
Abstract
Objectives
Locally advanced laryngeal cancer (LALC) treatment options include surgery followed by postoperative radiotherapy (PORT) or chemoradiotherapy (POCRT) versus non-surgical definitive radiotherapy (RT) or chemoradiotherapy (CRT). Their comparative efficacy remains debated. This study aimed to evaluate survival outcomes and prognostic factors in LALC patients receiving postoperative (PORT/POCRT) versus definitive (RT/CRT) treatment.
Methods
We retrospectively enrolled 210 LALC patients treated at our hospital (2010–2021). Overall survival (OS) and progression-free survival (PFS) were analyzed. Prognostic factors were identified using multivariate Cox regression.
Results
Median follow-up was 46 months. Median, 3- and 5-year OS was 70 months, 73.2%, and 57.7%, respectively, while the corresponding PFS was 45 months, 55.8%, and 41.3%. Multivariate analysis identified Karnofsky Performance Status (KPS) score, pathological differentiation, and pretreatment prognostic nutritional index (PNI) as independent risk factors for OS and PFS; second primary cancer and lesion site were independent risk factors for PFS. PORT/POCRT was associated with significantly higher local control and PFS than definitive CRT (P < 0.05). Both PORT/POCRT and definitive CRT were associated with significantly better OS and PFS than definitive RT alone (P < 0.05).
Conclusion
Higher KPS, moderate-to-high differentiation, and higher PNI predict better OS and PFS. Absence of a second primary cancer and presence of a glottic primary tumor predict better PFS. PORT/POCRT was most effective, followed by definitive CRT; definitive RT alone was least effective.
1. Introduction
Laryngeal cancer has the second highest incidence rate among head and neck cancers, and accounts for 30%–40% of all head and neck cancers and 1%–5% of all malignancies.1,2 Moreover, at the time of initial diagnosis, approximately 40%–50% of patients are found to have locally advanced disease, defined as T1–2 N1–3 or T3–4 any N, and have a relatively poor prognosis.3,4 Major risk factors include smoking and regular alcohol consumption. 5 The treatment strategies for locally advanced laryngeal cancer (LALC) include surgery or radiotherapy-based regimens. Most LALC patients require surgery followed by adjuvant postoperative radiotherapy (PORT) or postoperative chemoradiotherapy (POCRT), especially those with positive/close margins or extracapsular lymph node invasion. 6 However, the Veterans’ Affairs (VA) study and the Radiation Therapy Oncology Group (RTOG) 91-11 study have reported that concurrent chemoradiotherapy (CRT) or induction chemotherapy followed by radiotherapy (RT) improved laryngeal preservation rates and quality of life, and yielded efficacy rates similar to that of surgery-based comprehensive therapy.7,8 However, other studies have suggested that non-surgical treatment for LALC is inferior to surgical treatment.9,10 Hence, the present retrospective study aimed to comparatively analyze the treatment efficacy and prognostic factors in LALC patients treated with surgery followed by PORT or POCRT vs. patients treated non-surgically with definitive RT, either alone or combined with chemotherapy (CRT).
2. Methods
2.1 Patient Selection
We retrospectively enrolled LALC patients who were treated at our hospital between January 2010 and December 2021, and satisfied the following criteria: (1) patients with histologically or cytologically confirmed squamous cell carcinoma or other carcinomas; (2) patients diagnosed for the first time at our hospital, and confirmed to have LALC using the American Joint Committee on Cancer (AJCC) 7th or 8th edition TNM classification (T1–2 N1–3 M0 or T3–4 any N M0) without distant metastasis at initial diagnosis and at least one measurable lesion on imaging studies; (3) patients treated with surgery followed by PORT or POCRT, or those treated non-surgically with definitive RT alone or CRT; and (4) patients with complete clinical records and detailed pre- and post-treatment data.
We excluded patients who (1) had early-stage laryngeal cancer (T1–2 N0 M0) or distant metastasis (M1) at the time of initial diagnosis; (2) received palliative treatment only or had recurrent disease at the time of initial presentation to our hospital; or (3) had incomplete clinical records or missing follow-up data.
The diagnosis of laryngeal cancer was initially made via fiberoptic laryngoscopy and microlaryngoscopy with biopsy. Subsequently, imaging studies including contrast-enhanced computed tomography (CT) and/or magnetic resonance imaging (MRI) of the neck and chest were performed for TNM staging.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the ethics committee of the *** Hospital of *** University (approval code: 2022KT262), and the need for written informed patient consent was waived by the ethics committee due to the retrospective nature of this study.
2.2 Hematological Indicators
We collected pretreatment data on the following hematological indicators: total white blood cell, lymphocyte, neutrophil, monocyte, and platelet counts, and albumin and fibrinogen levels. We used the above information to calculate the following parameters: platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), fibrinogen-to-lymphocyte ratio (FLR), fibrinogen-to-albumin ratio (FAR), systemic immune-inflammation index (SII), and prognostic nutritional index (PNI). We calculated SII by using the equation SII = P × N/L, where P, N, and L are the pre-treatment peripheral blood platelet, neutrophil, and lymphocyte counts per liter, respectively. We calculated PNI by using the equation PNI = [(10 × serum albumin (g/dL)) + (0.005 × total lymphocyte count)]. Subsequently, we determined the optimal cutoff values for the above ratios and indices by using receiver operating characteristic (ROC) curve analysis and X-tile software (v3.6.1): NLR, 2.6; PLR, 169.2; LMR, 2.7; SII, 391.0; PNI, 48.3; FLR, 2.7; and FAR, 96.4.
2.3 Treatment Modalities
2.3.1 Radiotherapy
Patients received either intensity-modulated RT or tomotherapy using 6 MV X-rays. The target volumes included the gross tumor volume (GTV), GTV-postoperative tumor bed (GTV-tb), GTV-positive lymph nodes (GTVnd), high-risk clinical target volume (CTV1), and low-risk clinical target volume (CTV2). GTV and GTV-tb were expanded by 3–5 mm to create the planning GTV (PGTV) and planning tumor volume-postoperative tumor bed (PTV-tb), respectively, and CTV1 and CTV2 were expanded by 3–5 mm to create PTV1 and PTV2, respectively. Conventional fractionation was used, with 5 fractions per week. The median duration of radiotherapy was 6.5 weeks (range: 4–8 weeks). In the non-surgical group, the doses of RT ranged from 32 to 72.6 Gy (median dose: 67.5 Gy, median dose for CRT alone: 66 Gy, and median dose for RT alone: 69 Gy). In the surgical group, the doses of PORT/POCRT ranged from 50 to 69.96 Gy (median dose: 60.2 Gy).
2.3.2 Chemotherapy
Chemotherapy was primarily based on platinum-containing regimens. According to its timing relative to RT, chemotherapy was classified as induction chemotherapy, concurrent CRT, and adjuvant chemotherapy.
In the non-surgical group, 58 patients received RT combined with chemotherapy; among them, 42 patients received induction chemotherapy with the following regimens: TP regimen (paclitaxel + platinum; 25 patients), FLP regimen (fluorouracil + leucovorin + platinum; 6 patients), PVF regimen (vincristine + nedaplatin + fluorouracil; 5 patients), PF regimen (platinum + fluorouracil; 4 patients), TPF regimen (paclitaxel + platinum + fluorouracil; 1 patient), and CPF regimen (boanmycin + platinum + fluorouracil; 1 patient). Concurrent CRT was administered to 22 patients in the non-surgical group, by using the following regimens: TP regimen (14 patients), single-agent paclitaxel (2 patients); single-agent platinum (2 patients), single-agent S-1 (tegafur + gimeracil + oteracil potassium; 2 patients), and FLP regimen (2 patients). Adjuvant chemotherapy was administered to 24 patients in the non-surgical group, by using the following regimens: TP regimen (13 patients), FLP regimen (6 patients), PVF regimen (3 patients), PC regimen (cyclophosphamide + nedaplatin; 1 patient), and GP regimen (gemcitabine + cisplatin; 1 patient).
In the surgical group, 37 patients received adjuvant chemotherapy with the TP regimen (20 patients), FLP regimen (12 patients), PVF regimen (2 patients), EP regimen (etoposide + cisplatin; 2 patients), and CPF regimen (1 patient). CCRT was administered to 19 patients, with the TP regimen (12 patients), FLP regimen (5 patients), single-agent T (1 patient), and EP regimen (1 patient).
2.3.3 Surgery
The surgical procedures performed in our patients included total laryngectomy (27 patients), partial laryngectomy (69 patients), and transoral laser resection (5 patients), with laryngeal reconstruction and unilateral or bilateral neck dissection, as indicated. Transoral laser resection was performed in select patients with early T-stage (e.g., T1/T2) but N+ disease, which was considered locally advanced disease due to the nodal status.
2.3.4 Statistical Analysis
Statistical analyses were conducted using SPSS (v29.0) software [IBM Corp., Armonk, NY, USA]. Categorical data and their intergroup differences were analyzed using the chi-square test. The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. As the data were not normally distributed, continuous variables are presented as medians (ranges). Continuous variables were analyzed using ROC curves and X-tile software to determine optimal cutoff values for dichotomization. Survival analysis was performed using the Kaplan–Meier method, and differences in survival data between groups were tested using the log-rank test. The Cox proportional hazards model was used to perform multivariate analysis. Differences with P-values < 0.05 were considered to be statistically significant.
3. Results
3.1 Patient Characteristics
Clinical Characteristics of Patients With Locally Advanced Laryngeal Cancer
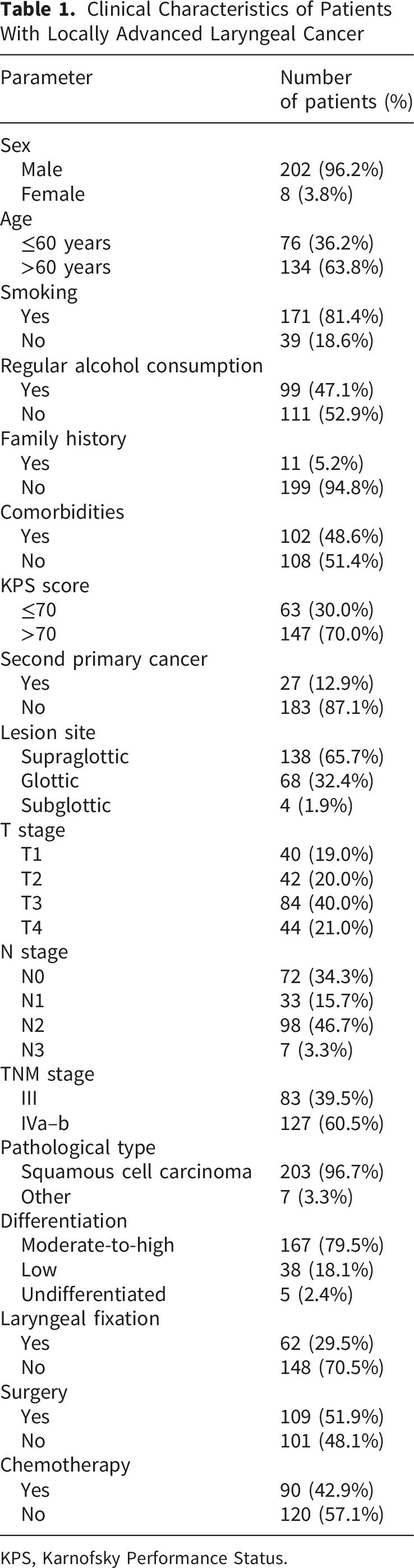
KPS, Karnofsky Performance Status.
3.2 Treatment Outcomes
By the end of the follow-up, 105 of the 210 patients (50.0%) had died. The causes of death are detailed in Supplementary Table S1.
Tumor progression occurred in 79 patients by the end of the follow-up period. Locoregional recurrence occurred in 57 patients, including 37 patients with recurrence in the larynx (with concurrent cervical lymph node disease in 7 patients) and 20 patients with regional lymph node recurrence alone (cervical lymph nodes in 16 patients, parapharyngeal lymph nodes in 1 patient, submandibular and submental lymph nodes in 1 patient, parotid lymph nodes in 1 patient, and supraclavicular lymph nodes in 1 patient). Distant metastasis occurred in 22 patients, with single-organ metastasis occurring in 17 patients and multiple metastases occurring in 5 patients. Lung metastasis occurred in 16 patients, extraregional lymph node metastasis in 6 patients, liver metastasis in 2 patients, bone and bone marrow metastasis in 2 patients, spleen metastasis in 1 patient, and brain metastasis occurred in 1 patient.
3.3 Overall Survival
Univariate Analysis of Potential Influencing Factors for OS in LALC Patients
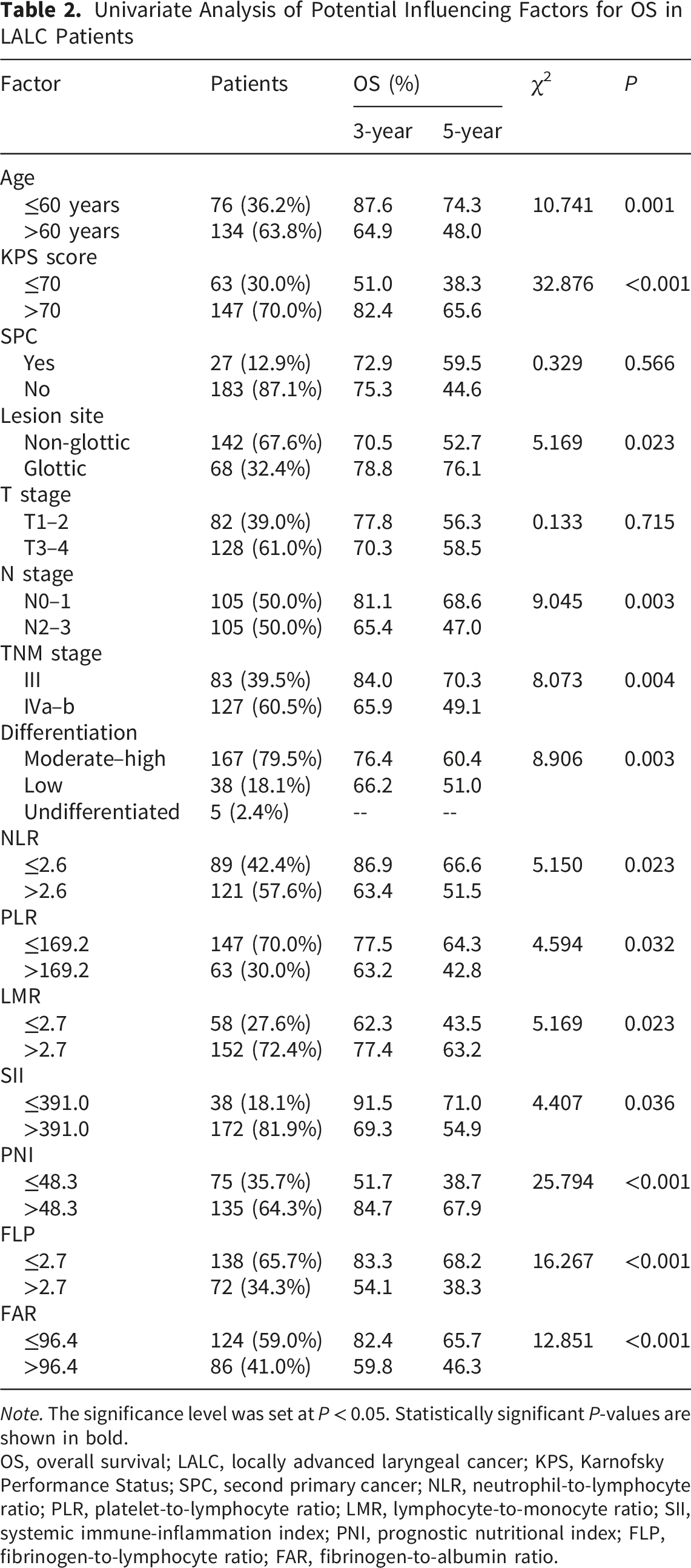
Note. The significance level was set at P < 0.05. Statistically significant P-values are shown in bold.
OS, overall survival; LALC, locally advanced laryngeal cancer; KPS, Karnofsky Performance Status; SPC, second primary cancer; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SII, systemic immune-inflammation index; PNI, prognostic nutritional index; FLP, fibrinogen-to-lymphocyte ratio; FAR, fibrinogen-to-albumin ratio.
Multivariate Analysis of Influencing Factors for OS in LALC Patients
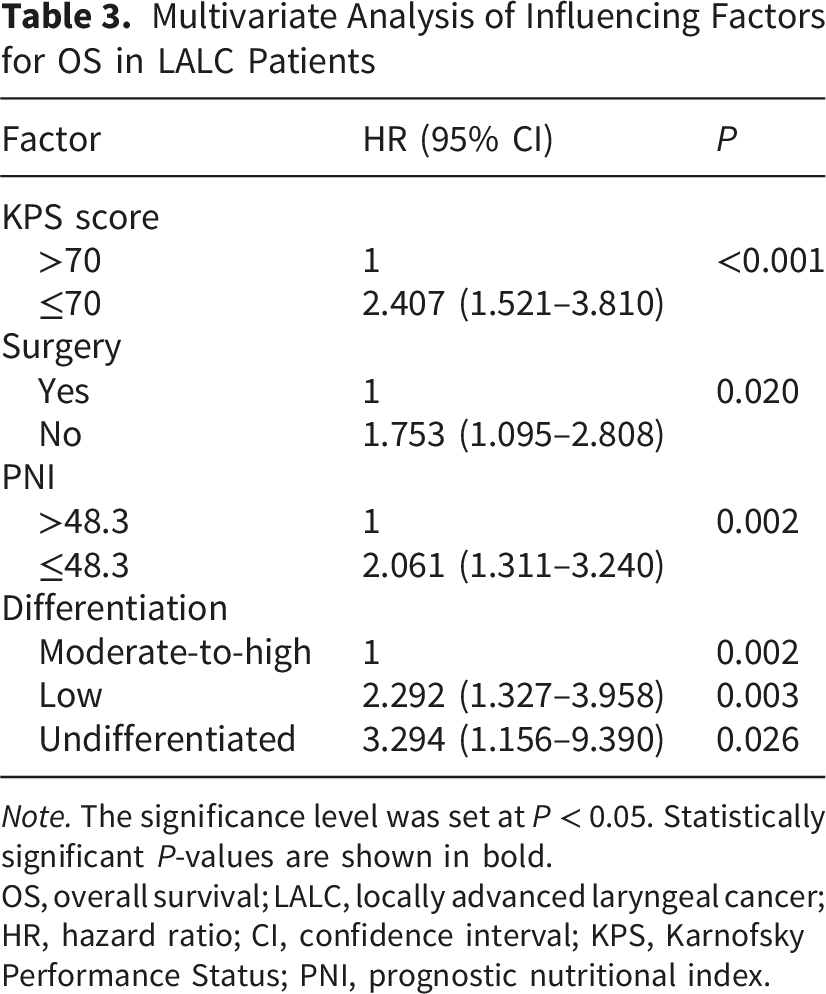
Note. The significance level was set at P < 0.05. Statistically significant P-values are shown in bold.
OS, overall survival; LALC, locally advanced laryngeal cancer; HR, hazard ratio; CI, confidence interval; KPS, Karnofsky Performance Status; PNI, prognostic nutritional index.
3.4 Progression-free Survival
Univariate Analysis of Potential Influencing Factors for PFS in LALC Patients
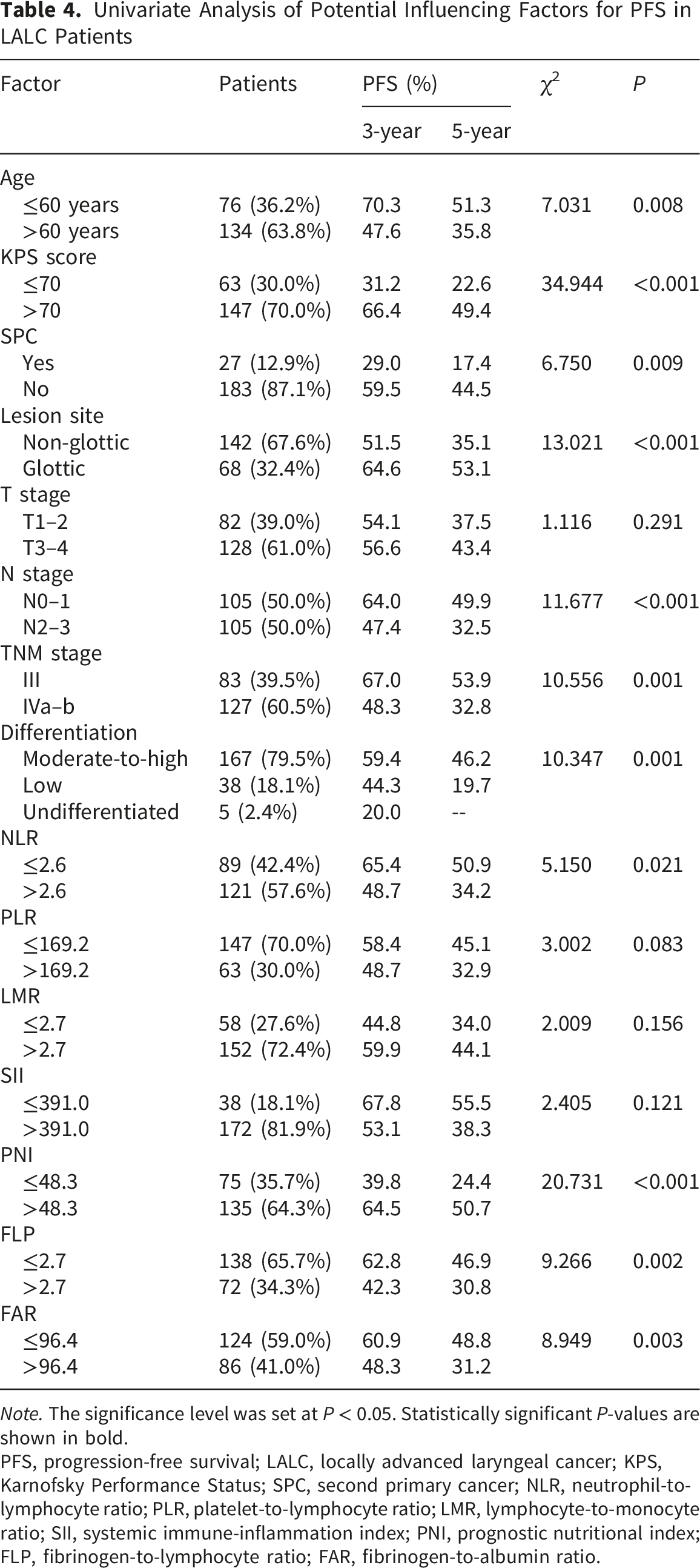
Note. The significance level was set at P < 0.05. Statistically significant P-values are shown in bold.
PFS, progression-free survival; LALC, locally advanced laryngeal cancer; KPS, Karnofsky Performance Status; SPC, second primary cancer; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SII, systemic immune-inflammation index; PNI, prognostic nutritional index; FLP, fibrinogen-to-lymphocyte ratio; FAR, fibrinogen-to-albumin ratio.
Multivariate Analysis of Factors Influencing PFS of LALC Patients
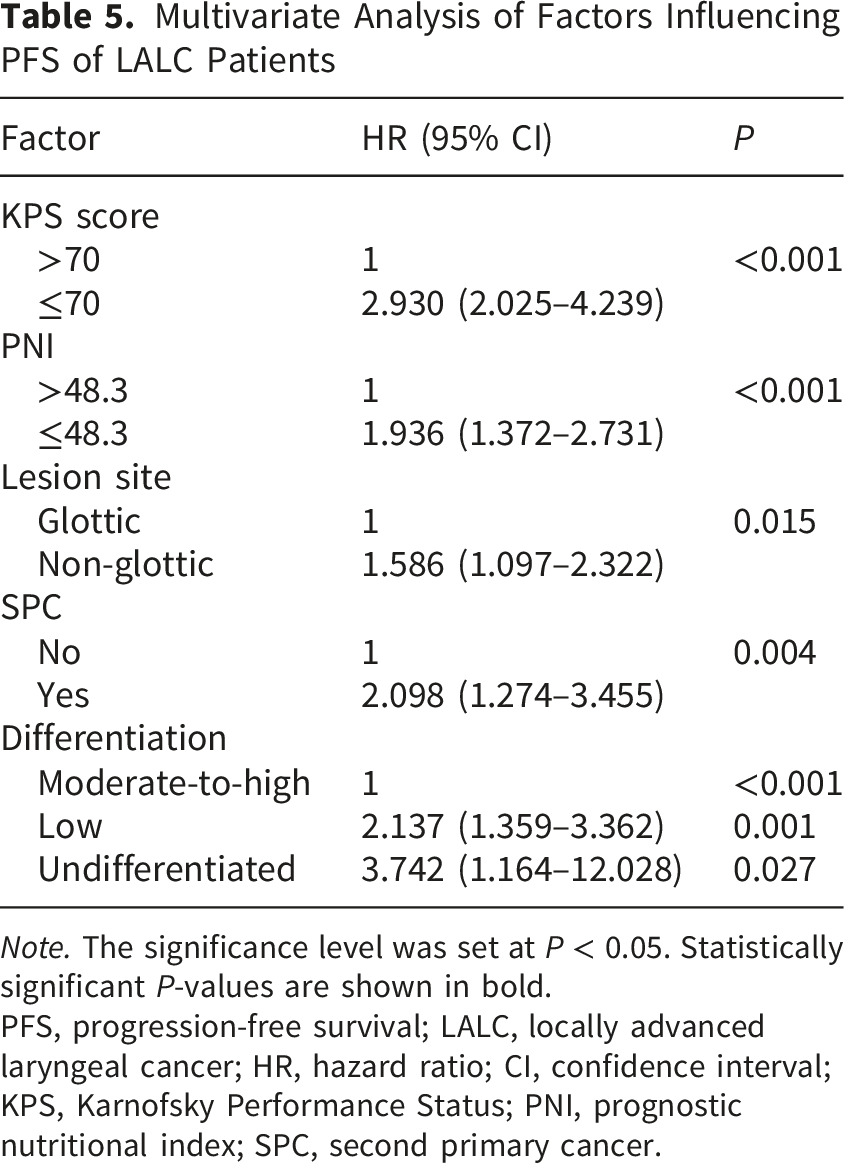
Note. The significance level was set at P < 0.05. Statistically significant P-values are shown in bold.
PFS, progression-free survival; LALC, locally advanced laryngeal cancer; HR, hazard ratio; CI, confidence interval; KPS, Karnofsky Performance Status; PNI, prognostic nutritional index; SPC, second primary cancer.
3.5 Comparison of Different Treatment Modalities
3.5.1 Clinical Characteristics
Comparison of Clinical Characteristics Among Different Treatment Groups
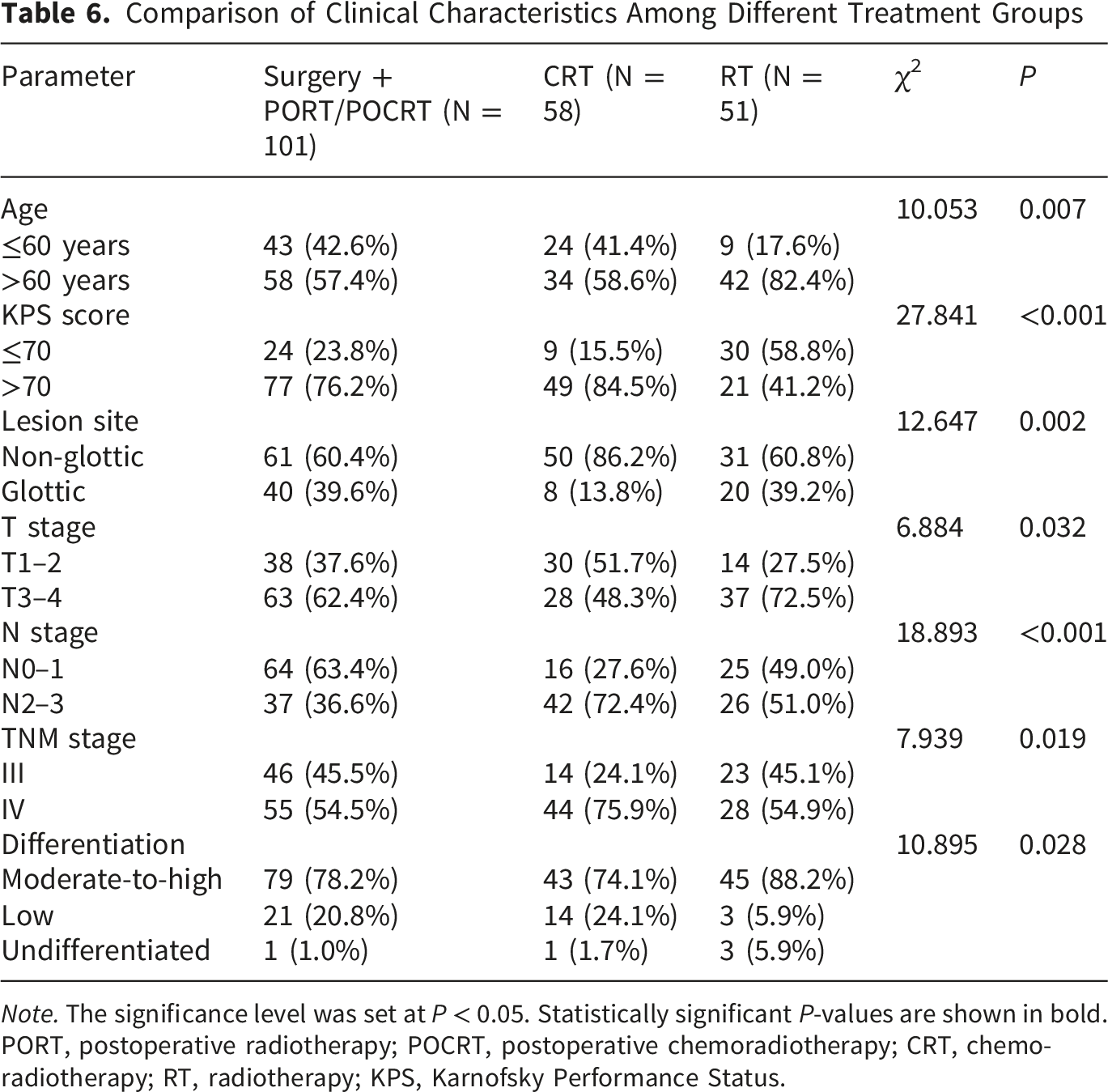
Note. The significance level was set at P < 0.05. Statistically significant P-values are shown in bold.
PORT, postoperative radiotherapy; POCRT, postoperative chemoradiotherapy; CRT, chemoradiotherapy; RT, radiotherapy; KPS, Karnofsky Performance Status.
Specifically, the surgery + PORT/POCRT group had a higher proportion of glottic tumors (40/101, 39.6%) than the CRT group (8/58, 13.8%) and the RT alone group (20/51, 39.2%; P = 0.002). Furthermore, the surgery + PORT/POCRT group had a significantly lower proportion of patients with N2-3 disease (37/101, 36.6%) than the CRT group (42/58, 72.4%; P < 0.001).
3.5.2 OS and PFS
The 3- and 5-year OS rates were 81.1% and 71.8%, respectively, in those treated with surgery + PORT/POCRT; 77.6% and 51.3%, respectively, in those treated with CRT; and 52.9% and 37.7%, respectively, in those treated with RT alone (χ2 = 23.707, P < 0.01). Post-hoc comparisons revealed that both the surgery + PORT/POCRT group and the CRT group had significantly better OS than the RT alone group (P < 0.001), while the difference between the surgery + PORT/POCRT group and the CRT group did not reach statistical significance (P = 0.057; Figure 1). Overall survival (OS) in patients with locally advanced laryngeal cancer (LALC) treated with surgery followed by postoperative radiotherapy (PORT) or postoperative chemoradiotherapy (POCRT) vs. chemoradiotherapy (CRT) vs. radiotherapy (RT) alone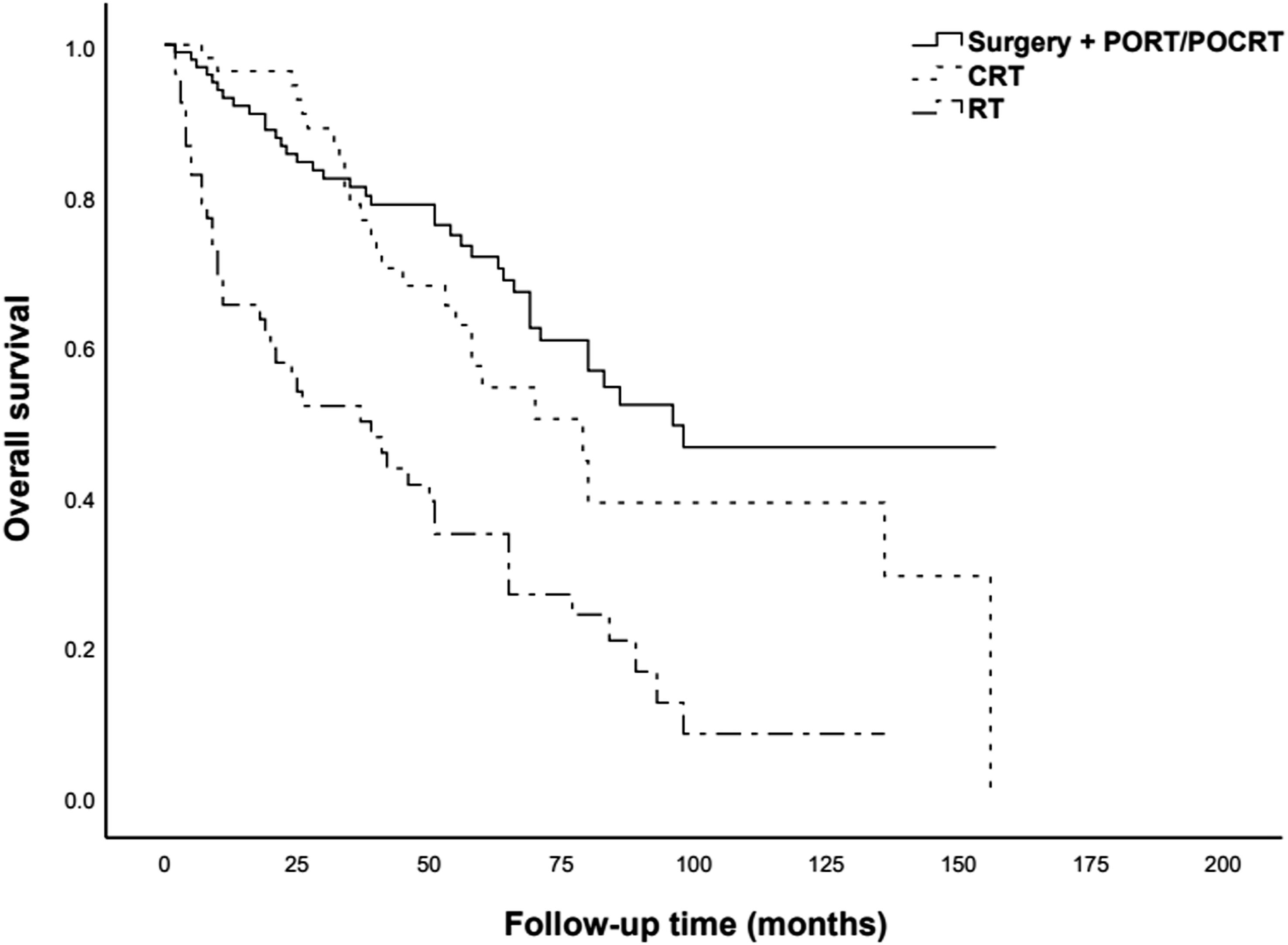
The 3- and 5-year PFS rates were 66.7% and 54.2%, respectively, in the surgery + PORT/POCRT group; 49.7% and 32.9%, respectively, in the CRT group; and 40.9% and 26.0%, respectively in the RT group (χ2 = 15.361, P < 0.01). Post-hoc comparisons revealed that the surgery + PORT/POCRT group had significantly better PFS than the CRT group (P = 0.018), and both the surgery + PORT/POCRT and CRT groups had significantly better PFS than the RT alone group (P < 0.001; Figure 2). Progression-free survival (PFS) in patients with locally advanced laryngeal cancer (LALC) treated with surgery followed by postoperative radiotherapy (PORT) or postoperative chemoradiotherapy (POCRT) vs. chemoradiotherapy (CRT) vs. radiotherapy (RT) alone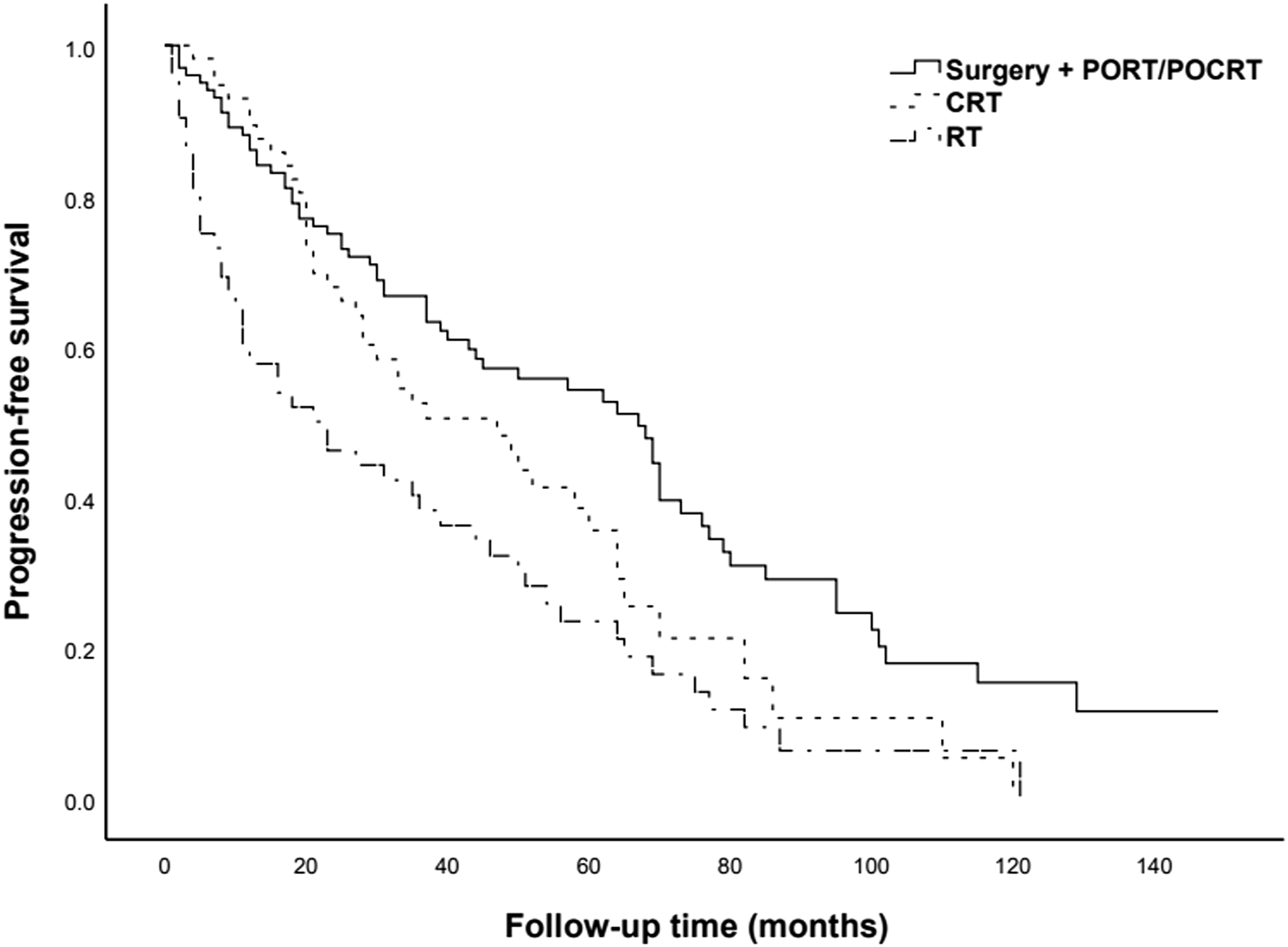
3.5.3 Locoregional Recurrence-free Survival
The 3- and 5-year locoregional recurrence-free survival (LRFS) rates were 87.4% and 83.4%, respectively, in the surgery + PORT/POCRT group; 63.3% and 46.0%, respectively, in the CRT group; and 50.0% and 33.9%, respectively, in the RT group (χ2 = 27.641, P < 0.01). Post-hoc comparisons revealed that the surgery + PORT/POCRT group had significantly higher LRFS than both the CRT group and the RT alone group (P < 0.001), and the CRT group had significantly higher LRFS than the RT alone group (P = 0.03; Figure 3). Locoregional recurrence-free survival (LRFS) in patients with locally advanced laryngeal cancer (LALC) treated with surgery followed by postoperative radiotherapy (PORT) or postoperative chemoradiotherapy (POCRT) vs. chemoradiotherapy (CRT) vs. radiotherapy (RT) alone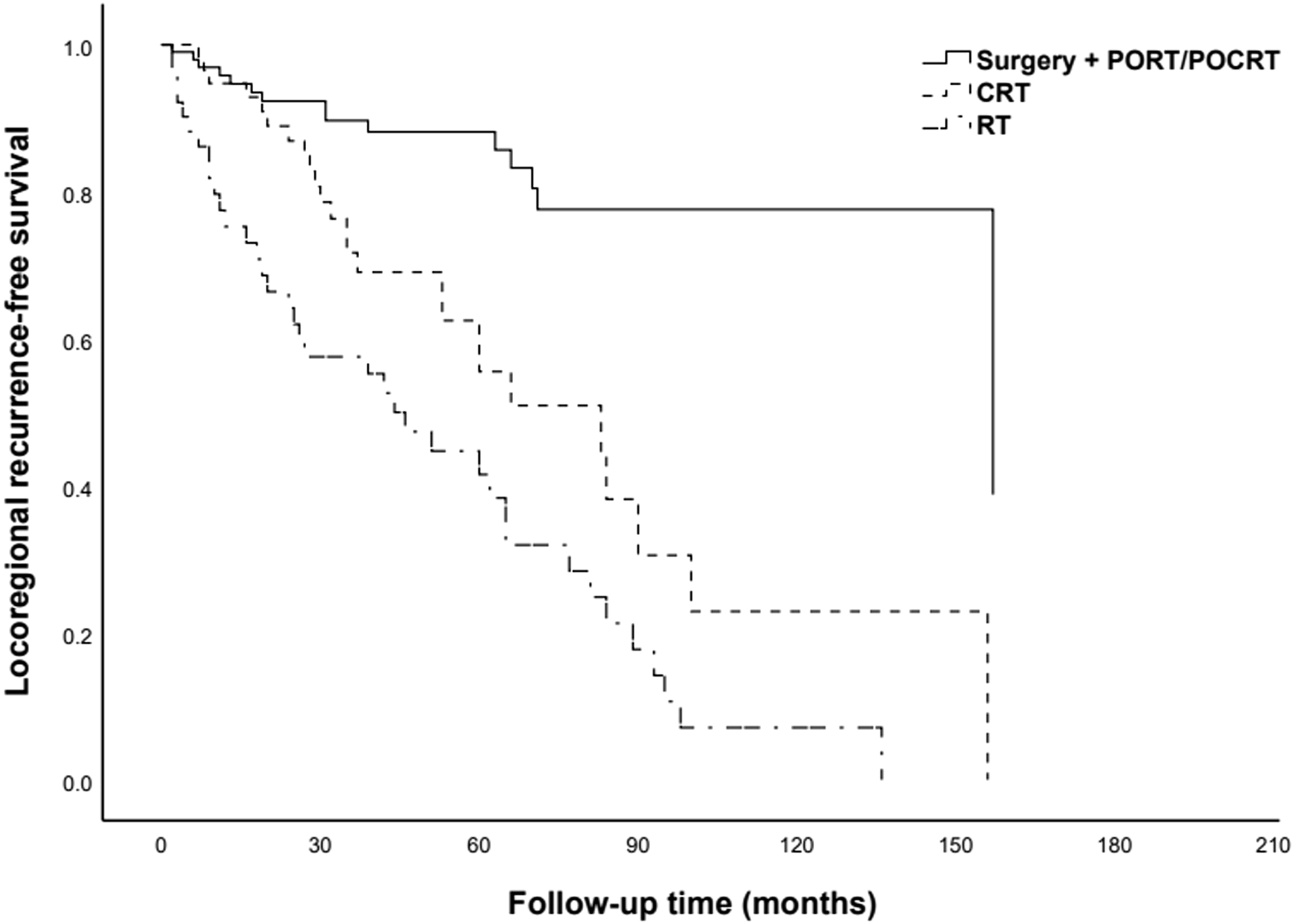
4. Discussion
In this retrospective study of 210 patients with LALC, we found that surgery + PORT/POCRT was associated with the most favorable outcomes, followed by definitive CRT, while definitive RT alone was the least effective. Independent prognostic factors for better OS and PFS included higher KPS score, moderate-to-high pathological differentiation, and higher pretreatment PNI. Additionally, the absence of a second primary cancer and the presence of a glottic primary tumor were independent predictors of better PFS.
Numerous studies have reported that the 3-year OS rate of LALC patients ranges from 48% to 86%, and their 5-year OS rate ranges from 40% to 70%,11-15 which is consistent with the results of this study. The inflammatory microenvironment, hypercoagulable state, and immune/nutritional status have generally been shown to influence the prognosis of patients with malignant tumors, and many inflammatory factors have been linked with patient prognosis specifically in laryngeal cancer.16-19 In the present study, several inflammatory factors were found to correlate with the OS and PFS of LALC patients. The pretreatment PNI was a prognostic factor for LALC, with low and high PNI values being associated with significantly worse 5-year OS rates. This result aligns with those of previous studies.20-22
The primary tumor site was also an important prognostic factor in LALC patients, and glottic cancers were generally associated with a better prognosis than non-glottic cancers. This is likely due to earlier symptom presentation (e.g., hoarseness) leading to earlier diagnosis, and the lower density of lymphatic drainage in the glottis, resulting in a lower risk of lymph node metastasis. Jin et al. 23 analyzed the outcomes of 256 LALC patients treated with PORT. They found that the primary tumor site was an independent risk factor for the prognosis of LALC patients, with significantly higher 5-year OS and disease-free survival rates in patients with glottic cancers than in those with supraglottic cancers. In the present study, patients with glottic cancers had better OS and PFS rates than those with non-glottic cancers. Our study showed the primary tumor site was an important but not an independent factor influencing the OS and an independent risk factor influencing the PFS of LALC patients.
Many studies have indicated that pathological differentiation is a significant prognostic factor in laryngeal cancer. Zhu et al. 24 analyzed their patients’ clinical data as well as data from the SEER database, and reported that poor tumor differentiation was an independent adverse prognostic factor for LALC patients undergoing PORT. Liu WS et al. 25 reported that among 1023 patients with supraglottic LALC, patients with higher tumor differentiation had significantly better 5-year OS and disease-free survival rates. Xie F 26 also reported that among 236 LALC patients who underwent PORT, the degree of pathological differentiation was an independent prognostic factor. Consistent with the above findings, the present study also identified pathological differentiation as an independent prognostic factor for OS and PFS, with patients with moderate-to-high differentiation having significantly better outcomes than those with low differentiation.
Most studies indicate that for LALC patients, surgical treatment yields better outcomes than non-surgical treatment. Wang et al. 27 reported that the 5-year OS rates of LALC patients treated with surgery + PORT/POCRT were significantly higher than those treated with definitive CRT/RT. Zhang et al. 28 and Megwalu and Sikora 29 reported similar findings. However, Bates et al. 30 reported that the 5-year OS rates were similar between PORT and definitive CRT for stage T3 LALC, and Stokes et al. 31 reported comparable OS rates for stage T4 LALC. Consistent with a recent study demonstrating superior survival with surgical approaches, 32 our results show that surgery + PORT/POCRT yielded significantly better outcomes than definitive CRT/RT in LALC patients.
While our study focused on survival outcomes, the choice of treatment for LALC must also consider laryngeal preservation. The VA and RTOG 91-11 trials established CRT as an effective organ-preservation strategy.7,8 However, detailed data on laryngeal preservation rates were not systematically collected in this retrospective study. This is a limitation of our study, and should be addressed in future prospective research.
Treatment-related toxicities are another critical factor. In our surgical group (n =101), perioperative complications were observed. In the non-surgical group, acute grade 3 or higher toxicities (primarily mucositis, dermatitis, and leukopenia) were recorded. Detailed toxicity data were not systematically collected due to the retrospective nature of this study, which is a limitation. Future studies should incorporate standardized toxicity reporting.
Another limitation of this study is that it is a retrospective, single-center study, which may introduce selection bias. Further, the sample size was relatively small, and the treatment protocols were not uniform. As mentioned before, detailed data on laryngeal preservation rates and treatment-related toxicities were not systematically collected, which are important outcomes for comparing surgical and non-surgical approaches. Further multicenter studies with larger sample sizes are needed to validate these findings.
5. Conclusion
In conclusion, our findings indicate that LALC patients with higher pretreatment KPS scores and PNI as well as moderate-to-high pathological tumor differentiation have better OS and PFS. Additionally, patients without a second primary cancer and those who have glottic laryngeal cancer have better PFS. Among the treatment modalities for LALC, surgery + PORT/POCRT was associated with the most favorable survival outcomes, followed by definitive CRT; definitive RT alone was the least effective. These results underscore the importance of patient selection and multimodality treatment planning. While surgery-based approaches remain highly effective in fit patients, definitive CRT offers a reasonable alternative with the potential for laryngeal preservation, albeit with its own toxicity profile. Prospective, multicenter studies are needed to validate these findings and further refine treatment algorithms for LALC.
Supplemental Material
Supplemental Material - Comparative Efficacy of Surgery Followed by Postoperative Radiotherapy/Chemoradiotherapy Versus Definitive Radiotherapy/Chemoradiotherapy Alone in Patients With Locally Advanced Laryngeal Cancer: Survival Outcomes and Prognostic Factors
Supplemental Material for Comparative Efficacy of Surgery Followed by Postoperative Radiotherapy/Chemoradiotherapy Versus Definitive Radiotherapy/Chemoradiotherapy Alone in Patients With Locally Advanced Laryngeal Cancer: Survival Outcomes and Prognostic Factors by Zhimeng Zhang, Yan Zhao, Meng Liu, Rong Qiu, Qi Liu, Meng Song, Zhuofan Wang, Yunfan Wu, Yuxiang Wang in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We thank Medjaden Inc. for the scientific editing of this manuscript.
Ethical Considerations
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the ethics committee of the Fourth Hospital of Hebei Medical University (2022KT262).
Consent to Participate
The need for patient consent was waived by the ethics committee due to the retrospective nature of this study.
Author Contributions
Z.Z. contributed to the acquisition and analysis of data, and to write the manuscript. Y.Z. and M.L. contributed to the acquisition and analysis of data on operative therapy, and to write the article. R.Q., M.S., Q.L., Z.W. and Y.F.W. contributed to the acquisition and analysis of data on radiotherapy, and to write the article. Y.X.W. contributed to the concept or design of the article, to direct the acquisition and analysis of data, and to write the manuscript. All authors critically revised the manuscript for intellectual content and approved the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.