodermal and mesodermal elements without endodermal components. Specifically, lobules of mature adipose tissue admixed with skeletal muscle and cartilage covered by keratinized squamous epithelium with hair follicles and associated sebaceous and seromucinous glands (Figure 2C-D). These findings are consistent with a hairy polyp, a benign developmental malformation of bigerminal origin usually found in the nasopharynx.
The patient was seen 4 weeks postoperatively, at which time the caregivers reported no current complaints and improvement in both snoring and nasal congestion. Physical examination showed no evidence of persistent mass, additional lesions, or palatal abnormalities. Nasal endoscopy was not performed, given the complete resolution of symptoms as well as the reassuring physical examination findings. Post-operative polysomnography was not pursued since snoring was completely resolved, and parents had no concerns about her breathing. The patient additionally underwent evaluation with the pediatric neurosurgery service at this time, and an interval postoperative MRI is planned for 6 months.
Discussion
Nasopharyngeal hairy polyps are benign congenital malformations containing mature ectodermal and mesodermal elements, which may present with snoring, stridor, and intermittent sleep-disordered breathing. 2 Previous categorization of hairy polyps as dermoid polyps is no longer recommended, given that they lack a cystic component and consist of only two germ layers. The designation of hairy polyps as choristomas is considered more appropriate, as it more accurately defines this entity as normal mature tissue in an abnormal location. The characteristic hair bearing, stalk-like morphology distinguishes these lesions from other nasopharyngeal masses, including teratomas. Symptoms often resemble those of common pediatric conditions, such as adenotonsillar hypertrophy, often leading to diagnostic delays.
Despite their congenital origin, nasopharyngeal hairy polyps are often overlooked as a cause of neonatal and infant respiratory or feeding difficulties. 2 Even small lesions can result in significant airway obstruction, illustrating the importance of prompt diagnosis. 6 Smaller polyps can cause intermittent positional obstruction, which can lead to life-threatening respiratory events. 7 A review demonstrated that polyps measuring 3.0 cm or less were associated with an increased risk of respiratory distress, likely due to intermittent obstruction. 6
Persistent stridor, unexplained apnea, feeding difficulties, or sleep-disordered breathing unresponsive to standard interventions should prompt nasopharyngoscopic evaluation. When a lesion is identified, MRI is the preferred diagnostic modality due to its superior soft-tissue characterization and value in surgical planning. 8 In this case, MRI delineated the lesion and its stalk-like attachment near the Eustachian tube, consistent with previous reports. 2 CT imaging can also be used to provide complementary evaluation of adjacent bony structures; in this case, it was not necessary because the lesion’s stalk-like attachment was not near osseous anatomy on MRI. Complete excision at the base of attachment is curative and associated with an excellent prognosis. 4 Here, a combined endoscopic and transoral approach allowed precise resection near critical structures and facilitated safe, complete removal.
Histopathological examination confirms the diagnosis and typically reveals mature ectodermal and mesodermal tissue derivatives, including skin, adipose tissue, skeletal muscle, and cartilage. 9
This case highlights how congenital nasopharyngeal lesions, specifically hairy polyps, may initially mimic common pediatric conditions that lead to sleep-disordered breathing or persistent nasal congestion, such as adenoid hypertrophy, potentially delaying diagnosis until surgical intervention is attempted. While prior literature demonstrates that these lesions can cause clinically significant obstructive symptoms, this case further illustrates that even relatively small nasopharyngeal polyps can produce such symptoms and remain unrecognized despite prior otolaryngologic evaluation. In addition, the lesion’s proximity to the Eustachian tube illustrates the importance of detailed preoperative imaging and endoscopic visualization to facilitate safe resection while preserving adjacent critical structures.
Conclusion
This case underscores the importance of considering nasopharyngeal hairy polyps in infants with unexplained upper airway symptoms. Early diagnosis and complete surgical excision provide excellent outcomes.
Footnotes
Acknowledgements
The authors thank the patient’s family for their cooperation and consent for publication. The authors used AI-assisted tools for language editing and clarity.
Ethical Considerations
This study was approved by the Institutional Review Board.
Consent to Participate
Written informed consent has been obtained from the patient’s mother prior to proceeding with this case report.
Consent for Publication
Written informed consent for publication of the patient’s clinical details and any accompanying images was obtained from the patient.
Author Contributions
Hunter Hammett, BS, served as the first author and was responsible for manuscript preparation, figure organization, and conducting the literature review to support and contextualize the study. Jeffrey D. Carron, MD, serves as the senior author and corresponding author, providing overall project oversight and contributing to critical revisions of the manuscript. Amy K. Krecker, MD, performed the operative procedure, contributed essential clinical details of the case, and assisted with manuscript revisions. Samantha L. Payton, DO, contributed to the interpretation and editing of the pathology slides, assisted with the primary pathological assessment, and oversaw revisions related to the pathology components of the manuscript. Varsha Manucha, MD, contributed to the pathology analysis, assisted in obtaining the pathology slides, and participated in revising the pathology sections of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated.